

Abstract
A 62‐year‐old man presented with a 3‐day history of dyspnea. Chest X‐ray revealed a pleural effusion. We performed chest tube drainage, and then the patient experienced re‐expansion pulmonary edema. His respiratory distress improved after the treatment of noninvasive positive pressure ventilation and intravenous methylprednisolone.
Keywords: complication, non‐cardiac pulmonary edema, thoracentesis, thoracostomy tube
Short abstract
Re‐expansion pulmonary edema is an uncommon complication of chest tube drainage. Early recognition of re‐expansion pulmonary edema is critical because it is a potentially fatal complication of chest tube drainage.
1. CASE HISTORY
A 62‐year‐old man with metastatic lung adenocarcinoma presented with a 3‐day history of dyspnea. Chest X‐ray demonstrated a pleural effusion (Figure 1A). We performed chest tube drainage, and cytology showed adenocarcinoma. Fifteen minutes after the insertion of the chest tube, the patient experienced acute distress with coughing. Approximately 1500 ml of pleural effusion had been drained via water‐seal drainage. Chest X‐ray showed the disappearance of almost all the pleural effusion and near‐complete lung re‐expansion (Figure 1B). About 2 h later, he became acutely distressed again with a productive cough. Chest X‐ray revealed ipsilateral pulmonary edema (Figure 1C). Re‐expansion pulmonary edema (RPE) was diagnosed. He was managed with noninvasive positive pressure ventilation (NPPV) and intravenous methylprednisolone. His respiratory distress gradually improved, and he was weaned from NPPV in 4 h.
FIGURE 1.
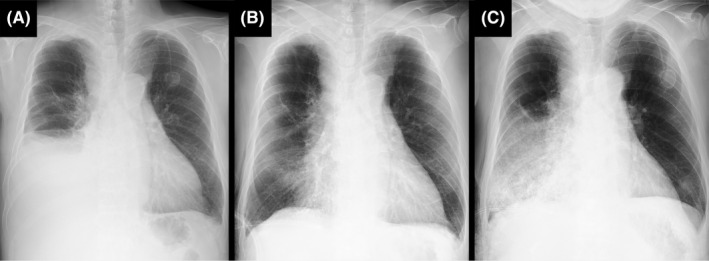
Chest X‐ray. (A) Before chest tube drainage, a pleural effusion occupied half of the right lung cavity. (B) Fifteen minutes after the insertion of the chest tube, almost all the pleural effusion disappeared. (C) Two hours after the insertion of the chest tube, ipsilateral pulmonary edema appeared
RPE is a complication of chest tube drainage, which occurs due to the re‐expansion of a collapsed lung. The incidence of RPE is higher following drainage for pneumothorax (16%) than that for pleural effusion (0.08%). 1 , 2 The mortality rate among patients with RPE has been reported to be as high as 25%. 2 Early recognition of RPE is critical because it is a potentially fatal complication of chest tube drainage.
AUTHOR CONTRIBUTIONS
SI and HS cared for the patient, collected the data, and drafted the manuscript. KN cared for the patient, collected the data, and revised the manuscript.
CONFLICT OF INTEREST
All of the authors declare no conflicts of interest.
CONSENT
Written consent was obtained from the patient.
ACKNOWLEDGEMENTS
None.
Inada S, Sugimoto H, Nakata K. Re‐expansion pulmonary edema after chest tube drainage of malignant pleural effusion. Clin Case Rep. 2022;10:e06088. doi: 10.1002/ccr3.6088
DATA AVAILABILITY STATEMENT
Data available on request from the authors.
REFERENCES
- 1. Yoon JS, Suh JH, Choi SY, et al. Risk factors for the development of reexpansion pulmonary edema in patients with spontaneous pneumothorax. J Cardiothorac Surg. 2013;8:164. doi: 10.1186/1749-8090-8-164 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Sagar AES, Landaeta MF, Adrianza AM, et al. Complications following symptom‐limited thoracentesis using suction. Eur Respir J. 2020;56:1902356. doi: 10.1183/13993003.02356-2019 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Data available on request from the authors.