

Abstract
Introduction: Secondary lesions in the breast from extramammary malignancies are rarely encountered in medical practice. Medical imaging of the breast (mammography and ultrasonography) may not differentiate between a primary breast mass and a secondary tumor from an extramammary malignancy.
Case description: A 90-year-old woman with a history of thyroid cancer, skin metastasis, thyroidectomy, and radiotherapy 12 years prior presented with pain in the left breast and no palpable masses in either breast or axilla. Mammography and ultrasonography of the breast confirmed a suspicious lesion in the upper outer quadrant of the left breast. Histopathology of the core biopsy, including immune histochemistry staining of the lesion, confirmed secondary follicular carcinoma of the thyroid.
Conclusion: Thyroid cancer is a rare extramammary malignancy that may metastasize to the breast; however, it may rarely occur a few years after thyroidectomy and radiotherapy.
Keywords: Extramammary breast secondary lesion, Follicular carcinoma of the thyroid, Mammography and breast ultrasound, Thyroidectomy and radiotherapy
Introduction
Despite being common among women with breast cancer, breast metastasis from an extramammary malignancy is rare. The sources of these extramammary malignancies vary but include lymphoma, leukemia, melanoma, lung, stomach, and ovarian tumors. In addition, other cancers, such as gastrointestinal, genitourinary, and thyroid tumors, have also been reported [1,2].
In terms of the methods of metastasis, the routes are hematogenous and lymphatic. Although their exact reasons or risk factors are not well known, they are believed to be hormonal.
Common radiological changes are not specific to metastases [2].
Case presentation
Here we report the case of a 90-year-old woman with a known history of thyroid cancer with ongoing skin and lung metastasis who presented with left breast pain and reported feeling a lump in the lower part of the left breast.
The patient had a past history of thyroid carcinoma with radiotherapy and thyroidectomy 12 years prior. She was orally administered levothyroxine (125 mcg) once daily. She had no family history of breast or ovarian cancer. She had limited mobility and was looked after twice daily by her caregiver.
A physical examination revealed mild tenderness in the upper lateral quadrant of the left breast, with no palpable masses in either breast or axilla. No palpable neck swelling was observed, and the rest of the clinical examination was unremarkable. However, a bilateral mammogram and left breast ultrasound identified an incidental finding of an 8-mm Breast Imaging Reporting and Data System (BI-RADS) 4 lesion in the 1D position in the left breast.
Radiologically, mammograms of both breast mediolateral oblique and craniocaudal views revealed an asymmetrical round lesion that could not be seen on the previous mammogram in 2014 (6 years prior). No suspicious features were observed in her right breast. The conclusion from the mammogram was a BI-RADS 1 for the right breast and a BI-RADS 4 for the left breast (Fig. 1)
Fig. 1.
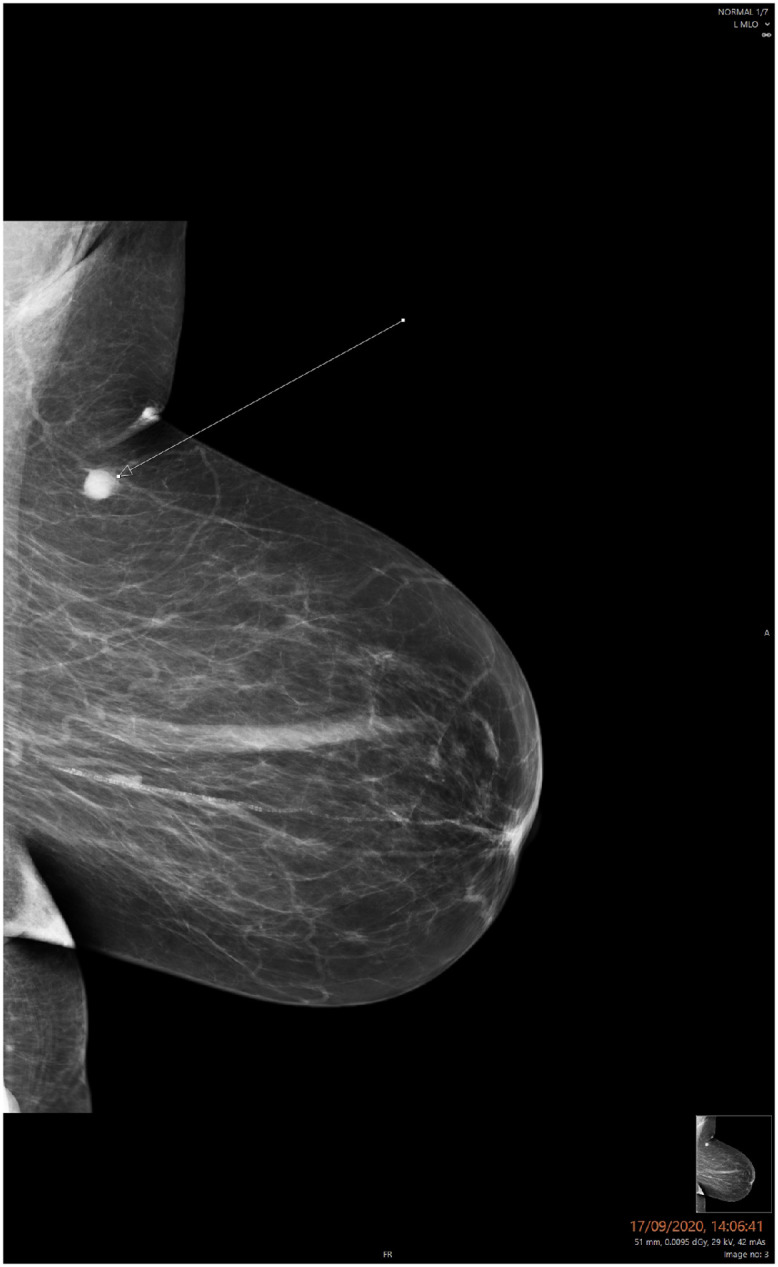
Mammogram of the left breast in the mediolateral oblique view showing an asymmetric mass in the upper outer part measuring 11 mm in diameter with suspicious features in keeping with a BI-RADS 4 lesion.
Ultrasonography confirmed the mammographic findings, and the lesion was hypoechoic with a lobulated wall. This finding could represent a breast lesion (suspicious for malignancy) or abnormal intramammary lymph node. The conclusion from the ultrasound was a BI-RADS4, considering the recency of the lesion compared with the previous scan (Fig. 2).
Fig. 2.
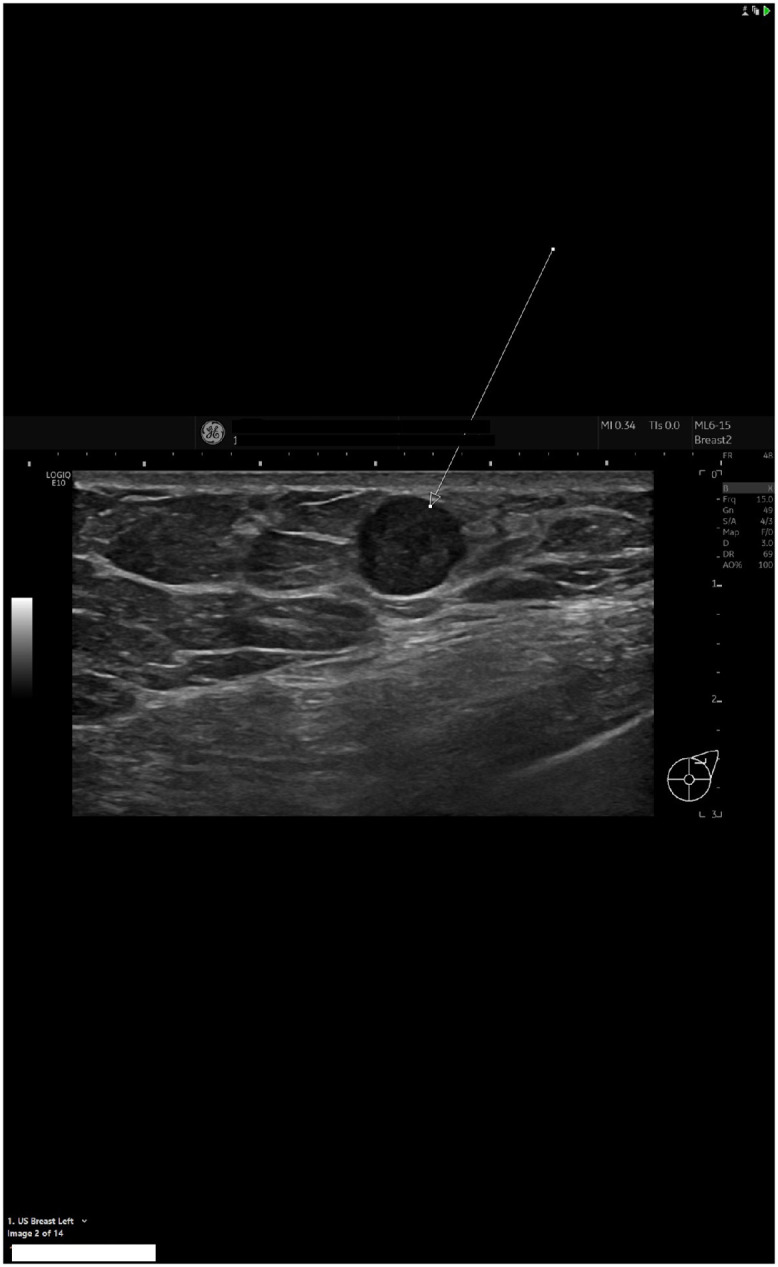
Ultrasound of the left breast revealed a hypoechoic mass measuring 10 mm in the widest diameter at 1 o'clock position with suspicious features consistent with a BI-RADS 4 lesion.
After verbal consent was obtained from the patient, a local anesthetic was injected and a core biopsy was taken from the lesion.
Histologically, the ultrasound-guided core biopsy of the left breast showed a metastatic thyroid follicular carcinoma. Macroscopically, it showed 2 cores, 13 and 9 mm, fragments; microscopically, the section showed a tumor composed of thyroid follicles filled with colloid. No residual breast tissue was identified (Figs. 3A and B).
Fig. 3.

(A) & (B) Histopathology of macroscopically 2 core biopsies of the left breast mass showing a tumor composed of thyroid follicles filled with colloid, without a residual breast tissue. (C) Histopathology of the left breast mass with TTF-1 immune stain revealed a thyroid transcription factor positive (TTF-1 positive) tumor.
The tumor was thyroid transcription factor-1-positive, estrogen receptor-negative, and progesterone receptor-negative (Fig. 3C).
The histological features were those of metastatic follicular carcinoma of the thyroid gland. There was no evidence of primary breast malignancy.
The patient was referred to the breast multidisciplinary team, but she declined any further intervention.
Discussion
The association between breast cancer and thyroid cancer was proven in a study of 13,798 patients with breast cancer in Fudan University Shanghai Cancer Center, Shanghai, China [3]. Both thyroid metastasis from breast cancer and breast metastasis from thyroid cancer have been reported [4].
The most common mammography findings of extramammary secondary lesions in the breast are single or multiple high-density mass (es); round, circumscribed, possibly micro-lobulated, or indistinct margins without a desmoplastic reaction, and uncommon calcifications [5].
The most common ultrasound findings of extramammary secondary lesions in the breast are round or oval mass/masses with circumscribed, indistinct, or micro-lobulated margins; skin thickening; edema; and enlarged lymph nodes (lymphatic dissemination) [5].
Metastasis from a thyroid tumor to the breast is extremely rare. Although mammography and cytology are helpful for detecting the origin of a tumor, they are not 100% accurate in all cases. Hence, it is difficult to detect the origin of all breast lumps or tumors. If we are still unable to distinguish between primary and secondary tumors, immunohistochemical techniques can be added to examine the aspirated material [6].
It is important to know whether the breast lump is a primary or secondary tumor (metastasis), as this affects the treatment plan. For example, in this case, the primary tumor was in the thyroid gland, while the metastasis is in the breast. Major surgery of the breast, such as mastectomy is not indicated [6].
Papillary carcinoma is the most common type of well-differentiated thyroid cancer (90% of cases). It usually presents as a lump or mass in the neck and rarely metastasizes (lung and bone are the commonest sites). Breast metastasis of thyroid cancer is rare, and only a few cases have been reported worldwide [6].
Medullary carcinoma of the thyroid gland, the other type, is more aggressive and mainly transmitted by blood and accounts for 5%-8% of cases [7].
A case of follicular papillary carcinoma was reported in 1991 in a patient with a history of goiter who developed a mass on the left breast. Both the fine needle aspiration biopsy from the goiter and the breast nodule showed thyroid follicular carcinoma on histological examination, which confirmed the origin of the primary tumor. The patient then underwent thyroidectomy with removal of the breast nodule. Fortunately, after 2 years, the patient was alive and well after iodine treatment [6].
Two other cases were reported, the first of which was seen in a 48-year-old woman who presented with a neck and breast mass that were confirmed to be thyroid follicular carcinoma with breast metastasis. She underwent a total thyroidectomy, and 4 weeks after the surgery, radioactive iodine intake showed skeletal metastasis. She underwent radiolabeling therapy, to which she showed a good response and she did well during follow-up [7].
The second case was a tall cell type, a type of thyroid papillary carcinoma that is known to have a more aggressive course with breast metastasis. Fortunately, no mammary metastasis has been reported to date [8].
In terms of genetic screening, there was a Spanish study of 2 cases of mutations reported in 2013 and 2017. There was a high epidermal growth factor receptor (EGFR) level, which was approved by a study to increase the proliferation of cancer cells. EGFR also plays a role in cancer cell migration and apoptosis. Therefore, this study recommended that anti-EGFR antibodies and EGFR kinase inhibitors may be useful in treating this type of malignancy [9].
In terms of prognosis and severity, compared with the other type (medullary), which is more aggressive, another case was reported in 2015 in a 67-year-old man who visited the hospital with medullary thyroid carcinoma with massive metastases to the bone, lungs, lymph nodes, and breast. The patient died 10 months later of extensive cancer extension [10]. Our patient declined further treatment and moved to another area.
Conclusion
Suspected primary vs secondary (extramammary) breast cancer lesions may not be differentiated by imaging.
Extramammary malignancies that may metastasize to the breast include lymphoma, leukemia, lung cancer, stomach cancer, ovarian cancer, genitourinary cancer, and thyroid cancer (extremely rare).
Unfortunately, secondary lesions in the breast from thyroid cancer may occur later after thyroidectomy and radiotherapy (as in our case report).
Patient consent
We authors of this case report declare that an informed consent was obtained for publication of this case report and all patient's personal data were kept anonymous in the text and images.
Footnotes
Competing Interests: All authors of the submitted manuscript declared that they did not have any conflict of interest regarding their case report, and they did not receive any type of fund for their work.
Supplementary material associated with this article can be found, in the online version, at doi:10.1016/j.radcr.2022.07.047.
Appendix. Supplementary materials
References
- 1.Akçay MN. Metastatic disease in the breast. Breast. 2002;11(6):526–528. doi: 10.1054/brst.2002.0467. PMID: 14965721. [DOI] [PubMed] [Google Scholar]
- 2.Mun SH, Ko EY, Han BK, Shin JH, Kim SJ, Cho EY. Breast metastases from extramammary malignancies: typical and atypical ultrasound features. Korean J Radiol. 2014;15(1):20–28. doi: 10.3348/kjr.2014.15.1.20. Epub 2014 Jan 8. PMID: 24497788; PMCID: PMC3909857. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Huang NS, Chen XX, Wei WJ, Mo M, Chen JY, Ma B, et al. Association between breast cancer and thyroid cancer: a study based on 13 978 patients with breast cancer. Cancer Med. 2018;7(12):6393–6400. doi: 10.1002/cam4.1856. Epub 2018 Nov 27. PMID: 30480382; PMCID: PMC6308067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Dettloff J, Seethala RR, Stevens TM, Brandwein-Gensler M, Centeno BA, Otto K, et al. Mammary Analog Secretory Carcinoma (MASC) involving the thyroid gland: a report of the first 3 cases. Head Neck Pathol. 2017;11(2):124–130. doi: 10.1007/s12105-016-0741-6. Epub 2016 Jul 11. PMID: 27400918; PMCID: PMC5429265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bitencourt AGV, Gama RRM, Graziano L, Negrão EMS, Sabino SMPS, Watanabe AHU, et al. Breast metastases from extramammary malignancies: multimodality imaging aspects. Br J Radiol. 2017;90(1077) doi: 10.1259/bjr.20170197. Epub 2017 May 25. PMID: 28485985; PMCID: PMC5858809. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cristallini EG, Ascani S, Nati S, Liberati F, Farabi R. Breast metastasis of thyroid follicular carcinoma. Acta Oncol. 1994;33(1):71–73. doi: 10.3109/02841869409098381. Erratum in: Acta Oncol 1994;33(2):224. PMID: 8037794. [DOI] [PubMed] [Google Scholar]
- 7.Nusrath S, Mahajan M, Rao TS, Raju KV, Murthy SS. Follicular variant of papillary thyroid cancer with breast metastasis. Indian J Surg Oncol. 2016;7(3):356–358. doi: 10.1007/s13193-016-0496-2. Epub 2016 Mar 29. PMID: 27651701; PMCID: PMC5016329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fiche M, Cassagnau E, Aillet G, Bailly J, Chupin M, Classe JM, et al. Métastase mammaire d'un carcinome papillaire à cellules hautes de la thyroïde [Breast metastasis from a "tall cell variant" of papillary thyroid carcinoma] Ann Pathol. 1998;18(2):130–132. French. PMID: 9608866. [PubMed] [Google Scholar]
- 9.Meng K, Chen W, Tian W, Sun K, Chen H. Medullary thyroid carcinoma with breast metastasis: two case reports. Medicine (Baltimore) 2018;97(47):e13193. doi: 10.1097/MD.0000000000013193. PMID: 30461619; PMCID: PMC6392924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Mandanas S, Margaritidou E, Christoforidou V, Karoglou E, Geranou C, Chrisoulidou A, et al. Breast metastasis from medullary thyroid carcinoma in a male patient: case report and review of the literature. Rare Tumors. 2015;7(2):5765. doi: 10.4081/rt.2015.5765. PMID: 26266011; PMCID: PMC4508642. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.