

Abstract
Background
Electrochemotherapy (ECT) is a minimally invasive and safe treatment gaining positive and long-lasting antitumoral results that are receiving the attention of the scientific community. It is a local treatment that combines the use of electroporation and the administration of cytotoxic drugs to induce cell death in the target tissue. ECT is largely used for the treatment of cutaneous and subcutaneous lesions, and good results have been reported for the treatment of deep visceral tumors. The latest literature review is provided. Moreover, in line with its development for the treatment of visceral tumors in this article, we describe a novel approach of ECT: endoscopic treatment of colorectal cancer. Endoscopic ECT application was combined with systemic chemotherapy in the treatment of obstructing rectal cancer without prospective surgery. A good response after ECT was described: concentric involvement of the rectum was reduced, and no stenosing lesions were detected.
Conclusions
Clinical studies have demonstrated that ECT is a very effective treatment for tumors of different histologic types and localizations. Endoscopic treatment for gastrointestinal cancer is an innovative application of ECT. The combination of systemic treatment and ECT was safe and highly effective in the treatment of colorectal cancer, especially when obstructive, giving the patient a significant gain in quality of life.
Key words: electrochemotherapy, colorectal cancer, endoscopy
Introduction
Electrochemotherapy (ECT) is a local ablative therapy based on electroporation, a physical approach for enhanced delivery of cytotoxic drugs into tumors. Electroporation is the application of short-intensity high-voltage electric pulses to tumors, where it creates transient pores in the cell membrane of tumor cells and consequently increases the permeability of the cell membrane to allow hydrophilic drugs to enter the cytoplasm and induce cell death.1
Electroporation can be reversible or irreversible. Irreversible electroporation is a nonthermal ablation procedure employing multiple short-term electrical pulses that irreversibly destroy cells in the application area; reversible electroporation, on the other hand, can induce apoptosis instead of necrotic cell death due to the action of cytotoxic drugs, which can result in a superior immune effect. The reversibility or irreversibility of electroporation mainly depends on two electric pulse characteristics: electric field strength and time pulse length. For reversible electroporation, pulses of 1000 V/cm intensity and 100 μsec duration are used. In irreversible electroporation, higher electric field strengths or time pulse lengths are commonly used.2
Several clinically approved drugs have been tested in preclinical studies, but bleomycin and cisplatin are currently the most suitable and most commonly used chemotherapeutic drugs in association with ECT. In ECT after drug administration, a short time interval is needed for anticancer drugs, either administered intravenously or intratumorally, to distribute in the tumors. Bleomycin causes multiple DNA breaks and cisplatin intra- and interstrand DNA bonds in tumor cells. The cytotoxic effect of antitumoral drugs in ECT is increased 1000-fold for bleomycin and 80-fold for cisplatin.3
For several years, ECT has received attention in the scientific community because it is a minimally invasive and safe treatment, gaining positive and long-lasting antitumoral results. Great experience has been collected in the literature in the treatment of cutaneous and subcutaneous lesions, and in recent years, the first experiences with ECT treatment in deep-seated tumors have been reported with promising results.4
This article aims to describe the technique and clinical applications of ECT as a review of the latest publications. The review focuses on the treatment results and indications of this interesting treatment option. Furthermore, a new technical advancement is reported in a case of an obstructing rectal cancer not indicated for radiotherapy, treated with systemic chemotherapy combined with ECT, gaining systemic and local response after 3 months of FOLFOXIRI and bevacizumab chemotherapy and a single ECT treatment conducted endoscopically.
ECT indications, contraindications
The indication for ECT should be made by clinicians after a multidisciplinary team discussion to better evaluate the localization, size, characteristics of the lesions, general conditions and expected survival of the patient to define the purpose of the treatment. The technique can be applied in a variety of malignant lesions; fields of applications of ECT may be classified into three groups: treatment of cutaneous and subcutaneous lesions, treatment of deep metastases located in liver, bone, renal cancer, soft tissues and treatment of primary tumors.3 During patient selection, it is important to evaluate laboratory tests (number of platelets, coagulation, creatinine), cardiac, renal and lung function, body surface, and performance status (PS).
The choice of treatment modality is standardized for use in cutaneous and subcutaneous lesions.6 Physicians have to accurately select, on the basis of current recommendations, the employed drug (bleomycin or cisplatin), delivery route (intratumoral or intravenous), type of anesthesia (local or general) and type of electrodes.
The ECT procedure may vary depending on the size and location of the lesions. A correlation between tumor size and effectiveness of ECT has been evaluated for cutaneous and subcutaneous tumors by Mali et al. on cutaneous tumors: ECT was less effective on tumors larger than 3 cm. In the case of large lesions, the multiple application and repositioning of electrodes needs to be considered.7
As a standardized procedure in the treatment of deep-seated tumors is lacking, it is difficult to design a general ECT protocol.
The time of response may vary depending on tumor characteristics and adopted techniques: for cutaneous tumors, the 2-month follow-up time is used as a reference for response, but for deep-seated tumors, it is difficult to establish a specific follow-up scheduled time after ECT treatment.
ECT is not indicated in pregnancy or lactation or in cases of allergy or hypersensitivity to bleomycin or cisplatin.
Literature review
The earliest in vivo studies on the efficacy of ECT were carried out in the early 1990s: ECT was proven to be very efficient in animal studies, and safety and dosage were assessed in phase I and II studies.8, 9 Several drugs commonly used in clinical settings were experimentally investigated, and the data supported the role of bleomycin, a hydrophilic molecule, as the drug of choice for ECT and demonstrated an increase in carboplatin and cisplatin cytotoxicity when used in ECT.10
Treatment of cutaneous and subcutaneous tumor nodules was one of the first effective applications of ECT.05 The management of this tumor location often represents a challenge for clinicians, particularly when surgical excision is not possible or when lesions are radiotherapy-resistant.
Several trials confirmed the efficacy of ECT in the treatment of cutaneous and subcutaneous primary tumors or metastases from different malignancies (melanoma, basal cell carcinoma, squamous cell carcinoma, breast cancer, sarcomas): both bleomycin and cisplatin ECT were proven to be safe and well tolerated. Moreover, efficacy was excellent, reaching high objective response rates (ORs) and a high percentage of long-lasting responses. ECT was effective regardless of the histological type of tumor.11
The analysis of recent literature showed a wide variability according to the number, size and histological type of treated cutaneous and subcutaneous metastases.12, 13 Benevento et al. reported a 75.3% complete response (CR) and a 92.3% objective response rate (ORR) without intolerable side effects14 in breast cancer patients. Campana et al. identified a subgroup of elderly breast cancer patients as the most responsive to ECT.15 A recent review of the literature by a Swiss group confirmed ECT as a feasible, safe and easy-to-perform procedure; moreover, their analysis identified an OR rate for ECT across all the selected studies of 84.0%.16 Borgognoni et al. found similar results in the treatment of cutaneous melanoma metastases and rare nonmelanoma skin cancer: the OR rate was 88.6% in melanoma and 91.7% in nonmelanoma tumors.17 Caracò et al. reported a long-lasting response after ECT, with a mean duration of follow-up of 27.5 months for melanoma patients.18 Other authors analyzed data on ECT treatment of cutaneous metastasis from head and neck (HN) cancer and noticed a significant correlation between response to ECT and tumor size: ECT seems more effective in small tumor nodules (< 3 cm).19, 20
Because of the results obtained with ECT in cutaneous and lesions, many efforts have recently been made to translate the application of ECT into the treatment of non-superficial tumors. Preclinical in vitro studies were carried out on colorectal carcinoma cells, showing an increased cytotoxicity of bleomycin combined with electroporation.21
Bianchi et al. performed a prospective phase II trial to evaluate the safety and efficacy of ECT in the treatment of bone metastases.22 Twenty-nine patients affected by painful bone metastases from various malignancies in different skeleton sites were treated: 27 patients obtained a partial response (PR) or stable disease (SD) after 3 months, 20 patients reported improvement of pain condition (>50%) and reduction of consumption of analgesic drugs, and no complications were observed during and after ECT treatment. These results demonstrate that ECT might be safe and feasible for the treatment of painful bone metastases.
Furthermore, in 2014, a pilot study was performed on 16 patients to evaluate the feasibility, safety and efficacy of intraoperative ECT in the treatment of colorectal liver metastasis: the technique was proven to be safe (no serious adverse events were observed) and effective (85% of patients with complete response and 15% of those with partial response).23 A similar Italian study conducted in 2017 obtained comparable results.24
The long-term safety and effectiveness of ECT was recently confirmed in the treatment of colorectal liver metastases in the vicinity of major hepatic vessels and was thus unsuitable for surgery, radiofrequency or microwave ablation.25, 26
Based on the encouraging clinical results obtained in the treatment of colorectal liver metastases, Djokic et al. conducted a prospective pilot study to evaluate the role of ECT in the treatment of hepatocellular carcinoma (HCC).27 Ten patients resistant or not suitable for surgery or local ablative technique (TACE/RFA) were enrolled; they were treated with ECT during open surgery; bleomycin was the injected drug. Treatment was safe and well tolerated; at the first radiologic follow-up after 1 month, 88% of the lesions achieved a complete response (CR), and the others achieved a PR. The treatment was safe and effective even in tumors located in proximity to the hepatic or portal vessels and for tumors larger than 3 cm. ECT was shown to be a safe and effective treatment; it is minimally invasive with short hospitalization and good patient compliance; moreover, in selected cases, it may be considered a technique with curative intent; more studies need to be carried out to confirm these results. Recently, the first percutaneous ECT of HCC was performed.28
In 2018, Tarantino et al. published the results of the first study evaluating the safety and effectiveness of percutaneous ECT in the treatment of unresectable perihilar-cholangiocarcinoma (PHCCA).29 Five patients were enrolled in the study: two patients had CR, and in one patient, a complete restoration ad integrum of liver parenchyma and high local efficacy without hepatic recurrence during follow-up were observed. These results confirmed the efficacy of ECT, even in combination with systemic chemotherapy. An Italian group of works recently obtained similar results.30
In the last 10 years, several studies have been conducted to evaluate the potential adjunctive role of ECT and IRE in patients affected by locally advanced pancreatic cancer, who currently have a poor prognosis, with a 5-year survival rate of approximately 12%.31 Preclinical studies were performed to evaluate ECT’s role: the results of an animal study conducted on 10 mice with orthotropic human pancreatic carcinoma suggested that ECT might allow increased drug delivery in tumor cells, increasing gemcitabine efficacy and potentially reducing local tumor recurrence.32 IRE’s role has been evaluated in clinical studies: results of a multicenter prospective trial published in 2014 conducted on 200 patients with pancreatic cancer demonstrated that the addition of irreversible electroporation (IRE) to systemic chemotherapy could prolong survival.33 Irreversible laparotomic and laparoscopic electroporation in addition to systemic chemotherapy was performed in a total of 70 patients with locally advanced pancreatic cancer enrolled in a multicenter Asian study.34 The results suggested that adding IRE to chemotherapy might provide a survival advantage. The necessity to evaluate the combination of IRE and multidrug systemic chemotherapy for the treatment of pancreatic cancer led to the creation of the American Hepato-Pancreato-Biliary Association (AHPBA) Pancreatic Registry. Holland et al. reported initial outcomes of the AHPBA registry on 152 patients. The median overall survival (OS) was 30.7 months, the median progression-free survival (PFS) was 22.8 months, and the median time to tumor progression (TTP) was 27.3 months. The combination of ECT and systemic chemotherapy for pancreatic cancer is a safe treatment with encouraging survival.35
The efficacy of ECT was evaluated in the treatment of refractory cases of vulvar cancer in a multicenter observational study carried out in five Italian centers.36 Sixty-one patients were treated: a clinical response rate was obtained in 83.6% of cases, and the procedure was safe and well tolerated. Corrado et al. observed similar results in the palliative treatment of primary or recurrent vulvar cancer.37 The overall response rate (ORR) was 80% after 1 month, 61.5% of patients were alive at the 6-month follow-up and 50% at 1 year. ECT may have a role in the management of vulvar cancer in palliative setting. ECT with bleomycin may be considered also for vulvar metastasis to reduce pain and bleeding.38
ECT may be used for the treatment of different histological types of cancer. Andresciani et al. described the application of ECT as a treatment option in local recurrences of renal cell carcinoma 2 years after radical nephrectomy: ECT was effective, without evidence of residual disease 6 months after the procedure.01
Endoscopic treatment for gastrointestinal cancer is a novel application of ECT. The first human phase I study in patients affected by advanced esophageal cancer was conducted in 2018: ECT treatment was well tolerated, and tumor regression was gained and endoscopically confirmed in all patients.39
A similar phase I clinical study was conducted by Hansen et al. to investigate the safety and efficacy of endoscopically delivered ECT in patients with colorectal tumors.40 The results were encouraging: all the treated patients, elderly and with multiple comorbidities, were successfully treated and gained local complete or partial tumor response after one treatment; the procedure was well tolerated without relevant side effects.
Case report
A 61-year-old male patient affected by metastatic colorectal cancer was treated by ECT in January 2021. The study was conducted in accordance with the Declaration of Helsinki and informed consent was obtained, also for the publication of the results. The patient had no known significant comorbidity; he was overweight and suffered from hypertension controlled with therapies. The diagnosis of cancer was obtained in November 2020. During the colonoscopy, a substenosing, ulcerated bleeding lesion was observed from 20 cm to 10 cm before the anal edge. The lesion was histologically proven to be poorly differentiated adenocarcinoma.
At the basal CT scan, multiple hepatic lesions and a single lung metastasis were described.
The low abdominal MRI, performed in December 2020 (Figure 1A), described a bulky pathological cancer mass extending from the distal part of the sigma to the rectum until 8 centimeters from the anal border. The rectum was concentrically involved by the tumor, and local nodes were increased in volume.
Figure 1.
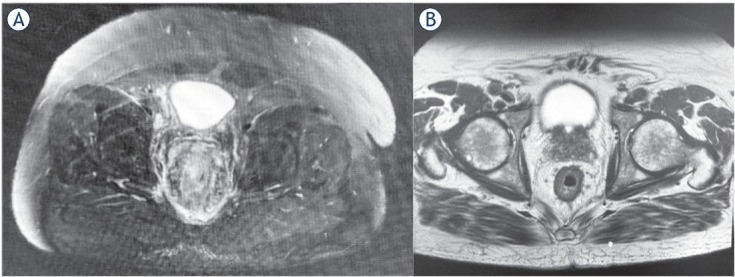
(A) NMR imaging before Electrochemotherapy (ECT) and (B) follow-up evaluation 4 weeks after the ECT session.
The radiotherapist rejected the possibility of combined chemoradiotherapy: local radiotherapy was not indicated because of the high risk of colorectal obstruction.
First-line systemic chemotherapy with fluorouracil, leucovorin, irinotecan and oxaliplatin (FOLFOXIRI) plus BEVACIZUMAB was started in December 2020.
Four cycles of chemotherapy were led between December 2020 and January 2021; therapy was well tolerated, and a dose reduction of 25% of IRINOTECAN was required for IV cycles of gastroenteric G3 toxicity therapy.
At the first abdominal MRI evaluation (Figure 1B), a good response was described. Concentrical involvement of the rectum was reduced, there were no stenosing lesions, and pathological local nodes were reduced in volume and number.
Local treatment with ECT was endoscopically conducted in the region of colorectal cancer by employing colonoscopy. One day before the treat
ment, physical examination, laboratory tests and cardiologic evaluation were carried out. Treatment was performed under general anesthesia (deep sedation with Propofol) with standard hemodynamic monitoring.
This procedure was conducted in the presence of a multidisciplinary team constituted by an oncologist, gastroenterologist, anesthetist and specialized nurse. The Cliniporator EPS-02 produced by IGEA was used. Software was used to optimize the placement of electrodes in the predefined area. Electric pulses were delivered by linear needle electrodes. The electrode used (Stinger E_L2_00_S4) has been developed by IGEA and is dedicated to laparoscopic/endoscopic approach, being equipped with a long connector cable (20 cm) and 4 expandable needle electrodes positioned at a fixed distance of 0.4 cm in a square geometry and parallel one to each other. Total needle electrode length is 4 cm, with an active part at the 2 cm extremity (Figure 2)
Figure 2.
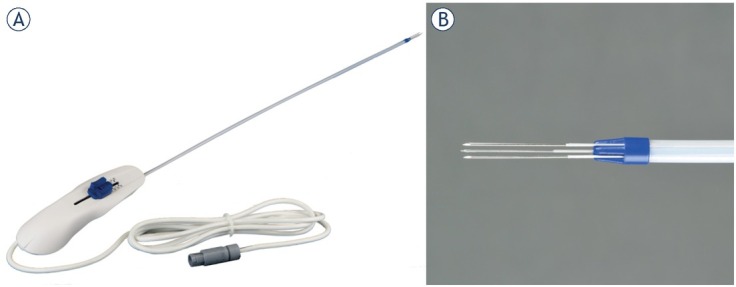
The new Stinger electrode. (A) The overall support with the connecting cable. (B) The needle expandable electrodes at the extremity.
In accordance with European Standard Operating Procedures of Electrochemotherapy (ESOPE) guidelines, ECT was performed 8 minutes after the end of slow bleomycin intravenous infusion (bleomycin 15000 IU/m2 of body surface area diluted in 100 cc of physiologic solution in 10 minutes).05
Rectosigmoidoscopy was performed, and then the electrode was endoscopically introduced to perform electroporation of the lesion (Figure 3). Five applications of the electric pulses were performed with repositioning of the electrode, in order to completely cover the lesion.
Figure 3.

Electrochemotherapy (ECT) session. (A) before ECT, (B) electrode positioning, (C) at the 4-week follow-up.
The duration of the procedure was 30 minutes. Antibiotic prophylaxis with cephalosporin was employed. The hospitalization time was 2 days.
The procedure was well tolerated, without side effects.
At the first colonoscopy performed 4 days after ECT treatment, tumor downstaging was confirmed, the endoscopic device could easily pass through the lesions, and all the colon tubes were studied. Moreover, at the total body CT performed 4 weeks after ECT treatment, lung and hepatic metastasis were reduced in volume (Figure 1B, 2C).
Systemic chemotherapy treatment was carried out after the procedure. After one month, no adverse events were reported; moreover, the patient reported a reduction in gastroenteric symptomatology and a subjective improvement in his wellbeing and quality of life.
Conclusions
ECT was the main topic of the present article. Literature data show the role of ECT as both curative and palliative treatment, improving quality of life of patients with different tumour types.
Moreover, the present article described our center’s preliminary experience with ECT combined with standard systemic chemotherapy in the treatment of advanced colorectal adenocarcinoma not indicated for surgery or radiotherapy.
The combination of systemic treatment and ECT was highly effective and safe in the treatment of this tumor: a good local response was observed with a resolution of the local stenosis caused by cancer and an improvement in patient quality of life because of a reduction in gastroenteric symptoms.
To the best of our knowledge, at the time of writing this paper, no data concerning colorectal endoscopic ECT treatment are available. Preliminary results may be considered a proof of concept for future prospective studies that are needed to confirm these data.
Disclosure
No potential conflicts of interest were disclosed.
References
- 1.Andresciani F, Faiella E, Altomare C, Pacella G, Beomonte Zobel B, Grasso RF. Reversible electrochemotherapy (ECT) as a treatment option for local RCC recurrence in solitary kidney. Cardiovasc Intervent Radiol. 2020;43:1091–4. doi: 10.1007/s00270-020-02498-2. [DOI] [PubMed] [Google Scholar]
- 2.Ritter A, Bruners P, Isfort P, Barabasch A, Pfeffer J, Schmitz J. Electroporation of the liver: more than 2 concurrently active, curved electrodes allow new concepts for irreversible electroporation and electro-chemotherapy. Technol Cancer Res Treat. 2018;17:153303381880999. doi: 10.1177/1533033818809994. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Probst U, Fuhrmann I, Beyer L, Wiggermann P. Electrochemotherapy as a new modality in interventional oncology: a review. Technol Cancer Res Treat. 2018;17:153303381878532. doi: 10.1177/1533033818785329. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Leiter U, Gutzmer R, Alter M, Ulrich C, Meiwes A, Heppt MV. [Cutaneous squamous cell carcinoma] [German]. Hautarzt. 2020;71:597–606. doi: 10.1007/s00105-020-04620-4. et al. [DOI] [PubMed] [Google Scholar]
- 5.Marty M, Sersa G, Garbay JR, Gehl J, Collins CG, Snoj M. Electrochemotherapy – an easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur J Cancer Suppl. 2006;4:3–13. doi: 10.1016/j.ejcsup.2006.08.002. et al. [DOI] [Google Scholar]
- 6.Gehl J, Sersa G, Matthiessen LW, Muir T, Soden D, Occhini A. Updated standard operating procedures for electrochemotherapy of cutaneous tumours and skin metastases. Acta Oncologica. 2018;57:874–82. doi: 10.1080/0284186X.2018.1454602. et al. [DOI] [PubMed] [Google Scholar]
- 7.Mali B, Miklavcic D, Campana LG, Cemazar M, Sersa G, Snoj M. Tumor size and effectiveness of electrochemotherapy. Radiol Oncol. 2013;47:32–41. doi: 10.2478/raon-2013-0002. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mir LM, Orlowski S, Belehradek J, Paoletti C. Electrochemotherapy potentiation of antitumour effect of bleomycin by local electric pulses. Eur J Cancer Clin Oncol. 1991;27:68–72. doi: 10.1016/0277-5379(91)90064-K. [DOI] [PubMed] [Google Scholar]
- 9.Belehradek M, Domenge C, Luboinski B, Orlowski S, Belehradek J, Mir LM. Electrochemotherapy, a new antitumor treatment. First clinical phase I-II trial. Cancer. 1993;72:3694–700. doi: 10.1002/1097-0142(19931215). 72:12<3694::aid-cncr2820721222>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 10.Gehl J, Skovsgaard T, Mir LM. Enhancement of cytotoxicity by electropermeabilization: an improved method for screening drugs. Anticancer Drugs. 1998;9:319–25. doi: 10.1097/00001813-199804000-00005. [DOI] [PubMed] [Google Scholar]
- 11.Mir LM, Glass LF, Sersa G, Teissié J, Domenge C, Miklavcic D. Effective treatment of cutaneous and subcutaneous malignant tumours by electrochemotherapy. Br J Cancer. 1998;77:2336–42. doi: 10.1038/bjc.1998.388. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ferioli M, Perrone AM, Buwenge M, Arcelli A, Zamagni A, Macchia G. Electrochemotherapy of skin metastases from breast cancer: a systematic review. Clin Exp Metastasis. 2021;38:1–10. doi: 10.1007/s10585-020-10063-x. et al. [DOI] [PubMed] [Google Scholar]
- 13.Crimini E, Roberto M, Degli Effetti V, Marchetti P, Botticelli A, Schipilliti FM. Electrochemotherapy as promising treatment option in rare recurrent cutaneous neoplasm of the scalp: case report of an elderly patient. Case Rep Oncol Med. 2019;2019:2507642. doi: 10.1155/2019/2507642. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Benevento R, Santoriello A, Perna G, Canonico S. Electrochemotherapy of cutaneous metastasis from breast cancer in elderly patients: a preliminary report. BMC Surg. 2012;12(Suppl 1):S6. doi: 10.1186/1471-2482-12-S1-S6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Campana LG, Galuppo S, Valpione S, Brunello A, Ghiotto C, Ongaro A. Bleomycin electrochemotherapy in elderly metastatic breast cancer patients: clinical outcome and management considerations. J Cancer Res Clin Oncol. 2014;140:1557–65. doi: 10.1007/s00432-014-1691-6. et al. [DOI] [PubMed] [Google Scholar]
- 16.Seyed Jafari SM, Jabbary Lak F, Gazdhar A, Shafighi M, Borradori L, Hunger RE. Application of electrochemotherapy in the management of primary and metastatic cutaneous malignant tumours: a systematic review and meta-analysis. Eur J Dermatol. 2018;28:287–313. doi: 10.1684/ejd.2018.3291. [DOI] [PubMed] [Google Scholar]
- 17.Borgognoni L, Pescitelli L, Gerlini G, Brandani P, Gelli R, Giannotti V. Efficacy of electrochemotherapy in the treatment of cutaneous melanoma metastases and rare non-melanoma skin cancer. Anticancer Res. 2020;40:6485–92. doi: 10.21873/anticanres.14670. et al. [DOI] [PubMed] [Google Scholar]
- 18.Caracò C, Mozzillo N, Marone U, Simeone E, Benedetto L, Di Monta G. Long-lasting response to electrochemotherapy in melanoma patients with cutaneous metastasis. BMC Cancer. 2013;13:564. doi: 10.1186/1471-2407-13-564. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Bertino G, Sersa G, De Terlizzi F, Occhini A, Plaschke CC, Groselj A. European Research on Electrochemotherapy in Head and Neck Cancer (EURECA) project: results of the treatment of skin cancer. Eur J Cancer. 2016;63:41–52. doi: 10.1016/j.ejca.2016.05.001. et al. [DOI] [PubMed] [Google Scholar]
- 20.Clover AJP, de Terlizzi F, Bertino G, Curatolo P, Odili J, Campana LG. Electrochemotherapy in the treatment of cutaneous malignancy: outcomes and subgroup analysis from the cumulative results from the pan-European International Network for Sharing Practice in Electrochemotherapy database for 2482 lesions in 987 patients (2008-2019) Eur J Cancer. 2020;138:30–40. doi: 10.1016/j.ejca.2020.06.020. et al. [DOI] [PubMed] [Google Scholar]
- 21.Todorovic V, Sersa G, Flisar K, Cemazar M. Enhanced cytotoxicity of bleomycin and cisplatin after electroporation in murine colorectal carcinoma cells. Radiol Oncol. 2009;43:264–73. doi: 10.2478/v10019-009-0037-5. [DOI] [Google Scholar]
- 22.Bianchi G, Campanacci L, Ronchetti M, Donati D. Electrochemotherapy in the treatment of bone metastases: a phase II trial. World J Surg. 2016;40:3088–94. doi: 10.1007/s00268-016-3627-6.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Edhemovic I, Brecelj E, Gasljevic G, Marolt Music M, Gorjup V, Mali B. Intraoperative electrochemotherapy of colorectal liver metastases. J Surg Oncol. 2014;110:320–7. doi: 10.1002/jso.23625. et al. [DOI] [PubMed] [Google Scholar]
- 24.Coletti L, Battaglia V, De Simone P, Turturici L, Bartolozzi C, Filipponi F. Safety and feasibility of electrochemotherapy in patients with unresectable colorectal liver metastases: a pilot study. Internat J Surg. 2017;44:26–32. doi: 10.1016/j.ijsu.2017.06.033. [DOI] [PubMed] [Google Scholar]
- 25.Edhemovic I, Brecelj E, Cemazar M, Boc N, Trotovsek B, Djokic M. Intraoperative electrochemotherapy of colorectal liver metastases: a prospective phase II study. Eur J Surg Oncol. 2020;46:1628–33. doi: 10.1016/j.ejso.2020.04.037. et al. [DOI] [PubMed] [Google Scholar]
- 26.Edhemovic I, Gadzijev EM, Brecelj E, Miklavcic D, Kos B, Zupanic A. Electrochemotherapy: a new technological approach in treatment of metastases in the liver. Technol Cancer Res Treat. 2011;10:475–85. doi: 10.7785/tcrt.2012.500224. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Djokic M, Cemazar M, Popovic P, Kos B, Dezman R, Bosnjak M. Electrochemotherapy as treatment option for hepatocellular carcinoma, a prospective pilot study. Eur J Surg Oncol. 2018;44:651–7. doi: 10.1016/j.ejso.2018.01.090. et al. [DOI] [PubMed] [Google Scholar]
- 28.Djokic M, Dezman R, Cemazar M, Stabuc M, Petric M, Smid LM. Percutaneous image guided electrochemotherapy of hepatocellular carcinoma: technological advancement. Radiol Oncol. 2020;54:347–52. doi: 10.2478/raon-2020-0038. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Tarantino L, Busto G, Nasto A, Nasto RA, Tarantino P, Fristachi R. Electrochemotherapy of cholangiocellular carcinoma at hepatic hilum: a feasibility study. Eur J Surg Oncol. 2018;44:1603–9. doi: 10.1016/j.ejso.2018.06.025. et al. [DOI] [PubMed] [Google Scholar]
- 30.Granata V, Palaia R, Albino V, Piccirillo M, Venanzio Setola S, Petrillo A. Electrochemotherapy of cholangiocellular carcinoma at hepatic hilum: a case report. Eur Review Med Pharmacol Sci. 2020;24:7051–7. doi: 10.26355/eurrev_202006_21698. et al. [DOI] [PubMed] [Google Scholar]
- 31.Bhutiani N, Li Y, Zheng Q, Pandit H, Shi X, Chen Y. Electrochemotherapy with irreversible electroporation and FOLFIRINOX improves survival in murine models of pancreatic adenocarcinoma. Ann Surg Oncol. 2020;27:4348–59. doi: 10.1245/s10434-020-08782-2. et al. [DOI] [PubMed] [Google Scholar]
- 32.Bhutiani N, Agle S, Li Y, Li S, Martin RCG. Irreversible electroporation enhances delivery of gemcitabine to pancreatic adenocarcinoma. J Surg Oncol. 2016;114:181–6. doi: 10.1002/jso.24288. [DOI] [PubMed] [Google Scholar]
- 33.Martin RCG, Kwon D, Chalikonda S, Sellers M, Kotz E, Scoggins C. Treatment of 200 locally advanced (stage III) pancreatic adenocarcinoma patients with irreversible electroporation: safety and efficacy. Ann Surg. 2015;262:486–94. doi: 10.1097/SLA.0000000000001441. et al. discussion 492-494. [DOI] [PubMed] [Google Scholar]
- 34.Huang K-W, Yang P-C, Pua U, Kim M-D, Li S-P, Qiu Y-D. The efficacy of combination of induction chemotherapy and irreversible electroporation ablation for patients with locally advanced pancreatic adenocarcinoma. J Surg Oncol. 2018;118:31–6. doi: 10.1002/jso.25110. et al. [DOI] [PubMed] [Google Scholar]
- 35.Holland MM, Bhutiani N, Kruse EJ, Weiss MJ, Christein JD, White RR. A prospective, multi-institution assessment of irreversible electroporation for treatment of locally advanced pancreatic adenocarcinoma: initial outcomes from the AHPBA pancreatic registry. HPB (Oxford) 2019;21:1024–31. doi: 10.1016/j.hpb.2018.12.004. et al. [DOI] [PubMed] [Google Scholar]
- 36.Perrone AM, Cima S, Pozzati F, Frakulli R, Cammelli S, Tesei M. Palliative electro-chemotherapy in elderly patients with vulvar cancer: a phase II trial: electro-chemotherapy in vulvar cancer. J Surg Oncol. 2015;112:529–32. doi: 10.1002/jso.24036. et al. [DOI] [PubMed] [Google Scholar]
- 37.Corrado G, Cutillo G, Fragomeni SM, Bruno V, Tagliaferri L, Mancini E. Palliative electrochemotherapy in primary or recurrent vulvar cancer. Int J Gynecol Cancer. 2020;30:927–31. doi: 10.1136/ijgc-2019-001178. et al. [DOI] [PubMed] [Google Scholar]
- 38.Merlo S, Vivod G, Bebar S, Bošnjak M, Čemažar M, Serša G. Literature review and our experience with bleomycin-based electrochemotherapy for cutaneous vulvar metastases from endometrial cancer. Technol Cancer Res Treat. 2021;20:15330338211010134. doi: 10.1177/15330338211010134. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Egeland C, Baeksgaard L, Johannesen HH, Löfgren J, Plaschke CC, Svendsen LB. Endoscopic electrochemotherapy for esophageal cancer: a phase I clinical study. Endosc Int Open. 2018;6:E727–34. doi: 10.1055/a-0590-4053. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Falk Hansen H, Bourke M, Stigaard T, Clover J, Buckley M, O’Riordain M. Electrochemotherapy for colorectal cancer using endoscopic electroporation: a phase 1 clinical study. Endosc Int Open. 2020;8:E124–32. doi: 10.1055/a-1027-6735. et al. [DOI] [PMC free article] [PubMed] [Google Scholar]