

Abstract
There is convincing evidence that trauma-related psychological distress and aggressive behavior are highly related among adolescents. The evidence is less clear regarding the direction of this relation. Objective: The purpose of this study was to examine reciprocal longitudinal relations between trauma-related distress and physical aggression. Method: A predominantly African American sample of early adolescents (N = 2,271; mean age = 12.9) living in an urban, under-resourced community participated in this investigation. The current study used autoregressive cross-lagged models to examine changes across four waves of data within each grade of middle school. Results: Support was found for trauma-related distress uniquely predicting increased levels of physical aggression. This effect was consistent across gender and within and across middle school grades. Conversely, physical aggression did not predict changes in trauma-related distress. Conclusions: Violence prevention efforts should routinely screen for trauma-related distress.
Keywords: trauma-related psychological distress, physical aggression, early adolescence, gender differences, seasons
A consistent finding in the literature is that experiencing stressful life events predicts increased emotional and behavioral problems overtime (e.g., Grant et al., 2003; Liu, Bolland, Dick, Mustanski, & Kertes, 2016). Indeed, exposure to traumatic and stressful life events during childhood has been linked to cognitive impairments, poorer academic performance, trauma-related psychological distress, lower self-esteem, and increased office disciplinary referrals in schools (for a review, see Perfect, Turley, Carlson, Yohanna, & Saint Gilles, 2016). As such, developmental researchers have increasingly advocated for the use of a more holistic approach to understanding psychopathology by examining how internalizing and externalizing symptoms co-occur (Eaton, Rodriguez-Seijas, Carragher, & Krueger, 2015; van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005). Although researchers have found an association between trauma-related distress (e.g., re-experiencing traumatic events, avoiding places and people, hypervigilance) and aggression among early adolescents (e.g., Aebi et al., 2017; Wolfe, Wekerle, Scott, Straatman, & Grasley, 2004), most prior studies have used cross-sectional designs. It thus remains unclear whether trauma-related distress increases risk for physical aggression, physical aggression increases risk for experiencing trauma-related distress, or whether both are related to other factors.
Moreover, multiple theories have posited the importance of examining comorbid psychopathology among urban youth living in violent neighborhood. According to the stress process (Foster & Brooks-Gunn, 2009) and cultural ecological models (Garcia Coll et al., 1996), youth living in impoverished areas are more likely to accumulate stressors that affect their overall development. For example, structural factors, such as living in a neighborhood with concentrated disadvantage and lack of youth services, have been shown to account for over a third of the difference in exposure to community violence between African American and White youth (Zimmerman & Messner, 2013). Unfortunately, the examination of how trauma-related distress and externalizing behaviors are interrelated among adolescents living in urban, under-resourced communities is a largely understudied endeavor (for an exception, see Liu et al., 2016). The purpose of the current study was to test bidirectional relations between trauma-related distress and physical aggression among a predominantly African American sample of early adolescents living in under-resourced communities exposed to high violence rates. In particular, we examined changes across multiple waves within each grade of middle school, which represents an important developmental period for the initiation of problem behaviors.
Examining the relation between trauma-related distress and aggressive behavior is particularly salient among urban, minority youth. African American adolescents are significantly more likely to be violently victimized and exposed to community violence than are White youth (Zimmerman & Messner, 2013), particularly among children and adolescents from under-resourced communities (Turner, Finkelhor, & Ormrod, 2006). The increased use of intersectional approaches to examine the effects of multiple dimensions simultaneously (e.g., race, gender, neighborhood disadvantage) has highlighted the unique experiences of minority youth living in highly violent, under-resourced communities (Baskin-Sommers et al., 2017).
Carter (2007) has proposed a race-based traumatic stress injury model arguing that trauma is experienced differently across racial and ethnic groups. This is supported by emerging research that has found racism to be linked to trauma-related distress among adolescents of color, and that both racist experiences and trauma-related symptoms are associated with problem behaviors among adolescents of color (Kang & Burton, 2014). Researchers have also found that disparities in school disciplinary referrals and contact with the juvenile justice system between minority and non-minority youth cannot be explained by differences in problem behaviors alone (Bradshaw, Mitchell, O’Brennan, & Leaf, 2010). These disparities may be better explained by cumulative stressors, such as poverty and exposure to community violence, and subsequent trauma-related distress. For example, incarcerated youth are at a significantly higher risk of reporting psychological distress than community youth (see Kerig & Becker, 2012 for a review). These unique experiences highlight the importance of using longitudinal analyses to clarify the association between trauma-related distress and problem behaviors within urban under-resourced communities.
Although a clinical diagnosis of post-traumatic stress disorder (PTSD) requires meeting specific criteria listed in the Diagnostic and Statistical Manual of the American Psychiatric Association (American Psychiatric Association, 2013), children and adolescents who have experienced a traumatic event often exhibit a range of symptomatology. Studies examining symptoms associated with PTSD have consistently found significant psychological and behavioral impairment among traumatized individuals who do not meet full criteria for PTSD (for a review, see Brancu et al., 2016). Within the current article, we define trauma-related distress as a continuous measure of internalizing symptoms that are often associated with a traumatic event. Symptoms include hyperarousal, negative mood, re-experiencing of a traumatic event, and avoidance of places or experiences related to a distressing event.
Relations Between Trauma-Related Distress and Physical Aggression
The association between trauma-related distress and various forms of aggression is supported by numerous cross-sectional studies (e.g., Abate, Marshall, Sharp, & Venta, 2017; Aebi et al., 2017; Marsee, 2008). Two longitudinal studies found that trauma-related distress mediated the relation between traumatic experiences and externalizing behaviors, including dating violence (Wolf et al., 2004) and symptoms of conduct disorder, oppositional defiant disorder, and attention deficit/hyperactivity disorder (Cromer & Villodas, 2017). These studies provide further evidence of the impact of trauma-related distress on later externalizing symptoms. Neither study, however, investigated the relation between externalizing behavior and subsequent frequencies of trauma-related distress. In other words, the authors did not explore whether there was a bidirectional relation between trauma-related distress and aggression.
There is some evidence to suggest that aggressive behavior among adolescents increases the likelihood of later exposure to traumatic events (e.g., Farrell, Mehari, Kramer-Kuhn, & Goncy, 2014; Gvirsman et al., 2014). For example, in a longitudinal study of a diverse sample of sixth graders, Farrell and colleagues (2014) found evidence of bidirectional effects between witnessing violence and physical aggression. Given the close link between trauma exposure and trauma-related distress (e.g., Alisic et al., 2014), their research suggests that initial levels of aggression could put adolescents at an increased risk for the development of distress through their exposure to violence. Van der Molen and colleagues (2015) provided further clarification of the link between aggressive behavior and later trauma-related distress, based on nine waves of data from the Pittsburgh Girls Study. They found that early onset of disruptive behavior during childhood was associated with adjustment problems in early adolescence, including trauma-related distress. Their study provides a clear link between early aggressive behavior and later trauma-related distress, underscoring the need to test the bidirectionality of this relation simultaneously.
The possibility of bidirectional relations between trauma-related distress and aggression is supported by theoretical and empirical work indicating a cyclical relation between violence and victimization (Merlo & Benekos, 2016). A trauma-informed social information processing model (Taft, Murphy, & Creech, 2016) posits that trauma shifts the way an individual uses social information to respond to others, including inadequate decoding of relevant social cues, hostile attribution biases, decision-making, and self-monitoring. This can lead to a tendency to misinterpret social situations and respond aggressively. This is supported by studies that have found that these maladaptive social-cognitive patterns mediate the relation between PTSD and aggression (Abate et al., 2017). Engagement in aggressive behavior could thus lead to further victimization that, in turn, increases one’s risk for trauma-related distress. However, the literature has yet to provide clear evidence for bidirectional relations between trauma-related distress and aggressive behavior among early adolescents.
Examining Change During Early Adolescence
Early adolescence is a particularly salient time to study the relation between trauma-related distress and aggression. Early adolescence is a time of rapid developmental change (Wigfield, Byrnes, & Eccles, 2006). The transition from elementary to middle school creates new social contexts and increases in autonomy that put adolescents at an increased risk for victimization and aggression (Akers, 1998; Wigfield et al., 2006). Seasonal factors, such as the transition back to school that occurs at the start of each school year, changes within peer groups throughout the school year, the potential for greater unsupervised time during the summer months, or conversely, the lack of transportation to see friends during school breaks, all have the potential to influence adolescents’ levels of risk for psychological distress and physical aggression.
Most school-based longitudinal studies collect at most two waves of data within the same school year, typically near beginning and end of the school year. It is thus unclear how trauma-related distress and physical aggression are related during other times of the year. Results of studies examining changes in adolescents’ frequency of aggression during middle school have been mixed (e.g., Farrell, Goncy, Sullivan, & Thompson, 2018; Romero, Richards, Harrison, Garbarino, & Mozley, 2015). Even less is known about changes in trauma-related distress across middle school, although there is some research to suggest that these symptoms may decrease as exposure to violence reaches critically high levels due to emotional desensitization (Mrug, Madan, & Windle, 2016).
It is also unclear whether gender moderates the association between trauma-related distress and physical aggression during early adolescence. Girls have been shown to be at a higher risk for developing trauma-related distress (Alisic et al., 2014), whereas prior research indicates that boys are at a higher risk for engaging in physically aggressive behavior (for a review, see Card, Stucky, Sawalani, & Little, 2008), although the latter finding has been less consistent across studies (e.g., Bettencourt & Farrell, 2013; Bradshaw, Schaeffer, Petras, & Ialongo, 2010). There is some evidence to suggest that trauma-related distress mediates the relation between exposure to traumatic events and aggressive behavior equally across boys and girls (Wolfe et al., 2004). However, a cross-sectional study found evidence of a stronger relation between PTSD and aggression among boys than among girls (Aebi et al., 2017).
Present Study/Hypotheses
The purpose of this study was to examine bidirectional longitudinal relations between trauma-related distress and physical aggression within a predominately African American sample of early adolescents living in under-resourced communities with high rates of poverty and crime. We conducted cross-lagged path analyses examining change across three-month intervals from the fall to summer within the school year. We hypothesized: (1) bidirectional positive relations between trauma-related distress and physical aggression across all waves; (2) that the relations would be stronger during the sixth grade compared with the seventh and eighth grade, given past research indicating emotional desensitization over time; and (3) that the relations would be more strongly associated across the fall to winter (i.e., Wave 1 to Wave 2) compared with other time points, given the period of transition to a new grade. We also conducted exploratory analyses to determine the extent to which these relations differed by gender.
Method
Participants and Procedures
We conducted secondary analyses of data collected four times per year (i.e., every 3 months) for seven years between 2010 and 2017 as part of a study (Author reference) to evaluate the Olweus Bullying Prevention Program (Olweus & Limber, 2010). The evaluation study was conducted in three schools that were selected based on attendance zones in neighborhoods with high rates of violence-related crimes. The majority of students at these schools (i.e., 74% to 85%) came from low-income families based on their eligibility for the federal free lunch program. The intervention study used a multiple-baseline design in which the investigators randomly determined the timing of initiating intervention activities in each school. The randomization process involved having the school principals draw from a shuffled deck of playing cards. The principal drawing the highest card had the intervention start at their school in fall of 2011; the principal drawing the next highest card had it started at their school in fall of 2012, and the intervention was initiated at the remaining school in fall of 2015. Once initiated, intervention activities continued in each school until the end of the project (see Author reference for details).
Recruitment of participants for the evaluation study proceeded as follows. During the first year of the study, the researchers obtained rosters of all sixth, seventh, and eighth grade students enrolled at each school (total N = 419 to 574 per school). They then used a random numbers generator within a database to randomly sample approximately 91 eligible students per grade within each school. They considered students eligible if they spoke English, were in fact attending the school, and were not in self-contained classrooms. The researchers obtained active parental consent and student assent from 669 students (81% of those eligible). This included 217 to 228 per grade and 219 to 225 per school. Participants completed assessments each year until they left middle school or chose to discontinue participation. Participants completed measures using a computer-assisted self-administered interview generally in small groups in the schools during the school year and individually in their homes during the summer. Participants were compensated with a $10 gift card at each wave. For each of the next six years the researchers used this same procedure to recruit, consent, and assess a new cohort of sixth graders, and seventh and eighth graders to replace those who left the schools or study. This provided a total sample of 2,271 participants, which represented 80% of all eligible students who were randomly selected from the class rosters.
The project used a planned missingness design wherein each participant was randomly assigned to participate at two of the four waves (i.e., October, January, April, and July) each year. This strategy was used to reduce participant fatigue and testing effects while still providing a large overall sample with sufficient coverage to examine changes across all waves (see Little & Rhemtulla, 2013). This resulted in data that were missing completely at random, which can be addressed by current methods of data analysis. Practical constraints prevented the collection of a fall wave of data during two of the seven years of the project. This occurred in Year 1 because funding for the project was not received until after the school year had started, and in Year 6 because participants had to be re-consented when the source of funding for the project changed.
We conducted analyses for the present study on a de-identified dataset in which all data obtained for each participant were linked across waves using a number that could not be linked to his or her name. Although many students participated across several grades, four of the nine cohorts were not in the study for all three grades (i.e., were recruited in the seventh or eighth grade, or were in the sixth or seventh grade in the last year of data collection), and some students in other cohorts were recruited in the seventh or eighth grades. Rather than attempt to model individual-level change across all three grades, we chose to use the data from all 2,271 participants to examine changes within each grade as a within-person factor, and differences across grades as a between-persons (i.e., group) factor. For students who participated during more than one grade, we randomly selected data from one of the grades for inclusion in the study to avoid confounding between-person and within-person effects in the cross-grade comparisons. We conducted all analyses on the resulting longitudinal dataset, which included all waves from a single one grade for each of the 2,271 participants for whom active parental consent and student assent were obtained. This included data from most (i.e., 89.8%) of the waves to which these students were assigned. Challenges locating participants during the summers between school years resulted in a lower participation rate at the summer wave (i.e., 74.1%). Prior to analyses, we screened out a small percentage of the surveys because they were too incomplete (0.2%), or because it seemed likely that the student was randomly responding based on either an unreasonably short completion time (0.3%) or staff observations of student behavior suggesting they were randomly responding (0.9%). The number of participants at each wave was 989 for the fall wave, 1,130 for the winter wave, 1,074 for the spring wave, and 868 for the summer wave. This reflects the planned missingness whereby half the sample was assigned to each wave and the lower rate of participation in the summer.
The sample in the final dataset had approximately equal representation across grades (N = 761, 758, and 752 across grades 6, 7, and 8, respectively). The final sample ranged in age from 11 to 16 years old. The mean age at the fall wave was 11.3 (SD = 0.54) for sixth graders, 12.3 (SD = .60) for seventh graders, and 13.3 (SD = 0.57) for eighth graders. Slightly more than half of participants (51%) identified their gender as female. The majority of youth who disclosed their race identified themselves as Black or African American (89%) as either the sole category (78%) or as one of multiple categories (11%). Of the remainder, 5% identified themselves as White, 1% as Native American or Alaska Native, with less than 2% in all remaining categories. Overall, 16% identified their ethnicity as Hispanic or Latino. The majority of participants (66%) completed measures while at a school that was implementing the intervention. The study was approved by the IRB of the authors’ university.
Measures
Physical Aggression.
The frequency of engaging in physical aggression was assessed by the Problem Behavior Frequency Scale – Adolescent Report (PBFS-AR; Farrell, Sullivan, Goncy, & Le, 2016). Physical aggression toward others was measured using five items (e.g., “hit or slapped someone,” “threatened someone with a weapon [gun, knife, club, etc.]). Respondents rated how frequently they engaged in physical aggression in the past 30 days using a 6-point anchored scale (i.e., 1 = Never, 2 = 1–2 times, 3 = 3–5 times, 4 = 6–9 times, 5 = 10–19 times, and 6 = 20 or more times). Farrell et al. (2016) found support for strong measurement invariance across gender, location, and time, as well as support for construct validity of the PBFS-AR using measures of related constructs based on teacher- and student-report. We calculated the total score by combining the three highest categories based on prior IRT analyses (Author reference), and calculating the mean across items. Alpha coefficients ranged from .76 to .82 across waves.
Trauma-Related Distress.
The Checklist of Children’s Distress Symptoms (CCDS; Richters & Martinez, 1993) was designed to assess the type and frequency of symptoms experienced by youth who live with long-term exposure to community violence. The CCDS is a 28-item measure based on diagnostic criteria for PTSD described in the Diagnostic and Statistical Manual of Mental Disorders, third edition (DSM-III-R) (APA, 1987). The CCDS does not allow for clinical diagnoses of PTSD, as it does not identify the precipitating traumatic event. However, it does provide an index of post-traumatic psychological distress symptoms (Mash & Barkley, 2007). Items represent clusters of trauma-related distress symptoms including hyperarousal (e.g., “How often do you watch things around you real closely in order to protect yourself from something bad happening?”), re-experiencing the event (e.g., How often do you feel like something bad or frightening from the past is happening all over again?”), and avoidance (e.g., “How often do you avoid or try not to go to places or do things that remind you of something bad that happened?”). Responses are rated on a 5-point scale (i.e., 1 = Never, 2 = Seldom, 3 = Once in a while, 4 = A lot of the time, and 5 = Most of the time). Children’s composite symptom scores on the CCDS have been significantly related to exposure to trauma (Overstreet & Braun, 2000) and violence (Mathews, Dempsey, & Overstreet, 2009). As recommended by Mash and Barkley (2007), we used the total CCDS score as in previous studies (e.g., Mathews, Dempsey, & Overstreet, 2009), such that higher scores corresponded to more adverse trauma-related distress.
Data Analyses
We log transformed scores on the measure of adolescent physical aggression to reduce their skewness and kurtosis, and used linear transformations to provide scores with similar means and standard deviation as the original scores. We conducted analyses for each model using all data available for each participant. We addressed missing data using used full information maximum likelihood estimation (FIML). This approach is preferred over alternatives such as listwise and pairwise deletion, even in cases where the assumption of missing at random is not supported (Enders, 2011, p. 344). FIML is particularly effective in longitudinal studies such as the current study in which the same measures are given at each wave (Graham, Taylor, & Cumsille, 2001).
We conducted analyses using Mplus Version 7.11 (Muthén & Muthén, 2015), which computes standard errors using a robust estimator to account for non-normality (i.e., MLR) and a chi-square test of model fit. We used sandwich estimators (i.e., Mplus type=complex and stratification options) to address non-independence resulting from students being nested within grades, cohorts, and schools (Muthén & Satorra, 1995). We ran cross-lagged autoregressive path models to investigate the longitudinal reciprocal relations between trauma-related distress and physical aggression. The models examined the extent to which trauma-related distress at each wave predicted changes in physical aggression at the subsequent wave, and the extent to which physical aggression predicted subsequent changes in trauma-related distress. All models controlled for gender, intervention status, grade, previous levels of trauma-related distress and physical aggression, and included correlations between trauma-related distress and aggression within each wave. We used a multiple group approach to test whether the relations between trauma-related distress and aggression differed as a function of grade and gender by comparing unconstrained models in which parameters were allowed to vary across groups to models in which we constrained corresponding parameters to the same values across groups. We compared models using the scaled chi-square difference test (Satorra & Bentler, 2010) and evaluated overall fit based on their root mean square error of approximation (RMSEA), comparative fit index (CFI), and Tucker-Lewis index (TLI) using general guidelines recommended by Hu and Bentler (1999). Significance for all tests was determined using a two-tailed alpha of .05.
We also evaluated the stability of the relations between trauma-related distress and physical aggression across waves within each grade by comparing unconstrained models that allowed these coefficients to vary across waves with models that constrained corresponding coefficients across waves. We provided context for evaluating the magnitude of effects based on recommendations by Adachi and Willoughby (2015), who argued for interpreting standardized regression coefficients as effect sizes within the context of the concurrent association between the variables (e.g., Wave 1 correlations), the bivariate correlations across waves (i.e., cross-wave correlations), and the stability coefficients (i.e., autoregressive paths).
Results
Descriptive Statistics
Means, standard deviations, and correlations among all variables are reported in Table 1. Table 1 also reports effect sizes representing mean differences across gender and grades. These are based on Cohen’s d, which we calculated in Mplus by dividing parameter estimates reflecting pairwise differences in means by the standard deviation of the outcome. Significance tests on mean differences were obtained in Mplus by dividing these coefficients by their standard errors. As expected, stability coefficients based on autocorrelations across adjacent waves were high for both physical aggression (rs = .37 to .67) and trauma-related distress (rs = .54 to .64). There were also significant positive cross-sectional correlations between physical aggression and trauma-related distress within each wave (rs = .28 to .35). Across waves, physical aggression was significantly correlated with psychological distress at the following wave (rs = .14 to .22), and trauma-related distress was significantly correlated with physical aggression at the subsequent wave (rs = .24 to .36). Based on Cohen’s (1992) criteria for small, medium, and large effect sizes, there were medium-to-large gender differences on psychological distress (ds = .42 to .53, ps < .001), indicating that girls reported higher levels of trauma-related distress across waves. Girls also reported significantly higher levels of physical aggression at Wave 3, albeit at only slightly higher rates (d = .13, p = 0.03). No other differences were found across gender in the reported frequency of engaging in physical aggression. Comparison of means across grades revealed significantly lower frequencies of trauma-related distress in the seventh grade at Wave 4 compared with the sixth grade (d = −.19, p = .02) and significantly higher frequencies of physical aggression in the eighth grade compared with the sixth grade at waves 1 and 2 (ds = .15 and .21, ps < .05 and .01, respectively). These reflected small-to-medium differences in trauma-related distress and physical aggression across grades, and were not consistent across time.
Table 1.
Means, Standard Deviations, and Correlations Within and Across Waves for Trauma-Related Psychological Distress, Physical Aggression, and Gender and Grade Differences
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Distress | ||||||||
| 1. Wave 1 | - | |||||||
| 2. Wave 2 | .54*** | - | ||||||
| 3. Wave 3 | .61*** | .60*** | - | |||||
| 4. Wave 4 | .54*** | .61*** | .64*** | - | ||||
| Physical aggression | ||||||||
| 5. Wave 1 | .30*** | .14** | .20** | .24*** | - | |||
| 6. Wave 2 | .36*** | .35*** | .22*** | .24*** | .58*** | - | ||
| 7. Wave 3 | .30*** | .26*** | .28*** | .19*** | .54*** | .67*** | - | |
| 8. Wave 4 | .17** | .20*** | .24*** | .30*** | .37*** | .51*** | .59*** | - |
| Means | 2.04 | 1.93 | 1.94 | 1.81 | 1.41 | 1.38 | 1.41 | 1.32 |
| Standard deviations | 0.78 | 0.77 | 0.80 | 0.73 | 0.54 | 0.53 | 0.57 | 0.50 |
| d-coefficients | ||||||||
| Girls v boys | 0.42*** | 0.50*** | 0.53*** | 0.53*** | 0.06 | 0.11 | 0.13* | 0.08 |
| 7th grade v 6th grade | −0.12 | 0.01 | −0.06 | −0.19* | 0.08 | 0.14 | 0.02 | 0.04 |
| 8th grade v 6th grade | −0.01 | −0.01 | 0.07 | 0.00 | 0.15* | 0.21** | 0.14 | 0.02 |
Note. N = 2,271.
p < .05
p < 01
p < .001.
Relation Between Trauma-Related Distress and Physical Aggression
Analyses by grade.
Our initial model regressed physical aggression and trauma-related distress on the scores of these constructs at the preceding wave (i.e., autoregressive paths), the cross-lagged paths, and the demographic variables (see Model 1 in Table 2). We also tested a second model that added paths linking physical aggression at Wave 1 to physical aggression at every wave, and trauma-related distress at Wave 1 to trauma-related distress at every wave to see if the initial levels of these constructs predicted changes at every subsequent wave (see Model 2). This significantly improved the overall fit compared to Model 1. We therefore included these effects in all subsequent models. Comparison of multiple group models indicated that constraining regression coefficients representing relations between trauma-related distress, physical aggression, and covariates to the same values across grades did not significantly reduce the fit compared with an unconstrained model that allowed these parameters to vary across grades. Moreover, the RMSEA, CFI, and TLI fit statistics all favored the more parsimonious constrained model (see Model 2 versus 3). We also conducted a more focused test in which we evaluated whether freeing the specific parameters we hypothesized to differ across grades (i.e., cross-lagged relations between trauma-related distress and physical aggression) would improve the fit (see Model 4). It did not. In other words, we did not find support for our hypothesis that the relations between trauma-related distress and physical aggression would differ across grades.
Table 2.
Fit Indices and Comparison of Competing Models Investigating Bidirectional Relations Between Trauma-Related Psychological Distress and Physical Aggression
| Model | χ 2a | df | RMSEA | CFI | TLI | χ2Δb | dfΔ | Comparison Model |
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| Multiple group by grade | ||||||||
| 1. Initial unconstrained modelc | 141.49*** | 48 | .051 | .926 | .820 | - | - | - |
| 2. Unconstrained model | 105.56*** | 36 | .051 | .945 | .820 | 35.72*** | 12 | 1 |
| 3. Fully constrained model | 144.71 *** | 92 | .028 | .958 | .947 | 45.08 | 56 | 2 |
| 4. Partially constrained model | 138.14*** | 80 | .031 | .954 | .932 | 5.70 | 12 | 3 |
| Multiple group by gender | ||||||||
| 5. Initial unconstrained modelc | 125.03*** | 66 | .028 | .949 | .930 | - | - | - |
| 6. Unconstrained model | 62.45*** | 28 | .033 | .970 | .903 | 63.56** | 38 | 5 |
| 7. Fully constrained model | 79.90 | 62 | .016 | .984 | .977 | 19.70 | 34 | 6 |
| 8. Partially constrained model | 78.91* | 56 | .019 | .980 | .960 | 0.98 | 6 | 7 |
| Across Time | ||||||||
| 9. Initial unconstrained model across timec | 117.22*** | 20 | .046 | .926 | .841 | - | - | - |
| 10. Unconstrained across time | 81.43*** | 16 | .042 | .950 | .841 | 31.72*** | 4 | 9 |
| 11. Fully constrained across time | 118.10 *** | 40 | .029 | .940 | .924 | 37.21 * | 24 | 10 |
| 12. Partially constrained across time | 112.14*** | 36 | .031 | .942 | .918 | 6.31 | 4 | 11 |
Note. N = 2,271. Bolded model determined to best fit the data within each set of analyses. RMSEA = Root mean square error of approximation. CFI = comparative fit index. TLI = Tucker-Lewis Fit index.
Chi-square test of model fit.
Satorra-Bentler scaled chi-square difference test comparing fit of each model to the comparison model. Significant chi-square difference test values indicate that the comparison model resulted in a significant improvement in fit.
Initial model that regressed values on constructs at wave 2 to 4 on the value for that construct at the preceding wave. All other models regressed values on the prior wave and on Wave 1.
p < .05.
p < .01.
p < .001.
Analyses by gender.
Compared to our baseline model, adding paths linking physical aggression at Wave 1 to physical aggression at every wave, and trauma-related distress at Wave 1 to trauma-related distress at every wave significantly improved the overall fit (see Model 5 versus 6). Our analyses of multiple group models by gender did not find evidence supporting gender differences in coefficients representing relations among trauma-related distress, physical aggression, and covariates. As with our analyses by grade, the RMSEA, CFI, and TLI fit statistics all improved when coefficients were constrained across grades (see Model 6 versus 7). A more focused test that compared the fully constrained model to a model that allowed the cross-lagged paths to vary across gender (see Model 8) did not significantly improve the fit. In other words, there was no support for our hypothesis of gender differences in the cross-construct relations.
Analyses across time.
We next examined the consistency of effects across waves within the school year (i.e., fall, winter, spring, and summer). Unlike the multiple group models, these analyses included grade and gender as covariates rather than as a grouping factor. As in our multiple group models, adding autoregressive paths representing the coefficients between Wave 1 to Waves 3 through 4 significantly improved model fit (see Model 9 versus 10). To investigate seasonal effects, the second set of models evaluated the stability of coefficients over time (i.e., constraining regression coefficients linking Wave 1 and 2 variables to be equal to the corresponding coefficients linking Wave 2 and 3 variables and Wave 3 and 4 variables). Freeing coefficients between trauma-related distress, physical aggression, and covariates across time significantly improved the model fit based on the difference test. However, this slightly decreased the fit based on the RMSEA and TLI and only slightly improved the CFI (i.e., CFIΔ = .010 (see Model 10 versus 11). Results of a more focused test that allowed only the cross-lagged paths to vary across time did not significantly improve the fit compared with the constrained model (see Model 12). This suggested that the cross-lagged paths were stable across time.
The final model (see Model 12 in Table 2) that constrained unstandardized parameters across time fit the data adequately (RMSEA = .029, CFI = .940, TLI = .924). The standardized coefficients from this model are reported in Table 3 and Figure 1. Prior levels of trauma-related distress predicted increases in physical aggression (βs = 0.08 to 0.09, ps < .001). In contrast, prior levels of physical aggression did not predict changes in trauma-related distress (ps = .83).
Table 3.
Standardized Parameter Estimates (Standard Errors) for Regression of Trauma-Related Psychological Distress and Physical Aggression at Waves 2, 3 and 4
| Independent variable | Wave 2 | Wave 3 | Wave 4 |
|---|---|---|---|
|
| |||
| Dependent Variable: Trauma-Related Psychological Distress | |||
| Physical aggression (prior wave) | 0.01 (0.02) | 0.01 (0.02) | 0.01 (0.03) |
| Distress (prior wave) | 0.48*** (0.04) | 0.44*** (0.04) | 0.51*** (0.04) |
| Distress (Wave 1) | c | 0.34*** (0.08) | 0.22*** (0.06) |
| Male gender | −0.14*** (0.02) | −0.13*** (0.01) | −0.15*** (0.02) |
| Grade 7a | −0.02 (0.02) | −0.02 (0.02) | −0.02 (0.02) |
| Grade 8a | 0.00 (0.02) | −0.00 (0.02) | −0.00 (0.02) |
| Intervention statusb | 0.02 (0.01) | 0.02 (0.01) | 0.02 (0.01) |
| R 2 | 0.25*** (0.04) | 0.48*** (0.06) | 0.48*** (0.05) |
|
| |||
| Dependent Variable: Physical Aggression | |||
| Distress (prior wave) | 0.08*** (0.03) | 0.08*** (0.08) | 0.09*** (0.03) |
| Physical aggression (prior wave) | 0.55*** (0.03) | 0.49*** (0.03) | 0.60*** (0.04) |
| Physical aggression (Wave 1) | c | 0.27*** (0.05) | 0.01 (0.06) |
| Male gender | −0.01 (0.01) | −0.01 (0.01) | −0.01 (0.01) |
| Grade 7a | 0.03 (0.02) | 0.02 (0.01) | 0.03 (0.02) |
| Grade 8a | 0.01 (0.02) | 0.01 (0.01) | 0.01 (0.02) |
| Intervention statusb | −0.03* (0.01) | −0.03* (0.01) | −0.03* (0.01) |
| R 2 | 0.34*** (0.04) | 0.50*** (0.04) | 0.40*** (0.04) |
Note. N = 2,271.
Dummy coded with grade 6 as reference.
Dummy coded with control condition as reference.
Value is same as reported in table under “prior wave.”
p < .05.
p < .01.
p < .001.
Figure 1.
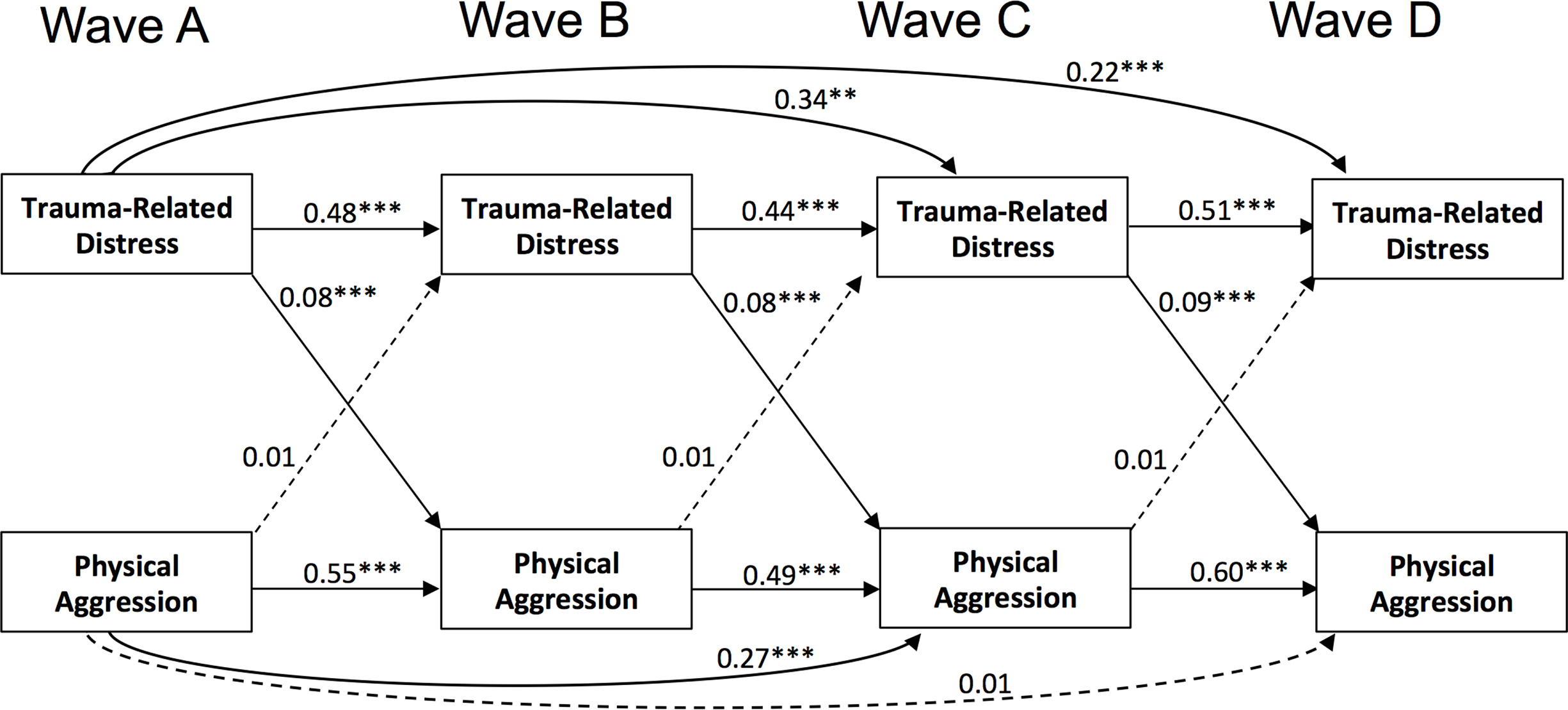
Autoregressive path model (standardized coefficients) representing reciprocal relations between trauma-related psychological distress and physical aggression across a year within middle school. Demographic covariates and correlations between measures within each wave were included in the model, but are not shown in the figure.
We followed Adachi and Willoughby’s (2015) recommendation to interpret effect sizes based on standardized coefficients within the context of their concurrent association, the bivariate cross-lagged correlations (see Table 1), and the stability coefficients within the autoregressive models (see Table 3). The within-wave correlations between adolescents’ trauma-related distress and physical aggression were small to moderate across waves (rs = .28 to .34), as were the cross-lagged bivariate correlations (r = .24 to .35). Notably, the stability coefficients were moderate to large across both constructs (βs = 0.44 to 0.51 and 0.49 to 0.60 for trauma-related distress and physical aggression, respectively). Although path coefficients within our final model were small (i.e., .08 to .09), Adachi and Willoughby (2015) argued that the magnitude of these effects is limited when a large percentage of variance is explained by within-wave correlations and stability coefficients. In such instances, they noted that even small effects, such as those found in the current study, are meaningful and can accumulate over time.
Discussion
The purpose of this study was threefold: (a) to examine reciprocal longitudinal relations between physical aggression and trauma-related distress among early adolescents, (b) to examine gender differences in these relations, and (c) to assess the extent to which these relations differed within and across middle school grades. We addressed these aims within a predominantly African American sample of adolescents living in urban areas with high rates of crime and poverty. Identifying key periods within middle school when the association between trauma-related distress and aggression is strongest has important implications for screening purposes. Overall, we did not find support for reciprocal relations between physical aggression and trauma-related distress. We found evidence supporting trauma-related distress as a significant risk factor for physical aggression. However, physical aggression did not predict changes in trauma-related distress. These findings were stable across gender, grade, and waves.
The direct impact of trauma-related distress on physical aggression found in the current study underscores the unique contribution of trauma-related distress on later aggression, even after controlling for aggression at previous waves. The current findings are consistent with past cross-sectional studies that have found a strong association between trauma-related distress and aggression (Abate et al., 2017; Aebi et al., 2017; Marsee, 2008). Given the high prevalence rates of childhood victimization and exposure to violence, assessment of trauma-related distress should be more widespread within violence prevention and intervention research. This could provide additional elucidation regarding trauma-related distress as a mediator of the relation between exposure to various traumatic events and aggressive behavior.
The pattern of relations between trauma-related distress and physical aggression was consistent across middle school grades, time of year, and gender. That is, the impact of trauma-related distress on physical aggression was stable across sixth, seventh, and eighth grade, including the summer months, and the effects were similar for boys and girls. This is counter to our hypotheses that these relations would be stronger at the beginning of the school year and during the sixth grade as compared with seventh and eighth grade. Although no gender differences were found in the relation between the two constructs, descriptive statistics indicated that girls were more likely to experience trauma-related distress, which is consistent with prior research (e.g., Alisic et al, 2014). In contrast, we did not find consistent differences in physical aggression across gender. Girls reported slightly higher rates of physical aggression at Wave 3 (i.e., spring) but no differences were found at the other three waves. Although boys are often found to have higher rates of physical aggression overall (e.g., Card et al., 2008), the current findings are more consistent with prior studies that examined prevalence rates within predominately African American samples living in urban, under-resources communities with high rates of violence (Bettencourt & Farrell, 2013; Bradshaw et al., 2010).
We found small effect sizes representing the relation between trauma-related distress and subsequent physical aggression. This may reflect the short period of time over which change was examined (i.e., 3-month intervals), which likely contributed to the large stability coefficients representing each construct’s stability over time (i.e., βs = 0.44 to 0.60). Given these large stability coefficients, we believe even small cross-lagged effects can be interpreted meaningfully. The small effect sizes for the cross-lagged paths may also be due to potential moderators that warrant further examination. For example, among youth exposed to political violence, initial levels of aggressive behavior moderated the relations between exposure to violence and later trauma-related distress and aggression (Gvirsman et al., 2014). This suggests that youth who are highly aggressive may be particularly at risk for increased aggressive behavior after experiencing trauma-related distress. Trauma-related distress rates also vary by specific types of trauma (e.g., Alisic et al., 2014). Given evidence for desensitization after repeated exposure to violence (Mrug et al., 2016), the link between trauma-related distress and aggression most likely differs dependent upon the prior level of exposure to traumatic events. The current study’s finding of a longitudinal pathway between trauma-related distress and physical aggression suggests the need for further research to investigate trauma-related distress as a mediator between various traumatic events and physical aggression.
A second aim of our study was to investigate whether the frequency of physical aggression predicted changes in trauma-related distress over time. We did not find support for our hypothesis that physical aggression would predict increases in psychological distress during middle school. We were unable to find any prior studies that examined a causal link between physical aggression and changes in trauma-related distress. However, this finding is inconsistent with prior theory and past findings that have suggested a path between aggression and different forms of victimization that could potentially lead to trauma-related distress among early adolescents (Merlo & Benekos, 2016; van der Molen et al., 2015). The current sample was limited to middle school youth and investigated change over short periods of time (i.e., 3-month intervals). In one of the largest prospective longitudinal birth cohort studies examining developmental mental health histories across three decades, over 40% of individuals diagnosed with PTSD at age 32 had received a diagnosis of conduct disorder by the age of 15 (Koenen et al., 2008). Therefore, aggression (i.e., a symptom of conduct disorder) may still be an important risk factor for later development of trauma-related distress, yet it may not emerge until much later.
Limitations
This study had several limitations that should be considered in interpreting our findings. We examined longitudinal relations between physical aggression and trauma-related distress within a predominantly African American sample of middle school youth living in urban areas with high rates of crime and poverty. This is a particularly relevant sample given their high risk of exposure to community violence and other events that may lead to trauma-related distress (Baskin-Sommers et al., 2017). Unfortunately however, our sample was not sufficiently diverse to allow us to examine race or socio-economic status as possible moderators of relations between trauma-related distress and aggression. Further work is needed to determine the extent to which our findings might generalize to other samples, including more racially and ethnically diverse samples of youth from broader age ranges.
Moreover, our focus was on relations with a continuous measure of trauma-related distress symptoms often associated with traumatic events and not on whether the participants met DSM-5 criteria for PTSD. Whether similar results would be obtained in studies examining differences in aggression for adolescents diagnosed with PTSD remains to be seen. We also focused broadly on relations between aggression and trauma-related distress symptoms without regard to the specific traumatic event(s) that led to the distress. The fact that our participants were from communities with high rates of poverty and violence suggests that exposure to community violence may have been the primary source of trauma for many participants. However, we were not able to test this assumption explicitly. In addition, our analyses were based on adolescent report of their frequency of physical aggression and experience of trauma-related distress. Self-report of problem behaviors may lead to underreporting due to social desirability or biased results due to shared variance in measurement error. It is important to note however, that parents and teachers may not be the best reporters on internalizing behaviors or on adolescent behaviors that are less likely to occur in their presence (Youngstrom, Loeber, & Stouthamer-Loeber, 2000). Finally, our analyses were conducted using data from a study that evaluated the impact of a bullying prevention program. We controlled for the potential impact of the intervention on trauma-related distress and physical aggression by including it as a covariate in our models. Moreover, it is important to note that the evaluation project did not find intervention effects on student reports of trauma-related distress or physical aggression (Author reference). Nonetheless we cannot rule out the possibility that the intervention produced more subtle effects on our findings.
Conclusions
Despite some limitations, this is the first study of which we are aware that examined reciprocal relations between trauma-related distress and physical aggression across more than two waves of data and that controlled for prior levels of both constructs. The majority of prior studies examining these relations have been cross-sectional, making it difficult to infer causation. Within the current study, we found a direct impact of trauma-related distress on physical aggression, which was stable across middle school and gender. Given these results, it is recommended that future work examine possible moderators of the relation between trauma-related distress and physical aggression, such as the precipitating traumatic events, race, ethnicity, and neighborhood disadvantage.
Overall, our findings highlight the potential value of screening for trauma-related distress within public systems that adolescents come into contact with, such as the educational and juvenile justice systems. Traumatic experiences are common among adolescents (e.g., Finkelhor, Turner, Ormrod, & Hamby, 2009), yet teachers, administrators, and health professionals who lack trauma-informed training may misinterpret youths’ responses to trauma (e.g., aggression), which can lead to harsher punishment or misdiagnoses without addressing youth’s comorbid internalizing symptoms. This is particularly salient given the fact that African American girls receive more severe disciplinary actions than all other female students (Blake, Butler, Lewis, Darensbourg, 2011) and are the fastest growing population in the juvenile justice system (Crenshaw, Ocen, & Nanda, 2015).
Trying to assess for risk factors of problem behaviors, such as past traumas and their associated internalizing symptoms, may provide school administrators with additional information that can inform their decisions regarding school policies and disciplinary tactics. Notably, traumatized adolescents of color exhibiting problems behaviors are at a higher risk than White adolescents to be misdiagnosed with attention-deficit/hyperactivity disorder, oppositional defiant disorder, and conduct disorder (e.g., Ford & Courtois, 2009; Mizock & Harkins, 2011). These youth have been shown to exhibit increased emotion dysregulation after developing psychological distress (Marsee, 2008), are more likely to be suspended or expelled in school (e.g., Skiba et al., 2011), and are disproportionally represented in special education and the juvenile justice system (e.g., Abramovitz & Mingus, 2016). This further underscores the importance of screening for trauma-related distress among urban minority youth who are at greater risk of exposure to traumatic events. Additional work should examine the reciprocal longitudinal relations between trauma-related distress and other forms of maladjustment, such as delinquency, substance use, and office disciplinary referrals.
Acknowledgments
This study was funded by the National Center for Injury Prevention and Control, Centers for Disease Control and Prevention, CDC Cooperative Agreements 5U01CE001956 and National Institute of Justice, grant number 2014-CK-BX-0009. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention or the National Institute of Justice.
Footnotes
The authors do not have any conflict of interests to disclose.
References
- Abate A, Marshall K, Sharp C, & Venta A (2017). Trauma and aggression: Investigating the mediating role of mentalizing in female and male inpatient adolescents. Child Psychiatry Human Development, 48, 881–890. doi: 10.1007/s10578-017-0711-6 [DOI] [PubMed] [Google Scholar]
- Abramovitz R, & Mingus J (2016). Unpacking racism, poverty, and trauma’s impact on the school-to-prison pipeline. In Carten AJ, Siskind AB, & Green MP (Eds.), Strategies for deconstructing racism in the health and human services (pp. 245–265). New York, NY: Oxford University Press. [Google Scholar]
- Adachi P, & Willoughby T (2015). Interpreting effect sizes when controlling for stability effects in longitudinal autoregressive models: Implications for psychological science. European Journal of Developmental Psychology, 12, 116–128. doi: 10.1080/17405629.2014.963549 [DOI] [Google Scholar]
- Aebi M, Mohler-Kuo M, Barra S, Schnyder U, Maier T, & Landolt MA (2017). Postpsychological distress and youth violence perpetration: A population-based cross-sectional study. European Psychiatry, 40, 88–95. doi: 10.1016/j.eurpsy.2016.08.007 [DOI] [PubMed] [Google Scholar]
- Akers RL (1998). Social learning and social structure: a general theory of crime and deviance. Boston, MA: Northeastern University Press. [Google Scholar]
- Alisic E, Zalta AK, van Wesel F, Larsen SE, Hafstad GS, Hassanpour K, & Smid GE (2014). Rates of post-psychological distress disorder in trauma-exposed children and adolescents: Meta-analysis. The British Journal of Psychiatry: The Journal of Mental Science, 204, 335. doi: 10.1192/bjp.bp.113.131227 [DOI] [PubMed] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental Disorders (5th ed.). Arlington, VA: American Psychiatric Association. [Google Scholar]
- American Psychiatric Association. (1987). Diagnostic and statistical manual of mental Disorders (3rd ed.). Washington, D.C: American Psychiatric Association. [Google Scholar]
- Baskin-Sommers AR, Baskin DR, Sommers I, Casados AT, Crossman MK, & Javdani S (2016). The impact of psychopathology, race, and environmental context on violent offending in a male adolescent sample. Personality Disorders: Theory, Research, and Treatment, 7(4), 354–362. [DOI] [PubMed] [Google Scholar]
- Bettencourt AF, & Farrell AD (2013). Individual and contextual factors associated with patterns of aggression and peer victimization during middle school. Journal of Youth and Adolescence, 42, 285–302. doi: 10.1007/s10964-012-9854-8 [DOI] [PubMed] [Google Scholar]
- Blake JJ, Butler BR, Lewis CW, & Darensbourg A (2011). Unmasking the inequitable discipline experiences of urban black girls: Implications for urban educational stakeholders, The Urban Review, 43(1), 90–106. doi: 10.1007/s11256-009-0148-8 [DOI] [Google Scholar]
- Bradshaw CP, Mitchell MM, O’Brennan LM, & Leaf PJ (2010). Multilevel exploration of factors contributing to the overrepresentation of black students in office disciplinary referrals. Journal of Educational Psychology, 102(2), 508–520. doi: 10.1037/a0018450 [DOI] [Google Scholar]
- Bradshaw CP, Schaeffer CM, Petras H, & Ialongo N (2010). Predicting negative life outcomes from early aggressive-disruptive behavior trajectories: Gender differences in maladaption across life domains. Journal of Youth and Adolescence, 39, 953–966. doi: 10.1007/s10964-009-9442-8 [DOI] [PubMed] [Google Scholar]
- Brancu M, Mann-Wrobel M, Beckham JC, Wagner HR, Elliott A, Robbins AT, . . . Runnals JJ (2016). Subthreshold postpsychological distress disorder: A meta-analytic review of DSM–IV prevalence and a proposed DSM–5 approach to measurement. Psychological Trauma: Theory, Research, Practice, and Policy, 8(2), 222–232. doi: 10.1037/tra0000078 [DOI] [PubMed] [Google Scholar]
- Card NA, Stucky BD, Sawalani GM, & Little TD (2008). Direct and indirect aggression during childhood and adolescence: A meta-analytic review of gender differences, intercorrelations, and relations to maladjustment. Child Development, 79(5), 1185–1229. doi: 10.1111/j.1467-8624.2008.01184.x [DOI] [PubMed] [Google Scholar]
- Carter RT (2007). Racism and psychological and emotional injury: Recognizing and assessing race-based traumatic stress. The Counseling Psychologist, 35(1), 13–105. doi: 10.1177/0011000006292033 [DOI] [Google Scholar]
- Cohen J (1992). A power primer. Psychological Bulletin, 112(1), 155–159. doi: 10.1037/0033-2909.112.1.155 [DOI] [PubMed] [Google Scholar]
- Crenshaw K, Ocen P, & Nanda J (2015). Black girls matter: Pushed out, overpoliced, and underprotected. Center for Intersectionality and Social Policy Studies. African American Policy Forum. Retrieved from https://static1.squarespace.com/static/53f20d90e4b0b80451158d8c/t/54d2d37ce4b024b41443b0ba/1423102844010/BlackGirlsMatter_Report.pdf. [Google Scholar]
- Cromer KD, & Villodas MT (2017). Postpsychological distress as a pathway to psychopathology among adolescents at high-risk for victimization. Child Abuse & Neglect, 67, 182–192. [DOI] [PubMed] [Google Scholar]
- Eaton NR, Rodriguez-Seijas C, Carragher N, & Krueger RF (2015). Transdiagnostic factors of psychopathology and substance use disorders: A review. Social Psychiatry and Psychiatric Epidemiology: The International Journal for Research in Social Genetic Epidemiology and Mental Health Services, 50(2), 171–182. [DOI] [PubMed] [Google Scholar]
- Enders CK (2011). Missing not at random models for latent growth curve analyses. Psychological Methods, 16, 1–16. doi: 10.1037/a0022640 [DOI] [PubMed] [Google Scholar]
- Farrell AD, Goncy EA, Sullivan TN, & Thompson EL (2018). Victimization, aggression, and other problem behaviors: Trajectories of change within and across middle school grades. Journal of Research on Adolescence. 28, 438–455. doi: 10.1111/jora.12346 [DOI] [PubMed] [Google Scholar]
- Farrell AD, Mehari KR, Kramer-Kuhn A, & Goncy EA (2014). The impact of victimization and witnessing violence on physical aggression among high-risk adolescents. Child Development, 85(4), 1694–1710. doi: 10.1111/cdev.12215 [DOI] [PubMed] [Google Scholar]
- Farrell AD, Sullivan TN, Goncy EA, & Le ATH (2016). Assessment of adolescents’ victimization, aggression, and problem behaviors: Evaluation of the Problem Behavior Frequency Scale. Psychological Assessment, 28(6), 702–714. doi: 10.1037/pas0000225 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Finkelhor D, Turner H, Ormrod R, & Hamby SL (2009). Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics, 124(5), 1411–1423. doi: 10.1542/peds.2009-0467 [DOI] [PubMed] [Google Scholar]
- Ford JD, & Courtois CA (2009). Defining and Understanding Complex Trauma and Complex Psychological distress Disorders. In Courtois CA & Ford JD (Eds.), Treating Complex Psychological distress Disorders (pp. 13–30). New York, New York: The Guilford Press. [Google Scholar]
- Foster H, & Brooks-Gunn J (2009). Toward a stress process model of children’s exposure to physical family and community violence. Clinical Child and Family Psychology Review, 12(2), 71–94. doi: 10.1007/s10567-009-0049-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- García Coll C, Lamberty G, Jenkins R, McAdoo HP, Crnic K, Wasik BH, Vázquez García H (1996). An integrative model for the study of developmental competencies in minority children. Child Development, 67(5), 1891–1914. doi: 10.1111/j.1467-8624.1996.tb01834.x [DOI] [PubMed] [Google Scholar]
- Graham JW, Taylor BJ, & Cumsille PE (2001). Planned missing-data designs in analysis of change. In Collins LM & Sayer A(Eds.). New methods for the analysis of change (pp. 335–353). Washington, DC: American Psychological Association. doi:org/10.1037/10409–011 [Google Scholar]
- Grant KE, Compas BE, Stuhlmacher AF, Thurm AE, McMahon SD, & Halpert JA, (2003). Stressors and child and adolescent psychopathology: Moving from markers to mechanisms of risk. Psychological Bulletin, 129(3), 447–466. doi: 10.1037/0033-2909.129.3.447 [DOI] [PubMed] [Google Scholar]
- Gvirsman SD, Huesmann LR, Dubow EF, Landau SF, Shikaki K, & Boxer P (2014). The effects of mediated exposure to ethnic-political violence on Middle East youth’s subsequent post-psychological distress symptoms and aggressive behavior. Communication Research, 41(7), 961–990. doi: 10.1177/0093650213510941 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6, 1–55. doi: 10.1080/10705519909540118 [DOI] [Google Scholar]
- Kang H, & Burton DL (2014). Effects of racial discrimination, childhood trauma, and psychological distress on juvenile delinquency in African American incarcerated youth. Journal of Aggression, Maltreatment & Trauma, 23(10), 1109–1125. doi: 10.1080/10926771.2014.968272 [DOI] [Google Scholar]
- Kerig PK, & Becker SP (2012). Trauma and girls delinquency. In Miller S, Leve L, & Kerig PK(Eds.), Delinquent girls: Context, relationships, and adaptation (pp. 119–143). New York: Springer Books. doi: 10.1007/978-1-4614-0416-6_8 [DOI] [Google Scholar]
- Koenen KC, Moffitt TE, Caspi A, Gregory A, Harrington H, & Poulton R (2008). The developmental mental-disorder histories of adults with postpsychological distress disorder: A prospective longitudinal birth cohort study. Journal of Abnormal Psychology, 117(2), 460–466. doi: 10.1037/0021-843X.117.2.460 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Little TL & Rhemtulla M (2013). Planned missing data designs for developmental researchers. Child Development Perspectives, 7, 199–204. doi: 10.1111/cdep.12043 [DOI] [Google Scholar]
- Liu J, Bolland JM, Dick D, Mustanski B, & Kertes DA (2016). Effect of environmental risk and externalizing comorbidity on internalizing problems among economically disadvantaged African American youth. Journal of Research on Adolescence, 26(3), 552–566. doi: 10.1111/jora.12213 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsee MA (2008). Reactive aggression and postpsychological distress in adolescents affected by Hurricane Katrina. Journal of Clinical Child and Adolescent Psychology, 37(3), 519–529. doi: 10.1080/15374410802148152 [DOI] [PubMed] [Google Scholar]
- Mash EJ, & Barkley RA (2007). Assessment of childhood disorders (4th ed.). New York: Guilford Press. [Google Scholar]
- Mathews T, Dempsey M, & Overstreet S (2009). Effects of exposure to community violence on school functioning: The mediating role of postpsychological distress symptoms. Behaviour Research and Therapy, 47(7), 586–591. doi: 10.1016/j.brat.2009.04.001 [DOI] [PubMed] [Google Scholar]
- Merlo AV, & Benekos PJ (2016). Maltreatment and delinquency: Breaking the cycle of offending. In McShane MD & Cavanaugh M (Eds.), Understanding Juvenile Justice and Delinquency (pp. 5–21). Santa Barbara, CA, US: Praeger/ABC-CLIO. [Google Scholar]
- Mizock L, & Harkins D (2011). Diagnostic bias and conduct disorder: Improving culturally sensitive diagnosis. Child & Youth Services, 32(3), 243–253. doi: 10.1080/0145935X.2011.605315 [DOI] [Google Scholar]
- Mrug S, Madan A, & Windle M (2016). Emotional desensitization to violence contributes to adolescents’ violent behavior. Journal of Abnormal Child Psychology, 44(1), 75–86. doi: 10.1007/s10802-015-9986-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK and Muthén BO (1998–2015). Mplus User’s Guide. Seventh Edition. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Muthén B, & Satorra A (1995). Complex sample data in structural equation modeling. In Marsden PV (Ed.), Sociological Methodology (pp. 267–316). Washington, DC: American Sociological Association. [Google Scholar]
- Olweus D, & Limber SP (2010). Bullying in school: Evaluation and dissemination of the Olweus Bullying Prevention Program. American Journal of Orthopsychiatry, 80, 124–134. doi: 10.1111/j.1939-0025.2010.01015.x [DOI] [PubMed] [Google Scholar]
- Overstreet S, & Braun S (2000). Exposure to community violence and post-psychological distress symptoms: Mediating factors. American Journal of Orthopsychiatry, 70(2), 263–271. doi: 10.1037/h0087828 [DOI] [PubMed] [Google Scholar]
- Perfect MM, Turley MR, Carlson JS, Yohanna J, Saint Gilles MP (2016). School-related outcomes of traumatic event exposure and psychological distress symptoms in students: A systematic review of research from 1990 to 2015. School Mental Health, 8(1), 7–43. doi: 10.1007/s12310-016-9175-2 [DOI] [Google Scholar]
- Richters JE, & Martinez P (1993). The NIMH community violence project: I. children as victims of and witnesses to violence. Psychiatry, 56(1), 7–21. [DOI] [PubMed] [Google Scholar]
- Romero E, Richards MH, Harrison PR, Garbarino J, & Mozley M (2015). The role of neighborhood in the development of aggression in urban African American youth: A multilevel analysis. American Journal of Community Psychology, 56, 156–169. doi: 10.1007/s10464-015-9739-6 [DOI] [PubMed] [Google Scholar]
- Satorra A, & Bentler PM (2010). Ensuring positiveness of the scaled difference chi-square test statistic. Psychometrika, 75, 243–248. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Skiba RJ, Horner RH, Chung C, Rausch MK, May SL, & Tobin T (2011). Race is not neutral: A national investigation of African American and Latino disproportionality in school discipline. School Psychology Review, 40(1), 85–107. [Google Scholar]
- Taft CT, Murphy CM, & Creech SK (2016). Social information processing model of trauma and intimate partner violence. In Tafter CT, Murphy CM, & Creech SK (Eds.), Trauma-informed treatment and prevention of intimate partner violence (pp. 15–25). Washington, DC, US: American Psychological Association. doi: 10.1037/14918-002 [DOI] [Google Scholar]
- Turner HA, Finkelhor D, & Ormrod R (2006). The effect of lifetime victimization on the mental health of children and adolescents. Social Science & Medicine (1982), 62(1), 13–27. doi:S0277–9536(05)00253–4 [DOI] [PubMed] [Google Scholar]
- van der Kolk BA, Roth S, Pelcovitz D, Sunday S, & Spinazzola J (2005). Disorders of extreme stress: The empirical foundation of a complex adaptation to trauma. Journal of Psychological distress, 18(5), 389–399. doi: 10.1002/jts.20047 [DOI] [PubMed] [Google Scholar]
- van der Molen E, Blokland AA, Hipwell AE, Vermeiren RR, Doreleijers TA, & Loeber R (2015). Girls’ childhood trajectories of disruptive behavior predict adjustment problems in early adolescence. Journal of Child Psychology and Psychiatry, 56(7), 766–773. doi: 10.1111/jcpp.12339 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wigfield A, Byrnes JP, & Eccles JS (2006). Development during early and middle adolescence. In Alexander PA & Winne PH (Eds.), Handbook of educational psychology (pp. 87–113). Mahwah, NJ, US: Lawrence Erlbaum Associates Publishers. [Google Scholar]
- Wolfe DA, Wekerle C, Scott K, Straatman A, & Grasley C (2004). Predicting abuse in adolescent dating relationships over 1 year: The role of child maltreatment and trauma. Journal of Abnormal Psychology, 113(3), 406–415. doi: 10.1037/0021-843X.113.3.406 [DOI] [PubMed] [Google Scholar]
- Youngstrom E, Loeber R, & Stouthamer-Loeber M (2000). Patterns and correlates of agreement between parent, teacher, and male adolescent ratings of externalizing and internalizing problems. Journal of Consulting and Clinical Psychology, 68, 1038–1050. doi: 10.1037/0022-006X.68.6.1038 [DOI] [PubMed] [Google Scholar]
- Zimmerman GM & Messner SF (2013). Individual, family background, and contextual explanations of racial and ethnic disparities in youths’ exposure to violence. American Journal of Public Health, 103(3), 435–442. doi: 10.2105/AJPH.2012.30093 [DOI] [PMC free article] [PubMed] [Google Scholar]