

Abstract
Introduction and importance
Textilloma or Gossypiboma refers as surgical sponges left behind in the surgical field during surgery. Although rare, occur commonly in practice and such cases are rarely encountered in the literature due to their under-reporting.
A retained surgical sponge is an avoidable surgical complication that can lead to patient morbidity, mortality and profound medico-legal implications.
Case presentation
We report a case of intra-abdominal textiloma discovered early in a 31-year-old woman who underwent cesarean section due to placenta previa.
Discussion
This complication in our surgical practice is still relevant despite the popularization of the World Health Organization checklist.
Conclusion
The purpose of reporting this case is to awaken practitioners to be more vigilant and avoid such circumstances.
Keywords: Textiloma, Abdominal surgery, Sponge, Goma
Highlights
-
•
We report a case of textilloma on a 31 years old female who underwent cesarean section due to placenta previa
-
•
Ultrasound performed found curvilinear echogenic stripes surrounded by a hypo echogenic zone suggesting a mesenteric dermoid cyst
-
•
The laparotomy was performed and discovered a gauze enveloped by the omentum at the level of the mesentery
1. Introduction
The term textiloma or corpus alienum also called gossypiboma, derived from the Latin word ‘gossypium’ meaning cotton and the Swahili word ‘boma’ meaning place of concealment or hiding place, commonly designates a foreign body, sponge or compress left involuntarily during a surgical intervention [1].
This oversight of a foreign body in the peritoneal cavity represents a formidable iatrogenic surgical complication whose frequency varies from 1 in 1000 to 1 in 5000 in the literature [2].
It is an infrequent complication of abdominal and pelvic surgery, which is difficult to estimate [3].
The incidence of gossypiboma is unclear due to the medico-legal ramifications of reporting. Its presenting symptoms vary from mild abdominal pain to significant complications including bowel perforation, bowel obstruction, inta-abdominal abscess, peritonitis, sepsis or fistula formation [4].
There are two physiological responses leading to detection of retained sponge. The first type is an exudative inflammatory reaction with abscess formation and usually leads to early detection and surgical removal. The second type is aseptic with a fibrotic reaction to the cotton material and the development of a mass [1].
We are reporting a case of mesenteric textilome on 31 years old female who underwent cesarean section due to placenta praevia with an underlying uterine fibroid. Patient was operated 3 weeks ago prior to this discovery. This case report has been reported in line with the SCARE 2020 criteria [5].
2. Case presentation
A 31-year-old patient, consulted, at the emergency room, for abdominal and pelvic pain (pelvic and right iliac fossa) 22 days after a cesarean section for placenta previa in December 2021.
The patient reported that the pain started 2 weeks after a cesarean section and was mainly localized on the right iliac fossa, without any associated gastrointestinal symptoms, consequently the apparition of fever and pain resistant to analgesics motivated the patient to consult the emergency room on night.
On physical examination, the patient was stable with a sicking look and a fever (38.1 °C). The abdomen was not distended, but a palpable mass was found in the right iliac fossa with rebound tenderness. Otherwise, the rest of the examination was unremarkable.
The laboratory workup showed an inflammatory syndrome with a CRP at 24 mg/l with a hyperleukocytosis at 14,000/mm3 PN at 79 %. The rest of the biological workup was normal.
The abdominopelvic ultrasound performed the same day reported an atypical heterogeneous calcified formation with multiple curvilinear echogenic stripes surrounded by a hypo echogenic zone suggesting a mesenteric dermoid cyst or an appendicular abcess.
There was any history of chronic disease, the patient was counselled for relaparotomy and investigations.
The patient denied any allergy to any anesthesia and consented for relaparotomy under general anesthesia. Intraoperatively a 7 cm gauze enveloped by the omentum at the level of the mesentery was discovered [Fig. 1]. The intestinal loops were normal and removal of the gauze was carried out without any incident [Fig. 2].
Fig. 1.
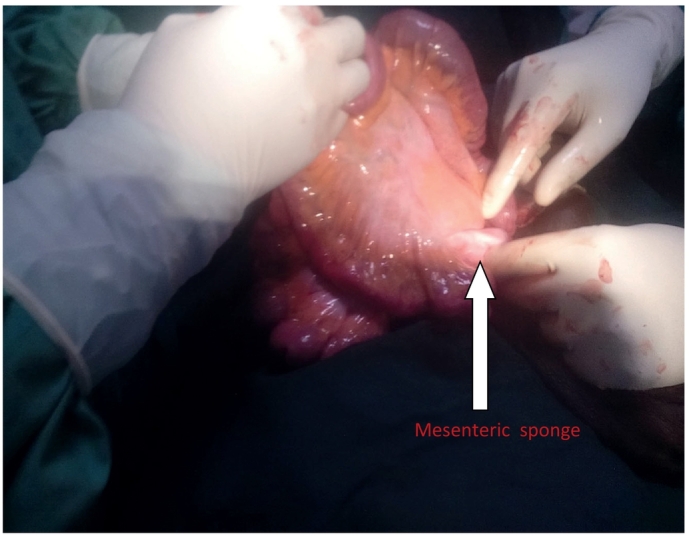
Intraoperative: The intra-abdominal gauze at the level of the mesentery.
Fig. 2.
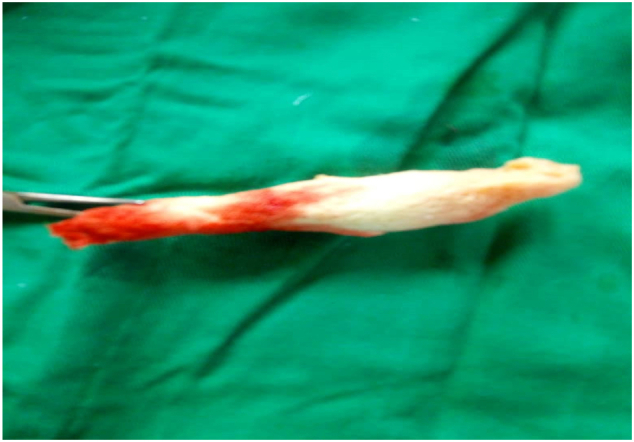
The abdominal gauze on the surgical field after its removal from the abdominal cavity.
The patient received 1 g of ceftriaxone 30 min prior to the surgery while in post-operative period, twice daily for 7 days and pain was controlled by 75 mg of diclofenac suppository per rectal twice daily for three days. She reported being satisfied with the intervention done and on 10th days post-operative, she was reviewed and reported no complaint.
The postoperative period was uneventful.
3. Discussion
Gossypiboma is a rare occurrence with a reported incidence of 1:1000–1:10,000 in intra-abdominal operations. Our case describes a mesenteric gossipiboma after cesarean section, which symptoms presented after three weeks.
The interval between the operation and presentation of gossypiboma depends on the anatomical location and pathological process. [1] Sponges may remain asymptomatic for a variable period depending on the size, site, and inflammatory response of body to it and may be detected incidentally. [6]
The possibility of a retain foreign body should be in the differential diagnosis of any postoperative condition where patient presents with pain, fever, or palpable mass. [4] Two different types of pathological foreign body reactions can occur: a fibrinous response creating adhesions and encapsulation or an exudative process leading to abscess formation. [7]
The most commonly affected site is the small intestine due to its relatively large surface area and thin walls that offer little resistance to invasion. [1]
In the abdominal cavity, the sponge may be covered by omentum and intestinal loops, which attempt to encapsulate it. The pressure and irritation exerted on the intestinal loops can lead to necrosis of the intestinal wall and the sponge erodes partially or entirely into the lumen of the intestine and this process can lead to an obstruction or a fistula.
Patients can develop symptoms including abdominal pain, nausea, vomiting, anorexia, and weight loss resulting from obstruction or malabsorption-like syndrome caused by multiple intestinal fistulas or intraluminal bacterial overgrowth [8], [9].
Prevention is an important part of disease management. Risk factors for retained surgical materials include patients with high body mass index, long operations, inexperienced staff or unexpected change in the procedure [1]. Simple precautions such as staff education, performing the WHO (World Health Organization) checklist, tagging the sponges with markers or multiple perioperative counts of sponges and materials reduce the incidence of gossypiboma [10].
Laparotomy was used for the removal of the sponge in our case and traditionally, the open approach for the removal of the sponge was more accepted compared to the laparoscopic approach. This was due to the belief that intense foreign body reaction and dense adhesions around the sponge may make the laparoscopic approach difficult [9]. Open surgery is a common approach; however, depending on location, size of foreign body and skill of the operator. Gossypiboma should be removed urgently to avoid further complications and legal ramifications [10].
4. Conclusion
Gossypibona is a frequent complication in abdominal surgery; however, precautions must be taken to avoid the retention of surgical sponge during surgical procedures because the consequences can endanger the patient's life if the diagnosis and treatment are not adapted in time.
Strict adherence to swab counts, and the avoidance of change of staff during procedures is important in decreasing the incidence. Minimally invasive accesses, simple precautions such as theater staff regular education, following the WHO checklist should be the way to reduce the incidence of gossypiboma.
Declaration of competing interest
The authors declare no conflicts of interest.
Acknowledgments
Acknowledgements
The authors are grateful to Dr. Franck Katembo SIKAKULYA for his input during revision and proof reading of this manuscript.
Sources of funding
There was no external funding sourced for this report.
Ethical approval
Not applicable.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Author contribution
JBM managed the patient and wrote the first draft. MVM, MNW helped in editing and reviewing the paper. All authors read and approved the final version to be published.
Research registration
Not applicable.
Guarantor
Jeannot Baanitse Munihire.
Provenance and peer review
Not commissioned, externally peer-reviewed.
References
- 1.Ryan George, Kawka Michal, Janakan G., Vincent Y. Presentation and surgical management of a gossypiboma presenting with small bowel obstruction. <sb:contribution><sb:title>Clin. J.</sb:title></sb:contribution><sb:host><sb:issue><sb:series><sb:title>Gastroenterol.</sb:title></sb:series></sb:issue></sb:host>. 2021;14:1067–1070. doi: 10.1007/s12328-021-01400-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Gibbs V.C., Coakley F.D., Reines H.D. Preventable errors in the operating room: retained foreign bodies after surgery. Curr. Probl. Surg. 2007;44:281–337. doi: 10.1067/j.cpsurg.2007.03.002. [DOI] [PubMed] [Google Scholar]
- 3.O'Connor A.R., Coakley F.V., Meng M.V., Eberhardt S.C. Imaging of retained surgical sponges in the abdomen and pelvis. AJR Am. J. Roentgenol. 2003 Feb;180(2):481–489. doi: 10.2214/ajr.180.2.1800481. [DOI] [PubMed] [Google Scholar]
- 4.Gawande A.A., Studdert D.M., Orav E.J., et al. Risk factors for retained instruments and sponges after surgery. N. Engl. J. Med. 2003;348:229–235. doi: 10.1056/NEJMsa021721. [DOI] [PubMed] [Google Scholar]
- 5.Agha R.A., Franchi T., Sohrabi C., Mathew G., for the SCARE Group The SCARE 2020 guideline: updating consensus Surgical CAse REport (SCARE) guidelines. Int. J. Surg. 2020;84:226–230. doi: 10.1016/j.ijsu.2020.10.034. [DOI] [PubMed] [Google Scholar]
- 6.Zantvoord Y., van der Weiden R.M., van Hooff M.H. Transmural migration of retained surgical sponges: a systematic review. Obst. Gyn. Surv. 2008;63:465–471. doi: 10.1097/OGX.0b013e318173538e. [DOI] [PubMed] [Google Scholar]
- 7.Cruz R.J., Jr., Poli de Figueiredo L.F., Guerra L. Intracolonic obstruction induced by a retained surgical sponge after trauma laparotomy. J. Trauma. 2003;55:989–991. doi: 10.1097/01.TA.0000027128.99334.E7. [DOI] [PubMed] [Google Scholar]
- 8.Saxena Neeraj, Chauhan Rohit, Chaudhary Tayod. Gossypiboma - successful retrieval through laparoscopy: a case report. Int.J.Surg. July 2021;84 doi: 10.1016/j.ijscr.2021.106109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sozutek A., Karabuga T., Bozdag A.D., et al. Asymptomatic gossypiboma mimicking a liver mass. Turk. J. Surg. 2010;26:225–228. [Google Scholar]
- 10.Kato K., Suzuki K., Sai S., Murase T., Haruta J. A case of paravesical foreign body granuloma due to surgical sponge retained for 40 years. Hinyokika Kiyo. 2000;46:491–494. [PubMed] [Google Scholar]