

Abstract
Background:
There is limited evidence on how cigarette smokers use electronic cigarettes (ECIGs) for smoking cessation and reduction. This study used concept mapping, a participatory mixed-methods research approach, to identify ECIG use behaviors and device characteristics perceived to be associated with cigarette smoking cessation or reduction.
Methods:
Current ECIG users aged 18–64 were recruited from seven cities selected randomly from U.S. census tract regions. Participants were invited to complete concept mapping tasks: brainstorming, sorting and rating (n=72). During brainstorming, participants generated statements in response to a focus prompt (“A SPECIFIC WAY I HAVE USED electronic cigarettes to reduce my cigarette smoking or a SPECIFIC WAY electronic cigarettes help me reduce my cigarette smoking is…”) and then sorted and rated the statements. Multidimensional scaling and hierarchical cluster analyses were used to generate a cluster map that was interpreted by the research team.
Results:
Eight thematic clusters were identified: Convenience, Perceived Health Effects, Ease of Use, Versatility and Variety, Advantages of ECIGs over Cigarettes, Cigarette Substitutability, Reducing Harms to Self and Others, and Social Benefits. Participants generated several statements that related to specific behavioral strategies used when using ECIGs for smoking reduction/complete switching behaviors such as making rapid transitions from smoking to ECIG use or using certain ECIG liquids or devices. Former smokers rated the Perceived Health Effects cluster and several behavioral strategy statements higher than current smokers.
Conclusions:
These results help to identify ECIG use behaviors and characteristics perceived by ECIG users to aid in cigarette smoking cessation or reduction.
Keywords: electronic cigarettes, smoking cessation, smoking reduction, perceptions, concept mapping
1. Introduction
Electronic cigarettes (ECIGs) are a class of products that heat and aerosolize a liquid containing propylene glycol (PG), vegetable glycerin (VG), nicotine, and chemical flavorants (Breland et al., 2016). ECIGs have become increasingly popular in the U.S. with dramatic increases observed since 2011 among youth (US Department of Health and Human Services, 2016) and adults (McMillen et al., 2015). Reported reasons for ECIG use include curiosity (Berg et al., 2015; Li et al., 2015) and perceived lower financial cost compared to cigarettes (Kadimpati et al., 2015; Soule et al., 2016c), but the reason reported most commonly among adults is smoking cessation or reduction (Adkison et al., 2013; Berg, et al., 2015; Brown et al., 2014; Goniewicz, et al., 2013; Hummel et al., 2015; Kadimpati, et al., 2015; Kralikova, et al., 2013; Li, et al., 2015; Mark, et al., 2015; Pepper, et al., 2014; Peters et al., 2015; Richardson, et al., 2014; Soule et al., 2016c; Stein et al., 2015). However, there is a limited evidence base on their effectiveness in aiding cigarette smoking cessation or reduction (Kalkhoran and Glantz, 2016; McRobbie et al., 2014).
A comprehensive review (Glasser et al., 2017) identified randomized controlled trials (Adriaens et al., 2014; Bullen et al., 2013; Caponnetto et al., 2013; Tseng et al., 2016) that have shown ECIG use was associated with smoking cessation or reduction for some smokers, but also longitudinal cohort studies (Adikson et al., 2013; Al-Delaimy et al., 2015; Grana et al., 2014; Pearson et al., 2015; Vickerman et al., 2013; Vickerman et al., 2017) that have shown no effect or negative effect of ECIG use on smoking cessation. Much of this recent research on ECIG use has focused on the extent to which cigarette smokers use ECIGs and how ECIG use status is associated with smoking status. For example, a recent meta-analysis reported that ECIG use is associated with continued smoking (Kalkhoran & Glantz, 2016) while other studies examining national survey data report that ECIG use is associated with smoking cessation (Zhu et al., 2017). However, these and other studies often focus on if smokers use ECIGs, but do not assess how smokers use ECIGs. Because ECIGs are a diverse class of products that allow for diverse user behaviors, research should examine how cigarette smokers use ECIGs for smoking cessation and reduction in addition to if cigarette smokers use ECIGs for smoking cessation and reduction. An understanding of the different types of behaviors and ECIG device characteristics that ECIG users report, especially those perceived to be associated with cigarette smoking cessation, may help explain why some cigarette smokers who use ECIGs continue to smoke while others reduce or quit smoking completely. Furthermore, a more thorough analysis of ECIG use behaviors and device characteristics may help identify strategies for aiding cigarette smokers in switching completely to ECIGs as a possible harm reduction approach.
Research that identifies ECIG use behaviors and device characteristics that are associated with cigarette smoking cessation or reduction can inform regulation by identifying characteristics of ECIG products and behaviors that have the greatest potential for positive and negative public health impact. However, national surveillance systems are often not sufficient to capture the diverse ECIG use characteristics and behaviors that may be associated with cigarette smoking cessation or reduction. Methods that allow for in-depth examination of ECIG use behaviors where users can describe their own experiences are needed to understand the association between ECIG use and cigarette smoking cessation or reduction. Concept mapping (CM; Kane & Trochim, 2007; Trochim, 1989), a mixed-method participatory approach, is such a method that has been used previously to examine ECIG use behaviors (Soule et al., 2016a, 2016b, 2016c, 2017). Importantly, this method allows individuals with firsthand knowledge on a topic (i.e., experienced ECIG users who self-report having decreased cigarette smoking by using ECIGs) to generate, organize, and rate importance of content related the research topic. CM also yields similar results compared to other methods such as exploratory factor analysis, but has unique advantages including being able to be completed in a relatively short time frame without the need of a large sample and generating a useful visual representation of the final framework. Therefore, the purpose of this study was to use CM to identify ECIG use behaviors and device characteristics that ECIG users perceive to be associated with cigarette smoking cessation or reduction. We hypothesized that some strategies and device characteristics identified by ECIG users would be more associated with complete switching from cigarette smoking to ECIGs than others.
2. Methods
2.1. Participants
This study was approved by the Virginia Commonwealth University Institutional Review Board. Past-30 day ECIG users between the ages of 18 and 64 who self-reported cigarette smoking reduction by using ECIGs were recruited by posting advertisements on Craigslist classified pages in a total of seven cities selected randomly from each U.S. census tract region (Northeast, Midwest, South, West; as in Soule et al., 2017). This method yields a more generalizable sample which ensures participation from individuals across the U.S. and results in a more diverse sample compared to other CM studies that recruited ECIG users from ECIG Internet forums (e.g., Soule et al., 2016c). Advertisements also were sent directly to ECIG users who were part of an IRB-approved research registry created using similar recruitment procedures (i.e. Craigslist advertisements). Individuals who were interested in the study contacted study staff and were screened for inclusion. Individuals who were not 18–64 years old, non-U.S. citizens, non-ECIG users, ECIG users who had not smoked 100 cigarettes in their lives, and individuals who did not report reducing cigarette smoking by using ECIGs were excluded. One hundred two individuals were contacted for screening and 18 were ineligible (14 reported smoking less than 100 lifetime cigarettes, 2 did not self-report reducing cigarette smoking using ECIGs, 2 were not U.S. citizens). Participants provided informed consent and were sent a link to an online CM program (The Concept System® Global MAX™) to complete the study. Of the 83 individuals invited to participate in the first task (brainstorming), 72 completed it (response rate = 86.7%).
2.2. Sociodemographic and tobacco measures
Participants answered a demographic questionnaire in the CM program that asked about their ECIG use history, device characteristics, other tobacco use, and demographics. ECIG use history items included an assessment of how long participants had used ECIGs regularly (some days or most days; as per items from the National Adult Tobacco Survey; Centers for Disease Control and Prevention, 2016), number of days of ECIG use in the past 30 days, and frequency of ECIG use throughout the day (at least once per day, every once in a while throughout the day, fairly frequently throughout the day, almost always throughout the day). ECIG liquid nicotine concentration, relative concentrations of propylene glycol and vegetable glycerin (PG/VG ratio), flavors used, liquid storage/delivery system (disposable, cartomizer, clearomizer/tank, drip tip), ECIG device type (cig-alike, vape pen style, box mod, rebuildable/mechanical mod), and electrical characteristics (battery voltage, power in watts, coil resistance in ohms) were assessed. Participants reported cigarettes smoked per day and smoking frequency (every day, some days, or not at all) in the past 30 days and one year ago. Participants then completed demographic questions on age, race/ethnicity, and gender.
2.3. Concept Mapping Procedures
2.3.1. Brainstorming
Participants were directed to provide five to eight statements in response to a prompt related to ways participants used ECIGs to reduce their cigarette smoking: “A SPECIFIC WAY I HAVE USED electronic cigarettes to reduce my cigarette smoking or a SPECIFIC WAY electronic cigarettes help me reduce my cigarette smoking is…”. Each participant completed the brainstorming task individually, however, statements entered by previous participants were visible. Each participant was instructed to review the list of statements and attempt to avoid duplicating content that had been submitted previously (as in Soule et al., 2016a, 2016b, 2016c, 2017; Trochim et al., 2003). The brainstorming task was closed after content saturation was reached, that is, when enrolling additional participants no longer resulted in new/unique statement content. Participants received a $10 e-gift card for completing the brainstorming task.
2.3.2. Sorting
Three researchers reviewed the statements independently to remove redundant statements and statements not addressing the prompt (e.g., “Vape culture is really interesting and pretty cool if you do some research.”) until a final list was achieved. If two or three reviewers identified a statement as redundant with other statements in the list or identified a statement as not relating to the focus prompt, this statement was removed from the list. The final list of 99 statements was then uploaded to the CM program. Participants from the brainstorming task were invited to complete the sorting and rating tasks at the CM website. Thirty-nine completed the sorting task and 41 completed the rating task. In the sorting task (Rosenberg & Kim, 1975; Weller & Romney, 1988), each participant organized statements from the final list into “piles” using rules: 1) piles were required to be made of statements of similar content or idea and not any other criteria (e.g., does not apply to me, important, true and false, etc.), 2) there could not be as many piles as statements or one pile with all statements, and 3) there could not be a miscellaneous pile. Participants received a $25 e-gift card for completing the sorting task.
2.3.3. Rating
After sorting, participants completed the rating task: all statements were presented in a list and participants rated each statement based on a prompt: “This is a way that I have used electronic cigarettes or an aspect of electronic cigarettes that has helped me reduce my cigarette smoking.” with a seven point semantic differential response option scale (as in Soule et al., 2016a, 2016b, 2016c, 2017) with anchors at 1 (Definitely NOT true for me) and 7 (Definitely true for me). Participants received a $10 e-gift card for completing the rating task.
2.3.4. Representation
Each participant’s sorting data were converted into a matrix by the CM program and a “1” was entered to represent the statements that were sorted into the same pile. For example, if statements 5 and 38 were sorted into the same pile by a participant, a “1” would be entered into the cells representing the overlap of statements 5 and 38 in that participant’s matrix. All participant matrices were aggregated to create a 99 × 99 matrix with larger cell counts indicating statements that were sorted together by more participants and smaller cell counts indicating statements that were sorted together by fewer participants. Using nonmetric multidimensional scaling, an algorithm assigned each statement a coordinate (x,y) in two-dimensional space with each statement being represented by a point on a map (“point map”; Kruskal & Wish, 1978). Points on the map that were closer to one another represented statements that were sorted together more often (i.e., by more participants) whereas points on the map that were further apart represented statements that were sorted together less often (i.e., by fewer participants). The stress value (0.29) of the model, which indicates the fit of the multidimensional scaling analysis, fell within the range of stress values reported in previous research (Rosas & Kane, 2012), indicating good fit and congruence between the processed data and the raw data (Davison, 1983; Kruskal, 1964).
2.3.5. Analysis and Interpretation
Clusters of statements related to similar content were identified empirically by using a hierarchical cluster analysis where an algorithm (Ward, 1963) identified non-overlapping cluster arrangements by minimizing distances between statements within clusters. A “cluster map” (Figure 2) was generated with the statement points enclosed by polygon-shaped boundaries identifying clusters of statements. Models were generated by adding a single additional cluster to the previous model wherein one cluster from the previous model would be divided into two new clusters (e.g, going from a two cluster model to a three cluster model would involve one cluster remaining the same and the other cluster being divided into two new clusters). Researchers examined multiple cluster maps to determine the best fitting model by ensuring that each of the clusters related to a single construct (interpretability) while preferring a model that had the fewest clusters (parsimony).
Fig 2.
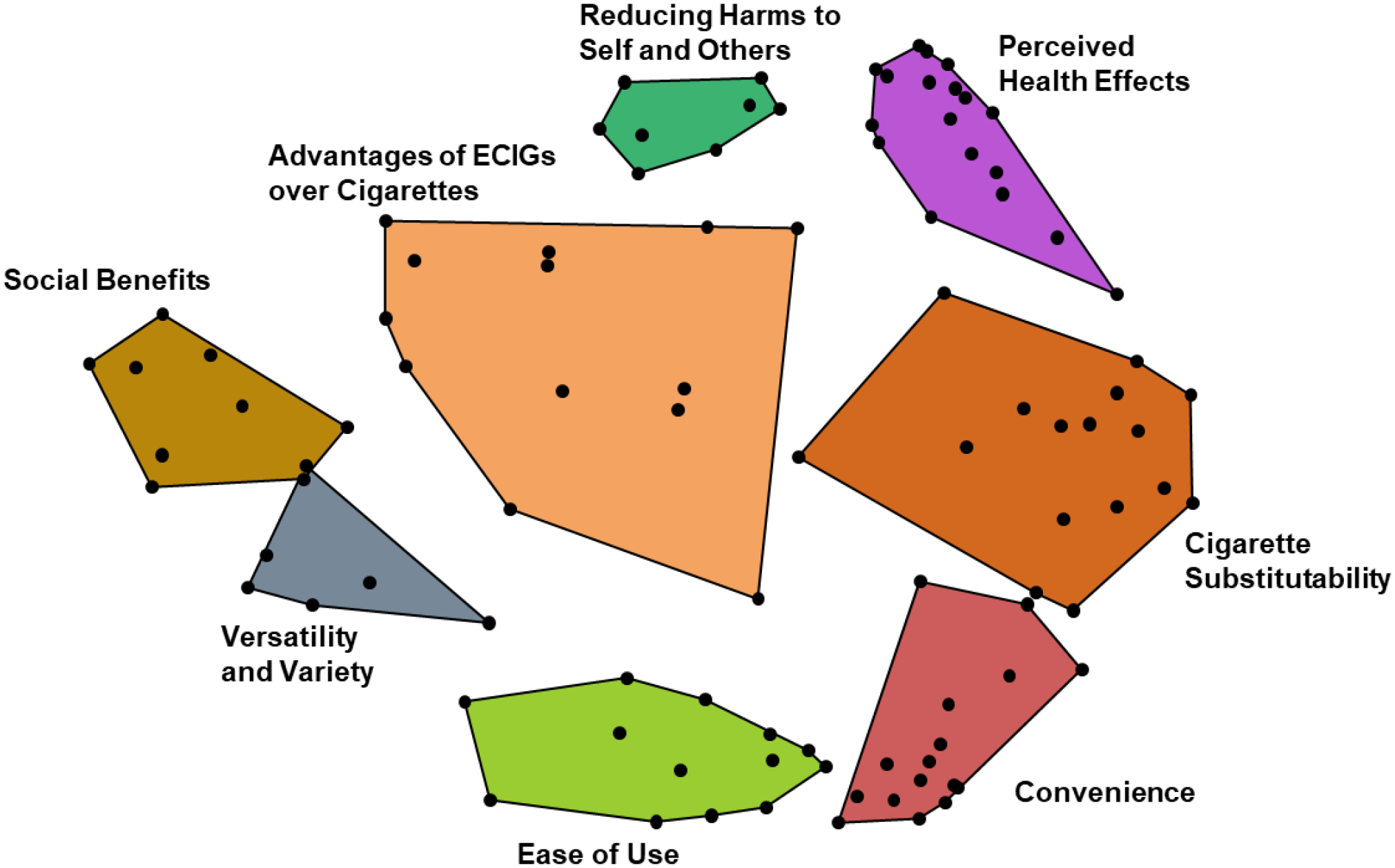
Cluster map. Points on the map represent statements generated in the brainstorming task. Points closer to one another represent statements that were sorted together by more participants in the sorting task and relate to similar content. Points further apart on the map represent statements that were rarely (or not at all) sorted together by participants in the sorting task and relate to different content.
Mean ratings were calculated for all statements and then were used to calculate mean cluster ratings for all of the identified clusters. Mean cluster ratings were compared between sample subgroups (age, gender, device type, cigarette smoking status, daily ECIG use, ECIG throughout the day) using t tests with an alpha level of 0.05 used to determine significance differences between groups.
3. Results
3.1. Participant characteristics
For a complete description of participant characteristics, see Table 1 and Figure 1. The average age of participants was 34.5 (SD=11.4), 55.6% were male, 73% white, and 84.7% were not of Hispanic origin. Most participants (57.0%) reported regular ECIG use for one year or more. ECIG liquid nicotine concentrations varied greatly (0–36 mg/ml) with 3 mg/ml reported most commonly (19.2% of participants). Approximately two-thirds (63.9%) reported using a box mod or mechanical mod ECIG device. Many of participants did not know the PG/VG ratio of their ECIG liquid (38.9%) or their device voltage (51.4%), power (50.0%), or resistance (56.9%). Of those who reported these device characteristics, the most common reported values were 50/50 PG/VG ratio, 3.7 volts (range=2.2–75.0), 5.5 watts (range=3.3–80.1), and 1.5 ohms (range=0.1–53.0) with some extreme values in ranges suggesting some participants who provided responses did not know these characteristics of their ECIGs. Twelve months prior to the study, participants reported smoking a mean of 10.4 cigarettes/day (SD=11.4), including 19 who reported 0 cigarettes/day (i.e., former smokers who had already quit 12 months ago). At the time of the study, participants reported smoking a mean of 5.6 cigarettes/day (SD=6.6). More than two thirds (68.1%) reported currently smoking cigarettes either every day or most days. ECIG use frequency was not associated with cigarette smoking frequency [χ2(6)=3.835, p=0.70] with each ECIG use frequency group having nearly even distribution across the cigarette smoking frequency groups.
Table 1.
Sample demographics and ECIG/tobacco use characteristics (n=72).
| Characteristic | N | % |
|---|---|---|
| Age (M, SD) | 34.5(11.4) | |
| Sex | ||
| Female | 30 | 41.7 |
| Male | 40 | 55.6 |
| Transgender | 2 | 2.8 |
| Ethnicity | ||
| Hispanic/Latino | 11 | 15.3 |
| Not Hispanic / Latino | 61 | 84.7 |
| Race | ||
| American Indian / Alaskan Native | 2 | 2.8 |
| Asian | 2 | 2.8 |
| Black / African American | 9 | 12.5 |
| White / European American | 53 | 73.6 |
| More than one race | 6 | 8.3 |
| Regular ECIG Use Duration | ||
| 1 – 3 months | 6 | 8.3 |
| 4 – 6 months | 7 | 9.7 |
| 7 – 12 months | 18 | 25.0 |
| Between 1 and 2 years | 19 | 26.4 |
| More than 2 years | 22 | 30.6 |
| ECIG Use in Past 30 Days | ||
| 6 – 10 days | 5 | 6.9 |
| 11 – 20 days | 7 | 9.7 |
| 21 – 29 days | 13 | 18.1 |
| All 30 days | 32 | 44.4 |
| ECIG Use Times per Day | ||
| At least once per day | 5 | 6.9 |
| Every once in a while throughout the day | 20 | 27.8 |
| Fairly frequently throughout the day | 33 | 45.8 |
| Almost always throughout most of the day | 14 | 19.4 |
| Nicotine Concentration | ||
| Zero (0mg / mL) | 4 | 5.6 |
| 3 – 4 mg / mL | 16 | 22.2 |
| 6 – 8 mg / mL | 17 | 23.6 |
| 11 – 19 mg / mL | 17 | 23.6 |
| 20 mg / mL or greater | 15 | 20.8 |
| Don’t know | 3 | 4.2 |
| Type of Liquid Storage | ||
| Prefilled disposable / Cig-alike | 20 | 27.8 |
| Refillable cartomizer | 7 | 9.7 |
| Refillable tank or clearomizer | 32 | 44.4 |
| Drip feed / Use drip tip | 10 | 13.9 |
| Don’t know / Other | 3 | 1.4 |
| Device Type | ||
| Cig-alike | 18 | 25.0 |
| Vape pen / eGo style product | 24 | 33.3 |
| Box mod | 22 | 30.6 |
| Rebuildable / Mechanical mod | 8 | 11.1 |
| ECIG Liquid Flavor Preference | ||
| Candy / Fruit flavor | 22 | 30.6 |
| Food / Dessert / Spices flavor (e.g., crème, vanilla, cinnamon) | 7 | 9.7 |
| Menthol flavor | 9 | 12.5 |
| Tobacco flavor | 16 | 22.2 |
| I usually use multiple flavors | 15 | 20.8 |
| I don’t use a flavor | 2 | 2.8 |
| Current cigarette smoking frequency | ||
| Every day | 23 | 31.9 |
| Some days | 26 | 36.1 |
| Not at all | 23 | 31.9 |
| Cigarettes per day (M, SD) | ||
| 12 months ago | 10.7 (11.8) | |
| Past 30 days | 5.5 (6.5) |
Note. Regular use was defined as using an ECIG some days or most days.
Fig 1.
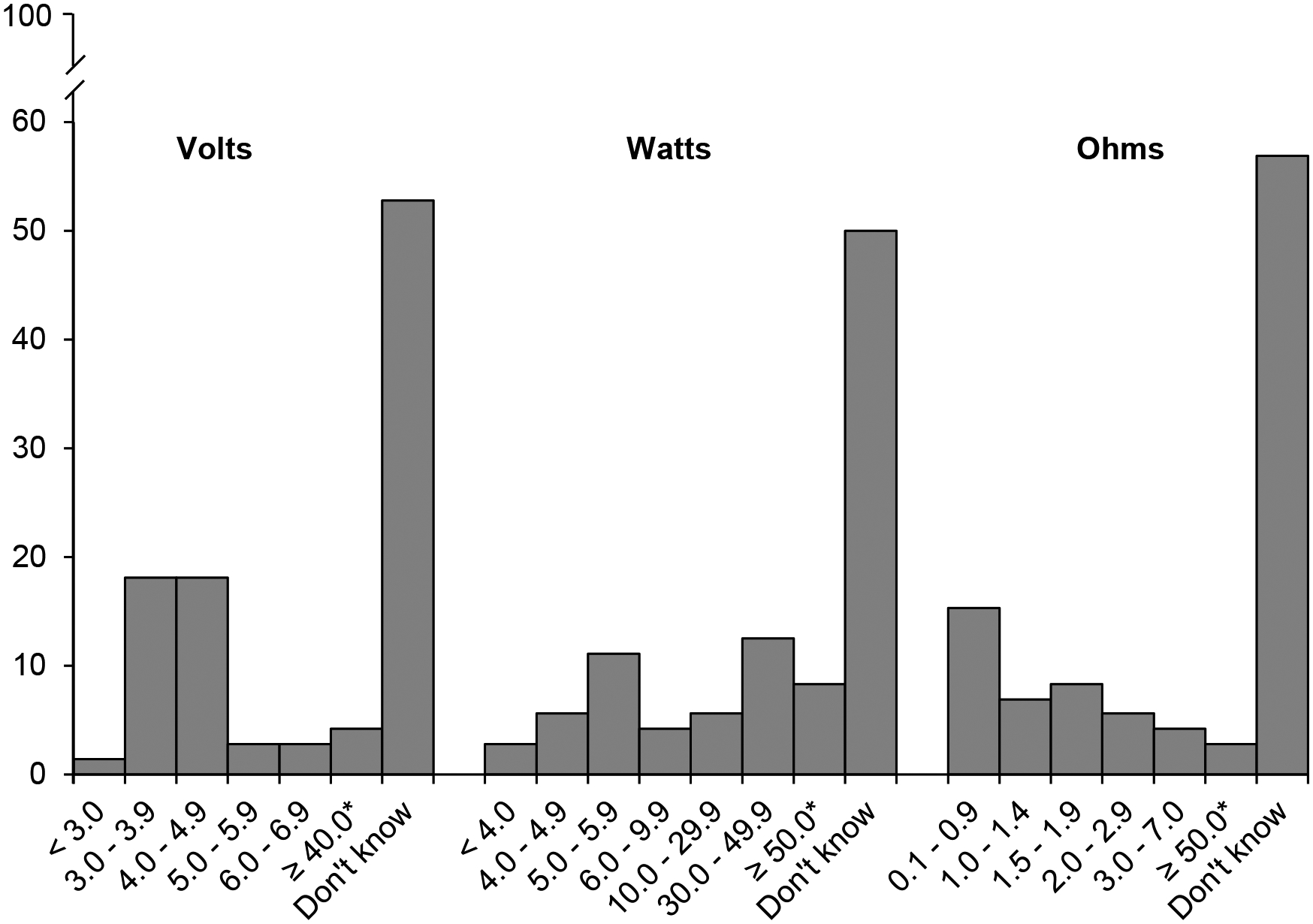
ECIG device characteristic percentages based on participant self-report. Note that some values reported by participants noted with an asterisk (*) are likely inaccurate.
3.2. Concept Mapping Results
An eight cluster model (Figure 2) was established and included the following clusters: Convenience, Perceived Health Effects, Fewer Limitations of Use, Versatility and Variety, Advantages of ECIGs over Cigarettes, Cigarette Substitutability, Reducing Harms to Self and Others, and Social Benefits. Clusters ranged in size from 6 statements to 18 statements. Mean cluster ratings ranged from the highest cluster, Convenience (M=5.44, SD=0.60), to the lowest cluster, Social Benefits (M=4.72, SD=0.65). Many of the statements included in the clusters were similar to other reasons for using ECIGs reported in the literature previously are not the focus of the current analysis and therefore are not described in the text further. See Table 2 for a full list of statements. Subgroup cluster rating comparisons and descriptions of specific ECIG use behavioral strategies for reducing cigarette smoking identified by participants are described in next section.
Table 2.
List of clusters and statements with mean statement ratings.
| Cluster | Statement | Average Rating |
|---|---|---|
| Convenience | 5.4 | |
| I do not have to constantly leave what I am doing to go and smoke a cigarette. | 6.2 | |
| I can take a drag or two off of my electronic cigarette instead of going out to smoke a whole cigarette. | 6.2 | |
| I can vape inside or outside whenever I have a craving. | 6.1 | |
| I keep my electronic cigarette with me at all times. | 6.0 | |
| When I crave a cigarette/nicotine I can easily grab my electronic cigarette instead of a cigarette. | 5.8 | |
| I do not have to make trips to the store, all I need is e-liquid and a charged battery. | 5.8 | |
| Electronic cigarettes are easier for me to store and carry. | 5.6 | |
| Keeping an electronic cigarette in my bag, in my car, and my house so it’s always available to me. | 5.6 | |
| It’s a lot easier to carry and I don’t have to carry a whole pack of cigarettes. | 5.5 | |
| Electronic cigarettes are easier to manage. Instead of having a cigarette and lighter, I have an “all-in-one.” | 5.4 | |
| Not having to worry about keeping the cigarette lit and having a lighter. | 5.4 | |
| I don’t have to buy ashtrays or lighters. | 5.3 | |
| Electronic cigarettes are easier to use than cigarettes. | 4.9 | |
| Vaping alters my usual, everyday smoking schedule. | 4.8 | |
| I got rid of all my cigarettes and lighters when I started vaping. | 4.6 | |
| I use electronic cigarettes when I run out of regular cigarettes. | 4.0 | |
| Perceived Health Effects | 5.4 | |
| Vaping has made me feel like I am making a better choice for my health. | 6.1 | |
| Vaping has made me feel healthier. | 6.0 | |
| I can vape more times per day with less negative effects. | 5.9 | |
| Vaping is easier on the throat and lungs. | 5.8 | |
| Even with nicotine, vaping doesn’t feel as addictive as smoking cigarettes. | 5.7 | |
| Vaping made it easier to gradually reduce my nicotine intake by reducing the nicotine strength in my e-liquid. | 5.7 | |
| Electronic cigarettes are healthier than regular cigarettes. | 5.7 | |
| I can use my electronic cigarette on an empty stomach and I don’t become light headed. | 5.6 | |
| I don’t cough uncontrollably anymore since I started using an electronic cigarette. | 5.5 | |
| Vaping has improved my lung capacity. | 5.4 | |
| I can use the electronic cigarette in the car without the second hand smoke harming my passengers. | 5.4 | |
| Vaping makes me feel better and makes me want to be active. | 5.2 | |
| I can vape even when I have a cold. | 5.1 | |
| It’s safer to use around people other people with asthma. | 5.0 | |
| I feel it vaping will not cause lung cancer. | 4.9 | |
| I couldn’t exercise or engage in physical activity when I smoked cigarettes, now I can with the help of electronic cigarettes. | 4.7 | |
| I seem to get sick less when I switched to vaping, and I recover faster when I do get sick. | 4.7 | |
| Electronic cigarettes are harmless to the body. | 4.3 | |
| Ease of use | 5.4 | |
| I can quickly vape whenever and wherever I need to. | 6.3 | |
| I vape when I am at home. | 6.1 | |
| I use them in places where I cannot smoke a cigarette. | 6.1 | |
| The electronic cigarettes/e-liquid lasts longer than cigarettes do. | 6.0 | |
| I don’t have to get up frequently to go outside and smoke a cigarette. | 5.9 | |
| Vaping is less expensive then smoking cigarettes. | 5.8 | |
| I can vape when I’m in a friend’s car who doesn’t smoke. | 5.6 | |
| I can vape discreetly. | 5.4 | |
| You can smoke in most public places. | 5.4 | |
| I don’t have to have the car window rolled down. | 5.3 | |
| I sometimes take a puff at work when no one is looking. | 4.4 | |
| I am allowed to vape in my office so I don’t have to go outside and walk away from my work. | 4.3 | |
| I can make my own e-liquid. | 3.1 | |
| Versatility and Variety | 5.3 | |
| Vaping gives you different options for nicotine strength. | 6.0 | |
| Electronic cigarettes have a variety of tobacco flavors. | 5.9 | |
| The flexibility of being able to choose nicotine concentration, some days you want more some days you may not need any. | 5.6 | |
| I started with a higher nicotine e-liquid to compensate for how much nicotine I was using when I smoked cigarettes. | 5.0 | |
| Having a variety of flavors makes me smoke less. | 4.9 | |
| I can sit at coffee shops/restaurants and use my electronic cigarette without persecution from others. | 4.6 | |
| Advantages of ECIGs over Cigarettes | 5.3 | |
| Vaping doesn’t smell as bad as regular cigarettes. | 6.2 | |
| Vaping tastes better than smoking cigarettes. | 6.0 | |
| Vaping doesn’t give me bad breath. | 5.9 | |
| I can change the amount I inhale at a time. | 5.6 | |
| The absence of smell on my clothes and hands reduces incidental cravings. | 5.6 | |
| Vaping keeps me occupied. | 5.5 | |
| I don’t feel the guilt when I vape. | 5.5 | |
| The flavors can help to satisfy a hunger craving and that kills the urge to smoke cigarettes. | 5.4 | |
| Vaping makes me feel more satisfied than smoking cigarettes. | 5.1 | |
| Watching the massive amount of vapor that looks like smoke satisfies me mentally and physically. | 4.9 | |
| Vaping feels easier on my lips. | 4.9 | |
| It really helped when I first started vaping that the e-liquid tasted like my cigarettes. | 4.5 | |
| Getting my partner on board to also try vaping and quitting smoking so I have a support system. | 4.1 | |
| Cigarette Substitutability | 5.2 | |
| Electronic cigarettes fulfill the hand to mouth action that mimics cigarette smoking. | 6.2 | |
| Vaping provides a substitute for the familiar smoking rituals. | 6.1 | |
| Fulfilled my nicotine urges and need to cradle an object in my hand. | 6.0 | |
| Whenever I crave a cigarette I puff on my electronic cigarette. | 6.0 | |
| I get the sensation of smoking without actually picking up a regular cigarette. | 5.7 | |
| I use it throughout the day so I don’t feel the withdrawal of going without a regular cigarette. | 5.6 | |
| After using my electronic cigarette I can still feel a nicotine buzz. | 5.4 | |
| Vaping gives me something to do with my hands. | 5.3 | |
| I use my electronic cigarette when I am stressed - when I see the exhaled vapor I feel like the stress leaves with it. | 5.3 | |
| Helps calm my nerves when driving to work or home since I can’t smoke in the car. | 5.2 | |
| I use electronic cigarette for late night/early morning cravings. | 5.1 | |
| I have imagined my electronic cigarette is a “real” cigarette, and it satisfies my urge to actually smoke a real cigarette. | 4.9 | |
| I am satisfied quicker with vaping compared to smoking cigarettes. | 4.8 | |
| The width and length of my electronic cigarette is similar to a real cigarette which helps me reduce my smoking. | 4.6 | |
| I use electronic cigarettes to fill in time between morning afternoon evening cigarettes. | 3.8 | |
| I switched totally to electronic cigarettes the first day I started using electronic cigarettes. | 3.5 | |
| Reducing Harms to Self and Others | 5.0 | |
| It helps to not yellow my teeth. | 5.6 | |
| I can taste my food better and enjoy it. | 5.5 | |
| Don’t feel as bad about secondhand smoke. | 5.5 | |
| I feel better vaping around my family/children and others because it doesn’t harm them. | 5.2 | |
| Vaping is safer for my animals to be around. | 5.0 | |
| Using electronic cigarettes around others who do not smoke helps me to smoke less. | 4.8 | |
| I feel like I can control the level of toxicity I ingest by only using organic e-liquid. | 4.2 | |
| I smoke half a pack of cigarettes instead of a full pack when using an electronic cigarette. | 4.0 | |
| Social Benefits | 4.7 | |
| Electronic cigarettes are more modern. | 5.5 | |
| I vape whenever I feel like it and people don’t mind it. | 5.5 | |
| Others are less irritated with me vaping than smoking. | 5.3 | |
| It is more socially acceptable than cigarette smoking. | 5.3 | |
| Vaping is easy on the eyes which has social value. | 4.6 | |
| Vaping looks cooler than smoking cigarettes. | 4.4 | |
| I buy higher wattage mods to get that smoke feeling. | 4.2 | |
| I use vaping as a social habit to connect with friends who also enjoy vaping. | 4.1 | |
| I experiment with a higher vegetable glycerin (VG) level and producing more smoke and attempting tricks as a hobby. | 3.7 | |
3.3. Cluster Rating Comparisons
Participants between the ages of 18 and 30 rated the Social Benefits cluster higher (M=5.17, SD=0.33) compared to those over the age of 30 (M=4.46, SD=0.87; p<0.05). There were no gender differences in cluster ratings. However, non-white participants rated the Social Benefits cluster higher (M = 5.48, SD = 0.63) than white participants (M=4.51, SD=0.79; p<0.02). Regarding device type, the Perceived Health Effects cluster was rated lower (M=4.93, SD=0.60) by 1st generation (e.g., cig-alike products) ECIG users compared to 2nd and 3rd generation (e.g., vape pens, box mods, mechanical mods) ECIG users (M=5.52, SD=0.48; p<0.005). Participants who did not report smoking cigarettes currently rated the Perceived Health Effects cluster higher (M=5.97, SD=0.51) compared to those who reported smoking cigarettes every day or most days (M=5.01, SD=0.51; p<0.001). Those who reported using ECIGs 25+ days out of the past 30 (daily or nearly daily users) rated the Convenience (M=5.59, SD=0.70), Advantages of ECIGs over Cigarettes (M=5.51, SD=0.67) and the Perceived Health Effects cluster (M=5.60, SD=0.52) higher than those who reported ECIG use on 1–29 days in the past 30 days (ps<0.02). Finally, participants who reported using their ECIG “almost always throughout most of the day” or “fairly frequently throughout the day” rated all the clusters higher than participants who reported using ECIGs either “at least once per day” or “every once in a while throughout the day” (ps<0.05), except for the Social Benefits cluster. However, there was no association between ECIG use frequency and cigarette use frequency.
3.4. Smoking Reduction Behavioral Strategy Statements
Many of the statements identified participants related to attributes about ECIGs that they perceived as supporting efforts to reduce cigarette smoking. For example, participants described that ECIGs allowed users greater freedom and versatility with regard to locations one can “smoke”, ECIGs are more socially acceptable, ECIGs do not cause users to smell bad (i.e., like cigarette smoke), and ECIG liquids come in many options with regard to flavor, nicotine concentration, and PG/VG ratio. However, some statements described specific ECIG use behavioral strategies that were perceived to aid in cigarette smoking reduction.
Several statements related to abrupt transitions from cigarettes to ECIGs: “I got rid of all of my cigarettes and lighters when I started vaping” and “I switched totally to electronic cigarettes the first day I started using electronic cigarettes.” These statements were less specific about how a smoker might use an ECIG to reduce or quit cigarette smoking, but rather indicated stopping smoking completely and switching to ECIGs was perceived by some as being more effective than reducing cigarette smoking and transitioning to ECIGs slowly. Former smokers rated these statements higher (Ms = 6.27 and 4.53) than current smokers (M=2.58 and 2.85) Other statements related to participants’ ECIG use behaviors: “I keep my electronic cigarette with me at all times,” “Keeping an electronic cigarette in my bag, in my car, and my house so it’s always available to me,” “I sometime take a puff when no one is looking,” “Whenever I crave a cigarette I puff on my electronic cigarette,” and “I use it throughout the day so I don’t feel the withdrawal of going without a regular cigarette.” These behavioral strategy statements seemed to relate to keeping an ECIG close at hand and using it frequently in order to prevent cigarette/nicotine cravings from getting too strong.
Other behavioral strategy statements related to choosing specific device and liquid characteristics. Several statements indicated different liquid characteristics were perceived to be helpful during the initial transition from cigarettes to ECIGs: “I started with a higher nicotine e-liquid to compensate for how much nicotine I was using when I smoked cigarettes” and “It really helped that when I first started vaping that the e-liquid tasted like my cigarettes.” Other statements related to ECIG liquid included “I experiment with a higher vegetable glycerin level and producing more smoke and attempting tricks as a hobby” and “I can make my own liquid.” Other statements identified behaviors related to choosing the appropriate ECIG device: “The width and length of my electronic cigarette is similar to a real cigarette which helps me reduce my smoking” and “I buy higher wattage mods to get that smoke feeling.”
4. Discussion
This study was the first to identify ECIG use behaviors and product characteristics that ECIG users perceive to be associated with cigarette smoking cessation or reduction. ECIG users perceived that ECIGs are more convenient to use, have more variety and versatility, have fewer limitations for use, and have social, health, and other benefits compared to cigarette smoking while still providing desired physical and psychological effects in substitution for cigarettes. Though there were few differences between sample subgroups regarding cluster ratings, ECIG use frequency was associated with mean cluster ratings, but not cigarette smoking frequency. The behaviors and device characteristics identified by participants included a broad range of concepts that indicated ECIG use is not a behavior that can be understood fully by measuring ECIG use status (i.e., “Do you use an electronic cigarette?”). Rather, because ECIG behaviors and device characteristics may differ among subgroups of the ECIG use population, considering the heterogeneity of ECIG use behaviors and device characteristics may help researchers understand why some cigarette smokers who use ECIGs continue to smoke cigarettes while others reduce or quit smoking completely. The results of this study highlight some of this heterogeneity.
The eight-cluster solution replicated clusters from other studies with different focus prompts (Soule et al., 2016a, 2016b, 2017) and some of these cluster ratings were associated with smoking status. In the current study the Perceived Health Effects cluster was the only cluster that ECIG users who were former smokers rated higher than dual users of ECIGs and cigarettes. Perhaps ECIG users who have quit smoking completely experience fewer smoking-related adverse effects whereas those who continue to dual use ECIGs and combustible cigarettes experience more smoking-related adverse effects. Additionally, higher ratings of the Perceived Health Effects cluster may also be an indication that some smokers switch to ECIGs because they believe ECIG use is associated with promoting positive health effects, cigarette smokers perceive experiencing positive health outcomes after switching to ECIGs, or a combination of these and other possible explanations. Former smokers also rated behavioral strategy statements related to rapid transitions from smoking to ECIGs higher than dual users of ECIGs and cigarettes indicating that some behavioral strategies may be more associated with complete switching from cigarettes to ECIGs. However, though others (Biener & Hargraves, 2015; Sharapova et al., 2017) have reported that more frequent/daily ECIG use is associated with greater likelihood of self-reported smoking cessation compared to non-ECIG use, this association was not seen in the current study. Taken together, the findings from the current study indicate that some associations between ECIG use frequency, cigarette smoking status, and ECIG use perceptions may mismatch such that some ECIG perceptions may be associated with ECIG use frequency or cigarette smoking status, but not both. Future studies are needed to test these associations and hypotheses.
Long term smokers of 1 to 10 cigarettes or even less than 1 cigarette per day are at significantly higher mortality risk than non-smokers and those who quit smoking completely (Inoue-Choi et al., 2017). For ECIG use to have the greatest potential positive impact on public health, cigarette smokers would need to switch completely to ECIGs. Our results reveal constructs and specific behaviors that may be associated with smoking reduction or complete switching to ECIGs, though the vast majority of participants continued smoking tobacco cigarettes. Additionally, ECIG nicotine yield (in the aerosol) is and delivery (to the user) is related directly to power (in watts, a function of battery voltage and coil resistance) and liquid nicotine concentration (Talih et al., 2015; Wagener et al., 2017; Hiler et al., in press). The majority of participants in the current study did not know these characteristics of their ECIG devices. To understand if certain device characteristics are associated with smoking cessation or reduction, greater user and researcher knowledge of these characteristics is needed. Then, future studies will be better able to examine which behaviors, perceptions, and device characteristics affect tobacco use behaviors.
This study had several limitations. The tobacco use measures were self-reported. The small sample may limit generalizability, although it was diverse and drawn from multiple states across the U.S. Cigarette smokers who desire to reduce their cigarette smoking may also seek to quit smoking completely, but some may want to reduce but not quit cigarette smoking. We speculate that the majority who seek to reduce their cigarette smoking are cessation seekers. Therefore, the perceptions identified in this study likely cut across cigarette reducers and cessation seekers, however, successful cigarette reduction using ECIGs may be related to level of cigarette dependence and should be examined further. Different ECIG users may have provided different statements, however, similar clusters have emerged across studies indicating reliability of the method and results.
5. Conclusions
Many ECIG users report using ECIGs for cigarette smoking reduction or cessation, however, many continue to use cigarettes or other tobacco products. A recent study identified that 83.6% of current adult ECIG users are also current users of cigarettes or other tobacco products while 14.5% of current adult ECIG users are former users of cigarettes or other tobacco products (Sharapova et al., 2017). While daily ECIG use was more common among former cigarette smokers and other tobacco users, many current cigarette smokers and other tobacco users also reported daily ECIG use. These data indicate that there are likely other factors affecting the association between ECIG use and cigarette smoking status. Taken together with the findings from the current study, ECIG use behaviors and device characteristics are heterogeneous and may help explain why some cigarette smokers who use ECIGs continue to smoke cigarettes while others do not. This study was the first to examine specific ECIG use characteristics and behaviors perceived to be associated with cigarette smoking cessation or reduction. We identified an eight-cluster model of factors that ECIG users perceived to be associated with cigarette smoking reduction, though approximately two-thirds of the sample reported dual use of ECIGs and cigarettes. These data can inform measures in larger national studies such as Population Assessment of Tobacco and Health (PATH; Hyland et al., 2017) and may be useful in building theories to predict ECIG initiation among cigarette smokers. Future studies should aim to confirm the reliability and validity of the findings to help inform FDA regulations related to device characteristics that may promote combustible cigarette abstinence.
References
- Adkison SE, O’Connor RJ, Bansal-Travers M, Hyland A, Borland R, Yong HH, Cummings KM, McNeill A, Thrasher JF, Hammond D, Fong GT, 2013. Electronic nicotine delivery systems: international tobacco control four-country survey. Am. J. Prev. Med 44, 207–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Adriaens K, Van Gucht D, Declerck P, Baeyens F, 2014. Effectiveness of the electronic cigarette: an eight-week Flemish study with six-month follow-up on smoking reduction, craving and experienced benefits and complaints. Int J Environ Res Public Health 11(11), 11220–11248. doi: 10.3390/ijerph111111220. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Al-Delaimy WK, Myers MG, Leas EC, Strong DR, Hofstetter CR, 2015. E-cigarette use in the past and quitting behavior in the future: a population-based study. Am J Public Health 105(6): 1213–1219. doi: 10.2105/AJPH.2014.302482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berg CJ, Haardoerfer R, Escoffery C, Zheng P, Kegler M, 2015. Cigarette users’ interest in using or switching to electronic nicotine delivery systems for smokeless tobacco for harm reduction, cessation, or novelty: a cross-sectional survey of US adults. Nicotine Tob. Res 17, 245–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biener L, Hargraves JL, 2015. A longitudinal study of electronic cigarette use among a population-based sample of adult smokers: association with smoking cessation and motivations to quit. Nicotine Tob Res 17(2), 127–133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown J, West R, Beard E, Michie S, Shahab L, McNeill A, 2014. Prevalence and characteristics of e-cigarette users in Great Britain: findings from a general population survey of smokers. Addict. Behav 39, 1120–1125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bullen C, Howe C, Laugesen M, McRobbie H, Parag V, Williman J, Walker N, 2013. Electronic cigarettes for smoking cessation: a randomised controlled trial. Lancet 382(9905), 1629–1637. doi: 10.1016/S0140-6736(13)61842-5. [DOI] [PubMed] [Google Scholar]
- Caponnetto P, Campagna D, Cibella F, Morjaria JB, Caruso M, Russo C, Polosa R, 2013. EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as tobacco cigarettes substitute: a prospective 12-month randomized control design study. PLoS One 8(6), e66317. doi: 10.1371/journal.pone.0066317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention, 2016. National Adult Tobacco Survey (NATS) Accessed from https://www.cdc.gov/tobacco/data_statistics/surveys/nats/index.htm on July 7, 2017.
- Davison ML (1983). Multidimensional scaling New York, NY: John Wiley and Sons. [Google Scholar]
- Glasser AM, Collins L, Pearson JL, Abudayyeh H, Niaura RS, Abrams DB, Villanti AC, 2017. Overview of electronic nicotine delivery systems: a systematic review. Am J Prev Med 52(2), e33–e-66. doi: 10.1016/j.amepre.2016.10.036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goniewicz ML, Lingas EO, Hajek P, 2013. Patterns of electronic cigarette use and user beliefs about their safety and benefits: an internet survey. Drug Alcohol Rev 32, 133–140. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grana RA, Popova L, Ling PM, 2014. A longitudinal analysis of electronic cigarette use and smoking cessation. JAMA Intern Med 174(5), 812–813. doi: 10.1001/jamainternmed.2014.187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hiler M, Breland A, Spindle T, Maloney S, Lipato T, Karaoghlanian N, Shihadeh A, Lopez A, Ramôa C, Eissenberg T (in press). Electronic cigarette user plasma nicotine concentration, puff topography, heart rate, and subjective effects: influence of liquid nicotine concentration and user experience. Exp Clin Psychopharmacol [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hummel K, Hoving C, Nagelhout GE, de Vries H, van den Putte B, Candel MJ, Borland R, Willemsen MC, 2015. Prevalence and reasons for use of electronic cigarettes among smokers: findings from the International Tobacco Control (ITC) Netherlands Survey. Int. J. Drug Policy 26, 601–608. [DOI] [PubMed] [Google Scholar]
- Hyland A, Ambrose BK, Conway KP, Borek N, Lambert E, Carusi C, Taylor K, Crosse S, Fong GT, Cummings KM, Abrams D, Pierce JP, Sargent J, Messer K, Bansal-Travers M, Niaura R, Vallone D, Hammond D, Hilmi N, Kwan J, Piesse A, Kalton G, Lohr S, Pharris-Ciurej N, Castleman V, Green VR, Tessman G, Kaufman A, Lawrence C, van Bemmel DM, Kimmel HL, Blount B, Yang L, O’Brien B, Tworek C, Alberding D, Hull LC, Cheng YC, Maklan D, Backinger CL, Compton WM, 2017. Design and methods of the Population Assessment of Tobacco and Health (PATH) Study. Tob Control, 26(4), 371–378. doi: 10.1136/tobaccocontrol-2016-052934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kadimpati S, Nolan M, Warner DO, 2015. Attitudes, beliefs, and practices regarding electronic nicotine delivery systems in patients scheduled for elective surgery. Mayo Clin. Proc 90, 71–76. [DOI] [PubMed] [Google Scholar]
- Kalkhoran S, Glantz SA, 2016. E-cigarettes and smoking cessation in real-world and clinical settings: a systematic review and meta-analysis. Lancet Respir Med 4(2),116–128. doi: 10.1016/S2213-2600(15)00521-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kralikova E, Novak J, West O, Kmetova A, Hajek P, 2013. Do e-cigarettes have the potential to compete with conventional cigarettes?: a survey of conventional cigarette smokers’ experiences with e-cigarettes. Chest 144, 1609–1614. [DOI] [PubMed] [Google Scholar]
- Kruskal JB, 1964. Multimensional scaling by optimizing goodness of fit to nonmetric hypothesis. Psychometrika, 29(1), 1–27. [Google Scholar]
- Kruskal JB, Wish M, 1978. Multidimensional scaling Beverly Hills, CA: Sage Publications. [Google Scholar]
- Mark KS, Farquhar B, Chisolm MS, Coleman-Cowger VH, Terplan M, 2015. Knowledge, attitudes, and practice of electronic cigarette use among pregnant women. J. Addict. Med 9, 266–272. [DOI] [PubMed] [Google Scholar]
- McMillen RC, Gottlieb MA, Shaefer RM, Winickoff JP, Klein JD, 2015. Trends in electronic cigarette use among U.S. adults: use is increasing in both smokers and nonsmokers. Nicotine Tob Res 17(10): 1195–1202. doi: 10.1093/ntr/ntu213. [DOI] [PubMed] [Google Scholar]
- McRobbie H, Bullen C, Hartmann-Boyce J, Hajek P, 2014. Electronic cigarettes for smoking cessation and reduction. Cochrane Database Syst Rev (12):CD010216. doi: 10.1002/14651858.CD010216.pub2. [DOI] [PubMed] [Google Scholar]
- Pearson JL, Stanton CA, Cha S, Niaura RS, Luta G, Graham AL, 2015. E-cigarettes and smoking cessation: insights and cautions from a secondary analysis of data from a study of online treatment-seeking smokers. Nicotine Tob Res 17(10), 1219–1227. doi: 10.1093/ntr/ntu269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pepper JK, Ribisl KM, Emery SL, Brewer NT, 2014. Reasons for starting and stopping electronic cigarette use. Int. J. Environ. Res. Public Health 11, 10345–10361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Peters EN, Harrell PT, Hendricks PS, O’Grady KE, Pickworth WB, Vocci FJ, 2015. Electronic cigarettes in adults in outpatient substance use treatment: Awareness, perceptions, use, and reasons for use. Am. J. Addict 24, 233–239. [DOI] [PubMed] [Google Scholar]
- Richardson A, Pearson J, Xiao H, Stalgaitis C, Vallone D, 2014. Prevalence, harm perceptions, and reasons for using noncombustible tobacco products among current and former smokers. Am J Public Health 104, 1437–1444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosas SR, Kane M, 2012. Quality and rigor of the concept mapping methodology: a pooled study analysis. Evaluation and Program Planning, 35, 236–245. doi: 10.1016/j.evalprogplan.2011.10.003. [DOI] [PubMed] [Google Scholar]
- Rosenberg S, Kim MP, 1975. The method of sorting as a data gathering procedure in multivariate research. Multivar. Behav. Res 10, 489–502. [DOI] [PubMed] [Google Scholar]
- Sharapova SR, Singh T, Agaku IT, Kennedy SM, King BA, 2017. Patterns of e-cigarette use frequency-National Adult Tobacco Survey, 2012–2014. Am J Prev Med S0749–3797(17), 30534–2. doi: 10.1016/j.amepre.2017.09.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Lopez AA, Guy MC, Cobb CO, 2016a. Reasons for using flavored liquids among electronic cigarette users: a concept mapping study. Drug Alcohol Depend 166, 168–176. doi: 10.1016/j.drugalcdep.2016.07.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Maloney SF, Guy MC, Eissenberg T, Fagan P, 2017. User identified positive outcome expectanices of electronic cigarette use: a concept mapping study. Psychol Addict Behav 31(3), 343–353. doi: 10.1037/adb0000263. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Nasim A, Rosas SR, 2016b. Adverse effects of electronic cigarette use. Nicotine Tob. Res 18, 678–685. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Soule EK, Rosas SR, Nasim A, 2016c. Reasons for electronic cigarette use beyond smoking cessation: a concept mapping approach. Addict. Behav 56, 41–50. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stein MD, Caviness CM, Grimone K, Audet D, Borges A, Anderson BJ, 2015. E-cigarette knowledge, attitudes, and use in opioid dependent smokers. J. Subst. Abuse Treat 52, 73–77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Talih S, Balhas Z, Eissenberg T, Salman R, Karaoghlanian N, El Hellani A, Baalbaki R, Saliba N, Shihadeh A, 2015. Effects of user puff topography, device voltage, and liquid nicotine concentration on electronic cigarette nicotine yield: measurements and model predictions. Nicotine Tob Res 17(2), 150–157. doi: 10.1093/ntr/ntu174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Trochim WM, Stillman FA, Clark PI, Schmitt CL, 2003. Development of a model of the tobacco industry’s interference with tobacco control programmes. Tob Control 12(2), 140–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tseng TY, Ostroff JS, Campo A, Gerard M, Kirchner T, Rotrosen J, Shelley D, 2016. A randomized trial comparing the effect of nicotine versus placebo electronic cigarettes on smoking reduction among young adult smokers. Nicotine Tob Res 18(10), 1937–1943. doi: 10.1093/ntr/ntw017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. E-cigarette use among youth and young adults: a report of the Surgeon General 2016. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. [Google Scholar]
- Vickerman KA, Carpenter KM, Altman T, Nash CM, Zbikowski SM, 2013. Use of electronic cigarettes among state tobacco cessation quitline callers. Nicotine Tob Res 15(10), 1787–1791. doi: 10.1093/ntr/ntt061. [DOI] [PubMed] [Google Scholar]
- Vickerman KA, Schauer GL, Malarcher AM, Zhang L, Mowery P, Nash CM, 2017. Reasons for electronic nicotine delivery system use and smoking abstinence at 6 months: a descriptive study of callers to employer and health plan-sponsored quitlines. Tob Control doi: 10.1136/tobaccocontrol-2015-052734. [DOI] [PubMed] [Google Scholar]
- Wagener TL, Floyd EL, Stepanov I, Driskill LM, Frank SG, Meier E, Leavens EL, Tackett AP, Molina N, Queimado L, 2017. Tob Control 26(e1), e23–e28. doi: 10.1136/tobaccocontrol-2016-053041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ward JH, 1963. Hierarchical grouping to optimize an objective function. J. Am. Statist. Assoc 58, 236–244. [Google Scholar]
- Weller SC, Romney AK, 1988. Systematic data collection Newbury Park, CA: Sage. [Google Scholar]
- Zhu S-H, Zhuang Y-L, Wong S, Cummins SE, Tedeschi GJ, 2017. E-cigarette use and associated changes in population smoking cessation: evidence from US current population surveys. BMJ j3262. doi: 10.1136/bmj.j3262. [DOI] [PMC free article] [PubMed] [Google Scholar]