

Abstract
The COVID-19 pandemic introduced lockdown and social distancing measures that made new methods of healthcare essential. Telehealth was introduced as a temporary measure but is being considered as a more permanent form of healthcare, particularly in rural areas, to provide more equitable healthcare. A survey was conducted on 200 rural dwellers (residents) regarding their experience with rural healthcare, any barriers to adequate healthcare, and openness to telehealth. The results demonstrated interest in telehealth and predominately positive experiences with telehealth in the areas where there was need and lack of access to healthcare, more commonly expressed in the younger age group. Quality healthcare should be equitable and available for every individual irrespective of zip code or the county they live. Telehealth is capable of bridging the gap of lack of access and transportation for individuals in rural areas to meet their healthcare needs in a timely fashion in the coming years.
Keywords: telehealth, rural health, telemedicine
Introduction
The implementation of telehealth and telemedicine services was spread by the COVID-19 pandemic1 due to lockdown and social distancing measures. Traditional medical appointments with in-person physicians became more difficult, and telehealth was implemented on a large scale in many hospital systems as a temporary substitute. In addition to spreading telehealth, the pandemic exposed underlying health disparities in several communities, especially rural areas.1 The rural health disparity is caused by a combination of complex factors, including economic opportunities, education quality, substance abuse, chronic illnesses, HIV, poverty, and unemployment.1,2 Almost one in five Americans live in rural areas.2 Although the rural health disparity has lasted for several decades, and it has been well-researched and extensively documented,2 it continues to persist today. The pandemic prompted innovative solutions to address these health needs in the face of a critical public health threat, one of which was telehealth.
Several studies have been done on the effectiveness of telehealth in rural areas.3–5 These showed consistently positive results. In a rural Tennessee-based study of a Tele oncology program, 95% of patients who initially saw the oncologist in person and had audiovisual conferencing for half of their visits reported that their experience was as good as or better than an in-person appointment.4 In a Kansas-based study of a Tele oncology program, all 22 participants were satisfied with the service.4 Pediatric research on addressing rural health disparities with telehealth concluded that in underserved communities, telemedicine can often significantly increase the quality of care; patient safety; patient, family, and provider satisfaction and reduce costs of care.5 With results showing the effectiveness of telehealth in addressing the rural health disparity, a recommended approach to decreasing the disparity is the conversion of pandemic-friendly telehealth policies to permanent medical services.2
Methods
Ethical considerations
The study was exempt by the HCA Centralized Algorithms for Research Rules on IRB Exemptions (CARRIE)/ IRB manager, study number 2022-583.
Recruitment and Data Collection
Two hundred U.S. rural dwellers (residents) were surveyed with questions related to rural healthcare access, healthcare barriers, and telehealth interest in rural areas. A single screening question determined survey eligibility by asking whether respondents lived in an urban, suburban, or rural area. Only those who selected rural were included in the survey. Age, gender, education, income, and race were also included. The survey consisted of ten questions, including multiple choice and free response questions. Five of the questions centered around rural healthcare and barriers, such as distance, transportation, access, and personal experience with rural health care or telehealth. Two questions inquired about the rural use of healthcare, such as reasons for seeing a doctor and reasons for barriers to receiving adequate medical attention. The remaining three questions addressed telehealth, including if the respondent had used telehealth services, the respondent’s openness to telehealth, and the respondent’s experience with telehealth.
Statistical Analysis
Data were analyzed using the statistical analysis software JMP. The significance threshold is alpha = .05 and all confidence intervals are 95%.
Results
Demographic Statistics
The cohort consisted of 111 females (55%) and 91 males (45%). The age group ranged from 18 years to 80 years, with a median of 39 and interquartile range of 33-52 years (Figure 1).
Figure 1. Age distribution of the cohort.
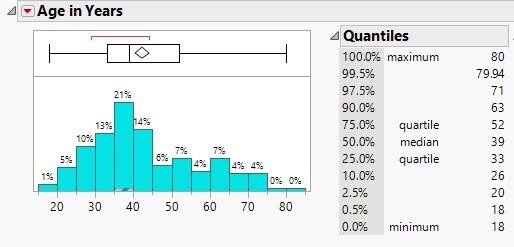
Among the sample size of 202, the majority were in the age group of 33-52 years with a median of 39 years.
Race distribution showed the respondents were 79.2% white, 8.9% black, 5% Hispanic/Latino, and 7% other. The income range showed that of the total respondents, 29.7% made below $25,000, 25.2% made between $25,000 and $50,000, 27.2% made between $50,000 and $100,000, 8.9% made between $100,000 and $150,000, 4.5% made above $150,000, and 4.5% preferred not to say. Education distribution showed that 44% had high school education, 18% had a university education, 15% had postgraduate education, 18% had vocational/technical college education, and 5% had middle school education.
Survey Questions
The average time for respondents to drive to their primary care doctor was 23.5 minutes. Single-choice questions often revealed near 50/50 splits. When asked if transportation or time was a barrier, 52% reported yes or sometimes, and 48% reported no. When asked if adequate health care or specialists was a concern, 48% said yes, 47% reported no, and 5% reported that they did not know. When asked if they would have preferred to see the doctor more often, 47.5% reported yes, and 52.5% reported no. When asked if they had previously used telehealth or telemedicine services, 48.5% reported yes, and 51.5% reported no.
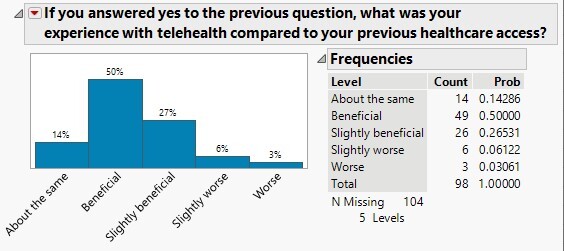
Univariate analysis of the responses to survey questions was also conducted. A question inquiring about the reasons for seeing a doctor in the past year, allowing multiple selected answers, revealed the following: only 56.4% had a routine physical in the past year, 32.7% had a routine visit for chronic conditions, 14.4% had a consultation regarding surgery, 38.1% had illness or injury, 28% had prescription refill only, 10.9% had physical therapy, 20.3% had mental health therapy/treatment, 8.4% had substance use treatment, and 3% reported other, including pregnancy and post-accident care. A question inquiring about barriers in attending appointments or receiving adequate healthcare, allowing multiple selected answers, revealed the following: 32.7% reported too long of a wait to see a doctor, 24.8% reported not having transportation to the hospital/clinic, 22.8% reported difficulty in getting appointments due to timings, 15.8% reported not attending appointments because they were not sick, 13.9% reported not trusting the quality of healthcare, 24.8% reported expenses as a barrier, and 4.5% reported other, including “my insurance isn’t accepted for at least 100 miles,” and 26.7% reported no barriers. When asked about the quality of their experience with telehealth, 76.5% reported it was beneficial, 9.2% reported it was worse, and 14.3% reported it was about the same. When asked if they were open to telehealth, 88% reported yes, and 12% reported no (Figure 2).
Figure 2. 88% of respondents were open to telehealth.
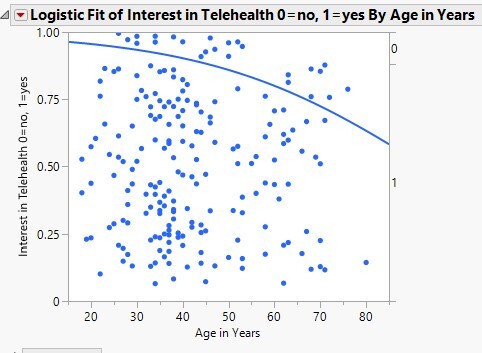
The survey showed that the younger age group was more interested in telehealth than the older age group (Figure 3).
Figure 3. Younger age group showed significantly greater interest in telehealth.
Transportation as a barrier to adequate healthcare was significantly correlated with needing to see a doctor more often (Figure 4).
Figure 4. When respondents reported preferring or needing to see a doctor more often, they were significantly more likely to have transportation barriers.
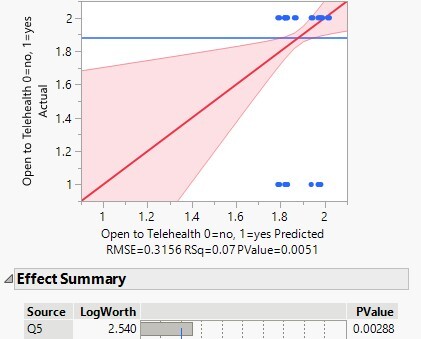
The people who wanted to see a doctor more often were more likely interested in and open to telehealth (Figure 5).
.
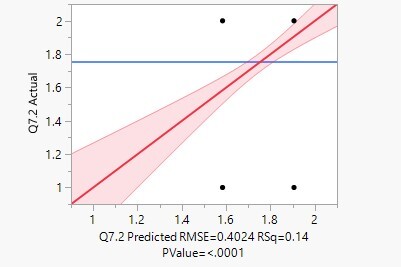
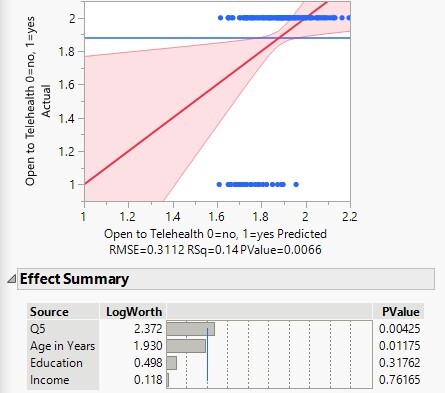
Those who wanted to see a doctor more often within the year and those of a younger age group were more likely to seek telehealth opportunities. Education and income were not significant determining factors in openness to telehealth (Figure 6).
Figure 6. Multivariate model demonstrating that desire to see a doctor more often and.
Discussion
Currently, rural interest in telehealth is present and predominately positive. In the survey, 88% were either considering or in favor of telehealth, and only 12% of respondents reported that they would not be open to telehealth at this time. Telehealth has been an emerging nontraditional form of healthcare in rural areas for addressing some of the issues underlying the disparity. Patients in rural areas often have to travel long distances to have access to healthcare, and even longer distances to get specialized care.4 Another problem is patients feeling that they received insufficient information from their physician and insufficient discussion time with their physician.4 Telehealth eliminates the patient’s travel time and distance and provides a more accessible option for communicating with their physician in a timely fashion.
Rural telehealth has been studied for use in multiple departments, such as specialty care, intensive care, and acute/emergency care.2
For example, telemedicine has been used in prehospital care to expedite stroke and myocardial infarction triage.6 One of the largest US integrated healthcare delivery systems in New York also used telemedicine to provide express care for patients presenting to the emergency room for minor complaints such as wound checks, upper respiratory infections, contusions, suture removals, and simple rashes.7 The same hospital systems also studied the acceptance of telemedicine amongst more than 1000 geriatric patients and found that they too were favorable towards telemedicine.8
Telehealth also has the potential to address the geographic misdistribution of specialties such as pediatrics and provide specialty care to rural populations lacking specialty access.4 There is a significant difference in the usage of telemedicine for urban and rural areas in terms of specialties and demographics, further demonstrating the importance of taking the concerns and needs of rural patients into consideration when providing quality telehealth.9 However, telehealth is not new to rural areas and has supplemented rural healthcare in the past, although the COVID-19 pandemic has increased awareness of its potential for rural populations. In the late 1990s, access to teleconsultation with a radiologist in rural areas significantly affected diagnosis and treatment plans.10 With the effectiveness of telehealth and substantial investment in improving rural health care, rural health systems are encouraged to ensure the sustainability of telehealth programs.1
Limitations
The survey sample size of 200 may not be as reflective of the needs of the general rural population as a survey conducted on a larger scale would be. Survey research is susceptible to bias in the truthfulness of responses, and the specific reasons for responses that may be obtained from a more detailed research method about the respondent’s situation remain unknown. In addition, using the third-party survey provider limits the population of respondents by sampling only people with incentives to complete surveys conducted through the third-party provider. In spite of these limitations, the survey provides valuable insight into the relationship between the needs of rural patients, the barriers to rural healthcare, and telehealth as an option to improve healthcare quality and accessibility.
Conclusion
Tailoring telehealth options and availability for residents of rural communities is an emerging tool for ensuring quality healthcare. Determining the needs rural residents use telehealth to meet can help establish a more sustainable model of telehealth in combination with traditional healthcare.
Quality healthcare should be available for every individual irrespective of zip code or the county they live. Telehealth is capable of bridging the gap of lack of access and transportation for individuals in rural areas to meet their healthcare needs in a timely fashion.
References
- 1. Hirko KA, Kerver JM, Ford S, et al. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. Journal of the American Medical Informatics Association. 2020;27(11):1816-1818. doi:10.1093/jamia/ocaa156 [DOI] [PMC free article] [PubMed]
- 2. U.S. Department of Health and Human Services. Improving rural health through telehealth-guided provider-to-provider communication. National Institutes of Health. Published February 4, 2022. Accessed June 30, 2022. https://prevention.nih.gov/research-priorities/research-needs-and-gaps/pathways-prevention/improving-rural-health-through-telehealth-guided-provider-provider-communication
- 3. Tsou C, Robinson S, Boyd J, et al. Effectiveness of Telehealth in Rural and Remote Emergency Departments: Systematic Review. J Med Internet Res. 2021;23(11):e30632. doi:10.2196/30632 [DOI] [PMC free article] [PubMed]
- 4. Charlton M, Schlichting J, Chioreso C, Ward M, Vikas P. Challenges of Rural Cancer Care in the United States. Oncology. 2015;29(9):633-640. [PubMed]
- 5. Marcin JP, Shaikh U, Steinhorn RH. Addressing health disparities in rural communities using telehealth. Pediatr Res. 2016;79(1-2):169-176. doi:10.1038/pr.2015.192 [DOI] [PubMed]
- 6. Amadi-Obi A, Gilligan P, Owens N, O’Donnell C. Telemedicine in pre-hospital care: A review of telemedicine applications in the pre-hospital environment. Int J Emerg Med. 2014;7(1):29. doi:10.1186/s12245-014-0029-0 [DOI] [PMC free article] [PubMed]
- 7. Sharma R, Fleischut P, Barchi D. Telemedicine and its transformation of emergency care: A case study of one of the largest US integrated healthcare delivery systems. Int J Emerg Med. 2017;10(1):21. doi:10.1186/s12245-017-0146-7 [DOI] [PMC free article] [PubMed]
- 8. Greenwald P, Stern ME, Clark S, Sharma R. Older adults and technology: in telehealth, they may not be who you think they are. Int J Emerg Med. 2018;11(1). doi:10.1186/s12245-017-0162-7 [DOI] [PMC free article] [PubMed]
- 9. Sheets LR, Wallach E, Khairat S, Mutrux R, Edison K, Becevic M. Similarities and Differences Between Rural and Urban Telemedicine Utilization. Perspectives in health information management. 2020;18(Winter):1e. [PMC free article] [PubMed]
- 10. Board on Health Care Services, Institute of Medicine. The Role of Telehealth in an Evolving Health Care Environment: Workshop Summary. In: The Evolution of Telehealth: Where Have We Been and Where Are We Going?. National Academies Press (US); 2012. https://www.ncbi.nlm.nih.gov/books/NBK207141 [PubMed]