

Abstract
Metoidioplasty is a variant of the gender affirmation technique neophalloplasty, where a hormonally enlarged clitoris is reconstructed to become a small penis. The goals of metoidioplasty are male appearance of the genitalia, voiding in standing position, and completely preserved erogenous sensation of the neophallus. However, it does not enable penetrative sexual intercourse due to the small dimensions of the neophallus. Basic principles of metoidioplasty were established 50 years ago, and many refinements of the technique have been reported since. The latest improvements are based on the advances in urethroplasty, perioperative care, and new insights into female genital anatomy. The current metoidioplasty technique is a one-stage procedure that includes vaginectomy, straightening and lengthening of the clitoris, urethral reconstruction by combined flaps and grafts, and scrotoplasty with insertion of testicular implants. Good aesthetic, functional, and psychosexual outcomes are achieved with this type of neophalloplasty.
Keywords: transman, metoidioplasty, clitoris, urethroplasty, gender affirmation, neophalloplasty
Introduction
Neophalloplasty presents the most challenging task in transmasculine gender affirmation surgery. Two surgical options currently exist—metoidioplasty and total phalloplasty, each with its well-known advantages and disadvantages. While searching for an ideal method of neophalloplasty to fulfill all aesthetic and functional goals, we are striving to improve outcomes of available techniques and adjust them to patients' desires and expectations. Metoidioplasty is a variant of transmasculine neophalloplasty, wherein a small neophallus is reconstructed from a hormonally enlarged clitoris. Total phalloplasty implies complex and multistaged procedures to create a neophallus large enough to enable penile prosthesis implantation and penetration during sexual intercourse. On the other hand, metoidioplasty is usually a one-stage procedure that results in the male appearance of the genitalia, voiding in a standing position, and completely preserved erogenous sensation, but does not enable penetrative sexual intercourse due to the dimensions of the neophallus. Since the first reports almost 50 years ago, the metoidioplasty procedure was greatly improved in all aspects. The latest innovations are based on the advances in urethroplasty, perioperative care, and new insights into female genital anatomy. 1 2 3 The aim of this review is to evaluate techniques of metoidioplasty and their outcomes, with focus on the latest improvements and our experience.
Principles and Techniques
The principle of using the clitoris for penile substitution in transmen was originally reported in 1973 by Durfee and Rowland. 4 The techniques and outcomes were gradually modified, and the term metoidioplasty was introduced, which was derived from the Greek words “meta”–“toward” and “oidion”–“male genitalia.” 5 Surgical principles of metoidioplasty were established by Laub and Eicher in the 1980s. 5 6 Laub described metoidioplasty as a reconstruction of hormonally hypertrophied female genitalia into the male embryological analogs: clitoris into a penis, labia majora into the scrotum, outer surface of labia minora into the penile skin, and inner surface into the urethra. 5 At the same time, Eicher reported a variant of the procedure named “clitorispenoid,” which included reposition of the clitoris toward the mons pubis and lengthening the urethra to enable voiding while standing. 6 In this way, metoidioplasty was defined as an operation that satisfies the legal requirements for gender affirmation surgery, resulting in the appearance of a small boy's penis with completely preserved sensitivity. 5 These principles remain to date, with many modifications that followed. In current literature, three different techniques of metoidioplasty have been reported: simple, ring, and Belgrade metoidioplasty.
Simple Metoidioplasty
Simple metoidioplasty is performed on the clitoris, which was quite enlarged by preoperative testosterone treatment. The first steps of the procedure involve degloving and transection of clitoral suspensory ligaments. The urethral plate is dissected ventrally and divided with additional correction of the chordee. The remaining clitoral skin with the labia minora and majora are used to cover the clitoral body and create a bulky neophallus. The bottom of the levator muscle is also dissected and sutured to support the enlarged clitoris. With this technique, the native urethral meatus remains intact for possible urethral lengthening in the future. Special care must be taken during skin closure, in order to not compromise urine outflow. A urinary catheter is used for urine drainage and to prevent leakage over the surrounding reconstructed skin. Vaginectomy can be performed as well. The complication rate is less than 5% and is mainly related to malunion or malrotation of the skin closure lines. Simple metoidioplasty offers a safe, complication-free gender affirmation surgery with fast recovery and acceptable cost. On the other hand, it is limited to transforming a clitoris into a small penis, without achieving the complete appearance of male genitalia and without urethral lengthening that would enable voiding in a standing position. 7
Ring Metoidioplasty
Ring metoidioplasty was reported initially in 2009, without further mention in the literature. 8 This technique is similar to simple metoidioplasty in the dissection of the chordee and transection of the urethral plate to lengthen and straighten the clitoris. However, clitoral ligaments are not transected. The main difference is the urethroplasty performed in the ring technique by using vascularized ring flap, which consists of urethral plate and inner surfaces of both labia minora. A special dorsal urethral ring flap is harvested from vaginal mucosa and attached to the underlying clitoral bodies, allowing its tubularization without pressure. The remaining labial skin is used to cover the clitoral body and gain a small neophallus. The main improvement of this technique is lengthening of the urethra to the tip of the neophallus by creation of ventral urethral plate that is closed with the long vaginal flap, which enables voiding while standing. Vaginectomy and scrotoplasty with testicular implants are performed in the second stage. The most common complications are urethral fistula (10–26%) and stricture (3–5%). In almost 30% of cases, revision surgery is necessary due to various complications, mostly urethral. Sexual satisfaction is presumed high, without exact data in the literature. 7 8
Belgrade Metoidioplasty
Belgrade metoidioplasty is originally based on the experience in repair of severe hypospadias and disorders of sexual development. 9 This technique underwent several modifications to become a one-stage procedure, which includes the following steps: vaginectomy, complete straightening, and lengthening of the clitoris by dissection of suspensory ligaments and urethral plate, urethral lengthening with available vascularized flaps and grafts, and scrotoplasty with insertion of testicular implants. 10
Preoperative protocol includes local application of dihydrotestosterone and use of vacuum devise for additional clitoral enlargement and better postoperative outcome. Dihydrotestosterone cream is administered locally twice a day for 3 months, and must be terminated 1 month before surgery. Vacuum device is also used for 3 months preoperatively, twice a day for 30 minutes, and is continued for at least 6 months postoperatively to prevent retraction of the neophallus.
Vaginectomy is performed by removing vaginal mucosa (colpocleisis), with preservation of part of anterior vaginal wall to be used for urethral reconstruction. Degloving is made, and dorsal clitoral ligaments are completely dissected to lengthen the clitoral body. The clitoris has only suspensory ligament, which consists of a superficial and deep part. These components keep the clitoral body in a curved position, providing stability during sexual activity. When releasing the ligaments, care must be taken to preserve neurovascular bundle intact, which lies just beneath the suspensory ligament. Another structure that is responsible for the curving of the clitoral body is the urethral plate. It is a short and wide mucosal plate, which is adherent ventrally to clitoral bodies. To straighten and lengthen the clitoral body as much as possible, this urethral plate has to be divided, usually at the level of glanular corona or just beneath it. During this maneuver, care must be taken to not only avoid injury of the spongiosal tissue and excessive bleeding but also preserve the blood supply to the urethral plate. The proximal part of the plate that surrounds the native meatus also has to be dissected to provide good mobility for urethral reconstruction. In this way, a complete straightening and lengthening of the clitoral body is achieved ( Figs. 1 and 2 ). 11
Fig. 1.
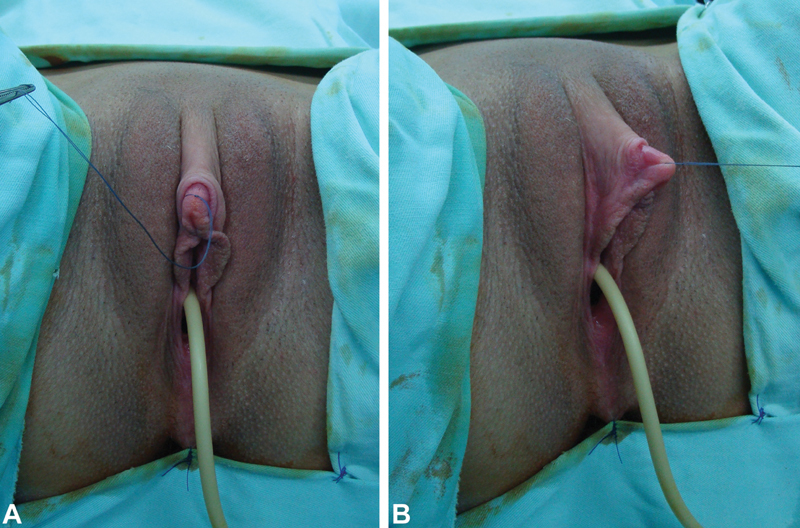
Preoperative appearance. Clitoris is enlarged after hormonal treatment. ( A ) Ventral view, ( B ) lateral view.
Fig. 2.

Planned surgical incisions are marked. Inner surface of left labia minora and anterior vaginal wall are planned and marked for harvesting of the flaps.
Urethral lengthening presents the most challenging part of metoidioplasty, and all available vascularized tissue is used to create a new channel that will enable voiding in standing position. Each segment of the neourethra is reconstructed in a special fashion. The bulbar part is created by joining the anterior vaginal wall flap or periurethral tissue with the divided urethral plate's proximal part. This part is most susceptible to postoperative fistula formation, because it suffers the highest urinary stream pressure and must be additionally covered with clitoral bulbs and surrounding vascularized tissue. Penile neourethra is reconstructed by using buccal mucosa graft and vascularized genital skin flaps. The buccal mucosa graft has become a gold standard in urethral reconstruction due to its histological characteristics. 12 The graft is harvested from the inner cheek, properly fashioned, and fixed to cover the defect of the urethral plate, in order to create the posterior wall of the neourethra. It is also quilted to the cavernosal bodies for better survival. Minora flap or dorsal clitoral skin flap are then harvested as a ventral wall of the penile neourethra. The inner portion of labia minora is dissected to create a flap with excellent vascularization ( Figs. 3 A, B ). In the case of poorly developed labia minora, a well-vascularized longitudinal island flap is harvested from dorsal clitoral skin and transposed ventrally using the buttonhole maneuver. Either labial or skin flap is anastomosed with buccal mucosa graft over a 12/14-French catheter to create penile neourethra. All suture lines are covered with vascularized tissue to prevent urethral fistula ( Fig. 4 ). Split-thickness skin graft can be used as an alternative to buccal mucosa graft, and it is harvested from labia minora or other genital area. Vaginal mucosa graft is another option, which is harvested during vaginectomy. However, urethroplasty with buccal mucosa graft has the best outcomes and remains the method of choice. 10 13 The distal part of the neourethra is created by tubularization of the urethral plate, which is also incised in the midline in case it is not elastic enough. The penile shaft is reconstructed using the remaining clitoral and labia minora skin. The labia majora are joined in the midline to create the scrotum, and silicone testicular implants are inserted through bilateral incisions at the top of the labia majora ( Figs. 5 A, B ). A suprapubic catheter is placed for urine drainage in all cases over 3 weeks postoperatively. 13
Fig. 3.
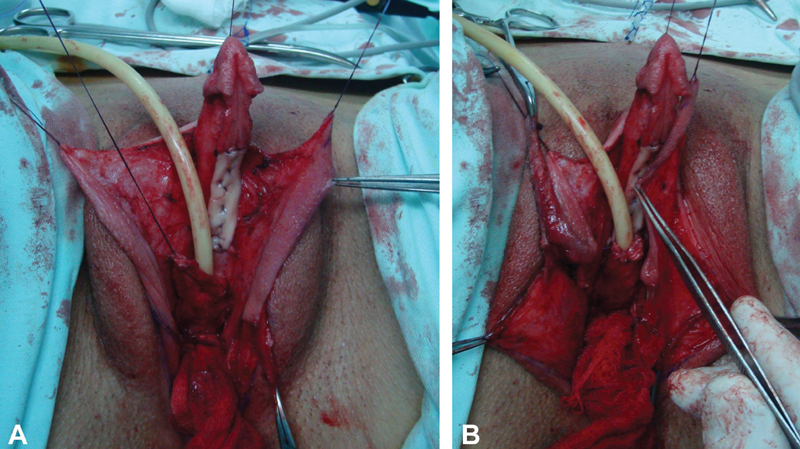
Urethral reconstruction. Defect after urethral plate transection is covered with buccal mucosa graft, which is fixed and quilted for better survival. ( A ). Bulbar urethra is created by joining of proximal urethral plate and vaginal flap. Flap from inner surface of left labia minora, with excellent vascularization, is created. ( B ). Labia minora flap is anastomosed with buccal mucosa graft to create penile neourethra.
Fig. 4.

Entire neourethra is created. Right labia minora flap is used to cover all suture lines.
Fig. 5.
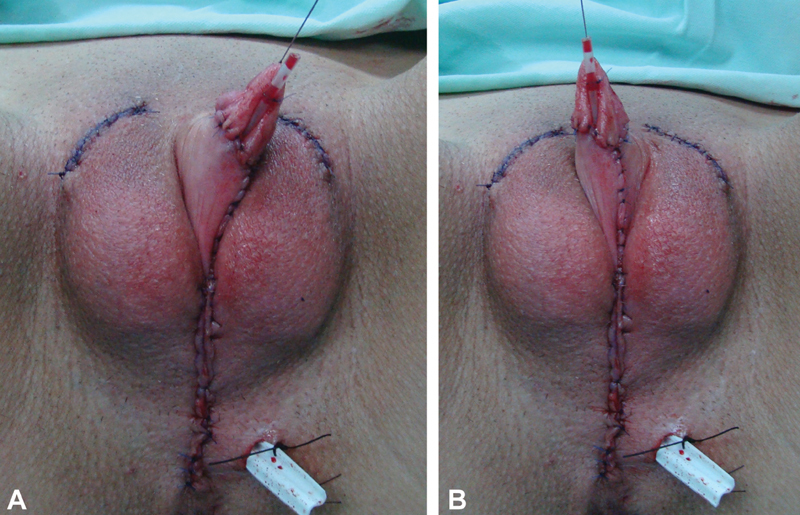
Final appearance. Penile skin reconstruction is done. Labia majora are joined in midline to create scrotum, and testicular implants are placed using suprascrotal incisions. A good relationship between the neophallus and scrotum is achieved. ( A ). Lateral view. ( B ). Ventral view.
Postoperative complications can be classified as minor and major. Minor complications are usually managed conservatively and include urinary infections, voiding issues like dribbling and spraying, partial skin necrosis or dehiscence, and local skin infection. Major complications include urethral (fistulas, strictures, diverticula), and nonurethral (displacement or rejection of testicular implants, perineal cyst or discharge) and require surgical repair. The most common complications are urethral fistula and stricture, which are reported in 7 to 15% and 2 to 5% of cases, respectively. However, the majority of patients are satisfied with the new appearance of their genitalia ( Fig. 6 ). All of them report good erection, sexual arousal, completely preserved erogenous sensation, as well as voiding while standing. Total phalloplasty is required in 12 to 15% of transmen after metoidioplasty, and it is feasible in all cases. 7 10 11 13
Fig. 6.

Outcome 6 months after surgery.
Recent Advances
Metoidioplasty technique has been modified and improved since its primary reports, mostly in urethral reconstruction. Initially, Laub performed the procedure in two steps to finalize urethroplasty in the second stage. 5 He used skin flaps or grafts for anastomosis of the native meatus and neourethra in the second stage. However, the rate of postoperative complications was high, and most of them were urethral fistulas that occurred at the point of anastomosis of the native urethra and neourethra. For this reason, Bouman introduced vaginal flap for reconstruction of bulbar urethra, and labial flaps for distal urethroplasty, with good short-term outcomes. 14 Still, long-term results showed a high level of urethral complications, and the neophallus was small and curved because the urethral plate remained intact. Hage reported that an average of 2.6 procedures was necessary to achieve optimal results in metoidioplasty, based on several studies. 15 New insights into female genital anatomy led to new approaches in metoidioplasty. Perovic and Hage performed reconstruction of the clitoris, which included transection of the urethral plate for maximal straightening and lengthening of the clitoral body. 16 17 Perovic published the results of metoidioplasty in 22 patients, with a mean follow-up of 3.9 years. 16 Three urethral fistulas and two strictures occurred in this period, and the mean penile length was 5.7 cm. Djordjevic used vast experience in severe hypospadias repair to improve outcomes in metoidioplasty. 18 In a series of 82 transmen who underwent a one-stage procedure, he reported urethral complications in 10.9% of cases (two urethral strictures and seven fistulas) in a mean follow-up of 32 months. The mean length of the neophallus and the neourethra were reported to be 5.7 cm and 11.3 cm, respectively. 19 Urethroplasty using buccal mucosa graft and labia minora flap proved to be the best option, with a low complication rate (7%). 20
The current metoidioplasty approach is based on the recognition in clitoral anatomy as well as the changes that occur to this anatomy with preoperative hormonal changes in transmen. 21 The clitoris has a fundamental role in female sexual functioning, and its main concerns, position, structure, and innervation, have been significantly clarified in recent studies on human cadavers and MRI. 22 The human penis and clitoris arise from the same embryological structure, genital tubercle, but the clitoris develops separately from the urethra. Although hormonal therapy in transmen leads to clitoral enlargement, the clitoral body remains shortened and curved due to attachments to the suspensory ligaments dorsally, short urethral plate ventrally, and labia minora. These attachments need to be released completely to achieve a good outcome and satisfy the patient. On the other hand, lengthening and straightening of the clitoris emphasized new refinements in urethral lengthening, with improved outcomes and acceptable complication rates. Although penetrative intercourse is not feasible due to the neophallus size, patients are mostly satisfied with the quality of erection, sensation of the neophallus, and sexual arousal, confirming good psychosexual outcome. 21 22
Recent advances in metoidioplasty techniques and multidisciplinary approach enabled safe and efficient one-stage surgery that includes the following: metoidioplasty with urethral lengthening and scrotoplasty, vaginectomy, hysterectomy, and bilateral mastectomy. 23 This procedure has many advantages, good aesthetic and functional outcomes, and a high patient satisfaction rate. A recent systematic review also revealed high aesthetic and sexual satisfaction in general after metoidioplasty. 24 Fistula rates ranged from 5% to 37%, while stricture ranged from 2% to 35% of cases. The Belgrade technique reported significantly lower rates of fistula and stricture compared with other techniques.
Personal Experience
Our one-stage approach was originally published in 2009 and significant advancement has been made since then, including possibility of combining metoidioplasty with hysterectomy and mastectomy in a one-stage procedure. 19 23 24 25 Belgrade metoidioplasty was performed at our center in 513 transmen, with a mean age of 31 years (ranging from 18 to 62 years), between 2007 and 2019. Out of 513 transmen, 151 underwent simultaneous hysterectomy and 84 had hysterectomy and bilateral mastectomy performed at the same stage with metoidioplasty. Urethral reconstruction was done with buccal mucosa graft combined with fasciocutaneous clitoral skin flap or labia minora flap. In 37 patients (7%), urethroplasty was performed by tubularization of wide and elastic urethral plate without transection. The mean length of the neophallus and neourethra was 6.5 cm (ranging between 4 cm to 10 cm) and 9.5 cm (ranging between 7.5 cm to 14 cm), respectively. Minor postoperative complications (spraying, urinary tract infections and wound dehiscence) occurred in 16% of cases and were managed conservatively. Urethral complications developed in 67 patients (fistula in 55, stricture in 12 patients) and were successfully repaired by minor surgical revision. Testicular implant rejection and dislocation also required revision surgery in 37 cases. In this group of 513 transmen, 47 developed postoperative complications related to vaginal remnants—perineal cyst formation with excessive mucus discharge, burning, or local infection. Voiding in standing position was achieved in all patients. There were no complications related to sexual function, meaning that all patients reported sexual arousal and orgasm. The majority of patients (465) were satisfied with the new appearance of their genitalia, and total phalloplasty was additionally required by 69 patients (13.5%).
Summary
Metoidioplasty is a variant of genital gender-affirmation surgery with well defined advantages and disadvantages. It presents an option for a select group of transmen, who prefer safe, one-stage procedure and do not have imperative of penetrative sexual intercourse. Fundamental principles of metoidioplasty were established 50 years ago and have remained to date. New insights in clitoral anatomy and urethral reconstruction, with improved operative techniques, shaped metoidioplasty to become a safe, one-stage surgery with good aesthetic and functional outcomes and high rate of patients' satisfaction. Thorough evaluation of every gender affirmation surgery and candidate results is necessary for successful outcomes.
Funding Statement
Funding This work is supported by the Ministry of Science and Technical Development, Republic of Serbia, Project No. 175048.
Footnotes
Conflict of Interest There are no conflicts of interest to declare.
References
- 1.Frey J D, Poudrier G, Chiodo M V, Hazen A. An update on genital reconstruction options for the female-to-male transgender patient: a review of the literature. Plast Reconstr Surg. 2017;139(03):728–737. doi: 10.1097/PRS.0000000000003062. [DOI] [PubMed] [Google Scholar]
- 2.Bizic M R, Stojanovic B, Djordjevic M L. Genital reconstruction for the transgendered individual. J Pediatr Urol. 2017;13(05):446–452. doi: 10.1016/j.jpurol.2017.07.015. [DOI] [PubMed] [Google Scholar]
- 3.Djordjevic M L. Novel surgical techniques in female to male gender confirming surgery. Transl Androl Urol. 2018;7(04):628–638. doi: 10.21037/tau.2018.03.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Durfee R, Rowland W.Penile substitution with clitoral enlargement and urethral transferIn: Laub DR, Gandy P, eds. Paper presented at: Proceedings of the Second Interdisciplinary Symposium on Gender Dysphoria Syndrome; 1973; Palo Alto, CA
- 5.Laub D R, Eicher W, Laub D R, II, Hentz V R. Berlin: Springer; 1989. Penis construction in female-to-male transsexuals; pp. 113–28. [Google Scholar]
- 6.Eicher W. Berlin: Springer; 1989. Surgical treatment of female-to-male transsexuals; pp. 106–12. [Google Scholar]
- 7.Bowers M L, Stojanovic B, Bizic M. New York: Thieme Medical Publishers Inc; 2017. Female-to-male gender affirmation metoidioplasty; pp. 109–18. [Google Scholar]
- 8.Takamatsu A, Harashina T. Labial ring flap: a new flap for metaidoioplasty in female-to-male transsexuals. J Plast Reconstr Aesthet Surg. 2009;62(03):318–325. doi: 10.1016/j.bjps.2008.11.038. [DOI] [PubMed] [Google Scholar]
- 9.Djordjevic M L, Majstorovic M, Stanojevic D. Combined buccal mucosa graft and dorsal penile skin flap for repair of severe hypospadias. Urology. 2008;71(05):821–825. doi: 10.1016/j.urology.2007.12.004. [DOI] [PubMed] [Google Scholar]
- 10.Djordjevic M L, Stojanovic B, Bizic M. Metoidioplasty: techniques and outcomes. Transl Androl Urol. 2019;8(03):248–253. doi: 10.21037/tau.2019.06.12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Djordjevic M L, Stojanovic B. Cham, Switzerland: Springer International Publishing AG; 2017. Metoidioplasty; pp. 573–7. [Google Scholar]
- 12.Markiewicz M R, Lukose M A, Margarone J E, III, Barbagli G, Miller K S, Chuang S K. The oral mucosa graft: a systematic review. J Urol. 2007;178(02):387–394. doi: 10.1016/j.juro.2007.03.094. [DOI] [PubMed] [Google Scholar]
- 13.Stojanovic B, Bizic M, Djordjevic M L. Cham, Switzerland: Springer International Publishing AG; 2020. Urethral reconstruction in female to male gender affirming surgery; pp. 883–96. [Google Scholar]
- 14.Bouman F G.The first step in phalloplasty in female transsexuals(Letter)Plast Reconstr Surg 19877904662–664. [PubMed] [Google Scholar]
- 15.Hage J J, van Turnhout A A. Long-term outcome of metaidoioplasty in 70 female-to-male transsexuals. Ann Plast Surg. 2006;57(03):312–316. doi: 10.1097/01.sap.0000221625.38212.2e. [DOI] [PubMed] [Google Scholar]
- 16.Perovic S V, Djordjevic M L. Metoidioplasty: a variant of phalloplasty in female transsexuals. BJU Int. 2003;92(09):981–985. doi: 10.1111/j.1464-410x.2003.04524.x. [DOI] [PubMed] [Google Scholar]
- 17.Hage J J. Metaidoioplasty: an alternative phalloplasty technique in transsexuals. Plast Reconstr Surg. 1996;97(01):161–167. doi: 10.1097/00006534-199601000-00026. [DOI] [PubMed] [Google Scholar]
- 18.Djordjevic M L, Bizic M, Stanojevic D. Urethral lengthening in metoidioplasty (female-to-male sex reassignment surgery) by combined buccal mucosa graft and labia minora flap. Urology. 2009;74(02):349–353. doi: 10.1016/j.urology.2009.02.036. [DOI] [PubMed] [Google Scholar]
- 19.Djordjevic M L, Stanojevic D, Bizic M. Metoidioplasty as a single stage sex reassignment surgery in female transsexuals: Belgrade experience. J Sex Med. 2009;6(05):1306–1313. doi: 10.1111/j.1743-6109.2008.01065.x. [DOI] [PubMed] [Google Scholar]
- 20.Djordjevic M L, Bizic M R. Comparison of two different methods for urethral lengthening in female to male (metoidioplasty) surgery. J Sex Med. 2013;10(05):1431–1438. doi: 10.1111/jsm.12108. [DOI] [PubMed] [Google Scholar]
- 21.Vukadinovic V, Stojanovic B, Majstorovic M, Milosevic A. The role of clitoral anatomy in female to male sex reassignment surgery. ScientificWorldJournal. 2014;2014:437378. doi: 10.1155/2014/437378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Stojanovic B, Djordjevic M L. Anatomy of the clitoris and its impact on neophalloplasty (metoidioplasty) in female transgenders. Clin Anat. 2015;28(03):368–375. doi: 10.1002/ca.22525. [DOI] [PubMed] [Google Scholar]
- 23.Stojanovic B, Bizic M, Bencic M. One-stage gender-confirmation surgery as a viable surgical procedure for female-to-male transsexuals. J Sex Med. 2017;14(05):741–746. doi: 10.1016/j.jsxm.2017.03.256. [DOI] [PubMed] [Google Scholar]
- 24.Jolly D, Wu C A, Boskey E R, Taghinia A H, Diamond D A, Ganor O. Is clitoral release another term for metoidioplasty? A systematic review and meta-analysis of metoidioplasty surgical technique and outcomes. Sex Med. 2021;9(01):100294. doi: 10.1016/j.esxm.2020.100294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bizic M R, Stojanovic B, Joksic I, Djordjevic M L. Metoidioplasty. Urol Clin North Am. 2019;46(04):555–566. doi: 10.1016/j.ucl.2019.07.009. [DOI] [PubMed] [Google Scholar]