

Abstract
Gender affirmation laryngeal and voice surgeries are components of “voice-lift” or cosmetic voice surgeries. Feminization surgery can modify vocal folds (fundamental frequency [Fo]) and vocal tract (resonance frequency). For increased pitch, vocal folds should be shorter, thinner, and tighter. Cricothyroid approximation (CTA) surgery increases tension of the vocal folds. Endoscopic procedures for pitch raising are done by shortening the length and reducing mass of vocal folds. This shortening is achieved by surgically creating anterior glottic web. Comparing the results of various open and endoscopic surgical techniques, fundamental frequency (Fo) is raised maximally and remains stable after GL as compared with CTA.
Keywords: transgender, phonosurgery
Introduction
The estimated incidence of transsexuality is 1 in 54000 individuals. Seventy-five percent of individuals desire to be men to women (male-to-female [MtF]), while the remainder wishes to transition from women to men (female-to-male [FtM]). 1
Voice is the most important secondary sex character for gender identity. Voice features such as pitch, voice quality, and inflection reflect a person's gender. The feminine voice is generally perceived as high pitch, slightly breathier, and with more varied inflection. In transwomen, male voice tends to have a negative influence on their femineity. During everyday communication, they face gender bias and are stigmatized. Patients feel inferior due to their deep voice, leading to depression. Negative impact on individual sense of identity and their lack of confidence in interacting with others affect their psychological well-being.
Pitch is the relative highness or lowness of a tone as perceived by the ear. It depends on the number of vibrations per second produced by vocal cords. It is also the main acoustic correlate of tone and intonation.
Male-to-female (MtF) transgender persons have a low pitch in speech. Hormonal (estrogen) treatment in MtF shows no improvement in their voice in everyday life communication. Hormone therapy is beneficial for masculinizing the voice in female-to-male (FtM) transsexuals. 2
MtF individuals having lower fundamental frequencies (Fo) also differ in resonance and speech characteristics like phrasing, speed, breathiness, volume, and presentation. Fo should be more than 150 to 160 Hz to be perceived as female. 3 Only 41% of the perception of gender in voice is explained by Fo, with the remainder of the variance being accounted for other parameters like resonance, intonation, breathiness and formants frequencies.
Out of all the characteristics, only pitch (Fo) is amenable to surgical correction. Other features can be corrected by speech and behavioral therapy. Oates and Dacakis introduced a classification of typical frequency ranges: male voice range (80–165Hz); female voice range (145–275Hz); and 145 to 165 Hz is the overlap range which cannot be assigned to one gender uniquely. 4
Voice Assessment
For any voice corrective measure, assessment of voice by a various tests is essential. These include Fo, frequency range, jitter, maximum phonation time (MPT), phonation quotient (PQ), estimated subglottic pressure (ESGP), and voice handicap index (VHI). The VHI is a self-assessment score. 5 Perceptual analysis is done using the grade, roughness, asthenia, breathiness, and strain (GRBAS) Hirano scale. 6 Voice assessment is performed by the speech-language pathologist. Posttreatment voice assessment is repeated again at regular intervals of 1 month, 2 months, 6 months and 2 years.
Procedure for Voice Feminization
The history of surgery for feminine-sounding voice dates back to the 16th century on the Italian castrati.
7
There are four factors that control the pitch, namely. tension, mass, length of the vocal cord and the subglottal pressure. Understanding the mathematical derivation (
 ) is important for the analysis in pitch-altering voice surgery. (Fo, L—length of the vocal cords;
σ
—longitudinal stress and ñ—tissue density [mass per unit length]). To increase vocal cord pitch (Fo), one will require the following procedures:
) is important for the analysis in pitch-altering voice surgery. (Fo, L—length of the vocal cords;
σ
—longitudinal stress and ñ—tissue density [mass per unit length]). To increase vocal cord pitch (Fo), one will require the following procedures:
Increasing vocal cord tension (ó), reducing vocal cord mass (ñ), or shortening the length of vocal cords (L).
MtF individuals take medical and hormonal therapy and undertake cosmetic and reconstructive surgeries before reaching the feminine status. Pitch altering phonosurgery can be done either by an external neck approach or endoscopic transoral approach. They include:
(A) Increasing tension—cricothyroid approximation (CTA).
(B) Shortening procedure—cold knife glottoplasty (GL)/laser-shortening GL (Wendler's).
(C) Decreasing mass—laser-assisted voice adjustment (LAVA)/laser reduction glottoplasty (LRG).
External Neck Approach
Cricothyroid Approximation (CTA)
CTA was introduced by Kitajima, Tanabe and Isshiki 8 9 to address low pitch voice in women. Cricoid and thyroid cartilage were approximated by interrupted sutures with small pieces of silicon, used underneath to prevent tearing through the soft cartilage ( Figs. 1 and 2 ). It was observed that 1 mm of approximation between the cricoid and thyroid cartilages resulted in a pitch elevation of 0.15 to 0.90 semitones. This results in lengthening of the cords and corresponding anteroinferior rotation of the larynx. This rotation causes the prominence of thyroid notch (“Adam's apple”). The prominent thyroid notch can be reduced by thyroid chondroplasty. Isshiki was successful in increasing the tension of the vocal folds by approximation of the cricoid cartilage to the lower edge of the thyroid cartilage using wired sutures. This approximation mimics the contraction of cricothyroid muscle, tensor of vocal cord. The disadvantage of using wire is the tearing of cartilage. Outcomes of CTA are not always favorable due to cricothyroid joint (CTJ) anatomy and ossification of thyroid cartilage in the older age group.
Fig. 1.
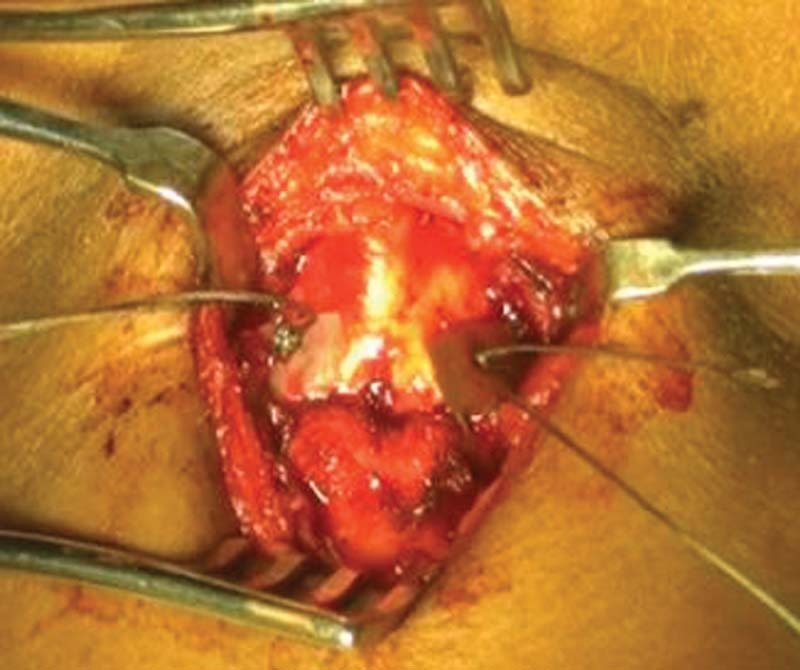
Cricothyroid approximation (CTA) by mobilizing cricothyroid soft-tissue bands, bringing thyroid down with skin hook, and suturing with nonabsorbable suture over silicon sheet.
Fig. 2.
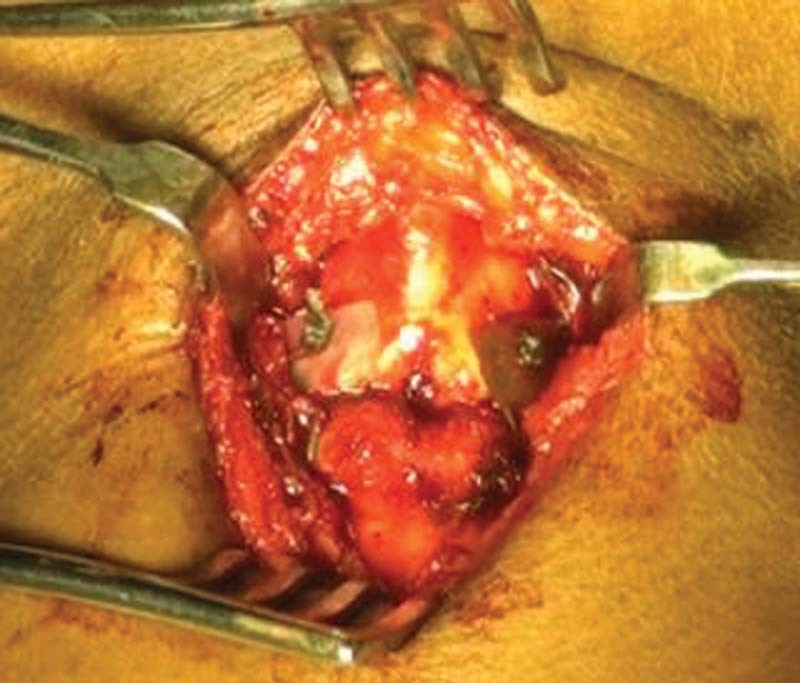
Cricothyroid approximation with silicon sheet.
Neumann and Welzel modified this technique by fixing cartilage using miniplates. 10 ( Fig. 3 ). CTA can be combined with the reduction of Adam's apple, using Wolfort technique. 11 Thyroid chondroplasty can be performed through the same skin incision. One more modification was introduced by Kanagalingam et al by combining CTA with subluxation of the cricoid. Long-term results of this technique were not very encouraging. 12
Fig. 3.
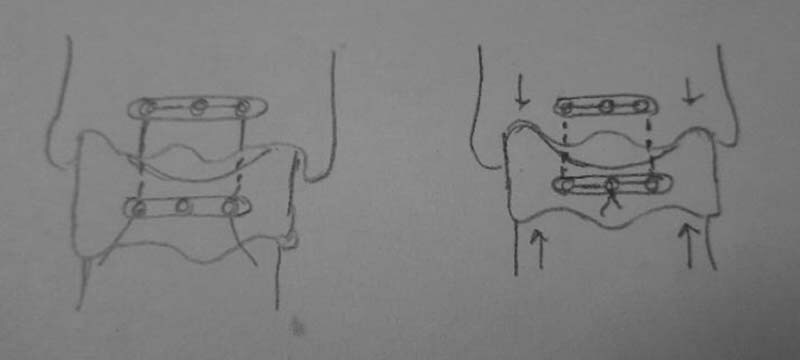
Cricothyroid approximation (CTA) using titanium miniplates with wire sutures.
There are other vocal ligament tightening procedures introduced by LeJeune et al and Tucker. In the LeJeune technique, inferiorly based thyroid cartilage flap is used, while it is exactly the opposite with the Tucker technique. Early results are encouraging with both the techniques, but long-term results are unsatisfactory. 13 , 14
Anterior Commissure Approaches
The first open surgical approach to anterior commissure was described by Donald on 14 patients. Anterior commissure was split open, anterior one-third of vocal folds deepithelized, and raw edges were sutured. This shortened the length of the vocal folds by creating an anterior web. 15 Kunachak et al described an extensive open technique by resecting the vertical anterior segment of thyroid cartilage and segment of anterior part of true and false cords ( Fig. 4 ). 16
Fig. 4.
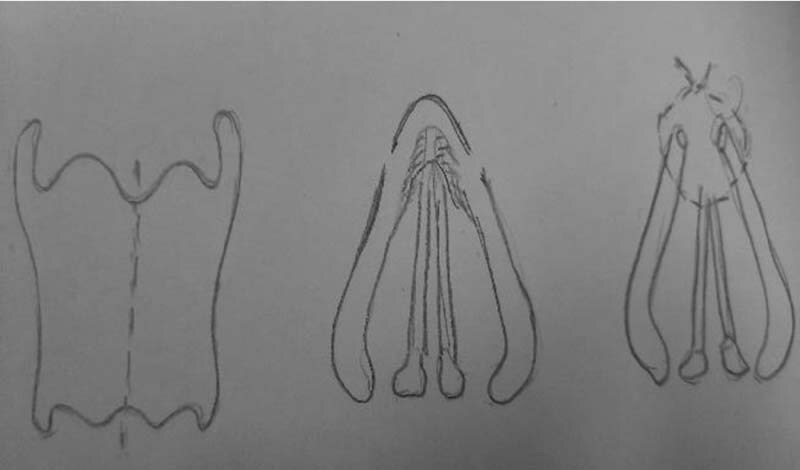
Anterior commissure approach.
Surgical Technique
Surgery is done under general anesthesia with the patient in Rose's position. Transverse neck incision was made over the midpoint of thyroid notch and inferior border of thyroid cartilage. Subcutaneous flaps were elevated and strap muscle separated in the midline. Two parallel vertical cuts were given 4 mm away from the midline or the anterior commissure running from the superior border down to the inferior border of the thyroid cartilage. A strip of cartilage with Broyle's ligament attached to it was then obtained and pulled forward. This exposed the inner perichondrium and vocal ligament. Vocal folds are then excised approximately 6 mm on each side. Closure was done with 3–0 nylon or prolene passed through cut end of cartilage at anterior commissure, with bite included attached perichondrium and vocal folds. It thus created a new anterior commissure. Remnant thyroid cartilage was lamina sutured by interrupted sutures ( Fig. 4 ).
Thomas and Macmillan combined feminization laryngoplasty with thyrohyoid approximation. They retrospectively studied 94 patients from 2002 to 2012. In their technique, midline anterior segment of the thyroid cartilage was removed (10–14 mm wide). Anterior false cord and vocal cord (mucosa, ligament and thyroarytenoid muscle) are excised on both sides. These are sutured back to create a new anterior commissure. The thyrohyoid approximation portion of the procedure consists of removing the superior portion of each thyroid ala (10 mm). Sutures are placed through the upper thyroid cartilage and the hyoid bone to suspend the thyroid cartilage as close as possible to the hyoid bone. This thyrohyoid approximation shortens the height of the pharynx, thus creating a feminine resonance cavity. The advantage of this combined approach is that the external masculine appearance of the thyroid cartilage is diminished, as the large anterior strip of cartilage is removed during feminization laryngoplasty. 17
Endoscopic Approaches
The endoscopic procedure entails shortening of the vibrating length of the vocal folds by creating new anterior commissure. This procedure was first described by Wendler. 18 Various other studies by Gross, Remacle et al and Mastronikolis et al showed good long-term results with this technique. 19 20 21 Anderson reported good results even without any suture placement over anterior commissure. 22
The advantage of this surgical technique is its low invasiveness without an external approach. The only disadvantage of this procedure is the irreversibility and risk of postoperative hoarseness.
Orloff described a procedure that modifies the vocal fold density (ñ). LAVA is the procedure in which the membrane of vocal folds is vaporized by Co2 laser to increase the stiffness of vocal cord, thus raising the Fo. The average pitch increase with LAVA was 26 Hz. It improves voice femininity, congruity with self-image, and satisfaction. It showed decreased vocal quality, loudness, and vocal range. Postoperative voice therapy optimizes outcomes. 23
LRG is a modified LAVA procedure in which epithelium and vocal fold muscle are ablated by laser in anterior part, according to Kocak et al. LRG was initially done in failed cases of CTA for pitch raising. 24
Voice Therapy
Voice therapy is a must before doing any pitch altering phonosurgery. Voice therapy can alter speaking pitch and resonance by active muscle contraction and efforts. Patients are able to alter daily speaking frequencies. In both endoscopic and open procedures, 10 to 14 days of voice rest is advisable. Components of voice production in voice feminization include pitch, resonance, and intonation. Therapy concentrates on flow phonation, which targets the exertion of airflow during voice production and resonant voice therapy which, in turn, focuses on vibration of sound in the mouth. In few patients, successful feminization of the voice is possible with conservative voice therapy. Male voice may reappear in uncontrolled and emotional situations like yawning, coughing, and laughing.
Surgical Complications of Voice Feminization Procedure
Complications related to CTA technique are lowering of pitch over time, scar/puckering at the incision site, dysphagia and, rarely, temporary subcutaneous emphysema. An external neck approach may cause reduced loudness, decreased vocal range, decreased clarity, and pitch instability. Sometimes, there may be no change in pitch or a less than desired increase in pitch. Shortening GL technique may cause strained or strangled voice, granulation tissue formation, and dehiscence of suture site at anterior commissure. Improper voice rest following shortening GL cause suture dehiscence.
Procedure for Thyroid Chondroplasty (“Tracheal Shave”)
Hormonal therapy influences hair growth, skin texture and breast development in transwomen but has no effect on the laryngeal framework. Prominence of thyroid cartilage (Adam's apple) is influenced by interlaminae angle, which is more acute (∼90°) in males and creates prominence in the neck. Thyroid prominence can be surgically reduced by thyroid chondroplasty, thyroid cartilage reduction, or thyroid shave. This procedure is combined with pitch-raising surgery of CTA (Isshiki type 4 procedure) in many patients. This procedure was first described by Wolfort and Parry. 25 Thyroid chondroplasty was included in the list of the gender affirmation surgeries of the World Professional Association for Transgender Health (WPATH) in 2011. The aim of this operation is to give the neck a more feminine look. The reverse of this procedure, masculinization of the thyroid cartilage, done by costal cartilage graft of the thyroid notch, was first described by Deschamps-Braly et al. 26
This procedure involves resection of anterosuperior portion of thyroid cartilage. Both right and left vocal folds meet each other at the anterior commissure. Anterior commissure is situated at the midpoint of thyroid cartilage (thyroid notch to inferior border of thyroid cartilage). Dissection above it endanger vocal folds. Another important aspect of dissection is ossification of thyroid cartilage, which starts around the age of 25 years with complete ossification by age of 65 years.
Discussion
CTA was found to be successful in 50 percent of our cases (eight) on more than 2-year follow-up. R.S. used nonabsorbable suture (braided ethibond) during CTA procedure. One can use miniplates for approximation. The Neumann technique used miniplates and observed satisfying results in 85 percent of patients.
Endoscopic technique by approximating anterior one-third of vocal cord (Wendler GL) has good long-term effects in our series of four cases. Fo improved significantly (around 200 Hz) and remained stable during the follow-up. Remacle et al studied 15 patients, and Fo improved significantly with a decrease in voice range.
Meister et al modified Wendler GL by injecting botox on both cricothyroid muscle to facilitate voice rest.(30) Anderson et al modified the technique of anterior GL by not suturing both the vocal cords and injecting carboxymethylcellulose gel to medialize the vocal cords. 27
Meta-analysis of 13 studies on transgender voice surgery by Song and Jiang observed maximum increase in Fo with endoscopic shortening technique, and second highest increase in Fo by CTA technique, while LRG had lowest increase in Fo. The largest heterogenicity in vocal pitch outcomes was observed with endoscopic shortening procedure. 28
Elena Mora et al compared CTA and GL on 28 CTA and 23 GL cases. Mean Fo improved in both the groups, but the increase was 27 Hz higher after GL than after CTA. After CTA, Fo decreased over time but remained stable after GL. 29
All our patients were examined by voice therapist. Pre- and postoperative voice therapy plays important role in raising pitch as compared with surgery alone. All patients were reviewed after 1, 3 and, sometimes, 6 months of voice therapy.
Conclusions
Gender-affirmation phonosurgery requires proper voice assessment and counselling. Endoscopic shortening procedures are highly satisfactory in improving vocal pitch on long-term follow-up. Postoperatively, voice therapy increases the Fo, stabilizes voice, and creates a more female timbre.
Footnotes
Conflict of Interest None declared.
References
- 1.Landén M, Wålinder J, Lundström B. Prevalence, incidence and sex ratio of transsexualism. Acta Psychiatr Scand. 1996;93(04):221–223. doi: 10.1111/j.1600-0447.1996.tb10638.x. [DOI] [PubMed] [Google Scholar]
- 2.Van Borsel J, De Cuypere G, Van den Berghe H. Physical appearance and voice in male-to-female transsexuals. J Voice. 2001;15(04):570–575. doi: 10.1016/S0892-1997(01)00059-5. [DOI] [PubMed] [Google Scholar]
- 3.Wolfe V I, Ratusnik D L, Smith F H, Northrop G. Intonation and fundamental frequency in male-to-female transsexuals. J Speech Hear Disord. 1990;55(01):43–50. doi: 10.1044/jshd.5501.43. [DOI] [PubMed] [Google Scholar]
- 4.Oates J, Dacakis G. Voice change in transsexuals. Venereology. 1997;10:178–187. [Google Scholar]
- 5.Jacobson B H, Johnson A, Grywalski C, Silbergleit A, Jaconsen G, Benninger M S. The voice handicap index (VHI): development and validation. Am J Speech Lang Pathol. 2001;6(03):66–70. [Google Scholar]
- 6.Hirano M, Saito S, Sawashima M, Hiki S, Hirose H. A guideline for phonatory function test. The Japan Journal of Logopedics and Phoniatrics. 1982;23:164–167. [Google Scholar]
- 7.Jenkins J S.The voice of the castrato Lancet 1998351(9119):1877–1880. [DOI] [PubMed] [Google Scholar]
- 8.Kitajima K, Tanabe M, Isshiki N.Cricothyroid distance and vocal pitch. Experimental surgical study to elevate the vocal pitch Ann Otol Rhinol Laryngol 197988(1 Pt 1):52–55. [DOI] [PubMed] [Google Scholar]
- 9.Isshiki N, Morita H, Okamura H, Hiramoto M.Thyroplasty as a new phonosurgical technique Acta Otolaryngol 197478(5-6):451–457. [DOI] [PubMed] [Google Scholar]
- 10.Neumann K, Welzel C. The importance of the voice in male-to-female transsexualism. J Voice. 2004;18(01):153–167. doi: 10.1016/S0892-1997(03)00084-5. [DOI] [PubMed] [Google Scholar]
- 11.Wolfort F G, Dejerine E S, Ramos D J, Parry R G.Chondrolaryngoplasty for appearance Plast Reconstr Surg 19908603464–469., discussion 470 [PubMed] [Google Scholar]
- 12.Kanagalingam J, Georgalas C, Wood G R, Ahluwalia S, Sandhu G, Cheesman A D. Cricothyroid approximation and subluxation in 21 male-to-female transsexuals. Laryngoscope. 2005;115(04):611–618. doi: 10.1097/01.mlg.0000161357.12826.33. [DOI] [PubMed] [Google Scholar]
- 13.LeJeune F E, Guice C E, Samuels P M.Early experiences with vocal ligament tightening Ann Otol Rhinol Laryngol 198392(5 Pt 1):475–477. [DOI] [PubMed] [Google Scholar]
- 14.Tucker H M.Anterior commissure laryngoplasty for adjustment of vocal fold tension Ann Otol Rhinol Laryngol 198594(6 Pt 1):547–549. [DOI] [PubMed] [Google Scholar]
- 15.Donald P J. Voice change surgery in the transsexual. Head Neck Surg. 1982;4(05):433–437. doi: 10.1002/hed.2890040512. [DOI] [PubMed] [Google Scholar]
- 16.Kunachak S, Prakunhungsit S, Sujjalak K. Thyroid cartilage and vocal fold reduction: a new phonosurgical method for male-to-female transsexuals. Ann Otol Rhinol Laryngol. 2000;109(11):1082–1086. doi: 10.1177/000348940010901116. [DOI] [PubMed] [Google Scholar]
- 17.Thomas J P, Macmillan C. Feminization laryngoplasty: assessment of surgical pitch elevation. Eur Arch Otorhinolaryngol. 2017;274(10):2049–2058. doi: 10.1007/s00405-013-2511-3. [DOI] [PubMed] [Google Scholar]
- 18.Wendler J.Vocal pitch elevation after transexualism male to femalePaper presented at: Proceedings of the Union of the European Phoniatricians; 1990;Salsomaggiore, Italy
- 19.Gross M. Pitch-raising surgery in male-to-female transsexuals. J Voice. 1999;13(02):246–250. doi: 10.1016/s0892-1997(99)80028-9. [DOI] [PubMed] [Google Scholar]
- 20.Remacle M, Matar N, Morsomme D, Veduyckt I, Lawson G. Glottoplasty for male-to-female transsexualism: voice results. J Voice. 2011;25(01):120–123. doi: 10.1016/j.jvoice.2009.07.004. [DOI] [PubMed] [Google Scholar]
- 21.Mastronikolis N S, Remacle M, Biagini M, Kiagiadaki D, Lawson G. Wendler glottoplasty: an effective pitch raising surgery in male-to-female transsexuals. J Voice. 2013;27(04):516–522. doi: 10.1016/j.jvoice.2013.04.004. [DOI] [PubMed] [Google Scholar]
- 22.Anderson J A. Pitch elevation in trangendered patients: anterior glottic web formation assisted by temporary injection augmentation. J Voice. 2014;28(06):816–821. doi: 10.1016/j.jvoice.2014.05.002. [DOI] [PubMed] [Google Scholar]
- 23.Orloff L A, Mann A P, Damrose J F, Goldman S N. Laser-assisted voice adjustment (LAVA) in transsexuals. Laryngoscope. 2006;116(04):655–660. doi: 10.1097/01.mlg.0000205198.65797.59. [DOI] [PubMed] [Google Scholar]
- 24.Koçak I, Akpınar M E, Cakır Z A, Doğan M, Bengisu S, Celikoyar M M. Laser reduction glottoplasty for managing androphonia after failed cricothyroid approximation surgery. J Voice. 2010;24(06):758–764. doi: 10.1016/j.jvoice.2009.06.004. [DOI] [PubMed] [Google Scholar]
- 25.Wolfort F G, Parry R G. Laryngeal chondroplasty for appearance. Plast Reconstr Surg. 1975;56(04):371–374. doi: 10.1097/00006534-197510000-00001. [DOI] [PubMed] [Google Scholar]
- 26.Deschamps-Braly J C, Sacher C L, Fick J, Ousterhout D K. First female-to- male facial confirmation surgry with description of a new procedure for masculinization of the thyroid cartilage (Adam's apple) Plast Reconstr Surg. 2017;139(04):883e–887e. doi: 10.1097/PRS.0000000000003185. [DOI] [PubMed] [Google Scholar]
- 27.Meister J, Hagen R, Shehata-Dieler W, Kühn H, Kraus F, Kleinsasser N. Pitch elevation in male-to-female trangender persons- the Wurzburg approach. J Voice. 2017;31(02):2.44E9–2.44E17. doi: 10.1016/j.jvoice.2016.07.018. [DOI] [PubMed] [Google Scholar]
- 28.Song T E, Jiang N. Transgender phonosurgery: a systematic review and meta-analysis. Otolaryngol Head Neck Surg. 2017;156(05):803–808. doi: 10.1177/0194599817697050. [DOI] [PubMed] [Google Scholar]
- 29.Mora E, Cobeta I, Becerra A, Lucio M J. Comparison of cricothyroid approximation and glottoplasty for surgical voice feminization in male-to-female transsexuals. Laryngoscope. 2018;128(09):2101–2109. doi: 10.1002/lary.27172. [DOI] [PubMed] [Google Scholar]