

Abstract
Background:
Social anxiety is amongst the most prevalent adolescent mental health problems; however, it is often unrecognized due to its comorbidity with other anxiety problems such as generalized anxiety (Kashdan & Herbert, 2001). Thus, understanding the unique developmental pathways to social anxiety is critical for improving its prevention. We examined the pathway from maternal shyness, when children were 4 years old, to adolescents’ social anxiety at age 15 through social wariness at age 7. We hypothesized that childhood social wariness would mediate the association between maternal shyness and social anxiety in adolescence.
Methods:
Participants (N=291; 54% female) were followed from early childhood to adolescence. Mothers reported on their own shyness when children were 4 years old. Social wariness toward unfamiliar peers was observed in the laboratory at ages 4 and 7. Adolescent social anxiety and generalized anxiety were assessed via self-report, parent-report and clinical diagnoses at age 15.
Results:
Maternal shyness was positively associated with adolescent social anxiety but not generalized anxiety at age 15. Higher levels of maternal shyness at age 4 predicted greater social wariness at age 7, which in turn predicted greater social anxiety but not generalized anxiety at age 15. Social wariness at age 7 partially mediated the association between maternal shyness and adolescent social anxiety.
Conclusions:
This study identifies a unique developmental pathway from maternal shyness to adolescent social anxiety. Findings suggest that childhood social wariness connects maternal shyness to adolescent social anxiety.
Keywords: Maternal shyness, temperament, social wariness, social anxiety, generalized anxiety
Introduction
Social anxiety disorder is amongst the most prevalent adolescent mental health disorders (Beesdo, Knappe, & Pine, 2009). Although social anxiety predicts subsequent problems (Burstein et al., 2011; de Lijster et al., 2018), it is often unrecognized, possibly due to comorbidity with other anxiety disorders such as generalized anxiety (Kashdan & Herbert, 2001). Despite their comorbidity, there is evidence showing that social anxiety and generalized anxiety are distinguishable and may predict differential outcomes (Pine 2007). Consistent with evidence of neural distinctions between fears of social and non-social stimuli (Gross & Canteras, 2012; Silva et al., 2013), social and generalized anxiety disorders show differential patterns of neural responding to fear-relevant stimuli (Blair et al., 2008; Kessel et al., 2015). Given the evidence that social anxiety is partially dissociable from generalized anxiety, it is important to examine developmental pathways into one or the other problem to inform prevention strategies.
Few longitudinal studies examine pathways leading to adolescent social or generalized anxiety disorder involving caregiver characteristics and early childhood behaviors quantified with both parent-report and direct observation. The scarcity of such research contrasts with extensive studies on developmental pathways leading to adolescent behavioral problems (e.g., Côté et al., 2006; Lahey et al., 2008; Murray & Farrington, 2010). The current study seeks to address this gap by considering whether maternal shyness uniquely predicts social as opposed to generalized anxiety in mid-adolescence through associations with social wariness in childhood.
Shyness is a broad construct referring to the tendency to experience discomfort, tension, and awkwardness in social situations involving unfamiliar people (Cheek & Buss, 1981). Previous work suggests that maternal shyness contributes to adolescent social anxiety at least partially through shared heritability, given the potential genetic overlap between shyness and anxiety (Eley et al., 2003) and the modest-to-high levels of heritability of these traits (Eley et al., 2015; Smith et al., 2012). However, maternal shyness may also influence parental socialization (Rickman & Davidson, 1994) that influences children through observational learning (Clément & Dukes, 2017; Olsson & Phelps, 2007). Likewise, mothers high in shyness may reinforce children’s shy or wary behaviors (Hastings, Nuselovici, Rubin, Cheah, 2010; Root, Hastings, & Rubin, 2016); provide negative information about social situations (Muris, van Zwol, Huijding, & Mayer, 2010), and/or provide limited opportunities to their children to socialize (Bögels et al., 2001; Rickman & Davidson, 1994). Few studies examine longitudinal relations between maternal shyness in early childhood and social anxiety in adolescence. However, cross-sectional studies find that maternal shyness is associated with shyness in infancy (Daniels & Plomin, 1985) and when children are 6-, but not 4-years old (MacGowan & Schmidt, 2020). Nevertheless, these studies rely only on mother-report data, which could produce associations through reporter bias or shared method variance. Thus, longitudinal multi-informant work is needed.
Maternal shyness may transmit risk for adolescents’ social anxiety through an early-childhood phase of social wariness. Social wariness relates to the broader construct of shyness. However, whereas shyness refers broadly to a person’s characteristics in many settings, the term social wariness has been used more narrowly to refer to inhibited and disengaged behaviors rated by an experimenter in novel laboratory situations. Social wariness is typically operationalized as expression of these behaviors during laboratory-based social interaction episodes involving unfamiliar peers (Buss et al., 2013; Degnan, Henderson, Fox, & Rubin, 2008). Previous work has suggested that wary and inhibited behaviors predict extreme fear of social performance and interactions, leading to social anxiety (Neal, Edelmann, & Glachan, 2002; Rapee & Spence, 2004). However, other work finds that parental reports of children’s shyness predict both adolescent social and generalized anxiety (Prior, Smart, Sanson, & Oberklaid, 2000). Likewise, recalled childhood shyness has also been linked with adults’ current levels of generalized anxiety (Neal et al., 2002). Thus, it remains unclear whether childhood laboratory-evoked social wariness explains unique variance in both adolescents’ social anxiety and generalized anxiety.
The current study examines whether maternal shyness predicts social anxiety in adolescence through increases in laboratory-evoked social wariness in childhood. Given the comorbidity in symptoms of anxiety subtypes, it is important to understand the specificity of effects from parental and child characteristics to adolescent social and generalized anxiety (Murray, Cresswell, & Cooper, 2009). This research would elucidate pathways to specific types of anxiety, informing future research characterizing how exposure to distinct fear-relevant experiences may shape the differential pathways to social and generalized anxiety, and the development of differential neural responding patterns. Likewise, evidence supporting specificity may provide support for the utility of developing fine-grained early identification and prevention strategies informed by the unique etiological courses of these anxieties.
We assessed maternal shyness when children were 4 years old, observed children’s social wariness with unfamiliar peers in a laboratory setting at ages 4 and 7, and conducted a multi-method assessment of adolescents’ social anxiety and generalized anxiety at age 15 consisting of diagnostic interviews, and adolescent- and parent-report of symptoms. Using structural equation modeling, we first constructed two latent variables for social anxiety and generalized anxiety. Next, we examined the direct and indirect pathways from maternal shyness at age 4 to social anxiety and generalized anxiety at age 15 through social wariness at age 7. We hypothesized that (a) maternal shyness would positively predict adolescent social anxiety but not necessarily generalized anxiety at age 15, (b) maternal shyness assessed when the child was age 4 would predict child social wariness at age 7, controlling for child social wariness at age 4, (c) social wariness at age 7 would predict adolescent social anxiety but not generalized anxiety at age 15, and (d) social wariness at age 7 would partially mediate the association between maternal shyness at age 4 and adolescent social anxiety at age 15.
Methods
Participants
Participants were from an ongoing longitudinal study and included 291 children (156 female), selected in infancy based on displays of positive and negative affect. Mothers were 69.4% White, 16.5% African American, 7.2% Hispanic, 3.1% Asian, 3.4% other, and 0.3% missing, with 35.7% as graduate school graduates, 41.9% as college graduates, 16.2% as high school graduates, 5.5% with other forms of education, and 0.7% were missing.
Of the original sample (N=291), 244 families provided data for maternal shyness at 4 years, 175 for social wariness at 7 years, 162 for adolescent self-report of social anxiety, 178 for parent-report of adolescent social anxiety, and 151 for clinical diagnosis of social anxiety. Examining the pattern of missing data revealed mother’s race/ethnicity was associated with missing data on maternal shyness, χ2(1) = 7.90, p = .005, and marginally associated with parent report of adolescent anxiety, χ2(1) = 3.39, p = .066, and adolescent self-report of anxiety, χ2(1) = 3.39, p = .066, such that children with data on these measures were more likely to have non-Hispanic, White mothers. Because of this, maternal ethnicity was included as a covariate in the primary analyses. Missing data on all other variables was not associated with children’s gender, mother’s ethnicity or maternal education, p’s > .05.
Procedures
We utilized data from the mothers’ report of their own shyness at 4 years, laboratory-based social wariness assessments at 4 and 7 years, mother and adolescent reports of social generalized anxiety at 15 years, and data from clinical diagnostic interviews conducted at 15 years. Mothers received monetary compensation and children picked a gift for participation at each time point. All procedures were approved by the Institutional Review Board of the University of Maryland. Signed consent was obtained from each child’s legal guardian prior to each assessment, and verbal or written assent was obtained from child participants.
Measures
Maternal Shyness (4 years).
Mothers provided self-report on the shyness scale (13 items) of The Revised Cheek & Buss Shyness Scale (Cheek & Buss, 1981). Internal consistency in our sample was strong (α=.85). This scale has good test-retest reliability and convergent validity with other measures of shyness (Hopko, Stowell, Jones, Armento, & Cheek, 2005). Items were summed, with greater values indicating greater maternal shyness.
Child Social Wariness (4 and 7 years).
At the 4- and 7-year assessments, child social wariness was observed in the laboratory during an unstructured free play task with an unfamiliar, same-age, same-sex peer recruited from the community. Trained coders rated children’s wariness, reflecting a hesitancy to play and fearful behavior toward the peer, as well as unfocused/disengaged behavior on a 1 to 7 scale with good inter-rater reliability (Degnan et al., 2008). Wariness and unfocused/disengaged scores were positively correlated at both assessments, r = .28 - .31, p < .001, and were averaged to create the social wariness variable for each time point. Higher values indicated greater laboratory-evoked child social wariness.
Mothers also completed the Child Behavior Questionnaire’s shyness scale at ages 4 and 7 (Putnam & Rothbart, 2006). Observed social wariness and mother-reported child shyness were positively correlated both at age 4 (r = .22, p = .002), and age 7 (r = .37, p < .001), suggesting that our laboratory evoked social wariness measure showed concurrent validity. For sensitivity analyses, we also created a composite including both in-lab and mother-report assessments (i.e., average of the standardized scores of observed social wariness and mother-report of shyness), which provided a comprehensive assessment of children’s shy and wary behaviors across multiple settings.
Adolescent Social Anxiety and Generalized Anxiety (15 years).
At the 15-year assessment, social anxiety and generalized anxiety were both assessed via: (a) adolescent self-report, (b) parent-report, and (c) clinical diagnosis. Adolescents and mothers completed the social phobia (7 items) and the generalized anxiety (9 items) scales of the Screen for Child Anxiety Related Emotional Disorders (Birmaher et al., 1999; SCARED). Both scales had strong internal consistency in our sample (social anxiety scale: α = .89 for child-report, α =.91 for parent-report; generalized anxiety scale: α =.87 for child-report, α =.89 for parent-report). Previous research showed these scales to have good discriminant validity, test-retest reliability, and moderate adolescent-mother agreement (Birmaher et al., 1997). Items were summed such that higher scores indicated greater anxiety.
Clinicians conducted semi-structured diagnostic interviews with parents and adolescents using the Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children (KSADS; Kaufman et al., 1997). All clinicians were trained and supervised by senior clinicians (ACT and DP), who confirmed all diagnoses. Audio recordings were taken of each interview and interviews were reviewed for reliability. Reliability for anxiety interviews was high (k=.91). Among the 151 adolescents evaluated, 24 met criteria for current presence of social anxiety disorder, 20 met criteria for generalized anxiety disorder, and 8 participants met criteria for both.
Data Analysis
A structural equation model was conducted in Mplus (Version 8; Muthén & Muthén, 2012) using two broad latent factors: one for social anxiety and one for generalized anxiety at age 15. Each latent variable included three indicators: adolescent-report, parent-report, and clinical diagnosis of the respective type of anxiety. We allowed the factors to correlate and covaried residuals of the same measures (e.g., parent report). Maternal shyness at 4 years was specified as a predictor of social wariness at 7 years and adolescent social anxiety at 15 years. Social wariness at 7 years was specified as a predictor of adolescent social anxiety and generalized anxiety at 15 years. To check the robustness of our results, we also conducted this model using a more comprehensive score including in-lab and mother-report assessments. Testing this additional model allowed us to determine whether a broader child shyness construct yielded similar results.
Based on the preliminary analyses described below with covariates and missing patterns and in line with previous studies with this sample (Zeytinoglu et al., 2021), we controlled for maternal education, maternal ethnicity, and gender on the main outcomes and any variable that showed a zero-order correlation with these covariates. We used full information maximum likelihood estimation to handle missing data to reduce potential bias in the parameter estimates (Enders & Bandalos, 2001). This permitted the inclusion of all participants with data on one or more variables. Due to missing data, potential departures from multivariate normality, and inclusion of categorical indicators in the latent variables (i.e., clinical diagnosis of anxiety), we used weighted least square mean and variance adjusted estimation, which is a maximum likelihood estimation with robust standard errors to correct skewness (Muthén & Muthén, 2012). Model fit was evaluated using the chi-square test of model fit, comparative fit index (CFI), and root-mean-square error of approximation (RMSEA). Finally, a bias-corrected bootstrapping procedure (5,000 draws) was used in estimating confidence intervals for indirect effects as this procedure has been shown to increase accuracy, reducing Type I error rates (MacKinnon, Lockwood, & Williams, 2004).
Results
Descriptive Statistics
Descriptive statistics and correlations of all study variables are presented in Table 1. Compared to boys, girls demonstrated greater social wariness at 7 years, reported greater social anxiety and generalized anxiety at 15 years, and were reported by their parents to have greater social anxiety and generalized anxiety at 15 years. Maternal ethnicity was associated with social wariness at 4 years, such that children of non-Hispanic, White mothers were less socially wary than children of non-White and/or Hispanic mothers. Higher maternal education was associated with greater child social wariness at 4 years. Thus, gender, maternal ethnicity, and maternal education were included as covariates in the primary model.
Table 1.
Descriptive information on the study variables
| Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | Gender (0=female) | – | – | – | ||||||||||
| 2. | Mother ethnicity (0=non-Hispanic, White) | – | – | .05 | – | |||||||||
| 3. | Maternal education | – | – | .01 | −.19** | – | ||||||||
| 4. | Maternal shyness, 4 years | 13.54 | 8.16 | −.01 | .05 | −.09 | – | |||||||
| 5. | Child social wariness, 4 years | 2.09 | .65 | .06 | −.19** | .17* | .10 | – | ||||||
| 6. | Child social wariness, 7 years | 1.92 | .65 | −.22** | .11 | −.13 | .25** | .06 | – | |||||
| 7. | Adolescent-reported social anxiety, 15 years | 5.58 | 3.80 | −.31** | .09 | −.14 | .25** | .07 | .36** | – | ||||
| 8. | Parent-reported social anxiety, 15 years | 3.81 | 3.65 | −.26** | −.06 | −.15 | .28** | .10 | .25** | .55** | – | |||
| 9. | Diagnosis of social anxiety (1=yes), 15 years | – | – | −.09 | −.11 | −.07 | .08 | .06 | .26** | .43** | .34** | – | ||
| 10. | Adolescent-reported anxiety, 15 years | 7.64 | 4.42 | −.28** | −.11 | −.07 | .18* | .02 | .12 | .52** | .27** | .23* | – | |
| 11. | Parent-reported anxiety, 15 years | 4.38 | 3.98 | −.20** | −.14 | −.10 | .08 | .12 | .03 | .39** | .60** | .33** | .41** | – |
| 12. | Diagnosis of generalized anxiety (1=yes), 15 years | – | – | −.07 | −.07 | −.01 | −.05 | .09 | .06 | .33** | .21* | .26** | .40** | .49** |
Note. N = 151-291.
p < .05
p < .01
p < .005.
Primary Analyses
The model fit was excellent: χ2 (36) = 38.31, p = .37; RMSEA = .02 [90% CI = .00 – .05]; and CFI = .99. Unstandardized path coefficients are reported in Table 2. Standardized path coefficients among the study variables are presented in Figure 1. As shown in Figure 1, all indicators loaded well on the intended latent constructs of adolescent social anxiety and generalized anxiety. Adolescent social anxiety and generalized anxiety at 15 years were positively associated, such that those who were higher in social anxiety were also higher in generalized anxiety. Maternal shyness at 4 years was positively related to child social wariness at 4 years and positively predicted child social wariness at 7 years, controlling for social wariness at 4 years. Maternal shyness at 4 years and child social wariness at 7 years positively predicted adolescents’ social anxiety, but not generalized anxiety, at 15 years, suggesting that maternal shyness and child social wariness were unique predictors of adolescent social anxiety. The indirect effect from maternal shyness at 4 years to adolescent social anxiety at 15 years through social wariness at 7 years was significant, β = .07, 95% CI [.005, .141]; B = .03, 95% Bootstrap CI [.002, .057]. These results suggest that childhood social wariness partially mediated the pathway between maternal shyness and adolescent social anxiety.
Table 2.
Unstandardized estimates of the paths in the structural equation model
| Outcome/Predictors | B | SE | CI Lower | CI Upper | p |
|---|---|---|---|---|---|
| Social Anxiety, 15 years | |||||
| Maternal Shyness, 4 years | 0.10 | 0.04 | 0.022 | 0.176 | 0.011 |
| Social Wariness, 7 years | 1.35 | 0.51 | 0.352 | 2.349 | 0.008 |
| Gender | −1.83 | 0.55 | −2.916 | −0.740 | 0.001 |
| Maternal Ethnicity | −0.63 | 0.63 | −1.865 | 0.600 | 0.315 |
| Maternal Education | −0.78 | 0.41 | −1.591 | 0.033 | 0.060 |
| Generalized Anxiety, 15 years | |||||
| Maternal Shyness, 4 years | 0.06 | 0.04 | −0.015 | 0.142 | 0.113 |
| Social Wariness, 7 years | 0.04 | 0.59 | −1.108 | 1.195 | 0.941 |
| Gender | −1.78 | 0.60 | −2.962 | −0.603 | 0.003 |
| Maternal Ethnicity | −1.53 | 0.68 | −2.866 | −0.201 | 0.024 |
| Maternal Education | −0.55 | 0.39 | −1.301 | 0.212 | 0.158 |
| Social Wariness, 7 years | |||||
| Maternal Shyness, 4 years | 0.02 | 0.01 | 0.010 | 0.032 | 0.000 |
| Social Wariness, 4 years | 0.01 | 0.06 | −0.115 | 0.133 | 0.886 |
| Gender | −0.29 | 0.11 | −0.498 | −0.083 | 0.006 |
| Social Wariness, 4 years | |||||
| Maternal Ethnicity | −0.28 | 0.09 | −0.460 | −0.096 | 0.003 |
| Maternal Education | 0.08 | 0.08 | −0.067 | 0.228 | 0.283 |
| Maternal Shyness, 4 years | |||||
| Maternal Ethnicity | 1.86 | 1.17 | −0.429 | 4.152 | 0.111 |
N=291.
Figure 1.
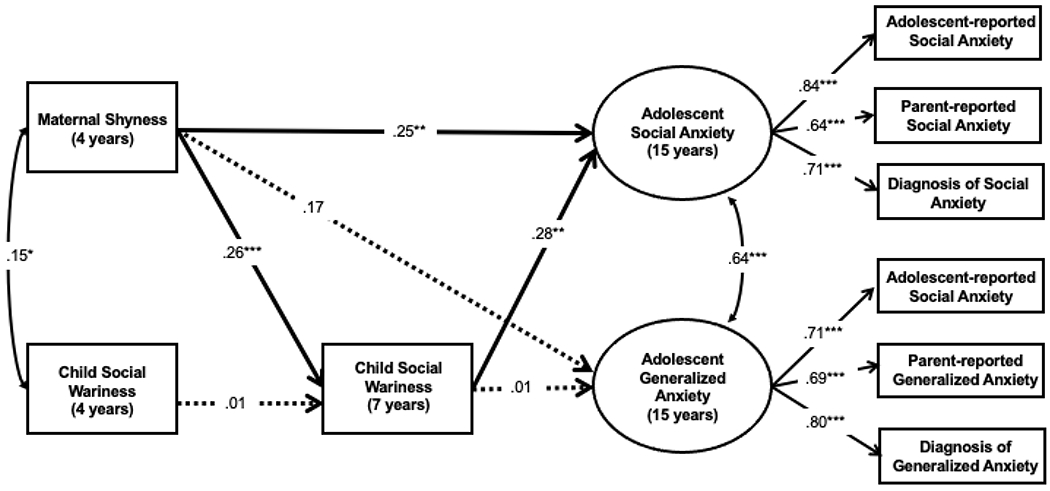
Standardized estimates from the structural equation model. N=291. Maternal education and minority status, and gender were included as covariates but are not depicted here. *p < .05, **p < .01, ***p < .005.
Further, sensitivity analyses yielded similar results (see FigS1 & Table S1). Maternal shyness at 4 years was positively related to child shyness composite at 4 years and positively predicted child shyness at 7 years. Child shyness showed moderate stability from age 4 to 7. Child shyness predicted adolescent social anxiety, but not generalized anxiety, at age 15. Maternal shyness marginally predicted adolescent social anxiety and did not predict generalized anxiety. The indirect effect from maternal shyness at 4 years to adolescent social anxiety at 15 years through child shyness at 7 years was significant, β = .12, 95% CI [.039, .206]; B = .04, 95% Bootstrap CI [.014, .078]. These results suggest that childhood shyness mediated the pathway between maternal shyness and adolescent social anxiety.
Discussion
This study examined the mediating role of social wariness at age 7 in the relation between maternal shyness at age 4 and social anxiety at age 15. Maternal shyness was directly associated with adolescent social but not generalized anxiety, and childhood social wariness partially mediated the association between maternal shyness and adolescent social anxiety. These findings suggest that maternal shyness uniquely predicts adolescent social anxiety, and that childhood social wariness is a mediator through which maternal shyness predicts social anxiety in adolescence.
Our findings extend previous research relating maternal shyness and children’s shyness (Daniels & Plomin, 1985; MacGowan & Schmidt, 2020). Maternal shyness may contribute to children’s social wariness through genetic or environmental transmission. Mothers high in shyness may model (Rickman & Davidson, 1994) or reinforce children’s socially wary behaviors (Coplan et al., 2008) and/or provide fewer opportunities for children’s socialization (Bögels et al., 2001).
In the current study, observed social wariness with unfamiliar peers at age 7 was associated with social anxiety but not generalized anxiety at age 15. This could reflect relations between early sub-clinical and later clinical reflections of social anxiety (Pérez-Edgar & Fox, 2005; Rapee & Coplan, 2010). Social wariness also may hinder social-skill acquisition by inhibiting peer interactions and limiting opportunities to practice social skills, with concomitant effects on self-esteem and social anxiety (Rubin, Coplan, & Bowker, 2009). Such results suggest that social wariness may provide a target for prevention efforts.
Our results suggest that maternal shyness directly relates to adolescent social anxiety, beyond relations to childhood social wariness. Although social wariness, observed in the laboratory, may be an early risk marker; it does not fully explain the relation between maternal shyness and adolescent social anxiety. A more comprehensive construct including assessments of children’s internal experiences and behaviors in multiple settings may better explain this relation. In fact, a shyness composite including mother-report and observed behavior, more fully mediated the link from maternal shyness to adolescent social anxiety (see FigS1). However, this mediation may also reflect reporter bias. In future work, it would be important to include other reporters such as teachers or fathers, and/or observe children’s wary behaviors across multiple contexts, when examining these relations.
Notably, consistent with our previous findings (Degnan et al., 2014), the stability in children’s observed social wariness from ages 4 to 7 was weak. Multiple factors could attenuate this relation, including the diversity in the number, nature and quality of social experiences (Fox et al., 2001; Rubin, Barstead, Smith, & Bowker, 2018). Similarly, children’s specific sociocultural experiences (e.g., intergroup contact, parental racial/ethnic socialization) and/or the temperament of the unfamiliar peer may also impact children’s laboratory-evoked social wariness. These factors further highlight the importance of replicating these results by assessing children’s wariness across multiple contexts and/or by incorporating caregiver reports. As such, our sensitivity analyses using a more comprehensive shyness assessment (including mother-report and observed behavior) showed moderate levels of stability in children’s shyness and demonstrated the robustness of our main results.
This study has several notable strengths including a 12-year prospective, longitudinal, multi-method design, including maternal self-report of shyness, observed measures of social wariness, and latent variables of social and generalized anxiety composed of adolescent self-report, parent-report, and clinical-reports. In addition, we examined social anxiety and generalized anxiety simultaneously with the aim to identify a unique developmental pathway to social anxiety.
Despite its strengths, the current study has several limitations. First, this study focused on only mothers’ shyness. Future studies would benefit from examining more than one caregiver to understand the independent and interactive effects of caregiver shyness on child temperament and anxiety. Second, we did not use a genetically informed study design to identify the extent to which the relations identified in this study are driven by genetic or environmental influences. Third, we did not measure maternal anxiety to understand the unique or shared effects of maternal shyness, after accounting for the effects of mothers’ social or generalized anxiety, on child temperament and anxiety. Fourth, we did not examine the specific parental behaviors (e.g., modeling, verbal communication) through which maternal shyness may contribute to the development of children’s social anxiety. Fifth, we did not assess siblings’ social wariness and anxiety, and whether mothers had different parenting experiences with them. Given that mothers may engage in different parenting behaviors with their children (Hudson & Rapee, 2002; Madigan et al., 2016), it would be important to examine the impact of maternal shyness on siblings based on mothers’ differential parenting experiences.
To conclude, this study provides evidence that higher levels of maternal shyness during the early part of a child’s life contributes to increased social wariness in childhood, which in turn leads to greater social anxiety in mid-adolescence. These findings have two main implications for the prevention of anxiety disorders. First, children of mothers with high levels of shyness may benefit from prevention efforts aimed at reducing the mother-to-child transmission of shyness and social anxiety. For example, previous work suggests that increasing parents’ encouragement of children’s approach behaviors in unfamiliar social situations may help reduce or prevent increases in children’s social wariness during early childhood (e.g., Chronis-Tuscano et al., 2015). Second, given the association between children’s social wariness and social anxiety in adolescence, targeting children with high social wariness in childhood (Luke, Chan, Au, & Lai, 2017) and improving their social skills during free play situations with peers may be viable strategies for the prevention of social anxiety disorders (Chronis-Tuscano, Danko, Rubin, Coplan, & Novick , 2018).
Supplementary Material
Key points:
Social anxiety is a prevalent mental health problem during adolescence with negative consequences.
Given the comorbidity between social anxiety and generalized anxiety in adolescence, it is important to identify the unique pathways to adolescent social anxiety to inform early prevention.
Maternal shyness assessed when their children were four years old was positively associated with adolescents’ social anxiety but not generalized anxiety at age fifteen.
Children’s social wariness at age seven partially mediated the association between maternal shyness when children are four and adolescent social anxiety at age fifteen.
Targeting mothers’ shy behaviors and children’s social wariness may help reduce the risk or severity of social anxiety in adolescence.
Acknowledgements:
This research was supported by grants MH093349 and HD017899 awarded to Dr. Nathan Fox from the National Institute of Health, and ZIA-MH-002782 project directed by Dr. Daniel Pine from Intramural Research Program at the National Institute of Mental Health. The authors thank the children and parents for their participation, and research assistants for their contributions. The authors have declared that they have no competing or potential conflicts of interest.
References
- Beesdo K, Knappe S, & Pine DS (2009). Anxiety and Anxiety Disorders in Children and Adolescents: Developmental Issues and Implications for DSM-V. Psychiatric Clinics of North America, 32(3), 483–524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, & Baugher M (1999). Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. Journal of the American Academy of Child and Adolescent Psychiatry, 38(10), 1230–1236. [DOI] [PubMed] [Google Scholar]
- Birmaher B, Khetarpal S, Brent D, Cully M, Balach L, Kaufman J, & Neer SM (1997). The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. Journal of the American Academy of Child and Adolescent Psychiatry, 36(4), 545–553. [DOI] [PubMed] [Google Scholar]
- Blair K, Shaywitz J, Smith BW, Rhodes R, Geraci M, Jones M, McCaffrey D, Vythilingam M, Finger E, Mondillo K, Jacobs M, Charney DS, Blair RJR, Drevets WC, & Pine DS (2008). Response to emotional expressions in generalized social phobia and generalized anxiety disorder: evidence for separate disorders. The American Journal of Psychiatry, 165(9), 1193–1202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bögels SM, van Oosten A, Muris P, & Smulders D (2001). Familial correlates of social anxiety in children and adolescents. Behaviour Research and Therapy, 39(3), 273–287. [DOI] [PubMed] [Google Scholar]
- Bruch MA, & Heimberg RG (1994). Differences in perceptions of parental and personal characteristics between generalized and nongeneralized social phobics. Journal of Anxiety Disorders, 8(2), 155–168. [Google Scholar]
- Burstein M, He J-P, Kattan G, Albano AM, Avenevoli S, & Merikangas KR (2011). Social phobia and subtypes in the national comorbidity survey-adolescent supplement: prevalence, correlates, and comorbidity. Journal of the American Academy of Child and Adolescent Psychiatry, 50(9), 870–880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buss KA, Davis EL, Kiel EJ, Brooker RJ, Beekman C, & Early MC (2013). Dysregulated fear predicts social wariness and social anxiety symptoms during kindergarten. Journal of Clinical Child and Adolescent Psychology, 42(5), 603–616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cheek JM, & Buss AH (1981). Shyness and sociability. Journal of Personality and Social Psychology, 41(2), 330–339. [Google Scholar]
- Chronis-Tuscano A, Danko CM, Rubin KH, Coplan RJ, & Novick DR (2018). Future directions for research on early intervention for young children at risk for social Anxiety. Journal of Clinical Child and Adolescent Psychology, 47(4), 655–667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chronis-Tuscano A, Rubin KH, O’Brien KA, Coplan RJ, Thomas SR, Dougherty LR, Cheah CSL, Watts K, Heverly-Fitt S, Huggins SL, Menzer M, Begle AS, & Wimsatt M (2015). Preliminary evaluation of a multimodal early intervention program for behaviorally inhibited preschoolers. Journal of Consulting and Clinical Psychology, 83(3), 534–540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clément F, & Dukes D (2017). Social appraisal and social referencing: Two components of affective social learning. Emotion Review, 9(3), 253–261. [Google Scholar]
- Coplan RJ, Arbeau KA, & Armer M (2008). Don’t fret, be supportive! maternal characteristics linking child shyness to psychosocial and school adjustment in kindergarten. Journal of Abnormal Child Psychology, 36(3), 359–371. [DOI] [PubMed] [Google Scholar]
- Côté SM, Vaillancourt T, LeBlanc JC, Nagin DS, & Tremblay RE (2006). The development of physical aggression from toddlerhood to pre-adolescence: a nation-wide longitudinal study of Canadian children. Journal of Abnormal Child Psychology, 34(1), 71–85. [DOI] [PubMed] [Google Scholar]
- Daniels D, & Plomin R (1985). Origins of individual differences in infant shyness. Developmental Psychology, 21(1), 118–121. [Google Scholar]
- de Lijster JM, Dieleman GC, Utens EMWJ, Dierckx B, Wierenga M, Verhulst FC, & Legerstee JS (2018). Social and academic functioning in adolescents with anxiety disorders: A systematic review. Journal of Affective Disorders, 230, 108–117. [DOI] [PubMed] [Google Scholar]
- Degnan KA, Henderson HA, Fox NA, & Rubin KH (2008). Predicting social wariness in middle childhood: The moderating roles of child care history, maternal personality and maternal behavior. Social Development, 17(3), 471–487. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Degnan KA, Almas AN, Henderson HA, Hane AA, Walker OL, & Fox NA (2014). Longitudinal trajectories of social reticence with unfamiliar peers across early childhood. Developmental Psychology, 50(10), 2311. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Eley TC, Bolton D, O’Connor TG, Perrin S, Smith P, & Plomin R (2003). A twin study of anxiety-related behaviours in pre-school children. Journal of Child Psychology and Psychiatry, 44(7), 945–960. [DOI] [PubMed] [Google Scholar]
- Eley TC, McAdams TA, Rijsdijk FV, Lichtenstein P, Narusyte J, Reiss D, … & Neiderhiser JM (2015). The intergenerational transmission of anxiety: a children-of-twins study. American Journal of Psychiatry, 172(7), 630–637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Enders CK, & Bandalos DL (2001). The relative performance of full information maximum likelihood estimation for missing data in structural equation models. Structural Equation Modeling, 8(3), 430–457. [Google Scholar]
- Fox NA, Henderson H.a., Rubin KH, Calkins SD, & Schmidt L. a. (2001). Continuity and discontinuity of behavioral inhibition and exuberance: psychophysiological and behavioral influences across the first four years of life. Child Development, 72(1), 1–21. [DOI] [PubMed] [Google Scholar]
- Gross CT, & Canteras NS (2012). The many paths to fear. Nature Reviews. Neuroscience, 13(9), 651–658. [DOI] [PubMed] [Google Scholar]
- Hastings PD, Nuselovici JN, Rubin KH, Cheah CSL (2010). Shyness, parenting, and parent-child relationships. In Kenneth RJC Rubin H (Ed.), The Development of Shyness and Social Withdrawal (pp. 107–130). [Google Scholar]
- Hopko DR, Stowell J, Jones WH, Armento MEA, & Cheek JM (2005). Psychometric properties of the Revised Cheek and Buss Shyness Scale. Journal of Personality Assessment, 84(2), 185–192. [DOI] [PubMed] [Google Scholar]
- Hudson JL, & Rapee RM (2002). Parent-child interactions in clinically anxious children and their siblings. Journal of Clinical Child and Adolescent Psychology, 31(4), 548–555. [DOI] [PubMed] [Google Scholar]
- Kashdan TB, & Herbert JD (2001). Social anxiety disorder in childhood and adolescence: Current status and future directions. Clinical Child and Family Psychology Review, 4(1), 37–61. [DOI] [PubMed] [Google Scholar]
- Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P, Williamson D, & Ryan N (1997). Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. Journal of the American Academy of Child and Adolescent Psychiatry, 36(7), 980–988. [DOI] [PubMed] [Google Scholar]
- Kendler KS, Karkowski LM, & Prescott CA (1999). Fears and phobias: reliability and heritability. Psychological Medicine, 29(3), 539–553. [DOI] [PubMed] [Google Scholar]
- Kessel EM, Kujawa A, Hajcak Proudfit G, & Klein DN (2015). Neural reactivity to monetary rewards and losses differentiates social from generalized anxiety in children. Journal of Child Psychology and Psychiatry, 56(7), 792–800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lahey BB, Van Hulle CA, Keenan K, Rathouz PJ, D’Onofrio BM, Rodgers JL, & Waldman ID (2008). Temperament and parenting during the first year of life predict future child conduct problems. Journal of Abnormal Child Psychology, 36(8), 1139–1158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luke F, Chan CC, Au A, & Lai SMK (2017). Adaptive parenting for alleviating young children’s shyness: A randomized controlled trial of an early intervention program. Infant and Child Development, 26(6), 1–19. [Google Scholar]
- MacGowan TL, & Schmidt LA (2020). Shyness, aggression, and empathy in children of shy mothers: Moderating influence of children’s psychophysiological self-regulation. Developmental Psychobiology, 62(3), 324–338. [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, & Williams J (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madigan S, Plamondon A, Browne D, & Jenkins J (2016). Stability of observed maternal behavior across tasks, time, and siblings. Parenting, 16(2), 108–124. [Google Scholar]
- Muris P, van Zwol L, Huijding J, & Mayer B (2010). Mom told me scary things about this animal: parents installing fear beliefs in their children via the verbal information pathway. Behaviour Research and Therapy, 48(4), 341–346. [DOI] [PubMed] [Google Scholar]
- Murray L, Creswell C, & Cooper PJ (2009). The development of anxiety disorders in childhood: An integrative review. Psychological Medicine, 39(9), 1413–1423. [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2012). Statistical analysis with latent variables using Mplus. Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Neal JA, Edelmann RJ, & Glachan M (2002). Behavioural inhibition and symptoms of anxiety and depression: Is there a specific relationship with social phobia? British Journal of Clinical Psychology, 41(4), 361–374. [DOI] [PubMed] [Google Scholar]
- Olsson A, & Phelps EA (2007). Social learning of fear. Nature Neuroscience, 10(9), 1095–1102. [DOI] [PubMed] [Google Scholar]
- Pérez-Edgar K, & Fox NA (2005). Temperament and anxiety disorders. Child and Adolescent Psychiatric Clinics of North America, 14(4), 681–706. [DOI] [PubMed] [Google Scholar]
- Pine DS (2007). Research review: a neuroscience framework for pediatric anxiety disorders. Journal of Child Psychology and Psychiatry, 48(7), 631–648. [DOI] [PubMed] [Google Scholar]
- Prior M, Smart D, Sanson A, & Oberklaid F (2000). Does shy-inhibited temperament in childhood lead to anxiety problems in adolescence? Journal of the American Academy of Child and Adolescent Psychiatry, 39(4), 461–468. [DOI] [PubMed] [Google Scholar]
- Rapee RM; Coplan RJ (2010). Conceptual relations between anxiety disorder and fearful temperament. In Gazelle KH, Heidi; Rubin (Ed.), Social anxiety in childhood: Bridging developmental and clinical perspectives. New Directions for Child and Adolescent Development (pp. 17–31). Jossey-Bass. [DOI] [PubMed] [Google Scholar]
- Rapee RM, & Spence SH (2004). The etiology of social phobia: Empirical evidence and an initial model. Clinical Psychology Review, 24(7), 737–767. [DOI] [PubMed] [Google Scholar]
- Rickman MD, & Davidson RJ (1994). Personality and Behavior in Parents of Temperamentally Inhibited and Uninhibited Children. Developmental Psychology, 30(3), 346–354. [Google Scholar]
- Root AE, Hastings PD, & Rubin KH (2016). The parenting behaviors of shy–anxious mothers: The moderating role of vagal tone. Journal of Child and Family Studies, 25(4), 1325–1333. [Google Scholar]
- Rubin KH, Barstead MG, Smith KA, Bowker JC, 2018. Peer relations and the behaviorally inhibited child (2018) In: Perez-Edgar K, Fox NA (Eds.), Behavioral Inhibition During Childhood and Adolescence. Springer. [Google Scholar]
- Rubin KH, Coplan RJ, & Bowker JC (2009). Social withdrawal in childhood. Annual Review of Psychology, 60(1), 141–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Silva BA, Mattucci C, Krzywkowski P, Murana E, Illarionova A, Grinevich V, Canteras NS, Ragozzino D, & Gross CT (2013). Independent hypothalamic circuits for social and predator fear. Nature Neuroscience, 16(12), 1731–1733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith AK, Rhee SH, Corley RP, Friedman NP, Hewitt JK, & Robinson JL (2012). The magnitude of genetic and environmental influences on parental and observational measures of behavioral inhibition and shyness in toddlerhood. Behavior genetics, 42(5), 764–777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zeytinoglu S, Morales S, Lorenzo NE, Chronis-Tuscano A, Degnan KA, Almas AN, … & Fox NA (2021). A Developmental Pathway From Early Behavioral Inhibition to Young Adults’ Anxiety During the COVID-19 Pandemic. Journal of the American Academy of Child & Adolescent Psychiatry. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.