

Abstract
Transgender and gender diverse (TGD) people commonly report the following gender identity milestones: feeling different about their gender than expectations for their sex assigned at birth, identifying as TGD, living in their affirmed gender, and, for some, accessing gender-affirming medical care. We explored the average ages of reaching these milestones and variations across gender groups and generational cohorts. We also examined how gender groups, generational cohorts, and endorsement of reaching each of the milestones related to minority stress variables and mental health. This online study included 695 TGD individuals ages 16–73. Boomers+ and Generation X groups were more likely to identify as trans women compared to the younger generational cohorts, who were more varied in their identities. Trans women had later ages of starting to live in their affirmed gender and receiving gender affirming medical care compared to other gender groups. The Boomers+ cohort reported later ages for the milestones compared to other generational cohorts. And, finally, younger generational cohorts had higher levels of internalized stigma, anxiety, and depression, compared to the older cohorts. Gender congruence emerged as a consistent predictor of mental health in the full sample and within each generational cohort. There are important generational differences across identity milestones, minority stress, and mental health that need exploration in future longitudinal research. In addition, beyond the effects of milestone timing, reporting feelings of congruence with one’s gender identity is an important consideration for mental health.
Keywords: transgender, identity development, nonaffirmation, gender minority, milestones
The gender identity development of transgender and gender diverse (TGD) people is an evolving process that often varies across individuals (e.g., Austin, 2016; Nuttbrock et al., 2010; Saltzburg & Davis, 2010; Tatum et al., 2020), with no single narrative for TGD identity development (Dentice & Dietert, 2015; Saltzburg & Davis, 2010). Even so, there are common milestones reported across TGD people, which include feeling different from peers or from expectations for their sex assigned at birth, adopting a gender identity that more closely aligns with their sense of self, living some or all of the time in the individual’s affirmed gender, and gender affirming medical care (James et al., 2016; Wilkinson, Pearson, & Liu, 2018; Tatum et al., 2020). In addition, researchers have found generational shifts in gender identities (Grant, Mottet, & Tanis, 2010; James et al., 2016) and gender identity milestones (Wilkinson et al., 2018).
In this study, we sought to explore gender identity milestones across gender groups and generational cohorts. We also were interested in how these milestones and generational timing related to mental health and other experiences for TGD people, such as internalized stigma, nonaffirmation of gender, gender identity acceptance, and appearance congruence. To explore these questions, we considered the concepts of milestone timing (i.e., considering sample means, as well as timing relative to the full sample and within each generational cohort) and milestone status (i.e., experienced versus not experienced; feelings of gender congruence).
Gender Identity Milestones
Research on gender identity milestones may consider both the status of a milestone (e.g., whether experienced or not experienced), as well as the relative timing of the milestone (i.e., whether the milestone occurs earlier or later than peers). Both of these aspects may be important across the common developmental milestones that TGD people report: recognition of difference, TGD identity, living in an affirmed gender, and medical gender affirmation. Furthermore, there are nuances within each of these milestones (e.g., the simultaneous exposure to stigma while feeling greater congruence with one’s self), gender differences, and contextual factors that are important to understanding each.
A common first milestone experienced by TGD individuals is the awareness that the person’s gender does not align with their sex assigned at birth (Gagne, Tewksbeury, & McGaughey, 1997; Grossman, D’Augelli, & Salter, 2008). Based on data from the 2015 US Transgender Survey which surveyed adults, retrospectively, the majority of TGD people reported feeling different from their peers regarding their gender identity by the age of 10 (60%), and many felt different before the age of 5 (32%) or between 6 and 10 years of age (28%; James et al., 2016). Even so, some TGD people reported having this experience after the age of 21 (6%; James et al., 2016).
Due to social systems that stigmatize and normalize the mistreatment of TGD people, those who have earlier timing of recognizing their gender minority identity also report more frequent gender-related victimization (Bradford et al., 2013). Another challenge that can arise for TGD individuals early on in identity development may include social isolation and symptoms of depression (Mallon & DeCrescenzo, 2006). However, some have found that this can be buffered if the individual knows of other people similar to themselves (Testa, Jimenez, & Rankins, 2014) or has a supportive family (Olson, Durwood, DeMeules, & McLaughlin, 2016).
TGD people describe discovering and labeling their gender identity after the experience of feeling different but before disclosure to a significant person in the individual’s life (Gagne et al 1997; Grossman et al., 2008; Tatum et al., 2020). Among cisgender children, acquisition of gender identity labels of others occurs around the age of 2, with personal gender identity labeling, based on their sex assigned at birth, occurring around 3 years of age (Fagot, Leinbach, & Hagan, 1986; Leinbach & Fagot, 1986; Thompson, 1975). Recent studies have found that children who are trans identified also label their gender identity as different from their sex assigned at birth at 3 years of age (Fast & Olson, 2017; Olson, Key, & Easton, 2015), although not everyone has this early experience. Research has found that there may be no differences between the gender identity development of transgender children and their cisgender siblings (Gulgoz et al., 2019).
The majority of respondents of the 2015 US Transgender Survey describe identifying and labeling their TGD identity by age 15 (54%), with some identifying as TGD at or before the age of 5 (10%), from 6 to 10 years of age (16%), from 11 to 15 years of age (28%), or later, after the age of 26 years old (8%; James et al., 2016). Using the same dataset, Tatum and colleagues (2020), found that transgender men and women were significantly younger when first labeling their gender identity compared to genderqueer people. This could be because genderqueer people may not have the language to define their experiences as such earlier on in development, given the limited knowledge children are often presented with about diverse gender identities.
Another milestone described among TGD people is living in their affirmed gender. For some TGD people this may include a social affirmation of their gender, such as changing the name they go by (in general or through legal means), the pronouns they use, or aspects of their physical appearance, such as the way they dress or their hairstyle. For others, this may include medical gender affirmation, such as the use of hormones or surgeries to either masculinize or feminize their appearance. In addition, for some TGD people, there may be a legal aspect to their gender affirmation, such as through legally changing their name or gender marker on their identification. It is important to note, however, that many TGD people may feel unsafe living in their affirmed gender due to dangerous sociopolitical contexts and may not have access to the means to medically or legally affirm their gender (James et al., 2016). For many, the ability to change a gender marker is unavailable due to local laws, criteria for changing gender markers, or the lack of ability to change identification documents to a nonbinary identity (Grant et al., 2011; James et al., 2016). For example, in separate studies, only 21% (Grant et al., 2011) and 11% (James et al., 2016) of participants were able to change all their records and identification documents to reflect their gender. Due to a variety of reasons, such as fear of rejection or threats of harm by others, some TGD people may not be able to live in their affirmed gender or may have uncertainty about doing so (Grant et al., 2011; James et al., 2016).
The age of starting to live in an affirmed gender identity is varied, yet many describe this milestone occurring during early to middle adulthood (Grant et al., 2011; James et al, 2015; Tatum et al., 2020). Specifically, Grant and colleagues (2011) found that most participants started living in their affirmed gender between the ages of 18 and 44. In another study, James and colleagues (2016) found that the majority of participants began living in their affirmed gender between the ages of 18 and 24 (43%) or between the ages of 25 and 34 (24%), with fewer beginning during adolescence (under the age of 18; 15%) and later in adulthood (over the age of 35; 18%; James et al., 2016). The timing of beginning to live in an affirmed gender also varies across gender identities. For example, some studies find that transgender men and nonbinary identified people start to live in their affirmed gender at earlier ages, on average, compared to transgender women (Grant et al., 2011; James et al., 2016; Tatum et al., 2020). Tatum and colleagues (2020) found that the average age for living in an affirmed gender occurred earliest and with the smallest age range for genderqueer people assigned female at birth (M = 20.32; SD = 6.44), transgender men (M = 23.85; SD = 8.88), and genderqueer people assigned male at birth (M = 24.22; SD = 10.01). Transgender women reported being significantly older, 34.48 years of age (SD = 13.62) on average, when living as their affirmed gender (Tatum et al., 2020).
Researchers have found that there are many benefits to living in one’s affirmed gender. Among TGD youth who were able to socially transition (meaning that this milestone status is experienced, and at an early timing), they reported similar depression symptoms compared to their cisgender peers (Olson et al., 2016), showing that social affirmation of identity can be protective for TGD youth. In a study of 300 transgender and nonbinary youth in Brazil, those who were unable to express their gender identity exhibited greater depressive symptoms and those who had a mother who never used their desired name reported greater depressive symptoms and anxiety (Fontanari et al., 2020). Other research has indicated that genderqueer people who affirmed their gender reported a decrease in gender dysphoria (Galupo, Pulice-Farrow, & Lindley, 2019). Generally, when TGD individuals can live according to the gender they identify with (i.e., when this milestone is experienced), they report better mental health and wellbeing (e.g., Fontanari et al., 2020; Olson et al., 2016).
Another milestone that is a part of some TGD people’s experience is receiving gender affirming medical care, most often in the form of hormone therapy (Grant et al., 2011). In a study of 229 transgender women and 121 transgender men, medical gender affirmation was first explored, on average, at 29 years of age (SD = 11.88; Bradford, Reisner, Honnold, & Xavier, 2013). A little over half of participants reported receiving hormone therapy (57%), with fewer reporting gender affirming surgeries (22%; Bradford et al., 2013). In one of the few studies to measure medical gender affirmation in a sample with more diverse gender identities, Puckett and colleagues (2018a) found that 61.3% of their sample had obtained hormone therapy, with this more frequently reported by trans men (76.8%) and transgender women (80.3%) compared to other gender groups. Even so, a notable portion of genderqueer (28.6%) and nonbinary participants (33.3%) had received hormone therapy. There were additional participants who desired this form of medical gender affirmation in the future (16.8%) and some who were questioning (13.7%) the use of hormone therapy in the future (Puckett et al., 2018a). It is important to note that only a small minority (7.8%) of the whole sample were uninterested in future hormone therapy (Puckett et al., 2018a). Similar to Bradford and colleagues (2013), surgeries were less common overall (Puckett et al., 2018a).
The experience of the milestone of TGD affirming healthcare (when desired), has been associated with better mental health outcomes and less need for mental health services (see reviews, Nguyen et al., 2018; White & Reisner, 2016). Among a sample of transgender men with high rates of depression (66%), those who had not begun but were in the planning stages of medical gender affirmation reported greater depressive symptoms compared to transgender men who had medically affirmed their gender (Rotondi et al., 2011). In a study of transgender women, those who received gender-affirming healthcare reported lower rates of suicidal ideation and engaged in less substance abuse related behaviors compared to those who did not seek gender-affirming healthcare (Wilson et al., 2015). In a study that compared transgender adults who had received gender affirming medical interventions to those who did not (all desired medical interventions), they found that those who received medical interventions reported better mental health and lower substance abuse (Tomita, Testa, & Balsam, 2018). Overall, a recent review found that gender affirming hormone therapy had a positive impact on multiple dimensions of psychological and behavioral health for transgender people (Nguyen et al., 2018).
Although gender affirming medical care is a common milestone reported by TGD people, it also is important to note that there are many barriers to receiving such care. Research has shown that TGD people often encounter providers who hold bias against TGD people, experience marginalization on the part of office staff, or are denied services (Grant et al., 2011; Kenagy, 2005; Puckett et al., 2018a). One of the largest barriers to healthcare is the lack of knowledge about transgender care among medical professionals (Bradford et al., 2013; Puckett et al., 2018a), with as many as 50% of TGD people reporting that they had to educate their providers about healthcare for TGD people (Grant et al., 2011). In addition, beyond these barriers, not all TGD people desire gender-affirming medical interventions and thus this milestone does not apply to every TGD person (Puckett et al., 2018a).
Generational Cohorts, Age, and Identity Milestones
Very little research has examined generational differences regarding the timing of gender identity milestones and associations with mental health outcomes. As mentioned prior, there have been generational shifts in gender identity labels with younger age groups being more likely to identify as nonbinary or gender nonconforming compared to older TGD people (e.g., Grant at el., 2011; James et al., 2016). In a study exploring gender identity milestones of TGD people across generations, researchers found that younger generations were experiencing gender identity milestones at earlier ages, specifically, identifying as transgender and living as their affirmed gender occurred at much earlier ages among younger generations of TGD people compared to older generations (Wilkinson et al., 2018). In a recent study, Barsigian and colleagues (2020), conducted semi-structured interviews with genderqueer people from three generations. They found that older generations had a difficult time finding terms that defined their gender experience and identity, which delayed their gender identification, along with feeling an increased risk of victimization and discrimination due to a lack of language and being disconnected from the LGBTQ community at the time (Barsigian et al., 2020). In addition, medical gender affirmation is likely helpful across the lifespan, with older adults who report recent medical affirmation displaying higher quality of life scores compared to those without medical affirmation or younger TGD people (Cai et al., 2019).
Although research examining the timing of these milestones has been limited, many more studies have examined the association between age overall (regardless of milestones) and mental health for TGD people, providing a context for understanding shifts across generational cohorts. Researchers have found that younger TGD people report greater mental health difficulties compared to their older peers (e.g., Bariola et al., 2015; Bockting, Miner, Swinburne Romine, Hamilton, & Coleman, 2013; Nuttbrock et al., 2010). In one study of 571 transgender women, older participants had lower levels of depression and suicidal ideation compared to their younger counterparts (Nuttbrock et al., 2010). Related, a survey of 169 transgender men and women found that younger TGD people had higher rates of mental health difficulties, along with more frequent victimization, compared to older TGD people (Bariola et al., 2015). It is possible that as TGD people age there are shifts in minority stressors, such as internalized stigma, with older TGD people reporting lower internalized transphobia and better mental health compared to their younger peers (Jackman, Dolezal, & Bockting, 2018). It also is possible that older TGD people have greater resilience in the face of marginalization. For instance, Nuttbrock et al. (2014) found that the association between psychological abuse and depression was much higher in younger trans women compared to older groups.
Although younger TGD people appear to be facing more challenges related to mental health and minority stress compared to older TGD people (e.g., Bariola et al., 2015; Bockting, Miner, Swinburne Romine, Hamilton, & Coleman, 2013; Nuttbrock et al., 2010), it should also be acknowledged that there are unique challenges that TGD older adults may face. For instance, TGD older adults may have challenges in paying for long-term care, may live alone and be isolated, may experience lasting effects of low wages and employment discrimination, and mistreatment in nursing homes (Williams & Freeman, 2007). As such, there are structural and environmental factors that may influence overall mental health for TGD older adults (Fredriksen-Goldsen et al., 2014).
Examining generational cohorts is one way to evaluate the roles of age, sociopolitical context, environment, and individual differences. Across time, there have been significant shifts in the visibility of TGD people (e.g., early narratives such as Christine Jorgensen and more recent experiences of people like Laverne Cox), legal recognition of TGD people’s identities (e.g., changes in policies that allow people to update their gender markers on birth certificates or identification documents), access to gender affirming medical care (e.g., shifts in the standards of care and practice guidelines), and protests for rights (e.g., early movements like Compton cafeteria riots and Stonewall riots, to more recent marches to protest the killings of Black trans women). Just as there has been a rise in visibility and in movements to advocate for TGD people, there also has been a rise in legislation that seeks to restrict the rights of TGD people in domains like access to gender inclusive restrooms (e.g., Schuster et al., 2016). Overall, examining generational cohorts may provide a way to contextualize these social shifts, mental health, and minority stress experiences.
Current study
Given the range of experiences that TGD people have in regards to identity development, we explored 1) milestone timing via the average ages that participants reported reaching each of the commonly endorsed milestones (awareness of difference, identifying as TGD, living in an affirmed gender, and gender-affirming medical care); 2) whether generational cohort groupings were associated with gender identity; 3) how the gender and generational cohort groups differed in regard to milestone timing (average ages at which they endorsed each of the gender identity milestones); 4) whether milestone status (experienced or not experienced) differed according to gender and generational cohort, as well as in relation to the following variables: internalized stigma, gender non-affirmation, appearance congruence, gender identity acceptance, anxiety symptoms, and depression symptoms; and 5) how relative timing of milestones (within the full sample and within the generational cohorts) and milestone status (measured by a gender congruence scale) related to mental health. This final analysis allowed us to consider, simultaneously, the effects of milestone timing and status, while controlling for current age of participants.
We hypothesized, based on existing literature (e.g., Grant et al., 2011; James et al., 2016), that older generational cohorts may be more likely to identify as trans women instead of other gender identities and that younger generational groups would have greater variation in their gender identities. We also expected that trans women would start living in their affirmed gender at older ages with later milestone timing than the other gender groups and younger generations would have earlier milestone timing and reach milestones at younger ages than the older generational cohorts. In addition, we hypothesized that milestone status (endorsing experiencing the gender identity milestones) would be associated with better outcomes (e.g., less internalized stigma and fewer symptoms of depression and anxiety); however, given the lack of literature in these areas we did not have a priori hypotheses for how the gender or generational cohorts would differ on these variables. Finally, we did not develop specific hypotheses about how relative timing of milestones may relate to mental health given the lack of literature to guide hypotheses in this area, but we did hypothesize that reporting greater gender congruence would be associated with more positive outcomes (e.g., less internalized stigma and fewer symptoms of depression and anxiety).
Method
Participants
A total of 861 individuals accessed the online survey and their responses were reviewed. After removing participants who were disqualified from the study due to data screening to ensure quality of the online data collection methods, the final sample included 695 participants. Full details regarding disqualification of individuals is available in Puckett et al. (2020). Individuals in the final sample had an average age of 25.52 years old (SD = 9.68; range 16 – 73 years). Participants reported a range of gender identities, including transgender men (30.4%), transgender women (16.6%), genderqueer (12.5%), and nonbinary (19%), as well as other gender identities (21.6%). Participants were able to write-in their gender identity if it was not listed as an option (examples of written responses: “neutrois,” “genderflux”). There were 534 (76.8%) participants who reported being female assigned at birth and 156 (22.4%) participants identified as male assigned at birth (5 participants did not report their sex assigned at birth). Most participants endorsed a sexual minority identity (87.8%) and were white (75.7%). Notably, there were very low levels of income despite participants’ education levels, with over half of the sample (51.4%) earning less than $10,000 a year. Table 1 includes a full description of the sample, along with a breakdown of demographics in each generational cohort.
Table 1.
Sample Demographics
| Characteristic | Total Sample (N = 695) n (%) |
Boomers+ (n = 27) n (%) |
Generation X (n = 55) n (%) |
Millennials (n = 415) n (%) |
Generation Z (n = 196) n (%) |
|---|---|---|---|---|---|
| Gender Identity | |||||
| Transgender Man | 180 (25.9%) | 2 (7.4%) | 10 (18.2%) | 109 (26.3%) | 58 (29.6%) |
| Transgender Woman | 105 (15.1%) | 17 (63%) | 22 (40%) | 50 (12%) | 16 (8.2%) |
| Woman | 10 (1.4%) | 2 (7.4%) | 0 | 6 (1.4%) | 2 (1%) |
| Man | 31 (4.5%) | 0 | 3 (5.5%) | 22 (5.3%) | 6 (3.1%) |
| Genderqueer | 87 (12.5%) | 3 (11.1%) | 8 (14.5%) | 62 (14.9%) | 14 (7.1%) |
| Nonbinary | 132 (19%) | 2 (7.4%) | 6 (10.9%) | 76 (18.3%) | 48 (24.5%) |
| Agender | 66 (9.5%) | 0 | 2 (3.6%) | 41 (9.9%) | 23 (11.7%) |
| Androgyne | 7 (1%) | 0 | 2 (3.6%) | 5 (1.2%) | 0 |
| Bigender | 22 (3.2%) | 0 | 1 (1.8%) | 14 (3.4%) | 7 (3.6%) |
| Option Not Listed | 55 (7.9%) | 2 (7.4%) | 1 (1.8%) | 30 (7.2%) | 22 (11.2%) |
| Sex Assigned at Birth | |||||
| Female | 534 (76.8%) | 8 (29.6%) | 29 (52.7%) | 329 (79.3%) | 166 (84.7%) |
| Male | 156 (22.4%) | 19 (70.4%) | 25 (45.5%) | 83 (20%) | 29 (14.8%) |
| Difference of Sex Development | |||||
| Unsure | 124 (17.8%) | 6 (22.2%) | 11 (20%) | 74 (17.8%) | 33 (16.8%) |
| Yes | 20 (2.9%) | 0 | 3 (5.5%) | 11 (2.7%) | 6 (3.1%) |
| No | 551 (79.3%) | 21 (77.8%) | 41 (74.5%) | 330 (79.5%) | 157 (80.1%) |
| Sexual Orientation | |||||
| Queer | 174 (25%) | 5 (18.5%) | 16 (29.1%) | 123 (29.6%) | 29 (14.8%) |
| Pansexual | 130 (18.7%) | 5 (18.5%) | 9 (16.4%) | 65 (15.7%) | 51 (26%) |
| Bisexual | 106 (15.3%) | 4 (14.8%) | 13 (23.6%) | 58 (14%) | 31 (15.8%) |
| Gay | 62 (8.9%) | 2 (7.4%) | 2 (3.6%) | 35 (8.4%) | 23 (11.7%) |
| Asexual | 100 (14.4%) | 2 (7.4%) | 4 (7.3%) | 59 (14.2%) | 34 (17.3%) |
| Heterosexual | 38 (5.5%) | 3 (11.1%) | 6 (10.9%) | 26 (6.3%) | 3 (1.5%) |
| Lesbian | 35 (5%) | 4 (14.8%) | 4 (7.3%) | 18 (4.3%) | 9 (4.6%) |
| Option Not Listed | 50 (7.2%) | 2 (7.4%) | 1 (1.8%) | 31 (7.5%) | 16 (8.2%) |
| Race/Ethnicity | |||||
| White | 526 (75.7%) | 23 (85.2%) | 45 (81.8%) | 317 (76.4%) | 139 (70.9%) |
| Black/African American | 13 (1.9%) | 1 (3.7%) | 1 (1.8%) | 5 (1.2%) | 6 (3.1%) |
| American Indian or Alaska Native | 1 (0.1%) | 0 | 0 | 1 (0.2%) | 0 |
| Native Hawaiian or Other Pacific Islander | 0 | 0 | 0 | 0 | 0 |
| Asian | 21 (3%) | 0 | 1 (1.8%) | 13 (3.1%) | 7 (3.6%) |
| Latino/a | 25 (3.6%) | 0 | 2 (3.6%) | 12 (2.9%) | 11 (5.6%) |
| Option Not Listed | 8 (1.2%) | 1 (3.7%) | 0 | 6 (1.4%) | 1 (0.5%) |
| Multiracial/Multiethnic | 98 (14.1%) | 2 (7.4%) | 6 (10.9%) | 58 (14%) | 32 (16.3%) |
| Education | |||||
| Less than high school diploma | 91 (13.1%) | 0 | 0 | 3 (0.7%) | 87 (44.4%) |
| High school graduate or equivalent | 88 (12.7%) | 0 | 4 (7.3%) | 46 (11.1%) | 38 (19.4%) |
| Some college, but have not graduated | 228 (32.8%) | 3 (11.1%) | 12 (21.8%) | 144 (34.7%) | 69 (35.2%) |
| Associates degree or technical school degree | 52 (7.5%) | 7 (25.9%) | 5 (9.1%) | 39 (9.4%) | 1 (0.5%) |
| Bachelor’s degree | 160 (23%) | 10 (37%) | 19 (34.5%) | 130 (31.3%) | 1 (0.5%) |
| Master’s degree | 63 (9.1%) | 5 (18.5%) | 12 (21.8%) | 45 (10.8%) | 0 |
| Doctorate or professional degree | 13 (1.9%) | 2 (7.4%) | 3 (5.5%) | 8 (1.9%) | 0 |
| Income | |||||
| Less than $10,000 | 357 (51.4%) | 6 (22.2%) | 13 (23.6%) | 193 (46.5%) | 143 (73%) |
| $10–19,999 | 112 (16.1%) | 6 (22.2%) | 5 (9.1%) | 91 (21.9%) | 10 (5.1%) |
| $20–29,999 | 59 (8.5%) | 2 (7.4%) | 4 (7.3%) | 47 (11.3%) | 6 (3.1%) |
| $30–39,999 | 49 (7.1%) | 3 (11.1%) | 3 (5.5%) | 34 (8.2%) | 9 (4.6%) |
| $40–49,999 | 39 (5.6%) | 4 (14.8%) | 10 (18.2%) | 19 (4.6%) | 6 (3.1%) |
| $50–69,999 | 36 (5.2%) | 2 (7.4%) | 10 (18.2%) | 17 (4.1%) | 7 (3.6%) |
| $70–99,999 | 29 (4.2%) | 2 (7.4%) | 9 (16.4%) | 10 (2.4%) | 8 (4.1%) |
| Over $100,000 | 11 (1.6%) | 2 (7.4%) | 1 (1.8%) | 3 (0.7%) | 5 (2.6%) |
Note. There were 5 participants with missing data on the question asking about sex assigned at birth, and 3 participants with missing data about their race/ethnicity and income. The classification of “man” and “woman” refer to trans men and trans women respectively, as there were no cisgender individuals in the sample. For analyses, the categories of “man” and “transgender man” were combined, as were the categories of “woman” and “transgender woman.” These options were provided for participants who do not identify with the prefix of “trans” for their gender identities.
Procedures
Recruitment took place through various social media outlets (e.g., Facebook, Twitter, Tumblr), flyers distributed electronically to community organizations that work with TGD people, and in-person recruitment at community events. Social media advertisements were sent to leaders of community organizations and groups that worked with TGD individuals and to social media sites that were for TGD people and we asked these individuals to share the call for participants. The flyers and posts that were distributed mentioned the inclusion criteria of being TGD and ages 16 and over, but did not mention a focus on substance use or sexual health as to avoid recruitment biases (more info below). All procedures were approved by the Institutional Review Board of the primary investigator’s institutions and there was a waiver of parental permission for participants who were 16–17 years old under 45 CFR 46.408(c). Although funding was not available for the first 200 participants who completed the study, the subsequent participants received a $5 Amazon gift card.
This data is from a broad study with two distinct components: 1) a daily diary study of minority stress, substance use, and sexual health, and 2) a one-time survey administered to individuals who did not meet inclusion criteria to receive the daily diaries. To qualify for the daily diary study, participants had to meet all of the following criteria: they were between 16 to 40 years old; identified as trans men, trans women, genderqueer, or nonbinary; lived in the US; had sex in the past 30 days; and either binge drank or used substances in the past 30 days. Participants who did not meet criteria for the daily diary study, but were ages 16 and over, living in the U.S., and TGD identified in any way were invited to participate in the one-time survey. A screener questionnaire was first completed to determine which component of the study participants qualified for and they were then contacted with follow up information about how to proceed. The data presented in this manuscript includes participants only from the one-time survey (measures differed across the survey and daily diary components and thus are not combined); both are described here as the enrollment procedures may influence the sample characteristics.
We employed several strategies for ensuring the quality of the online data collection (see Puckett et al., 2020, for a full description of these methods). In addition, a community advisory board (CAB) composed of local TGD individuals helped inform this study. The CAB met regularly prior to the launch of the study and throughout data collection and early stages of interpretation. These meetings helped to ensure that the study was examining meaningful questions in ways that were culturally appropriate for this marginalized community.
Measures
Demographics.
Demographic questions included: age, gender, sex assigned at birth, differences of sex development (i.e., intersex), sexual orientation, race/ethnicity, income, employment, and education. The response options for these items are available in Table 1.
Milestone timing and status.
Participants completed five questions regarding the ages at which they 1) first recognized they felt “different” about their gender, 2) first recognized a TGD identity, 3) began to live part time as a TGD person, 4) began to live full time as a TGD person, and 5) had any kind of medical gender affirmation (Grant et al., 2011). Participants were allowed to skip items that did not apply to them because not all milestones apply to every TGD individual’s process of gender affirmation or participants may not have moved through all of the milestones at that point in time. The specific ages participants reported were utilized as milestone timing variables, whether or not participants reported an age was utilized as one of the measures of milestone status (experienced or not).
Identity congruence and acceptance.
The Transgender Identity Congruence Scale (Kozee, Tylka, & Bauerband, 2012) included 12 items aligning to 2 subscales. The Appearance Congruence subscale included items regarding feeling that one’s appearance represented their gender identity (e.g., “I am happy with the way my appearance expresses my gender identity.”). The Gender Identity Acceptance subscale included items regarding personal acceptance about being TGD (e.g., “I have accepted my gender identity.”). Items were rated on a 5-point scale (1 = strongly disagree, 5 = strongly agree) and the appropriate items were reverse scored before calculating means for each subscale. Higher scores indicated stronger feelings of appearance congruence and higher levels of acceptance. This measure has been validated in prior research, demonstrating adequate construct validity and reliability (Kozee, Tylka, & Bauerband, 2012). In the current study, Cronbach’s alpha = .93 and .77 for the Appearance Congruence and Gender Identity Acceptance subscales, respectively. We used these subscales as a second measure of milestone status given that congruence is an outcome of these milestones.
Internalized stigma.
The Internalized Transphobia subscale of the Gender Minority Stress and Resilience Measure (Testa, Habarth, Balsam, & Bockting, 2015) was used to assess negative feelings about being transgender (e.g., “I resent my gender identity or expression.”). These eight items were rated on a 5-point scale (1 = strongly disagree, 5 = strongly agree) and a scale score was calculated by summing items so that higher scores indicated greater internalized stigma. Prior research provides support for the factor structure of this measure, construct validity, and reliability (Testa, Habarth, Balsam, & Bockting, 2015). In the current study Cronbach’s alpha = .89.
Non-affirmation of identity.
The Non-Affirmation subscale of the Gender Minority Stress and Resilience Measure assessed rejection of participants’ gender identity by others and the treatment of participants in ways that did not align with their gender, such as misgendering (e.g., using the wrong pronoun for participants) and similar actions (e.g., “People don’t respect my gender identity because of my appearance or body.”). These six items were rated on a 5-point scale (1 = strongly disagree, 5 = strongly agree) and a scale score was calculated by summing items. Higher scores indicated greater feelings of non-affirmation. Prior research provides support for the factor structure of this measure, construct validity, and reliability (Testa, Habarth, Balsam, & Bockting, 2015). Cronbach’s alpha in the current study was .88.
Mental health.
To assess mental health, we included two measures: the Patient-Reported Outcomes Measurement Information System (PROMIS) – Depression scale and the PROMIS – Anxiety scale (Cella et al., 2011). These scales assessed feelings of depression (8 items, e.g., feeling worthless, helpless, or sad) and anxiety (7 items, e.g., feeling fearfulness, worried, or tense) over the past week. Participants indicated how often they experienced each of the symptoms on a 5-point scale (1 = never, 5 = always). A raw score was first computed and then converted to T-scores to standardize the scores against national norm data. Both scales have demonstrated high levels of reliability and validity, with this scale originally developed with a large nationally representative sample of over 20,000 individuals (Cella et al., 2011). However, these measures have not been validated in a sample of TGD people. In the current study, Cronbach’s alpha was .95 and .94 for the depression and anxiety scales respectively.
Data Preparation and Statistical Analyses
All data analyses were conducted in SPSS. Only participants with at least 80% of data for each measure were retained when calculating scale scores. On the scales included in our analyses, the participants with missing data ranged from 1.6–2.7%. Given this low percentage, missing data was addressed using list-wise deletion across analyses. Participants were able to not report the age for milestones and thus, the number of participants without responses to these items are not captured in the missing data percentages and instead descriptive information is provided regarding endorsing these milestones.
First, we conducted analyses to provide descriptive information on characteristics of the sample. Due to a low number of participants in some gender groups, we combined androgyne and bigender, with the “Not Listed” group. Participants who selected “man” and “transgender man” in the gender item were combined, as were participants who selected “woman” and “transgender woman.” We calculated generational cohort groups based on the following ranges (Dimock, 2019; Wilkinson et al., 2018): participants born before 1964 were classified as the “Boomer+” group to indicate they were part of the baby boomer generation or older; participants born between 1965 and 1980 were classified as Generation X; participants born between 1981 and 1996 were classified as Millennials; and participants born between 1997–2012 were classified as Generation Z. Birth year was calculated by subtracting age from year of completing the study. Chi-square analyses were conducted to identify associations between generational cohort and gender identity.
Continuous variables were screened for normality and no variables needed to be transformed. A series of ANOVAs compared the gender groups and generational cohorts on milestone timing (i.e., average ages of each of the milestones) and on the following variables: internalized stigma, gender non-affirmation, appearance congruence, gender identity acceptance, anxiety symptoms, and depression symptoms. Then, t-tests were conducted to compare participants based on one of the measures of milestone status (i.e., comparing those who did and did not report an age for each milestones) on the same variables as the previous analysis.
Finally, we calculated z scores to determine the relative timing of the milestones in relation to the full sample, as well as z scores to determine the relative timing of the milestones in relation to each of the generational cohorts. After calculating these values, we conducted a series of regression analyses in which we entered 1) z scores (separate analyses for z scores relative to the full sample and generational cohorts), 2) age, and 3) the gender appearance congruence and gender identity acceptance subscales of the Transgender Identity Congruence Scale as a measure of milestone status to predict depression and anxiety symptoms. In this final analysis, we used the measure of gender congruence to assess milestone status because this is an outcome of affirming one’s gender and thus reflects moving through these milestones. Furthermore, we were not able to use our other milestone status variable (whether each milestone was experienced or not) in these analyses because there is no variability in this within each regression (i.e., to report an age for a milestone means that it was experienced and there would be no participants in each of the respective analyses who reported not experiencing a given milestone).
Results
When examining responses to the milestone questions, there were two participants with inconsistent responses (the ages reported were older than their current age) and these individuals were removed from the data. Of the 693 participants remaining in the sample, 27 were Boomers+ (3.9%), 55 were Generation X (7.9%), 415 were Millennials (59.9%), and 196 were Generation Z (28.3%). We found a significant association between generational cohort and gender identity groups [χ² (15) = 103.68, p < .001; Cramer’s V = .22.], such that the Boomers+ and Generation X cohorts were more likely to be trans women than other gender groups. Millennials and Generation Z groups were more varied in gender, especially among genderqueer, nonbinary, agender, and not listed groups (see Table 2). Some cell counts were very low, especially in the Boomers+ group, and should be interpreted with caution.
Table 2.
Chi-Square Analyses Examining the Associations between Gender and Generational Cohorts
| Trans Men |
Trans Women |
Genderqueer |
Nonbinary |
Agender |
Not Listed |
|||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Boomers + | 2a | 7.4% | 19b | 70.4% | 3a | 11.1% | 1a | 3.7% | 0a | 0% | 2a | 7.4% |
| Generation X | 13a | 23.6% | 22b | 40.0% | 8a | 14.5% | 6a | 10.9% | 2a | 3.6% | 4a | 7.3% |
| Millennials | 131a, b | 31.6% | 56c | 13.5% | 62b | 14.9% | 76a, c | 18.3% | 41a, b, c | 9.9% | 49a, b, c | 11.8% |
| Generation Z | 64a | 32.7% | 18b | 9.2% | 14b | 7.1% | 48a | 24.5% | 23a | 11.7% | 29a | 14.8% |
Note. Means sharing a subscript within a generational cohort are not significantly different from one another. Percentages align to percent of sample within a specific gender group in each generational cohort.
According to ANOVAs, there were significant differences between the gender groups across all of the gender identity milestones in regards to milestone timing, although the effects were small [Felt Different: F (5, 674) = 4.01, p < .01, eta squared = .03; TGD Identity: F (5, 685) = 3.29, p < .01, eta squared = .02; Living Part Time: F (5, 636) = 14.94, p < .001, eta squared = .11; Living Full Time: F (5, 462) = 17.26, p < .001, eta squared = .16; First TGD-Related Medical Care: F (5, 357) = 13.38, p < .001, eta squared = .16]. Tukey post-hoc comparisons revealed several between-group differences, displayed in Table 3. Most notably, trans women appeared to start living in their affirmed gender and receiving TGD-related medical care at later ages compared to the other groups, meaning they had later milestone timing (see Figure 1).
Table 3.
ANOVA Findings Regarding Group Differences in Ages Participants Reported Reaching Each Identity Milestone
| Felt Different |
TGD Identity |
Living PT |
Living FT |
First TGD-Related Medical Care |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Gender: | n | M | SD | n | M | SD | n | M | SD | n | M | SD | n | M | SD |
| Trans Men | 208 | 10.10a | 5.40 | 210 | 17.25a | 5.57 | 202 | 19.08a | 5.41 | 178 | 21.29a | 6.18 | 153 | 22.25a | 6.17 |
| Trans Women | 113 | 10.72ab | 9.37 | 114 | 19.44ab | 10.43 | 103 | 25.87c | 10.99 | 74 | 30.86c | 13.09 | 89 | 31.64c | 13.64 |
| Genderqueer | 85 | 12.66b | 6.76 | 87 | 20.45b | 8.20 | 80 | 22.05b | 8.27 | 64 | 24.57a | 8.40 | 33 | 25.67a | 6.33 |
| Nonbinary | 127 | 12.16ab | 4.98 | 131 | 18.37ab | 4.89 | 120 | 19.78ab | 5.29 | 70 | 20.93a | 6.42 | 39 | 23.54a | 6.86 |
| Agender | 64 | 12.92b | 5.90 | 66 | 18.83ab | 4.92 | 60 | 19.17ab | 4.54 | 40 | 20.90a | 5.73 | 17 | 23.29a | 5.03 |
| Not Listed | 83 | 12.33ab | 5.96 | 83 | 18.81ab | 5.98 | 77 | 20.72ab | 6.25 | 42 | 22.69a | 8.08 | 32 | 26.00a | 8.32 |
| Age Cohorts: | n | M | SD | N | M | SD | n | M | SD | n | M | SD | n | M | SD |
|
| |||||||||||||||
| Boomers + | 27 | 13.89a | 17.31 | 27 | 25.67a | 19.09 | 22 | 39.91a | 14.88 | 21 | 49.90a | 9.92 | 22 | 50.86a | 10.96 |
| Generation X | 55 | 9.35b | 6.88 | 54 | 23.72a | 12.21 | 51 | 30.29b | 10.74 | 43 | 33.81b | 9.68 | 43 | 35.60b | 7.89 |
| Millennials | 404 | 11.56ab | 6.11 | 414 | 19.04b | 4.87 | 388 | 20.77c | 4.36 | 297 | 22.17c | 4.40 | 240 | 23.09c | 4.21 |
| Generation Z | 194 | 11.47ab | 3.94 | 196 | 15.18c | 1.83 | 181 | 16.12d | 1.59 | 107 | 16.94d | 1.51 | 58 | 17.62d | 1.07 |
Note. Gender identity group means sharing subscripts are not significantly different from one another. TGD = transgender and gender diverse.
Figure 1.
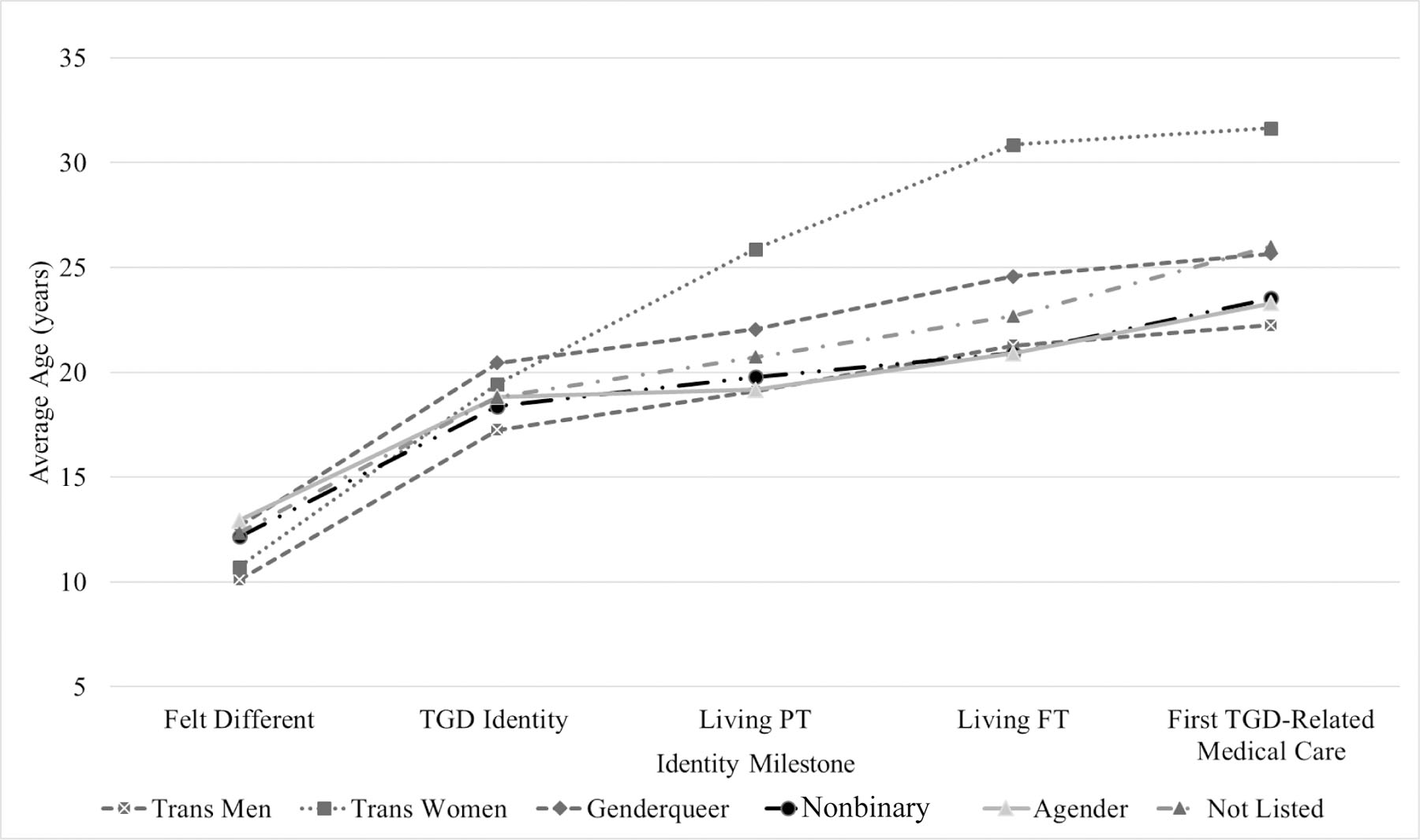
Average Ages Reported for Identity Milestones by Gender Groups.
ANOVAs revealed significant differences between the generational cohorts across all of the gender identity milestones in terms of milestone timing, with effect sizes ranging substantially across milestones [Felt Different: F (3, 676) = 3.25, p < .05, eta squared = .01; TGD Identity: F (3, 687) = 42.30, p < .001, eta squared = .16; Living Part Time: F (3, 638) = 193.66, p < .001 eta squared = .48; Living Full Time: F (3, 464) = 316.59, p < .001 eta squared = .67; First TGD-Related Medical Care: F (3, 359) = 298.09, p < .001 eta squared = .71]. Tukey post-hoc comparisons revealed several between-group differences, displayed in Table 3. Figure 2 displays the average ages at which each generational cohort reported reaching the identity milestones. Overall, Boomers+ tended to report older ages for reaching the identity milestones compared to the other generations, thus having later milestone timing. The younger generational cohorts also had shorter gaps of time between their milestones compared to the older generational cohorts.
Figure 2.
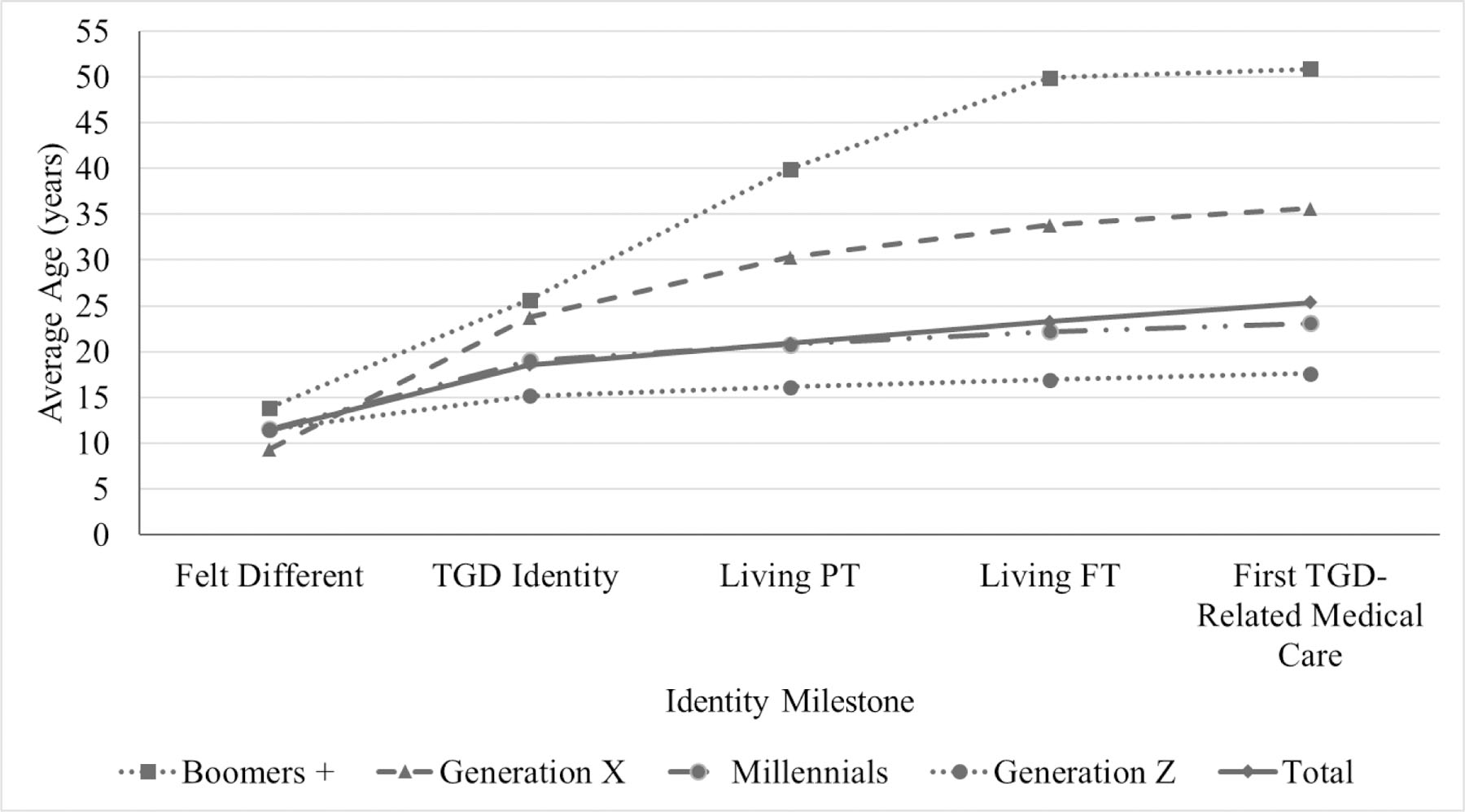
Average Ages Reported For Identity Milestones by Generational Cohorts.
The generational cohorts differed in regard to internalized stigma [F (3, 678) = 12.11, p < .001, eta squared = .05], gender non-affirmation [F (3, 676) = 12.72, p < .001, eta squared = .05], appearance congruence [F (3, 676) = 9.31, p < .001, eta squared = .04], gender identity acceptance [F (3, 676) = 4.73, p < .01, eta squared = .02], anxiety [F (3, 672) = 14.42, p < .001, eta squared = .06], and depression [F (3, 670) = 19.66, p < .001, eta squared = .08]. Tukey post-hoc comparisons revealed various between-group differences, with younger generations reporting more difficulty in their current lives compared to older generations (e.g., greater internalized stigma, more anxiety and depression symptoms; see Table 4). Notably, only the Boomers+ generational cohort (with an average age of 59 years old) had depression scores similar to the average for the nationally representative sample in the original validation study for the PROMIS measures, whereas all younger cohorts had depression symptoms that were almost a standard deviation higher or more.
Table 4.
ANOVA Findings Regarding Generational Differences on Study Variables
| Boomers+ M (SD) |
Generation X M (SD) |
Millennials M (SD) |
Generation Z M (SD) |
|
|---|---|---|---|---|
| Internalized Stigma | 16.12 (7.32)c | 21.44 (8.46)ab | 21.23 (7.99)a | 24.53 (8.40)b |
| Gender Non-Affirmation | 18.15 (7.58)a | 20.17 (7.54)ab | 22.38 (6.32)b | 24.33 (4.89)c |
| Appearance Congruence | 3.08 (1.34)a | 2.78 (1.24)ab | 2.50 (1.03)b | 2.21 (0.84)c |
| Gender Identity Acceptance | 4.46 (0.74)a | 4.01 (0.94)ab | 3.98 (0.82)b | 3.83 (0.91)b |
| Anxiety Symptoms | 53.91 (13.40)b | 60.23 (10.42)a | 63.36 (9.67)a | 65.88 (9.39)c |
| Depression Symptoms | 50.43 (9.69)b | 59.56 (10.07)a | 59.75 (9.13)a | 63.81 (9.44)c |
Note. Generational cohort means sharing a subscript are not significantly different from one another.
Regarding the status of milestones, this was measured in two ways: whether experienced or not, and through the gender congruence scale. First, not all questions applied to all participants – for instance, some participants were not living in their affirmed gender or had not affirmed their gender through medical means. As such, sample sizes varied across the milestones in terms of their status (experienced versus not experienced); 680 participants reported the age they first recognized feeling different about their gender (13 had not experienced this milestone), 691 reported the age they recognized a TGD-identity (2 had not experienced this milestone), 642 reported the age they began living part time in their affirmed gender (51 had not experienced this milestone), 468 reported the age they began living full time in their affirmed gender (225 had not experienced this milestone), and 363 reported the age they first had any kind of TGD-related medical care (330 had not experienced this milestone). The number of participants who did not experience the milestones of recognizing feeling different about their gender, recognizing a TGD identity, and living part time in their affirmed gender were relatively small compared to the full sample and therefore these milestones were not included in the next analysis; there was more variation in the status of milestones related to living full time in an affirmed gender and TGD-related medical care. Based on t-tests, we found that participants who had not experienced these latter milestones had higher levels of internalized stigma, gender non-affirmation, and anxiety and depression symptoms, as well as lower appearance congruence compared to participants who reported experiencing these milestones (see Table 5).
Table 5.
T-Tests Regarding Differences between Participants Based on Response Status for Identity Milestones
| Living Full Time in Affirmed Gender |
TGD-Related Medical Care |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Unreported M (SD) |
Reported M (SD) |
t | p | d | Unreported M (SD) |
Reported M (SD) |
t | p | d | |
| Internalized Stigma | 24.19 (8.19) | 20.95 (8.19) | −4.82 | <.001 | .40 | 22.96 (8.26) | 21.11 (8.29) | −2.93 | <.01 | .22 |
| Gender Non-Affirmation | 24.64 (3.78) | 21.63 (6.95) | −7.29 | <.001 | .54 | 24.81 (4.02) | 20.59 (7.20) | −9.54 | <.001 | .72 |
| Appearance Congruence | 1.97 (0.79) | 2.70 (1.05) | 10.13 | <.001 | .79 | 2.10 (0.82) | 2.80 (1.09) | 9.58 | <.001 | .73 |
| Gender Identity Acceptance | 3.75 (0.90) | 4.06 (0.82) | 4.44 | <.001 | .36 | 3.88 (0.87) | 4.03 (0.85) | 2.34 | <.05 | .17 |
| Anxiety Symptoms | 65.40 (9.23) | 62.52 (10.39) | −3.63 | <.001 | .29 | 64.62 (10.41) | 62.38 (9.73) | −2.89 | <.01 | .22 |
| Depression Symptoms | 61.85 (9.50) | 59.89 (9.74) | −2.46 | <.05 | .20 | 61.85 (9.92) | 59.31 (9.34) | −3.43 | <.01 | .26 |
Note. TGD = transgender and gender diverse.
For the subsequent analysis, we assessed status of milestones through a second means via scores on the gender identity acceptance and appearance congruence subscales of the Transgender Identity Congruence Scale. These scores represent outcomes of gender affirmation and were a proxy for milestone status that enabled us to conduct analyses with both the variables of timing of milestones and milestone status. For milestone timing, we calculated z scores to represent the relative timing compared to the full sample, as well as z scores relative to a given participant’s generational cohort. In each regression analysis we entered the z scores to measure milestone timing (separate analyses for the full sample z score and generational cohort z scores), current age, and the Gender Identity Acceptance and Appearance Congruence subscales to assess milestone status. Separate analyses were conducted predicting depression and anxiety symptoms.
This final set of analyses are reported in Table 6. There were a few consistencies across the analyses. First, when controlling for timing of milestones and current age, milestone status was still predictive of depression and anxiety symptoms – especially for the appearance congruence variable, although lower levels identity acceptance were also associated with greater depression and anxiety symptoms in most analyses. Milestone timing relative to the full sample was not a significant predictor of mental health in these models when controlling for the other variables. Furthermore, across most of the models, milestone timing relative to one’s generational cohort was also not a significant predictor of mental health, with one exception. Within one’s generational cohort, participants who started to identify as TGD earlier reported higher levels of depression compared to those who reported later ages of starting to identify as TGD.
Table 6.
Regressions Predicting Depression and Anxiety Symptoms based on Relative Timing of Milestones, Milestone Status, and Current Age
| Variables: | Depression |
Anxiety |
||||||
|---|---|---|---|---|---|---|---|---|
| B | Std. Error B | β | P Value | B | Std. Error B | β | P Value | |
| R2 = .20, F (4, 657) = 39.77, p < .001 | R2 = .15, F (4, 659) = 29.19, p < .001 | |||||||
| Felt Different | −0.52; −0.55 | 0.34; 0.34 | −.05; −.06 | .13; .11 | −0.58; −0.67 | 0.36; 0.36 | −.06; −.07 | .11; .06 |
| Current Age | −0.18 | 0.04 | −.18 | <.001 | −0.29 | 0.04 | −.19 | <.001 |
| Identity Acceptance | −1.04 | 0.41 | −.09 | .01 | −0.54 | 0.43 | −.05 | .21 |
| Appearance Congruence | −3.10 | 0.35 | −.33 | <.001 | −2.71 | 0.37 | −.28 | <.001 |
|
| ||||||||
| R2 = .20, F (4, 667) = 40.36, p < .001 | R2 = .14, F (4, 669) = 27.42, p < .001 | |||||||
| TGD Identity | −0.57; −0.85 | 0.37; 0.34 | −.06; −.09 | .12; .01 | −0.14; −0.35 | 0.40; 0.36 | −.01; −.04 | .74; .34 |
| Current Age | −0.15 | 0.04 | −.15 | <.001 | −0.19 | 0.04 | −.18 | <.001 |
| Identity Acceptance | −0.99 | 0.41 | −.09 | .02 | −0.58 | 0.44 | −.05 | .19 |
| Appearance Congruence | −3.12 | 0.35 | −.33 | <.001 | −2.61 | 0.38 | −.27 | <.001 |
|
| ||||||||
| R2 = .19, F (4, 619) = 36.11, p < .001 | R2 = .14, F (4, 621) = 25.97, p < .001 | |||||||
| Live Part-Time | −0.70; −0.69 | 0.52; 0.36 | −.07; −.07 | .17; .05 | −0.01; −0.24 | 0.55; 0.38 | −.001; −.02 | .99; .53 |
| Current Age | −0.11 | 0.06 | −.11 | .04 | −0.20 | 0.06 | −.19 | .001 |
| Identity Acceptance | −1.02 | 0.42 | −.09 | .02 | −0.42 | 0.44 | −.04 | .34 |
| Appearance Congruence | −3.12 | 0.37 | −.33 | <.001 | −2.68 | 0.39 | −.27 | <.001 |
|
| ||||||||
| R2 = .21, F (4, 451) = 29.94, p < .001 | R2 = .12, F (4, 453) = 14.97, p < .001 | |||||||
| Live Full-Time | −0.08; 0.18 | 0.82; 0.42 | −.01; .02 | .92; .67 | 0.64; 0.37 | 0.93; 0.47 | .06; .04 | .49; .43 |
| Current Age | −0.10 | 0.08 | −.11 | .22 | −0.21 | 0.10 | −.20 | .03 |
| Identity Acceptance | −1.05 | 0.51 | −.09 | .04 | −0.67 | 0.58 | −.05 | .24 |
| Appearance Congruence | −3.59 | 0.41 | −.39 | <.001 | −2.50 | 0.47 | −.25 | <.001 |
|
| ||||||||
| R2 = .21, F (4, 347) = 23.30, p < .001 | R2 = .19, F (4, 349) = 19.78, p < .001 | |||||||
| First TGD Medical Care | −0.88; −0.31 | 1.08; 0.47 | −.10; −.03 | .42; .52 | −0.60; −0.42 | 1.15; 0.50 | −.06; −.04 | .60; .40 |
| Current Age | −0.08 | 0.10 | −.09 | .44 | −0.13 | 0.11 | −.14 | .24 |
| Identity Acceptance | −0.58 | 0.54 | −.05 | .28 | 0.22 | 0.57 | .02 | .70 |
| Appearance Congruence | −3.27 | 0.45 | −.38 | <.001 | −3.16 | 0.47 | −.35 | <.001 |
Note. For milestone timing, all ages were transformed into z scores to represent the relative timing of each experience. The first values in each row for the milestones refers to the estimates using the z score calculated for milestone timing relative to the full sample. The second value in each row for the milestones refers to the estimates using the z scores calculated for milestone timing relative to their respective generational cohorts. For simplicity and since values were very similar, estimates for current age, identity acceptance, and appearance congruence are based on the regression with z scores relative to the full sample instead of repeating this information for regressions based on z scores from within each generational cohort. The only analyses in which significance values for these other variables differed across the regressions were: current age significantly predicted depression scores in the model including generational cohort z scores for living full time in an affirmed gender (B = −0.12, p < .01) and TGD related medical care (B = −0.15, p < .01); and, current age significantly predicted anxiety scores in the model including generational cohort z scores for TGD related medical care (B = −0.17, p < .001).
Discussion
The U.S. has seen many social shifts in terms of rights (e.g., access to employment protections, etc.), visibility (e.g., role models, social media, television), and information about the experiences of TGD people (e.g., the use of the internet and social media platforms to share stories), even though many challenges still exist (e.g., the high rates of murders of TGD women of color, legislation targeting TGD people). In addition, there have been shifts in how TGD people identify and label their genders (Grant et al., 2011; James et al., 2016). As we see in this study, TGD individuals across generational cohorts and gender groups have varying experiences in terms of gender identity milestone timing and status, minority stress and TGD-specific variables, as well as symptoms of depression and anxiety. Overall, these findings indicated the importance of considering the age and generational experiences of TGD people in relation to mental health.
In terms of the generational cohorts, the Boomers+ and Generation X groups were more likely to be trans women compared to other gender groups and the Boomers+ group reported older ages for reaching the identity milestones compared to the other generational cohorts. Although we cannot be certain the reason for this, these findings are similar to other studies and it could be that this reflects some of the social shifts that have occurred in regards to visibility of TGD individuals and the increased recognition of a variety of TGD identities (Grant et al., 2011; James et al., 2016). Like Wilkinson and colleagues (2018), we also found that younger generational cohorts reported shorter gaps between the identity milestones compared to the older groups. This may reflect that younger TGD people are living in a time when they are able to come out and live in their affirmed gender at younger ages compared to the older generations.
Although younger generational cohorts may be having positive experiences in the sense that they are reporting younger ages for milestones, we also found that the younger generational cohorts had more negative experiences on the other study variables. Younger generational cohorts reported higher levels of internalized stigma, depression, and anxiety compared to the older generational cohorts, which may reflect changes in self-acceptance and mental health. Findings regarding age and mental health mirror what is known more broadly, with younger adults having higher prevalence of major depressive episodes for example than older adults in the general population (e.g., Center for Behavioral Health Statistics and Quality, 2018). It may be that these younger generational cohorts are facing more challenges related to stigmatization given that they are coming out and affirming their gender at younger ages. Other research has shown that younger TGD people report higher levels of felt stigma (Bockting et al., 2013) and internalized stigma (Bariola et al., 2015) compared to older TGD people. Other research also has shown that there are a variety of positive aspects to being TGD (Riggle, Rostosky, McCants, & Pascale-Hague, 2011) and it could be that, at older ages, TGD people are drawing more on these positive experiences. In addition, younger TGD people may be more embedded within their family of origin or other networks that may be rejecting and have less agency for navigating these systems compared to older generational cohorts. Overall, we may have been observing either generational differences or normative developmental processes whereby with age TGD people report less mental health symptoms and minority stressors, or it could be that both are occurring.
In terms of mental health and generational cohorts, only the Boomers+ group reported depression symptoms that were similar to national averages for depression symptoms in the PROMIS measure’s original sample (Cella et al., 2011). All generations younger than the Boomers+ reported depression levels that were close to or above a standard deviation higher than the national averages. These findings may indicate that depression decreases over time for TGD people, but that this is a slow decline to reach levels typical of the general population. As such, it is likely that TGD people are being emotionally taxed by symptoms of depression and anxiety for large portions of their lifetimes, due to minority stress as other research has shown (e.g., Testa et al., 2015). However, it also is possible that changes in depression also differ across generational cohorts. For instance, Nuttbrock and colleagues (2010) found that depression peaked in adolescence for TGD people, but declines in depression are also likely more steep for younger generations. As such, the changes in mental health when the Millennials or Generation Z participants reach older ages may look different than the participants who were in the Boomers+ and Generation X cohorts, although only longitudinal research can answer this type of question. It also is essential to understand that these mental health symptoms are driven by minority stress experiences, such as gender-related discrimination, harassment, and victimization (e.g., Bariola et al., 2015; Bradford et al., 2013; D’Augelli et al., 2006). Thus, efforts to improve the social climate for TGD people are critical to reducing minority stress and stigma, which would ultimately improve the mental health of TGD communities.
As has been found in prior research, gender identity affirmation was associated with better mental health outcomes (Olson et al., 2016; Testa et al., 2014; Rotondi et al., 2011). In this study, milestone status – specifically experiencing the milestones of living fully in an affirmed gender and receiving gender affirming medical care – was associated with more positive outcomes compared to not experiencing these milestones. These positive outcomes included lower internalized stigma, lower gender non-affirmation, higher levels of gender identity acceptance, higher appearance congruence, and lower anxiety and depression. These findings highlight the importance of increasing access to these milestones and creating social contexts in which TGD people can affirm their gender. Even so, it also is important to note that this study was cross-sectional and we cannot be sure whether these milestones facilitate more positive outcomes or if the opposite is true. For example, it is possible that individuals with less internalized stigma and more acceptance of their gender may be more likely to pursue living fully in their affirmed gender or gender affirming medical care.
Finally, although some interesting findings emerged regarding average timing of milestones, generational cohorts, and the intersections of these variables, these must be considered in light of the findings in the final analyses. Models that accounted for both milestone timing and milestone status, while controlling for current age, revealed that the strongest predictor of depression and anxiety was appearance congruence and the status of the milestones. These findings suggest that regardless of when these milestones occur, the experience of embracing a TGD identity, living in an affirmed gender, and having gender affirming medical care are associated with positive mental health outcomes. This finding should not be taken to indicate that age is irrelevant – we know from other research that being supported in one’s gender experience early on is incredibly important to development and mental health (e.g., Olson et al., 2016). Instead, these findings indicate that shifts in appearance and personal acceptance of one’s self that can happen at any age can be predictive of mental health. This finding may be especially pertinent to some TGD people who do not experience earlier milestone timing or the life circumstances that facilitate earlier acknowledgement of a TGD identity or the other milestones.
Although this study fills a gap in the literature related to the timing of milestones across gender and generational cohorts and associations with mental health, there were also limitations to this study. This study was conducted online and thus may reflect individuals who are more likely to use or have access to the internet. The internet has served as a resource for many TGD people seeking information about transgender experiences and thus these participants may be more likely to report the milestones we examined compared to TGD individuals who do not use or have access to the internet. Similarly, our research study called for participants who identified as TGD and individuals who are earlier on in their identity development or not as tied to their gender identity may be less likely to be represented in this sample. In addition, given the cross-sectional nature of this data, conclusions should be made with caution about differences between the generational cohorts. It is possible that the average ages of the younger cohorts would increase as more people go through milestones at later ages, but these experiences are not captured in the current data. For example, Generation Z could only have been, at most, 20 years old at the time of the study, meaning that their average ages could not go beyond this as a function of the study being cross-sectional.
Although we had a variety of recruitment methods, it also is possible that recruitment through online sources resulted in many more Millennials and Generation Z participants than the other generational groups. Researchers using other recruitment methods may find different patterns of identity milestones, especially among the older generations. There also are other milestones that may be essential to measure in future research in these areas, such as identity disclosure (Restar et al., 2019). In addition, our sample was primarily white, and these milestones may vary across racial groups (Restar et al., 2019). Due to small sample size of participants of color in this study, we were not able to explore racial differences. These sampling limitations speak to the importance of future research utilizing representative samples. It also is difficult to disentangle the effects of current age in the analyses we conducted although we used some methods to address this (such as z scores and relative milestone timing). Our study was inherently limited in that mental health variables reflected current mental health instead of a closer approximation to what the mental health experiences may have been like for participants when going through each of the milestones. Future longitudinal research needs to address whether differences in mental health outcomes may be due to other factors, such as the amount of time TGD people delay milestones, the length of time between milestones, or when an individual experienced a milestone relative to the measurement of mental health symptoms. Such longitudinal research would also help to address the limitation of the inherent conflation of current age and average age within each generational cohort.
Conclusion
TGD individuals vary in their experience of identity milestone timing and status, with older generations reporting later timing of these milestones. Furthermore, status of milestones was also important, with experiencing these milestones being associated with less internalized stigma, less non-affirmation, more appearance congruence, and fewer symptoms of anxiety and depression compared to individuals who did not report these milestones. It is possible that these hardships, such as internalized stigma, decrease over time (as has been found in sexual minorities; Puckett et al., 2018b), but time alone cannot be the answer to managing marginalization.
Our findings also indicate that the status of milestones may be related to mental health. As such, improving access to supports and resources could alleviate some of the minority stress TGD people experience and will enable TGD people to have more positive, affirming experiences related to their gender identity. At the same time, even with social shifts, younger generations appear to be facing additional hardships compared to the older generations. Future research is needed to help explain why generational cohorts show differences in exposure to minority stress and mental health. This knowledge may potentially reveal how older TGD generations develop resilience over time.
Public Health Significance:
Challenges for gender minorities vary across generational context; younger generational cohorts of transgender individuals experienced greater challenges in relation to minority stressors and mental health, whereas older generational cohorts experienced gender identity milestones at later ages. Milestone status is especially important for more positive mental health outcomes for transgender individuals.
Acknowledgements
Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number F32DA038557. We thank the members of the Trans Health Community Advisory Board who assisted with this project for their time, feedback, and dedicated involvement. We also would like to thank the participants who took part in this research for their time and effort.
Contributor Information
Jae A. Puckett, Department of Psychology, Michigan State University, 316 Physics Rd., Rm 262, East Lansing, MI 48824.
Samantha Tornello, Human Development & Family Studies, Pennsylvania State University, 215 Health & Human Development Building, State College, PA 16801.
Brian Mustanski, Northwestern University Feinberg School of Medicine, Department of Medical Social Sciences, Institute for Sexual and Gender Minority Health and Wellbeing, 625 N Michigan Ave, Suite 1400, Chicago, IL 60657.
Michael E. Newcomb, Department of Medical Social Sciences, Northwestern University, Feinberg School of Medicine, Institute for Sexual and Gender Minority Health and Wellbeing, 625 N Michigan Ave, Suite 1400, Chicago, IL 60611.
References
- Austin A (2016). “There I am”: A grounded theory study of young adults navigating a transgender or gender nonconforming identity within a context of oppression and invisibility. Sex Roles, 75(5–6), 215–230. [Google Scholar]
- Bariola E, Lyons A, Leonard W, Pitts M, Badcock P, & Couch M (2015). Demographic and psychosocial factors associated with psychological distress and resilience among transgender individuals. American Journal of Public Health, 105(10), 2108–2116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barsigian LL, Hammack PL, Morrow QJ, Wilson BDM, & Russell ST (2020). Narratives of gender, sexuality, and community in three generations of genderqueer sexual minorities. Psychology of Sexual Orientation and Gender Diversity. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bockting WO, Miner MH, Swinburne Romine RE, Hamilton A, & Coleman E (2013). Stigma, mental health, and resilience in an online sample of the U.S. transgender population. American Journal of Public Health, 103(5), 943–951. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradford J, Reisner LS, Honnold AJ, & Xavier J (2013). Experiences of transgender-related discrimination and implications for health: results from the Virginia transgender health initiative study. American Journal of Public Health, 103(10), 1820–1829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cai X, Hughto JMW, Reisner SL, Pachankis JE, & Levy BR (2019). Benefit of gender-affirming medical treatment for transgender elders: Later-life alignment of mind and body. LGBT Health, 6, 34–39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cella D, Riley W, Stone A, Rothrock N, Reeve B, Yount S, … Hays R (2011). Initial adult health item banks and first wave testing of the Patient-Reported Outcomes Measurement Information System (PROMIS) Network: 2005–2008. Journal of Clinical Epidemiology, 63, 1179–1194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D’Augelli RA, Grossman HA, & Starks TM (2006). Childhood gender atypicality, victimization, and PTSD among lesbian, gay, and bisexual youth. Journal of Interpersonal Violence, 21(11), 1462–1482. [DOI] [PubMed] [Google Scholar]
- Dentice D, & Dietert M (2015). Liminal spaces and the transgender experience. Theory in Action, 8(2), 69–96. [Google Scholar]
- Dimock M (2019). Defining generations: Where millennials and generation Z begins. Pew Research Center. Retrieved from: https://www.pewresearch.org/fact-tank/2019/01/17/where-millennials-end-and-generation-z-begins/
- Fagot MD, & Leinbach RH (1986). Gender labeling and the adoption of sex-typed behaviors. Developmental Psychology, 22, 440–443. [Google Scholar]
- Fast AA, & Olson KR (2017). Gender development in preschool transgender children. Child Development, 89(2), 620–637. [DOI] [PubMed] [Google Scholar]
- Fontanari AMV, Vilanova F, Schneider MA, Chinazzo I, Soll BM, Schwarz K, ... & Costa AB (2020). Gender affirmation is associated with transgender and gender nonbinary youth mental health improvement. LGBT Health, 7(5), 237–247. [DOI] [PubMed] [Google Scholar]
- Fredriksen-Goldsen KI, Simoni JK, Kim H, Lehavot K, Walters KL, Yang J, Hoy-Ellis CP, & Muraco A (2014). The Health Equity Promotion Model: Reconceptualization of lesbian, gay, bisexual, and transgender (LGBT) health disparities. American Journal of Orthopsychiatry, 84, 653–663. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gagné P, Tewksbury R, & McGaughey D (1997). Coming out and crossing over: Identity formation and proclamation in a transgender community. Gender & Society, 11(4), 478–508. [Google Scholar]
- Galupo MP, Pulice-Farrow L, & Lindley L (2019). “Every time I get gendered male, I feel a pain in my chest”: Understanding the social context for gender dysphoria. Stigma and Health, 5(2), 199–208. [Google Scholar]
- Ge X, Conger RD, & Elder GH (2001). Pubertal transition, stressful life events, and the emergence of gender differences in adolescent depressive symptoms. Developmental Psychology, 37(3), 404–417. [DOI] [PubMed] [Google Scholar]
- Gower LA, Rider GN, Coleman E, Brown C, McMorris JB, & Eisenberg EM (2018). Perceived gender presentation among transgender and gender diverse youth: Approaches to analysis and associations with bullying victimization and emotional distress. LGBT Health, 5(5), 312–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant MJ, Mottet AL, & Tanis J (2011). Injustice at every turn: A Report of the national transgender discrimination survey. Washington: National Center for Transgender Equality and National Gay and Lesbian Task Force. [Google Scholar]
- Grossman AH, D’augelli AR, & Salter NP (2006). Male-to-female transgender youth: Gender expression milestones, gender atypicality, victimization, and parents’ responses. Journal of GLBT Family Studies, 2(1), 71–92. [Google Scholar]
- Gülgöz S, Glazier JJ, Enright EA, Alonso DJ, Durwood LJ, Fast AA, … & Olson KR (2019). Similarity in transgender and cisgender children’s gender development. Proceedings of the National Academy of Sciences, 116(49), 24480–24485. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Huddleston J, & Ge X (2003). Boys at puberty: Psychosocial implications. In Hayward Chris (Ed.), Gender differences at puberty (113–134). Cambridge University Press. [Google Scholar]
- Jackman KB, Dolezal C, & Bockting WO (2018). Generational differences in internalized transnegativity and psychological distress among feminine spectrum transgender people. LGBT health, 5(1), 54–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- James SE, Herman JL, Rankin S, Keisling M, Mottet L, & Anafi M (2016). The report of the 2015 U.S. transgender survey. Washington, DC: National Center for Transgender Equality. [Google Scholar]
- Kenagy PG (2005). Transgender health: Findings from two needs assessment studies in Philadelphia. Health & Social Work, 3(1), 19–26. [DOI] [PubMed] [Google Scholar]
- Kozee HB, Tylka TL, & Bauerband LA (2012). Measuring transgender individuals’ comfort with gender identity and appearance: Development and validation of the Transgender Congruence Scale. Psychology of Women Quarterly, 36(2), 179–196. [Google Scholar]
- Mallon PG, & DeCrescenzo T (2006). Transgender children and youth: A child welfare practice perspective. Child Welfare League of America, 85(2), 215–241. [PubMed] [Google Scholar]
- Nguyen HB, Chavez AM, Lipner E, Hantsoo L, Kornfield SL, Davies RD, & Epperson CN (2018). Gender-affirming hormone use in transgender individuals: impact on behavioral health and cognition. Current Psychiatry Reports, 20(12), 110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nuttbrock L, Hwahng S, Bockting W, Rosenblum A, Mason M, Macri M, & Becker J (2010). Psychiatric impact of gender-related abuse across the life course of male-to-female transgender persons. Journal of Sex Research, 47(1), 12–23. [DOI] [PubMed] [Google Scholar]
- Olson RK, Durwood L, DeMeules M, & McLaughlin AK (2016). Mental health of transgender children who are supported in their identities. American Academy of Pediatrics, 137(3), 2015–3223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olson KR, Key AC, & Eaton NR (2015). Gender cognition in transgender children. Psychological Science, 26, 467–474. [DOI] [PubMed] [Google Scholar]
- Pleak RR (2009). Formation of transgender identities in adolescence. Journal of Gay & Lesbian Mental Health, 13(1), 282–291. [Google Scholar]
- Puckett JA, Cleary P, Rossman K, Mustanski B, & Newcomb M (2018a). Barriers to gender-affirming care for transgender and gender nonconforming individuals. Sexuality Research and Social Policy, 15, 48–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puckett JA, Feinstein BA, Newcomb ME, & Mustanski B (2018b). Trajectories of internalized heterosexism among young men who have sex with men. Journal of Youth and Adolescence, 47(4), 872–889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Puckett JA, Maroney MR, Wadsworth LP, Mustanski B, & Newcomb ME (2020). Coping with discrimination: The insidious effects of gender minority stigma on depression and anxiety in transgender individuals. Journal of Clinical Psychology, 76, 176–194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Restar A Jin H Breslow SA, Surace A, Gruszka N, Kuhns L, Reisner LS, Garofalo R, & Mimiaga JM (2019). Developmental milestones in young transgender women in two American cities: Results from a racially and ethnically diverse sample. Transgender Health, 4(1), 162–167. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riggle DBE, Rostosky SS, McCants EL, & Pascale-Hague D (2011). The positive aspects of a transgender self-identification. Psychology & Sexuality, 2(2), 147–158. [Google Scholar]
- Rotondi KN, Bauer RG, Travers R, Scanlon K, & Kaay M (2011). Depression in male-to-female transgender Ontarians: Results from the Trans Pulse Project. Canadian Journal of Community Mental Health, 30(2), 113–133. [Google Scholar]
- Saltzburg S, & Davis TS (2010) Co-Authoring gender-queer youth identities: Discursive tellings and retellings. Journal of Ethnic & Cultural Diversity in Social Work, 19(2), 87–108. [Google Scholar]
- Seelman KL, Colón-Diaz MJ, LeCroix RH, Xavier-Brier M, & Kattari L (2017). Transgender noninclusive healthcare and delaying care because of fear: connections to general health and mental health among transgender adults. Transgender health, 2(1), 17–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shuster MA, Reisner SL, & Onorato SE (2016). Bayond bathrooms – meeting the health needs of transgender people. The New England Journal of Medicine, 375, 101–103. [DOI] [PubMed] [Google Scholar]
- Tatum AK, Catalpa J, Bradford NJ, Kovic A, & Berg DR (2020, March 5). Examining Identity development and transition differences among binary transgender and Genderqueer nonbinary (GQNB) Individuals. Psychology of Sexual Orientation and Gender Diversity. Advance online publication. [Google Scholar]
- Testa RJ, Habarth J, Peta J, Balsam K, & Bockting W (2015). Development of the Gender Minority Stress and Resilience Measure. Psychology of Sexual Orientation and Gender Diversity, 2(1), 65–77. [Google Scholar]
- Testa JR, Jimenez LC, & Rankin S (2014). Risk and resilience during transgender identity development: The effects of awareness and engagement with other transgender people on affect. Journal of Gay & Lesbian Mental Health, 18(1), 31–46. [Google Scholar]
- Tomita KK, Testa RJ, & Balsam KF (2019). Gender-affirming medical interventions and mental health in transgender adults. Psychology of Sexual Orientation and Gender Diversity, 6(2), 182–193. [Google Scholar]
- Toomey BR, Ryan C, Diaz MR, Card AN, & Russel TS (2013). Gender-nonconforming lesbian, gay, bisexual, and transgender youth: school victimization and young adult psychosocial adjustment. Psychology of Sexual Orientation and Gender Diversity, 1(S), 71–80. [DOI] [PubMed] [Google Scholar]
- White Hughto JM, & Reisner SL (2016). A systematic review of the effects of hormone therapy on psychological functioning and quality of life in transgender individuals. Transgender Health, 1(1), 21–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilkinson L, Pearson J, & Liu H (2018). Educational attainment of transgender adults: Does the timing of transgender identity milestones matter? Social Science Research, 74, 146– 160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Williams ME, & Freeman PA (2007). Transgender health: Implications for aging and caregiving. Journal of Gay & Lesbian Social Services, 18, 93–108. [Google Scholar]
- Wilson EC, Chen YH, Arayasirikul S, Wenzel C, & Raymond HF (2015). Connecting the dots: Examining transgender women’s utilization of transition-related medical care and associations with mental health, substance use, and HIV. Journal of Urban Health, 92(1), 182–192. [DOI] [PMC free article] [PubMed] [Google Scholar]