

Abstract
Purpose:
Many cancer survivors experience cancer-related cognitive impairment (CRCI). We conducted a randomized controlled pilot trial of 2 types of yoga practice and evaluated their effects on participants’ objective cognitive function.
Methods:
Sedentary breast or ovarian cancer survivors were randomized to practice either restorative yoga (with more meditative practice and minimal physical exertion) or vigorous yoga (with considerable physical exertion and minimal meditative practice) in 60-minute supervised sessions 3 times a week for 12 weeks, followed by 12 weeks of home practice. We used the NIH Toolbox Cognition Domain to evaluate participants at baseline, week 12, and week 24.
Results:
We enrolled 35 participants. For women in the restorative yoga group, overall cognitive function was statistically significantly improved at weeks 12 and 24 compared to baseline (P = .03 and 0.004; Cohen’s D = 0.3 and 0.5). Fluid cognitive function also significantly improved at weeks 12 and 24 (P = .02 and 0.0007; Cohen’s D = 0.3 and 0.6), whereas improvements in crystallized cognition were not significant. For women in the vigorous yoga group, significant improvement was only seen in tasks of crystallized cognition at week 24 (P = .03; Cohen’s D = 0.5). Between-group comparisons showed that at week 24, women in the restorative yoga group had significantly higher scores on fluid cognition tasks.
Conclusions:
Patients who participated in yoga practice demonstrated improvement in objective cognitive function over time. Restorative yoga may be more effective in improving fluid cognitive function at week 24 when compared to vigorous yoga. These promising findings should be confirmed in definitive studies.
Trial registration:
Clinicaltrials.gov; NCT02305498 (Date Registered: December 2, 2014)
Keywords: cancer-related cognitive impairment, CRCI, yoga, breast cancer, ovarian cancer, cancer survivor
Background
Cancer-related cognitive impairment (CRCI) is a common concern for patients during and after cancer treatment. Up to 35% of patients experience CRCI after completing cancer treatment.1-4 The mechanisms are not fully understood and optimal management is an area of active research. 5 Previous studies have evaluated self-reported cognitive impairment and observed gray matter density changes in bilateral frontal, temporal, and cerebellar regions in patients after cancer treatment. 1 So far, cognitive rehabilitation is the most studied treatment for CRCI and showed improvement in cognitive measure and has been used in clinical care. 6 However, the studies were limited by heterogeneity in study design, intervention, and outcome measures. Cognitive rehabilitation therapy itself is limited by availability of a therapist, time commitment, and lack of insurance coverage. More studies to explore therapeutic interventions that are cost effective, can be self-administered, and can lead to objective improvement of cognitive functions are needed.
Yoga practice has been investigated as an intervention for cancer patients during treatment for quality of life and other self-report measures. 7 Yoga combines physical activity with breathing and relaxation exercises to improve both physical and mental fitness. Interventions that have been associated with cognitive improvement across different cognitive impaired disease states including CRCI, aging, and early stages of cognitive degenerative diseases mostly involve aerobic exercise. 8 However, aerobic exercise requires motivated patients and discipline in complying with a regular exercise regimen. We are interested in whether yoga, with its physical and contemplative practices, can help sedentary patients who do not exercise regularly.
Previous yoga studies evaluated self-reported cognition complaints with the majority focusing on subjective patient-reported outcomes and very few focusing on objective cognitive function.9-13 Cognition has 4 domains: information processing speed, executive function, attention, and memory/concentration. In this study we used NIH Toolbox Cognition Domain testing to measure objective cognitive function. General cognitive function can be subdivided into fluid intelligence and crystallized intelligence. 14 Fluid intelligence is the ability to process new information and solve novel problems in real time. It is correlated with skills such as comprehension, problem solving, and learning. 15 Fluid cognition usually peaks early in life around age 20 then slowly declines. Crystallized intelligence is the ability to use knowledge that was previously acquired through education and experience. It experiences less age-related decline. 16
In this study we compared “restorative yoga,” which emphasizes the contemplative and relaxation components of yoga practice, with a vinyasa-based “vigorous yoga,” which emphasizes constant fluid movement in synch with breathing. Here we report data from a pilot randomized control trial that evaluated the effect of 2 types of yoga practice on cognitive function in sedentary breast and ovarian cancer survivors.
Methods
We recruited study participants at Memorial Sloan Kettering Cancer Center (MSK) through mailed recruitment letters or direct referral from breast and ovarian cancer clinics. The MSK Institutional Review Board (IRB) approved the clinical trial protocol and informed consent form (IRB #14-059). We obtained written informed consent from all individual participants included in the study. The primary end point of this pilot study is to determine the feasibility and safety of a supervised vigorous yoga practice in previously sedentary cancer patients. The results of the feasibility data have been published previously. 17
Briefly, our inclusion criteria were: woman age 18 or older; history of stage 0 to III breast cancer or stage I to III ovarian cancer; all antitumor therapies, excluding hormonal therapy, have been completed at least 60 days prior to enrollment; Eastern Cooperative Oncology Group (ECOG) Performance Status 0 to 1 within 90 days of enrollment; and sedentary: <90 minutes/week of moderate-intensity and <30 minutes/month of any high-intensity activity in the past 2 months. 18 Our exclusion criteria were: evidence of active malignant disease; breast implant; significant cardiopulmonary disease, severe arthritis, glaucoma, or any other medical conditions that make yoga practice unsafe; regular use of beta blockers or calcium channel blockers; use of any medication that would interfere with the study’s initial blood tests within 7 days of the initial study blood test; and unlikely to be compliant with the study intervention.
We randomized enrolled patients to either restorative or vigorous yoga practice groups and they attended a 60-minute class 3 times a week for 12 weeks. The Clinical Research Database (CRDB) at MSK conducted randomization in randomly permuted blocks. Assignment concealment was achieved by the CRDB computer system. Randomization was stratified by history of breast or ovarian cancer. The restorative yoga practice incorporated a combination of supine, prone, and seated resting postures with a closing 5-minute relaxation. 17 The vigorous yoga practice included a warm-up, a repeated quadruped posture sequence with arm and core strengthening, strengthening standing postures with an emphasis on breathing, inversion positions, stretching, and then a 5-minute centering and closing relaxation. 17 Participants in the vigorous yoga group wore heart rate monitors. Their heart rates were monitored in real time, and the yoga teacher instructed participants to repeat postures to increase the heart rate to 60% to 70% of each person’s individual maximal heart rate. After 12 weeks of in-person sessions, participants continued practicing the hour-long regimen at home 3 times a week for an additional 12 weeks.
We administered the NIH Toolbox Cognitive Domain 19 at baseline, week 12 after the in-person yoga practice intervention had finished, and week 24 after the home yoga practice period finished. The NIH Toolbox Cognitive Scoring uses various tasks to evaluate fluid cognitive domains including Flanker Inhibitory Control and Attention (executive functioning and attention), Dimensional Change Card Sort (executive functioning), Picture Sequence Memory (memory), List Sorting (working memory), and Pattern Comparison (processing speed) tests. There are 2 tasks that measure “crystallized intelligence” or accumulated experiential knowledge, single-word reading, and picture vocabulary. It has acceptable test-retest reliability with fluid cognitive domains concordance correlation coefficients (CCC) = 0.73 and crystallized cognitive domains CCC = 0.85. 20 It has good validity with median correlations of 0.88 for crystallized cognitive domains and 0.70 for fluid cognitive domains. 21
The sample size was 20 patients per treatment arm, which was determined by convenience rather than statistical power give that this is a pilot study. NIH Toolbox Cognitive Scores were analyzed using STATA statistical software. The NIH Toolbox Cognitive Scores prior to these analyses were adjusted for factors such as education to yield a fully-adjusted standard score. Cognition scores were analyzed using an ANCOVA model to detect significant differences between cognitive scores accounting for covariance of other variables such as baseline outcome and cancer types.
Results
We enrolled 42 subjects and randomized them equally to either group. Of the 21 subjects assigned to either group, 20 in the restorative yoga group and 15 in the vigorous yoga group started the intervention and were included in the analysis cohorts. 17 After reassessment immediately before starting the interventions, 7 subjects dropped out of the study because of safety concerns, unrelated cardiac events, scheduling issues, and no longer being sedentary. Subject characteristics at baseline are shown in Table 1. Objective cognitive function scores (NIH Toolbox Cognition Domain fully-adjusted Standard Scores (SS)) are shown in Table 2.
Table 1.
Study Subjects Baseline Characteristics.
| Restorative Yoga (N = 20; 57%) | Vigorous Yoga (N = 15; 43%) | |
|---|---|---|
| Age (range, years) | 55 (53, 60) | 58 (54, 62) |
| Race | ||
| White | 16 (80.0%) | 13 (88.6%) |
| Black | 3 (15.0%) | 0 (0.0%) |
| Asian | 1 (5.0%) | 1 (6.7%) |
| Unknown | 0 (0.0%) | 1 (6.7%) |
| Hispanic | 1 (5.0%) | 0 (0.0%) |
| Cancer type | ||
| Breast | 18 (90.0%) | 13 (86.7%) |
| Ovarian | 2 (10.0%) | 2 (13.3%) |
Table 2.
NIH Toolbox Cognition Domain Fully-Adjusted Standard Scores.
| Restorative Yoga | Vigorous Yoga | Difference between groups | Cohen’s D | |
|---|---|---|---|---|
| Fluid cognition (Baseline) | 97.1 (8.3) | 95.2 (7) | 1.9 (P = .4794) | |
| Change at Week 12 | +2.7* | +3.1 | 0.4 | 0.21 |
| (P = .0216)* | (P = .1279) | (P = .6725) | ||
| Change at Week 24 | +5.3* | +1.6 | 3.7* | 0.69 |
| (P = .0007)* | (P = .8088) | (P = .0254*) | ||
| Crystallized Cognition (Baseline) | 128.7 (10.7) | 130.2 (9.6) | 1.5(P = .6647) | |
| Change at Week 12 | +0.7 | −0.3 | 1 | 0.05 |
| (P = .4254) | (P = .9269) | (P = .6113) | ||
| Change at Week 24 | +1.5 | +4.0* | 2.5* | 0.37 |
| (P = .4594) | (P = .0294)* | (P = .0399*) | ||
| Overall Cognition Function (Baseline) | 115.9 (10.3) | 115.5 (11.1) | 0.4(P = .9049) | |
| Change at Week 12 | +2.7* | +2.1 | 0.6 | 0.10 |
| (P = .0331)* | (P = .3108) | (P = .6017) | ||
| Change at Week 24 | +5.6* | +4.9 | 0.7 | 0.09 |
| (P = .0042)* | (P = .0984) | (P = .8545) |
At baseline, the study population had high average overall cognitive function (SS 115.9 and 115.5 in Table 2), putting the study subjects in the 86th percentile of the general population, with superior to very superior scores in crystallized cognitive function with SS 128.7 and 130.2 (in the 97-98 percentile), but below average scores (mean SS = 95 and 97) on fluid cognitive function tasks (42nd-37th percentile). These scores indicate that the study participants are highly intelligent women, however their ability to solve novel problems, think and act quickly, and encode new episodic memories was disproportionately compromised (>2 standard deviations (SDs) lower).
For women in the restorative yoga group (Table 2, second column), overall cognitive function was statistically significantly improved at weeks 12 and 24, from 116 (86th percentile) to 119 (90th percentile), then 122 (93rd percentile) (Figure 3). Fluid cognitive function also significantly improved at weeks 12 and 24, from 97 (42nd percentile) to 100 (50th percentile), then 102 (55th percentile) (Figure 1), whereas the improvements in crystallized cognition were not significant, from 129 (97th percentile) to 129 (97th percentile), then 130 (98th percentile) (Figure 2). For women in the vigorous yoga group (Table 2, third column), the improvements in overall cognition, fluid cognition, and crystallized cognition were not statistically significant, except for the crystallized cognition at week 24, which went from 130 to 134 (98th-99th percentile) (Figure 1-3). Between-group comparisons showed that at week 24, women in the restorative yoga group had significantly higher scores on fluid cognition tasks. Those in the rigorous yoga group had significantly higher crystallized cognition scores at week 24. Other comparisons showed no significant between-group differences (Table 2, last column).
Figure 3.
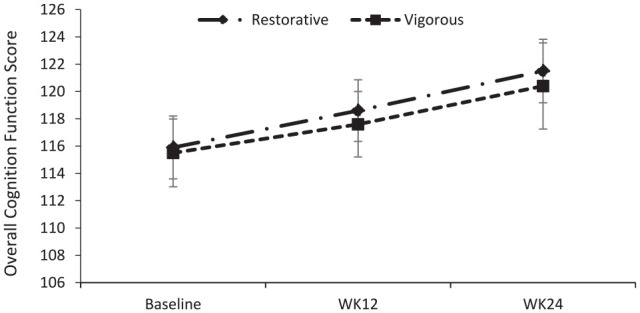
Overall cognition function over time by Yoga Group.
Figure 1.
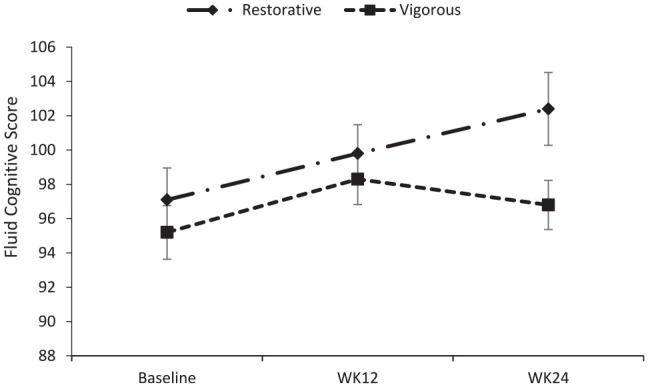
Fluid cognitive score over time by Yoga Group.
Figure 2.
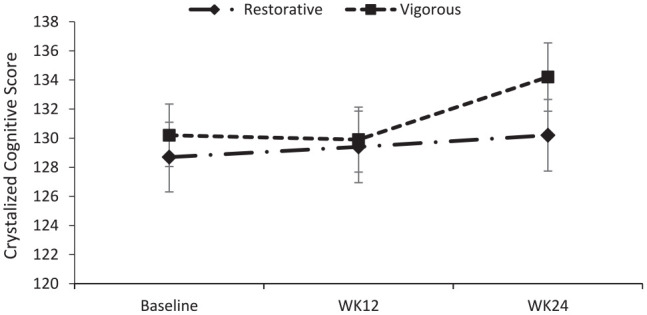
Crystalized cognitive score over time by Yoga Group.
In restorative yoga group, 2 (10%) patients experienced mild to moderate pain. In vigorous yoga group, 6 (40%) patients experience mild to moderate pain and 1 (7%) patient had mild vomiting during the study.
Discussion
CRCI is a major concern for many breast cancer survivors. They complain of decline in their ability to concentrate, form new memories, and execute problem solving, all functions of fluid cognition. Even though cognitive rehabilitation has been used and studied as a treatment for CRCI and shown some efficacy, 6 additional interventions are still needed. In this small trial, we found that consistent practice of restorative yoga by female cancer survivors led to a significant increase (a 13-percentile increase—from below average to above average) in tasks assessing fluid cognitive function when compared to baseline. This fluid cognitive score improvement suggests that the relaxation, breathing, and stretching practices supported by the restorative yoga practice may have potential to improve cognitive function in areas such as problem solving and memory. However, it is difficult to draw this conclusion because there is no usual care group to use as a comparison to tease out regression to the mean effect; additional research with an appropriate control arm is needed. Importantly, both interventions were safe.
For women in the restorative yoga group, fluid cognitive function also significantly improved at weeks 12 and 24 (P = .02 and .0007; Cohen’s D = 0.3 and 0.6), whereas improvements in crystallized cognition were not significant. To put the effect sizes in clinical context, fluid cognition in the restorative yoga group improved significantly from the 42nd percentile (score of 97) to the 55th percentile (score of 102) after 24 weeks, indicating that those participants moved up 10 percentiles among the general population.
For women in the vigorous yoga group, significant improvement was only seen in tasks of crystallized cognition at week 24 (P = .03, Cohen’s D = 0.5). This means that in the vigorous yoga group, fluid cognition improved from the 37th percentile to the 42nd percentile (score from 95 to 97), but it was not statistically significant.
For crystalized cognition, the restorative yoga group changed from the 97th percentile to the 98th percentile (score from 129 to 130), whereas the vigorous yoga group changed from the 98th percentile to the 99th percentile (score from 130 to 134). There may be a “ceiling effect” because the baseline crystalized cognition scores of this study population are already so high. From the patients’ perspective, impaired fluid cognition (ability to process and act on new information and task) is what bothered them the most. This is reflected in the relatively low fluid cognition score among this group of highly intelligent women (crystalized cognition score in the high 90th percentile of the general population). Therefore a 10-percentile improvement would be appreciated by these cancer survivors.
We also found that it was easier for sedentary cancer survivor to adhere to regular practice of restorative yoga than to the more physically demanding vigorous yoga. One hundred percent of the women in the restorative yoga group completed the 12-week period of supervised practice, with 85% completing more than two thirds of these sessions. 17 Eighty-five percent completed the 12-week home practice. The corresponding numbers for the vigorous yoga group were 87%, 73%, and 77%. Therefore, for sedentary female cancer survivors, restorative yoga is an intervention that is easier to adhere to, while also leading to improvement in fluid cognitive ability. On the other hand, it is also possible that restorative yoga focuses more on mindfulness, which has been shown to improve cognitive function, whereas vigorous yoga focuses more on the mechanistic aspects of yoga with less effect on cognition.
The main limitation of this study is its small sample size and not limited to participants with certain degree of cognitive dysfunction. It was designed as a pilot study to support a hypothesis. It was also limited by a young patient population, with average ages in the 50s in both groups. The second limitation is that most subjects in the study were breast cancer survivors. When expanded to sedentary patients with other cancer types, the results will likely vary. In addition, due to study design, as both groups received active interventions, it is difficult to discern the placebo effect. Also, the study lacked a usual care control arm, which makes it difficult to evaluate how much cognitive improvement was due to natural changes over time. Also, our study did not employ a mixed-methods design, which prevented us from including findings from different methodological perspectives. Further studies should include such outcome measurements. On the other hand, for this population, which had been highly functional cognitively, decline in fluid cognitive function was impactful and created emotional distress. Patients would very much welcome an increase in their fluid cognitive function. However, there are significant ceiling effects for crystal intelligence, making it very difficult to discern clinical significance in its improvement. Lastly, because the primary end point of this trial is not CRCI but feasibility and safety, the eligibility of this trial is not limited to patients with certain CRCI deficits. Moreover, per the International Cognition and Cancer Task Force’s recommendation, ideal CRCI research should be a double-blinded randomized controlled trial with cognitive assessments at baseline and at long-term follow-up. 22
Given that CRCI is a prevalent problem with no definitive treatment currently available, our data indicate that a restorative yoga practice is a feasible and practical intervention worthy of further adequately-powered, larger studies. Such studies will generate more definitive data on the practice of restorative yoga to improve cognitive function in breast and ovarian cancer survivors with cancer-related cognitive impairment.
Acknowledgments
The authors thank Pasha Hogan, Joseph Glaser, Catherine Genzler (yoga instructors) and Andrew Vickers, PhD (biostatistician) for their work in this study, as well as Christina Seluzicki for preparation of the manuscript.
Footnotes
Author Contributions: Design – Gary Deng, Elizabeth Ryan, Lara Benusis, Jason Konner; recruitment – Gary Deng, Ting Bao, Jason Konner; intervention – Lara Benusis, Pasha Hogan; data acquisition – Qing Li, Annika Dries; data analysis – Gary Deng, Elizabeth Ryan, Qing Li, Annika Dries; manuscript preparation – all authors.
Availability of Data and Material: Data used in the study is available for further examination from the principal investigator (Gary Deng) on reasonable request.
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Mao reports grants from Tibet Cheezheng Tibetan Medicine Co., Ltd. and from Zhongke Health International, LLC outside the submitted work. All other authors declare that they have no conflicts of interest.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by the Translational and Integrative Medicine Research Fund at Memorial Sloan Kettering Cancer Center, the Rockefeller Fund, and a National Institutes of Health/National Cancer Institute Cancer Center Support Grant (grant number P30 CA008748). Research reported in this article was also supported in part by a National Institutes of Health/National Cancer Institute award (grant number R25CA020449). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding agencies.
Consent to Participate: Written informed consent was obtained from all individual participants included in the study.
Consent for Publication: All authors consent to publication of this manuscript.
Clinical Trial Registration: NCT02305498 (Date Registered: December 2, 2014)
Ethics Approval: The study protocol has been reviewed and approved by the Institutional Review Board (IRB) of Memorial Sloan Kettering Cancer Center (MSK). All procedures performed in studies involving human participants were in accordance with the ethical standards of the IRB and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
References
- 1. Ahles TA, Root JC, Ryan EL. Cancer- and cancer treatment-associated cognitive change: an update on the state of the science. J Clin Oncol. 2012;30:3675-3686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Ganz PA, Petersen L, Castellon SA, et al. Cognitive function after the initiation of adjuvant endocrine therapy in early-stage breast cancer: an observational cohort study. J Clin Oncol. 2014;32:3559-3567. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Janelsins MC, Kesler SR, Ahles TA, Morrow GR. Prevalence, mechanisms, and management of cancer-related cognitive impairment. Int Rev Psychiatry. 2014;26:102-113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Merriman JD, Sereika SM, Brufsky AM, et al. Trajectories of self-reported cognitive function in postmenopausal women during adjuvant systemic therapy for breast cancer. Psychooncology. 2017;26:44-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Wefel JS, Kesler SR, Noll KR, Schagen SB. Clinical characteristics, pathophysiology, and management of noncentral nervous system cancer-related cognitive impairment in adults. CA Cancer J Clin. 2015;65:123-138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Fernandes HA, Richard NM, Edelstein K. Cognitive rehabilitation for cancer-related cognitive dysfunction: a systematic review. Support Care Cancer. 2019;27:3253-3279. [DOI] [PubMed] [Google Scholar]
- 7. Chandwani KD, Perkins G, Nagendra HR, et al. Randomized, controlled trial of yoga in women with breast cancer undergoing radiotherapy. J Clin Oncol. 2014;32:1058-1065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Zimmer P, Baumann FT, Oberste M, et al. Effects of exercise interventions and physical activity behavior on cancer related cognitive impairments: A systematic review. Biomed Res Int. 2016;2016:1820954. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Janelsins MC, Peppone LJ, Heckler CE, et al. YOCAS(c)(R) Yoga reduces self-reported memory difficulty in cancer survivors in a nationwide randomized clinical trial: investigating relationships between memory and sleep. Integr Cancer Ther. 2016;15:263-271. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Derry HM, Jaremka LM, Bennett JM, et al. Yoga and self-reported cognitive problems in breast cancer survivors: a randomized controlled trial. Psychooncology. 2015;24:958-966. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Galantino ML, Greene L, Daniels L, Dooley B, Muscatello L, O’Donnell L. Longitudinal impact of yoga on chemotherapy-related cognitive impairment and quality of life in women with early stage breast cancer: a case series. Explore. 2012;8:127-135. [DOI] [PubMed] [Google Scholar]
- 12. Zeng Y, Dong J, Huang M, et al. Nonpharmacological interventions for cancer-related cognitive impairment in adult cancer patients: A network meta-analysis. Int J Nurs Stud. 2020;104:103514. [DOI] [PubMed] [Google Scholar]
- 13. Baydoun M, Oberoi D, Flynn M, et al. Effects of Yoga-based interventions on cancer-associated cognitive decline: a systematic review. Curr Oncol Rep. 2020;22:100. [DOI] [PubMed] [Google Scholar]
- 14. Cattell RB. Theory of fluid and crystallized intelligence: A Critical Experiment. J Educ Psychol. 1963;54:1-22. [DOI] [PubMed] [Google Scholar]
- 15. Unsworth N, Fukuda K, Awh E, Vogel EK. Working memory and fluid intelligence: capacity, attention control, and secondary memory retrieval. Cogn Psychol. 2014;71:1-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. McArdle JJ, Ferrer-Caja E, Hamagami F, Woodcock RW. Comparative longitudinal structural analyses of the growth and decline of multiple intellectual abilities over the life span. Dev Psychol. 2002;38:115-142. [PubMed] [Google Scholar]
- 17. Lapen K, Benusis L, Pearson S, et al. A feasibility study of restorative yoga versus vigorous yoga intervention for sedentary breast and ovarian cancer survivors. Int J Yoga Ther. 2018;28:79-85. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Godin G, Shephard RJ. A simple method to assess exercise behavior in the community. Can J Appl Sport Sci. 1985;10:141-146. [PubMed] [Google Scholar]
- 19. Gershon RC, Wagster MV, Hendrie HC, Fox NA, Cook KF, Nowinski CJ. NIH toolbox for assessment of neurological and behavioral function. Neurology. 2013;80: 11 Suppl 3 S2-S6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Scott EP, Sorrell A, Benitez A. Psychometric Properties of the NIH Toolbox Cognition Battery in Healthy Older Adults: reliability, validity, and agreement with Standard Neuropsychological Tests. J Int Neuropsychol Soc. 2019;25:857-867. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Akshoomoff N, Beaumont JL, Bauer PJ, et al. VIII. NIH Toolbox Cognition Battery (CB): composite scores of crystallized, fluid, and overall cognition. Monogr Soc Res Child Dev. 2013;78:119-132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Wefel JS, Vardy J, Ahles T, Schagen SB. International Cognition and Cancer Task Force recommendations to harmonise studies of cognitive function in patients with cancer. Lancet Oncol. 2011;12:703-708. [DOI] [PubMed] [Google Scholar]