

Abstract
Case summary
An adult male neutered Russian Blue cat presented for a right-sided nasal mass with bilateral retropharyngeal and right mandibular lymphadenomegaly. Medial retropharyngeal lymph node excision with nasal mass biopsy revealed eosinophilic sclerosing lymphadenitis and eosinophilic and lymphoplasmacytic rhinitis, respectively. Bacterial culture of the lymph node grew Pseudomonas aeruginosa, and treatment with pradofloxacin was started. Despite initial improvement, clinical signs recurred after 9 months, and fine-needle aspirates of the right mandibular and left medial retropharyngeal lymph nodes showed eosinophilic and mastocytic infiltration. Bacterial culture of the left medial retropharyngeal lymph node grew P aeruginosa, and treatment with anti-inflammatory doses of prednisolone and, later, marbofloxacin was instituted.
Relevance and novel information
This report describes a case of feline eosinophilic sclerosing lymphadenitis diagnosed outside of the abdominal cavity and is the first case reported to be associated with P aeruginosa. Feline eosinophilic sclerosing lymphadenitis should be considered as a differential for lymphadenopathy occurring in areas other than the abdominal cavity. Feline eosinophilic sclerosing lymphadenitis may develop in cats due to a species-specific inflammatory response to chronic bacterial and fungal infections.
Keywords: Lymphadenopathy, lymphadenitis, eosinophilic sclerosing fibroplasia, Pseudomonas, eosinophilic enteritis
Introduction
Feline gastrointestinal eosinophilic sclerosing fibroplasia (FGESF) is an inflammatory condition that most commonly affects the gastrointestinal tract and associated lymph nodes.1,2 Recent reports have characterized lesions within the abdominal cavity but outside of the gastrointestinal tract, including multifocal mesenteric nodules and a retroperitoneal mass.3,4 Histopathologic characteristics of FGESF include eosinophilic inflammation, dense sclerotic collagen and numerous fibroblasts.1,5 The underlying cause is unknown; lesions have been reported in the presence of concurrent bacterial and fungal infections, and idiopathic immunological dysregulation has been hypothesized to contribute to the etiology of FGESF.1,2,6–8 Treatment with prednisolone has been shown to significantly improve survival time, but a multimodal approach involving prednisolone, antibiotics and immunomodulatory agents is recommended, owing to the undefined pathogenesis and variety of treatment regimens reported.1–3 This report details an extra-abdominal presentation of eosinophilic sclerosing lymphadenitis, and the first case associated with Pseudomonas aeruginosa.
Case description
A 6-year-old male neutered Russian Blue cat presented for a 1-year history of progressive abnormal respiratory noises, sneezing, nasal discharge and chronic right corneal changes and ocular discharge. A head CT had been performed prior to presentation, which revealed a right-sided nasal mass with bilateral retropharyngeal and right mandibular lymphadenomegaly. Treatment with famciclovir had diminished sneezing, but the remainder of the clinical signs had progressed despite reported treatment with chlorpheniramine, azithromycin and prednisolone. The cat had previously received a tapering course of prednisolone 2 years prior (0.3 mg/kg PO q12h for 2 days; 0.3 mg/kg PO q24h for 5 days; and 0.3 mg/kg PO q48h for 5 days). Physical examination revealed chronic corneal changes of the right eye with neovascularization secondary to an injury at least 5 years prior and rotary nystagmus. The cat was mildly stridorous and stertorous, with decreased airflow through the right nostril and visible nostril flare. The right retropharyngeal lymph node was palpably enlarged and firm at approximately 3 cm in diameter. The right submandibular lymph node was also mildly enlarged and firm. The cat had mildly increased bronchovesicular sounds and a grade I–II/VI heart murmur on auscultation.
A visually reviewed complete blood count (CBC) revealed a normal eosinophil number at 1.16 × 103/µl (reference interval [RI] 0.10–1.80 × 103/µl [Advia2120i; Siemens Healthcare Diagnostics]). A chemistry panel was performed prior to referral, and showed mild hyperglycemia at 174 mg/dl (RI 74–159 mg/dl [IDEXX VetLab Station]). Abdominal ultrasound revealed a mildly hypoechoic mottled liver, mild cecal thickening with mild ileocecal/colic and pancreaticoduodenal lymphadenopathy, and bladder sediment/grit. A fine-needle aspirate of the right retropharyngeal lymph node showed reactive lymphoid hyperplasia with a mild mastocytic component and moderate eosinophilic component (Figure 1). PCR for antigen receptor rearrangements of cytology samples was performed and no evidence of clonality was demonstrated. Owing to suspicion for neoplasia, right medial retropharyngeal lymph node excision and nasal mass biopsy were pursued.
Figure 1.
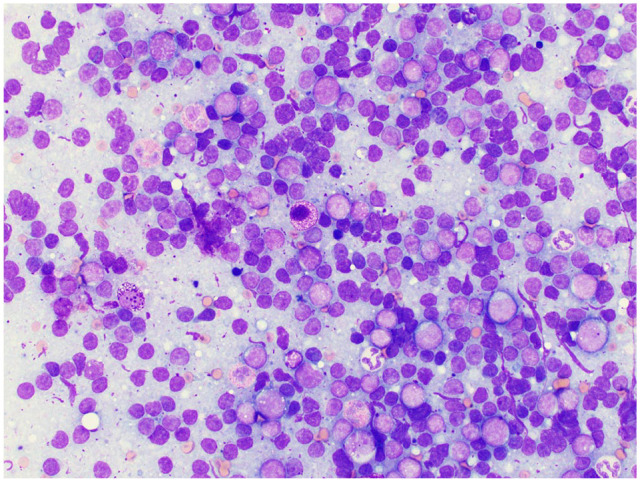
Photomicrograph of a fine-needle aspirate smear from the right retropharyngeal lymph node. The sample consists of a mixed lymphocyte population with scattered mast cells and eosinophils. Wright–Giemsa stain × 50 oil objective
Histopathology of the lymph node revealed marked chronic regionally extensive eosinophilic sclerosing lymphadenitis. The normal lymph node architecture was largely effaced by anastomosing bands of sclerotic collagen interrupted by multiple foci of necrosis surrounded by large numbers of neutrophils, macrophages, cellular debris, eosinophils and lymphocytes (Figure 2). The necrotic centers contained small numbers of bacteria, necrotic cells and cellular debris. Moderate numbers of eosinophils, neutrophils and macrophages, as well as fewer mast cells, lymphocytes and plasma cells, were noted between the collagen bands and expanding the adjacent lymph node parenchyma. The biopsies from the right nasal cavity were consistent with marked chronic diffuse eosinophilic and lymphoplasmacytic rhinitis. Aerobic and anaerobic cultures were performed of the lymph node tissue. Aerobic culture grew P aeruginosa; anaerobic culture exhibited no bacterial growth. The cat was started on pradofloxacin (7.5 mg/kg PO q24h [Veraflox; Bayer]) for 7 days.
Figure 2.
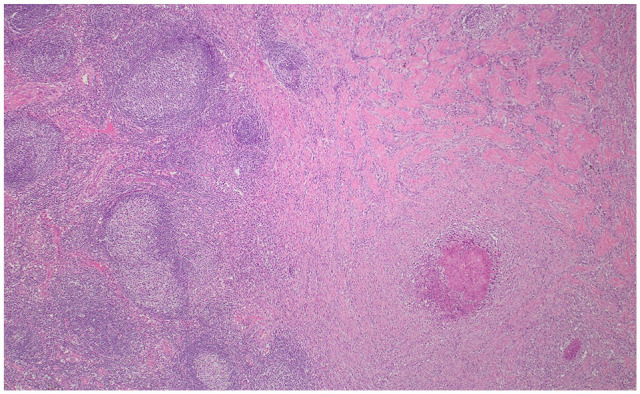
Histology of the right retropharyngeal lymph node demonstrating dense bands of sclerotic collagen interrupted by a focus of necrosis with intermixed eosinophils, macrophages, neutrophils and lymphocytes (× 10 magnification)
The cat was initially lost to follow-up, but then returned 282 days later for progressive respiratory signs, right-sided nasal discharge and a left-sided cervical mass. On physical examination, the cat had no airflow through the right nostril. The left medial retropharyngeal lymph node was severely enlarged and firm; the right mandibular lymph node was bilobed, enlarged and firm on palpation. A CBC showed a non-regenerative, normocytic, normochromic anemia of 23.3% (31–48%) and normal eosinophil count of 1.21 × 103/µl (RI 0.10–1.80 × 103/µl. A chemistry panel demonstrated mild hypermagnesemia at 2.7 mg/dl (RI 1.9–2.6 mg/dl [Vitros-4600; Ortho Clinical Diagnostics]). Cervical ultrasound confirmed severe left medial retropharyngeal lymphadenopathy (1.6 × 1.7 × 4.7 cm) and moderate right mandibular lymphadenopathy (7.8 mm diameter). The laryngeal cartilages were displaced axially and were asymmetrically heterogeneously hypoechoic, prioritized to be artifactual secondary to asymmetric position. Thoracic radiographs were performed under deep sedation following ultrasound, and revealed possible sternal lymphadenopathy and atelectasis of the right lung lobe, suspected to be secondary to anesthesia and recumbency.
Ultrasound-guided aspirates of the left retropharyngeal lymph node revealed reactive lymphoid hyperplasia with a moderate eosinophilic and mild mastocytic infiltrate. The right mandibular lymph node demonstrated atypical lymphoid hyperplasia with a mild eosinophilic and mastocytic infiltrate. Owing to concern for recurrent eosinophilic sclerosing lymphadenitis based on the prior histopathologic diagnosis, the cat was started on prednisolone (0.7 mg/kg PO q24h [PrednisTab; Lloyd]) and amoxicillin and clavulanate potassium (18 mg/kg PO q12h [Clavamox; Zoetis]) for 2 weeks pending culture results. Aerobic culture from the aspirate of the left retropharyngeal lymph node again grew P aeruginosa. Antibiotics were not adjusted based on culture owing to the initially reported clinical improvement.
The cat presented for re-evaluation 2 months later after completing the course of prednisolone. After discontinuing corticosteroids 2–3 weeks prior to evaluation, the cat developed a recurrence of upper respiratory noise and onset of frequent vomiting. Physical examination revealed an enlarged, firm left medial retropharyngeal lymph node. The cat was started on marbofloxacin (3.9 mg/kg PO q24h [Zeniquin; Zoetis]) for 3 weeks and then instructed to restart prednisolone (0.75 mg/kg PO q24h) once it had received 2 weeks of antibiotics. The cat initially responded well to therapy, but after 6 months, the sneezing, nasal discharge and lymph node swelling recurred. The cat was restarted on a tapering course of prednisolone and a 2-week course of marbofloxacin at that time by the referring veterinarian and demonstrated a rapid clinical response.
Discussion
This case details the novel identification of feline eosinophilic sclerosing fibroplasia involving the retropharyngeal lymph nodes associated with P aeruginosa. FGESF most commonly presents as a firm abdominal mass in the cranial and/or mid-gastrointestinal tract affecting the pylorus or ileocecocolic junction with or without mesenteric lymph node involvement.1,2 Additional cases have been documented outside the gastrointestinal tract but within the abdominal cavity.3,4,8 Prior to the naming of FGESF in 2009 by Craig et al, 1 similar lesions were described in cervical and mesenteric lymph nodes, subcutaneous tissues and the abdominal cavity of cats. 8 Similar to the present case, the lymph nodes in that study had abscesses with a necrotic center containing bacteria and eosinophils surrounded by maturing granulation tissue. 8 However, dissimilarly, the majority of the lymph nodes examined contained bacterial cocci, and while culture was only performed on 2/27 cervical lymph nodes, both grew methicillin-resistant Staphylococcus species. 8 Bacteria were observed on histopathology in the necrotic centers with in the right retropharyngeal lymph node of the cat in this case report, and P aeruginosa was cultured without growth of Staphylococcus species.
Bacteria have been noted in over 50% of cases of FGESF.1,2,7 However, therapy with prednisolone – and not antibiotic treatment – has been associated with significantly improved survival times.1,2 This cat was initially treated with pradofloxacin following culture results with no reported improvement, and eventual progression was noted with suspected recurrence of disease in the cervical lymph node chain. Marked improvement was noted after starting prednisolone concurrently with the antibiotics, with relapse noted after discontinuation of corticosteroids and no change documented after stopping antibiotic therapy. Given the multimodal therapeutic regimen required to treat this condition, including the use of corticosteroids, and that other important eosinophil-rich diseases occur in cats (ie, eosinophilic granuloma complex and eosinophilic enteritis), feline eosinophilic sclerosing lymphadenitis may represent yet another manifestation of species-specific inflammatory response to chronic bacterial infections and other infectious entities. 9 This process could indicate an overexuberant reaction to antigenic stimulation in cats that results in an eosinophilic infiltrate and fibrosis requiring a combination of antibiotic and immune-modulatory therapy to address this disease due to the lack of resolution seen with antibiotic therapy alone.
Cats exhibit eosinophil-rich inflammation in several disease entities, some with better-defined etiologies and others without. For example, feline eosinophilic enteritis is a relatively common inflammatory disease in cats characterized by eosinophilic inflammation within the mucosa and well-described ultrasonographic features, but for which a specific underlying etiology is unknown. 10 With eosinophilic granuloma complex, a number of possible etiologies have been suggested, and some studies have demonstrated an underlying bacterial etiology, though other studies have demonstrated a correlation with allergic skin diseases. 11 Additionally, in a little over half of FGESF cases, a bacterial cause has been found,1,2 and, importantly, bacteria were detected on histopathology and by culture in the case presented here. Taken together, this body of literature suggests that the eosinophilic inflammation seen in cats can not only be in response to bacteria, but can also be a stereotypic response to a number of different etiologies.1,2,6,9,11
Eosinophilic sclerosing lymphadenitis has been described in conjunction with inflammation in the gastrointestinal tract (ie, FGESF), 1 , 2 , 8 and also with eosinophilic inflammation and abscesses in subcutaneous tissues. 8 Additionally, aberrant expression of metalloproteinases – enzymes important in matrix remodeling during healing – have been demonstrated in feline eosinophilic inflammatory disease. 12 This suggests that the inflammatory mediators associated with eosinophil-rich disease processes in cats could drive remodeling of lymph node stroma, resulting in sclerosis of the matrix and enlargement of the lymph node grossly, as is seen in many of these entities and as was seen in this case. However, eosinophilic activity likely only plays a partial role as concurrent cytokines, lipid mediators, complement fragments and other associated immunomodulatory agents are released concurrently. 9 Additionally, the duration of the disease process may affect the exact histopathologic changes noted given the time needed to see fibrosis of these lesions. The histologic commonalities and the response to immunomodulatory therapy for eosinophilic sclerosing fibroplasia/lymphadenitis and other eosinophilic inflammatory diseases in cats support the previous hypothesis of a possible unique exuberant inflammatory reaction to bacterial and other infections in this species.1,6 Characterization of tissue-specific inflammatory mediators and matrix protein expression in cases of eosinophilic sclerosing fibroplasia (in the lymph nodes and other tissues) with known etiologies would help to better define the pathogenesis of this disease.
Conclusions
This report details a cat with eosinophilic sclerosing lymphadenitis in the retropharyngeal and mandibular lymph nodes, with histological findings similar to those described in FGESF and in some subcutaneous abscesses.1,2,8 This entity should therefore be included as a differential diagnosis in cases of lymph node enlargement with eosinophilic infiltrates at extra-abdominal sites. Thus, we propose a more inclusive name of ‘feline eosinophilic sclerosing fibroplasia (FESF)’ as a term to describe lesions that have a marked eosinophilic infiltrate and associated deposition of dense collagen. This term would include entities such as FGESF as a sub-classification, and other less well-defined lesions that exhibit these histopathologic changes. While Gram-negative bacteria have been identified previously in lesions within the gastrointestinal tract, 1 this is the first report of a case associated with the growth of P aeruginosa. Although associated with a confirmed infection of P aeruginosa, improvement was not noted with antibiotic therapy alone, documenting the importance of immunomodulatory therapy and supporting the consideration that this process could be a species-specific inflammatory reaction to chronic bacterial infections in cats.
Footnotes
Accepted: 15 July 2022
Conflict of interest: The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval: This work involved the use of non-experimental animals only (including owned or unowned animals and data from prospective or retrospective studies). Established internationally recognised high standards (‘best practice’) of individual veterinary clinical patient care were followed. Ethical approval from a committee was therefore not specifically required for publication in JFMS Open Reports.
Informed consent: Informed consent (either verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (either experimental or non-experimental animals) for the procedure(s) undertaken (either prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.
ORCID iD: Bianca Zampieri  https://orcid.org/0000-0001-8086-8675
https://orcid.org/0000-0001-8086-8675
References
- 1. Craig LE, Hardam EE, Hertzke DM, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia. Vet Pathol 2009; 46: 63–70. [DOI] [PubMed] [Google Scholar]
- 2. Linton M, Nimmo JS, Norris JM, et al. Feline gastrointestinal eosinophilic sclerosing fibroplasia: 13 cases and review of an emerging clinical entity. J Feline Med Surg 2015; 17: 392–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Kambe N, Okabe R, Osada H, et al. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia limited to the mesentery. J Small Anim Pract 2020; 61: 64–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Thieme ME, Olsen AM, Woolcock AD, et al. Diagnosis and management of a case of retroperitoneal eosinophilic sclerosing fibroplasia in a cat. JFMS Open Rep 2019. DOI: 10.1177/2055116919867178. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Sihvo HK, Simola OT, Vainionpää MH, et al. Pathology in practice. Severe chronic multifocal intramural fibrosing and eosinophilic enteritis, with occasional intralesional bacteria, consistent with feline gastrointestinal eosinophilic sclerosing fibroplasia. (FIESF). J Am Vet Med Assoc 2011; 238: 585–587. [DOI] [PubMed] [Google Scholar]
- 6. Grau-Roma L, Galindo-Cardiel I, Isidoro-Ayza M, et al. A case of feline gastrointestinal eosinophilic sclerosing fibroplasia associated with phycomycetes. J Comp Pathol 2014; 151: 318–321. [DOI] [PubMed] [Google Scholar]
- 7. Weissman A, Penninck D, Webster C, et al. Ultrasonographic and clinicopathological features of feline gastrointestinal eosinophilic sclerosing fibroplasia in four cats. J Feline Med Surg 2013; 15: 148–154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Ozaki K, Yamagami T, Nomura K, et al. Abscess-forming inflammatory granulation tissue with Gram-positive cocci and prominent eosinophil infiltration in cats: possible infection of methicillin-resistant Staphylococcus. Vet Pathol 2003; 40: 283–287. [DOI] [PubMed] [Google Scholar]
- 9. Bloom PB. Canine and feline eosinophilic skin diseases. Vet Clin North Am Small Anim Pract 2006; 36: 141–160. [DOI] [PubMed] [Google Scholar]
- 10. Tucker S, Penninck DG, Keating JH, et al. Clinicopathological and ultrasonographic features of cats with eosinophilic enteritis. J Feline Med Surg 2014; 16: 950–956. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Buckley L, Nuttall T. Feline eosinophilic granuloma complex(ities): some clinical clarification. J Feline Med Surg 2012; 14: 471–481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Porcellato I, Giontella A, Mechelli L, et al. Feline eosinophilic dermatoses: a retrospective immunohistochemical and ultrastructural study of extracellular matrix remodelling. Vet Dermatol 2014; 25: 86–94. [DOI] [PubMed] [Google Scholar]