

ABSTRACT
Objective.
To evaluate how sociodemographic factors and food intake affect survey respondents’ perceptions of the quality of their diet.
Methods.
This cross-sectional analysis is based on a nonprobability sample of 374 participants in Jamaica aged ≥18 years. The three-stage process used a simple random sample to select three parishes; the main commercial areas of each parish were chosen for sampling. To ensure the inclusion of a cross-section that was as representative as possible, the sample included both public and private sector businesses, such as those in retail, hospitality and tourism as well as nongovernmental organizations. Employees and patrons completed a questionnaire regarding their food consumption and their perception of their own diet. Multiple correspondence analysis was used to evaluate the nonlinear relationships among the variables. The results of the analysis guided the specification of a multivariate logistic regression model that was used to estimate the relationship between sociodemographic factors, food intake and perceived eating patterns.
Results.
The average predicted probability of perceiving a diet as unhealthy was reduced when the respondent was male, economically active, in good health, and married or in a common-law relationship. The probability of perceiving a diet as unhealthy was increased for respondents with a college degree and those living in a household that had a male as the sole head. Consuming healthful food and drink reduced the perception of having a poor diet and vice versa, indicating there are possibly connections between food intake, the perception of diet quality and actual diet quality.
Conclusions.
This exploratory analysis established links between perceived diet quality, eating habits and sociodemographic factors. The impact on the perception of diet quality can be negative or positive, depending on the variable under consideration.
Keywords: Demography, feeding behavior, perception, diet
RESUMEN
Objetivo.
Evaluar cómo los factores sociodemográficos y la ingesta de alimentos afectan las percepciones de las personas encuestadas sobre la calidad de su alimentación.
Métodos.
Este análisis transversal se basa en una muestra no probabilística de 374 participantes mayores de 18 años en Jamaica. En el proceso, de tres etapas, se utilizó una muestra aleatoria simple para seleccionar tres distritos; para el muestreo, se eligieron las principales áreas comerciales de cada distrito. Para garantizar la inclusión de una sección transversal lo más representativa posible, la muestra incluyó a empresas de los sectores público y privado, como las del comercio minorista, hotelería y turismo, así como a organizaciones no gubernamentales. Tanto empleados como clientes llenaron un cuestionario sobre su consumo de alimentos y su percepción sobre su alimentación. Para evaluar las relaciones no lineales entre las variables se utilizó el análisis de correspondencia múltiple. Los resultados del análisis se usaron como guía para las especificaciones de un modelo de regresión logística multivariante, utilizado para estimar la relación entre los factores sociodemográficos, la ingesta de alimentos y los patrones de alimentación percibidos.
Resultados.
La probabilidad promedio predicha de percibir que un régimen alimentario es poco saludable era menor cuando el encuestado era de sexo masculino y económicamente activo, tenía buena salud y estaba casado o en una unión de hecho. La probabilidad de percibir un régimen alimentario como poco saludable era mayor en el caso de los encuestados con título universitario y de los que vivían en un hogar con un hombre como único cabeza de familia. El consumo de alimentos y bebidas saludables redujo la percepción de tener una mala alimentación y viceversa, lo que indica la posible existencia de una relación entre la ingesta de alimentos, la percepción de la calidad del régimen alimentario y la calidad real del régimen alimentario.
Conclusiones.
En este análisis exploratorio se estableció una relación entre la percepción de la calidad del régimen alimentario, los hábitos alimentarios y los factores sociodemográficos. El impacto sobre la percepción de la calidad del régimen alimentario puede ser negativo o positivo, según la variable considerada.
Palabras clave: Demografía, conducta alimentaria, percepción, dieta
RESUMO
Objetivo.
Avaliar como fatores sociodemográficos e a ingestão de alimentos influenciam a percepção dos participantes da pesquisa sobre a qualidade de sua alimentação.
Métodos.
Trata-se de uma análise transversal realizada em uma amostra não probabilística com 374 participantes maiores de 18 anos na Jamaica. Três localidades no país foram selecionadas por meio de um processo de amostragem aleatória simples em três etapas, com amostragem da população nas áreas comerciais centrais de cada localidade. Para garantir uma boa amostra transversal representativa da população, foram incluídos estabelecimentos comerciais dos setores público e privado, como varejistas, hotelaria e turismo e organizações não governamentais. Clientes e empregados responderam um questionário sobre seu consumo de alimentos e percepção sobre a própria alimentação. Uma análise de correspondência múltipla foi realizada para avaliar as relações não lineares entre as variáveis e, a partir dos resultados desta análise, foi construído um modelo de regressão logística multivariada para estimar a relação entre fatores sociodemográficos, consumo de alimentos e padrões alimentares percebidos.
Resultados.
A probabilidade prevista média de perceber a alimentação como pouco saudável foi menor entre os participantes do sexo masculino, economicamente ativos, com boa saúde e casados ou em união estável. A probabilidade de perceber a alimentação como pouco saudável foi maior entre os participantes com nível superior de escolaridade e que residiam em um ambiente familiar com uma pessoa do sexo masculino como chefe de família. Consumir alimentos e bebidas saudáveis foi associado a uma percepção menor de má alimentação, e vice-versa, o que indica um possível vínculo entre o consumo de alimentos, a percepção da qualidade da alimentação e a qualidade efetiva da alimentação.
Conclusões.
Esta análise exploratória demonstrou existir um vínculo entre qualidade percebida da alimentação, hábitos alimentares e fatores sociodemográficos. A influência na percepção da qualidade da alimentação é negativa ou positiva dependendo da variável considerada.
Palavras-chave: Demografia, comportamento alimentar, percepção, dieta
The global impact of noncommunicable diseases (NCDs) is profound. Altogether 71% of all deaths are caused by NCDs, affecting roughly 41 million persons per year, with 85% of these deaths occurring in low- and middle-income countries. Of these deaths, 15 million are premature, occurring in people aged between 30 and 69 years. Globally, cardiovascular diseases are the leading annual cause of NCD-related death (17.9 million deaths), followed by cancers (9.3 million), respiratory diseases (4.1 million) and diabetes (1.5 million) (1). The World Health Organization’s Region of the Americas is not spared the ravages of this epidemiological phenomenon. The number of NCD-related deaths in the Region is estimated to be 5.5 million each year (2).
NCDs are a significant public health challenge in Jamaica, and they are among the foremost cause of mortality. Estimates in 2015 revealed that 70% of deaths in Jamaica occurred among persons dying from one of the four major NCDs. A substantial number of these deaths are preventable, as are the enduring disability and reduced quality of life brought on by these diseases (3).
In addition, the impact of NCDs extends far beyond epidemiology. Indeed, these diseases threaten to upend the substantial social and economic gains that have been secured during the past several decades. Estimates show that the cumulative loss of global output due to the top four NCDs and mental illness will be US$ 47 trillion during 2010–2030. In 2010, these losses represented 75% of global gross domestic product (4). A 2021 article noted that in Jamaica, NCDs and mental illness are predicted to produce losses in economic output of US$ 17.2 billion during the next 15 years (5).
Moreover, the burden associated with NCDs is propelled by a multifaceted collection of variables, including ageing populations and geoeconomic developments that have heightened individuals’ contact with several environmental and behavioral risk factors (6). Modifiable behavioral risk factors include the use of tobacco and alcohol, the amount of physical activity and the consumption of unhealthy diets containing substantial amounts of ultraprocessed foods. Meanwhile, raised blood pressure and overweight and obesity are among the metabolic risk factors (1). Therefore, achieving better health outcomes by controlling NCDs significantly hinges on reducing these risk factors by applying proven remedies, such as discouraging tobacco and alcohol use and encouraging increased levels of physical activity (7–10). In addition to the effectiveness of the above measures in averting significant NCD-related health, social and economic burdens, improving the quality of people’s diet is an important measure that can lead to better health outcomes and a substantial reduction in NCD-related premature deaths (11, 12).
Although the promotion of healthier dietary practices can prove invaluable, it requires a better understanding of the factors that influence people’s perceptions of their nutritional habits. Moreover, such knowledge can provide essential insights into how changes in these factors affect a person’s perceptions of their diet, and these changes in perception may reflect actual changes in diet quality (13). Therefore, this study sought to determine how sociodemographic factors affect survey respondents’ views of the quality of their diet and to assess the role that food consumption plays in forming the perception of diet quality.
MATERIALS AND METHODS
Given resource and other technical constraints, this cross-sectional analysis is based on a nonprobability sample of 374 participants in Jamaica aged ≥18 years. The three-stage process used a simple random sample to select three parishes; the main commercial areas of each parish were then sampled. A wide variety of businesses were included, spanning public, private and nongovernmental organizations in the retail, finance, hospitality and tourism, manufacturing, communications, health, education and other service sectors. This variety was included to ensure that the sample of respondents was as representative as possible. Employees of the businesses or organizations and some patrons were asked to complete a predesigned questionnaire that included questions about food consumption and a one-question self-assessment of the quality of the respondent’s diet. Respondents were asked, “Do you generally (most of the time) eat and drink healthily or unhealthily?”
Statistical analysis
A multivariate logistic regression model was used to investigate the determinants of perceived eating habits. The dichotomous dependent variable was perceived diet quality based on each respondent’s self-assessment: responses were coded 1 for unhealthy and 0 for healthy. However, first we used multiple correspondence analysis (MCA), an unsupervised, multivariate technique (14). This technique describes the nature of the relationships that exist between the outcome variable and the other sociodemographic and food intake variables. MCA provides early guidance regarding which variables are best suited for the regression model.
Using the results of the MCA analyses as a guide, the logistic regression was specified. The sociodemographic variables included in the model are gender, age group, college degree status (college degree versus no college degree) and health status (healthy versus having a health condition). Other variables in the model included income bracket (low, middle or high), gender of the head of household and region where the respondent lives (central, eastern or western region of Jamaica). The variable relationship status (married or in a common-law union versus not married or in a common-law union) and a binary variable indicating whether the household is single-headed or not (number of heads of household) were also specified. In addition, other binary variables signaling the intake of particular foods or drinks were included as explanatory variables, where 1 indicated the consumption of an item and 0 its non-consumption. These items included meat (pork, beef, goat or chicken), alcoholic drinks, carbonated beverages, crackers, chips, ice-cream, sausages and punches. A variable measuring the frequency of fruit consumption was also specified in the model, with values ranging from 0 to ≥3 times per day.
The model was estimated and tested for adherence to model assumptions and potential data and specification issues. To this end, a variance inflation factor test for multicollinearity was conducted. A link test for model misspecification (15) and several other goodness-of-fit tests, including count, adjusted count and receiver operating characteristic analyses, were also conducted. Another critical procedure involved identifying and remedying influential observations using the Pregibon (16) delta–beta influence statistic.
The impact of sociodemographic factors and food intake on a respondent’s perceptions of their general diet was quantified by estimating the probability of a “positive” outcome (that is, viewing oneself as an unhealthy eater). This is accomplished by estimating the average marginal effect. In our case, since most of the predictors are dichotomous (binary), the average marginal effect is calculated as the average of discrete changes from 0 to 1. The joint effects of pairs of variables on the probability of a perception of unhealthy eating were also assessed.
Ethical approval for this study was granted by the Faculty of Medical Sciences Ethics Committee of The University of the West Indies in Jamaica. Each participant gave informed consent at the beginning of the questionnaire. To ensure the anonymity of the data, no personal identifiers were used in the data collection process.
RESULTS
MCA was first conducted on the dependent variable and the sociodemographic variables, and then with the dependent variable and only the consumption variables. The biplot (Figure 1) of the sociodemographic analysis shows that 66.7% of the variation among the sociodemographic variables can be plotted in two dimensions. The MCA plot is a map of the variables plotted in a 2-dimensional geometric space. In this context, Dimensions 1 and 2 are similar in interpretation to the y- and x-axes. They can also represent a particular feature or factor as determined by the variables contained therein. Of particular interest are the variables that cluster in the same plot quadrant, indicating an association. In this case, the perception of a generally unhealthy diet (circle in the upper right quadrant) is associated with respondents living in a single-headed household with a female head and with respondents who were not married or in a common-law relationship, among others. Further, a clear and contrasting relationship emerges, when compared with unhealthy eating, between the perception of healthy eating and living in a non-single-headed household, being healthy and being married or cohabiting (lower left quadrant).
FIGURE 1. Multiple correspondence analysis plot of sociodemographic variables and outcome variables for survey respondents in Jamaica, 2020.
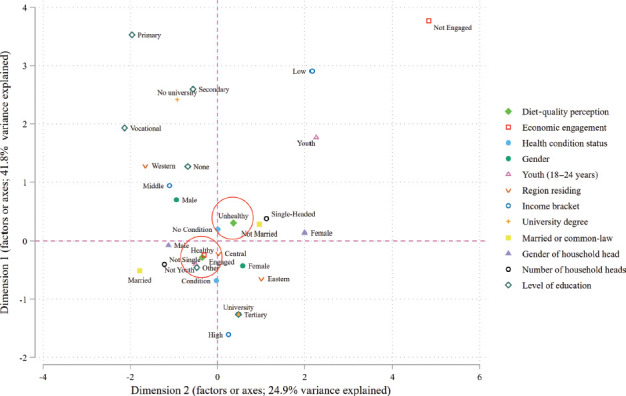
Source: Figure prepared by authors from the study results.
Note: The figure is a map of the variables plotted in a 2-dimensional geometric space. In this context, Dimensions 1 and 2 are similar in interpretation to the y- and x-axes. They can also represent a particular feature or factor as determined by the variables contained therein. Variables clustered in the same quadrant indicate that there is an association among them. Circles indicate the location of alternate values of the diet-quality perception variable.
Figure 2 shows the analysis of eating patterns: 92.8% of variation among the consumption variables can be plotted in two dimensions. In general, consuming less healthful items is associated with a perception of unhealthy eating; the reverse is also true. For this study, less healthful items are those that are high in salt, sugar or fat; that are highly processed or ultraprocessed; and those known to cause harm to the body, such as tobacco and alcohol. Healthier items are those that are not high in salt, fat or sugar; are not ultraprocessed; and contain no tobacco or alcohol.
FIGURE 2. Multiple correspondence analysis plot of food and drink consumed and outcome variables for survey respondents in Jamaica, 2020.
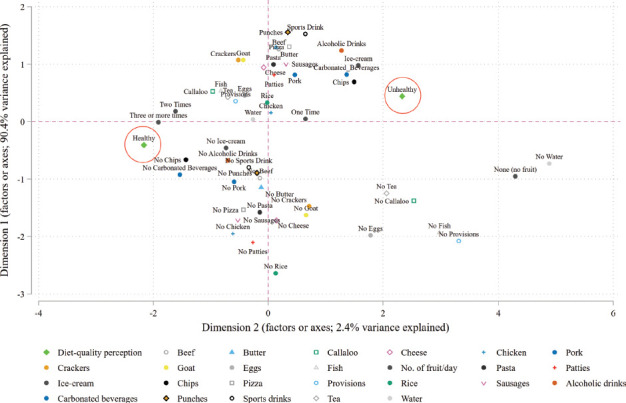
Source: Figure prepared by authors from the study results.
Note: The figure is a map of the variables plotted in a 2-dimensional geometric space. In this context, Dimensions 1 and 2 are similar in interpretation to the y- and x-axes. They can also represent a particular feature or factor as determined by the variables contained therein. Variables clustered in the same quadrant indicate that there is an association among them. Circles indicate the location of alternate values of the diet-quality perception variable.
The diagnostic test showed no evidence of model misspecification (link test P value = 0.867). The variance inflation factor indicated no evidence of multicollinearity (average = 1.44). Tests for high leverage points revealed data cleaning issues missed during the initial cleaning exercise; these were appropriately addressed and the model re-estimated. Furthermore, the count was 79%, the adjusted count (correctly classified outcomes) was 56% and receiver operating characteristic was 89%, all of which measure the model’s overall accuracy, indicating a reasonably accurate model.
Interpreting the model began with analyzing the predicted probabilities and their average discrete change. As scalar measures for assessing the magnitude of a variable’s effect, predicted probabilities and their average discrete change tend to provide more information compared with odds ratios, for instance (17). Table 1 displays the probabilities related to the sociodemographic variables and indicates that if a respondent is not economically active, looking for a job or engaged in some other type of economic activity, then the average predicted probability of a perception of unhealthy eating is reduced, from 0.675 to 0.463, a change of −0.212 (P = 0.035). Similarly, the model indicates that a large and statistically significant difference exists between male and female respondents, in which the perception of consuming an unhealthy diet is approximately two times more likely for a female (0.604) than for a male (0.291), a difference of −0.313 (P < 0.000).
TABLE 1. Average marginal effects for sociodemographic variables (predicted probabilities) for survey respondents in Jamaica, 2020.
|
Variables |
Change |
From |
To |
P value |
|---|---|---|---|---|
|
Economic activity |
|
|
|
|
|
Economically active versus not economically active |
−0.212 |
0.675 |
0.463 |
0.035 |
|
Health status |
|
|
|
|
|
Healthy versus having a health condition |
−0.114 |
0.570 |
0.456 |
0.032 |
|
Age group (years) |
|
|
|
|
|
25–34 versus 18–24 |
0.144 |
0.398 |
0.541 |
0.038 |
|
35–44 versus 18–24 |
0.128 |
0.398 |
0.526 |
0.100 |
|
≥45 versus 18–24 |
0.018 |
0.398 |
0.416 |
0.829 |
|
35–44 versus 25–34 |
−0.015 |
0.541 |
0.526 |
0.803 |
|
≥45 versus 25–34 |
−0.125 |
0.541 |
0.416 |
0.055 |
|
≥45 versus 35–44 |
−0.110 |
0.526 |
0.416 |
0.122 |
|
Gender |
|
|
|
|
|
Male versus female |
−0.313 |
0.604 |
0.291 |
0.000 |
|
Region where respondent lives |
|
|
|
|
|
Central versus western |
−0.182 |
0.584 |
0.402 |
0.003 |
|
Eastern versus western |
−0.112 |
0.584 |
0.472 |
0.072 |
|
Eastern versus central |
0.070 |
0.402 |
0.472 |
0.204 |
|
Income bracket |
|
|
|
|
|
Middle income versus low income |
0.063 |
0.425 |
0.488 |
0.478 |
|
High income versus low income |
−0.068 |
0.425 |
0.357 |
0.427 |
|
High income versus middle income |
−0.131 |
0.488 |
0.357 |
0.012 |
|
College education |
|
|
|
|
|
College degree versus no college degree |
0.126 |
0.339 |
0.465 |
0.007 |
|
Relationship status |
|
|
|
|
|
Married or in a common-law relationship versus not married or in a common-law relationship |
−0.205 |
0.544 |
0.339 |
0.000 |
|
Gender of head of household |
|
|
|
|
|
Male versus female |
0.182 |
0.392 |
0.574 |
0.001 |
|
Number of heads of household |
|
|
|
|
|
Single-headed versus not single-headed |
0.006 |
0.500 |
0.506 |
0.919 |
Source: Table prepared by authors from study results.
The gender of the head of household and the region in which respondents lived also proved crucial. Respondents who resided in a male-headed household compared with those living in a female-headed home were less likely to perceive that they ate an unhealthy diet: 0.392 for a male head of household and 0.574 for a female head of household, a difference of 0.182 (P = 0.001). This result did not agree with the MCA, which showed an association between female-headed households and perceptions of unhealthy eating. Furthermore, the model suggested that, on average, living in the central or eastern region compared with living in the western region reduced the probability of having a perception of unhealthy eating, from 0.584 to 0.402 (P = 0.003) for the central versus western region and from 0.584 to 0.472 (P = 0.072) for the eastern versus western region.
Relationship status significantly impacted a respondent’s perception of their general dietary habits. On average, union compared with not being married or in a common-law union reduced a respondent’s probability of perceiving that they generally ate unhealthily by −0.205 (from 0.544 to 0.339; P = 0.000). Additionally, on average, having a college degree made it more likely that a respondent perceived their general consumption practices to be unhealthy, increasing the probability from 0.339 to 0.465, a change of 0.126 (P = 0.007).
A person’s general health status was also shown to influence their perception of their diet. On average, being healthy decreased the probability of having the perception of unhealthy eating by −0.114 (P = 0.032), from 0.570 to 0.456, compared with those who had a health condition. The effects of age and income were only partially influential in the model. For the income brackets, only the change between middle income and high income was significant. On average, earning a monthly income in the high-income bracket compared with the middle-income range reduced the probability of having a perception of unhealthy eating by −0.131 (P = 0.012), from 0.488 to 0.357. Meanwhile, the effect of age was mixed and significant only at the change between 25–34 years and 18–24 years (0.144), and it was barely significant at the 5% level for the change between being aged ≥45 years and 25–34 years (−0.125).
Generally, the effects of the consumption variables (Table 2) were highly significant. Further, consuming all items that are commonly known to be less beneficial to health increased a respondent’s probability of indicating they consumed a generally unhealthy diet. The converse was also shown to be true. Additionally, on average, regular consumption of meat was shown to substantially increase the probability of a respondent perceiving that they ate unhealthily, from 0.116 to 0.499, a change of 0.383 (P = 0.000). Likewise, consuming carbonated beverages and alcoholic drinks predictably increased the probability of a respondent perceiving that they ate a generally unhealthy diet by, respectively, 0.177 (P = 0.001) and 0.130 (P = 0.012).
TABLE 2. Average marginal effects for consumption variables (predicted probabilities) for survey respondents in Jamaica, 2020.
|
Variables |
Change |
From |
To |
P value |
|---|---|---|---|---|
|
Alcoholic drinks versus no alcoholic drinks |
0.130 |
0.434 |
0.564 |
0.012 |
|
Carbonated beverages versus no carbonated beverages |
0.177 |
0.379 |
0.555 |
0.001 |
|
Sausages versus no sausages |
0.058 |
0.443 |
0.500 |
0.328 |
|
Ice-cream versus no ice-cream |
0.096 |
0.453 |
0.549 |
0.068 |
|
Crackers versus no crackers |
−0.144 |
0.568 |
0.424 |
0.003 |
|
Punches versus no punches |
0.120 |
0.433 |
0.553 |
0.029 |
|
Chips versus no chips |
0.161 |
0.401 |
0.563 |
0.001 |
|
Meat versus no meat |
0.383 |
0.116 |
0.499 |
0.000 |
|
Frequency of fruit consumption |
|
|
|
|
|
One time per day versus none |
−0.269 |
0.815 |
0.547 |
0.000 |
|
Two times per day versus none |
−0.474 |
0.815 |
0.341 |
0.000 |
|
Three or more times per day versus none |
−0.584 |
0.815 |
0.231 |
0.000 |
|
Two times per day versus one time per day |
−0.206 |
0.547 |
0.341 |
0.000 |
|
Three or more times per day versus one time per day |
−0.315 |
0.547 |
0.231 |
0.000 |
|
Three or more times per day versus two times per day |
−0.110 |
0.341 |
0.231 |
0.132 |
Source: Table prepared by authors from study results.
The results also show the strong influence of fruit consumption and its frequency. When compared with respondents who did not normally consume fruit, consuming fruit only once per day reduced the probability of having a self-perception of an unhealthy diet by −0.269 (P = 0.000), from 0.815 to 0.547. Also, when fruit was consumed twice per day, the reduction in the average predicted probability of perceiving one’s diet as unhealthy nearly doubled to −0.474 (P = 0.000). A similar trend was observed for every increase in fruit consumption except for that moving from twice per day to three or more times per day, which was not significant.
A table of predictions for selected pairs of variables was produced to assess their joint effects on the probability of a respondent perceiving that they consumed an unhealthy diet (Table 3). The results showed that for a participant who was average on all characteristics and lived in the western region, having a college degree significantly increased the predicted probability that they would perceive their diet as unhealthy by 0.355 (P = 0.012). The size of the effect was smaller for those residing in the central (0.226; P = 0.004) and eastern (0.292; P = 0.004) regions. Similarly, the effect of a college degree was larger for female and unmarried participants, increasing the respective predicted probabilities by 0.356 (P = 0.017) for female respondents with a college degree and 0.347 (P = 0.008) for unmarried respondents with a college degree compared with male participants with a college degree (0.116; P = 0.019) and male participants who are married (0.173; P = 0.01). The regular consumption of alcoholic beverages triggered a larger increase in the predicted probability of having a perception of unhealthy eating in females (0.221; P = 0.009) than in males (0.095; P = 0.044). Furthermore, for a female participant who was average on all characteristics, being married or in a common-law relationship significantly reduced the predicted probability of having a perception of an unhealthy diet by −0.370 (P = 0.000). Comparatively, the impact of marriage for males was −0.107 (P = 0.008).
TABLE 3. Joint average marginal effects of selected variables on the probability of the perception of consuming an unhealthy diet for survey respondents in Jamaica, 2020.
|
Change variable |
By variable |
Change |
P value |
|
|---|---|---|---|---|
|
Region |
College |
No college |
|
|
|
Western |
0.649 |
0.295 |
0.355 |
0.012 |
|
Central |
0.323 |
0.097 |
0.226 |
0.004 |
|
Eastern |
0.445 |
0.153 |
0.292 |
0.004 |
|
Gender |
College |
No college |
|
|
|
Female |
0.692 |
0.336 |
0.356 |
0.017 |
|
Male |
0.157 |
0.041 |
0.116 |
0.019 |
|
Married a |
College |
No college |
|
|
|
Not married |
0.599 |
0.252 |
0.347 |
0.008 |
|
Married |
0.239 |
0.066 |
0.173 |
0.010 |
|
Gender |
Alcohol use |
No alcohol use |
|
|
|
Female |
0.710 |
0.489 |
0.221 |
0.009 |
|
Male |
0.169 |
0.073 |
0.095 |
0.044 |
|
Gender |
Married |
Not married |
|
|
|
Female |
0.294 |
0.664 |
−0.370 |
0.000 |
|
Male |
0.033 |
0.141 |
−0.107 |
0.008 |
|
Number of heads of household |
Male head |
Female head |
|
|
|
Not single-headed |
0.369 |
0.264 |
0.105 |
0.432 |
|
Single-headed |
0.547 |
0.120 |
0.427 |
0.000 |
|
Age group (years) |
Healthy |
Has health condition |
|
|
|
18–24 |
0.187 |
0.354 |
−0.167 |
0.087 |
|
25–34 |
0.403 |
0.616 |
−0.213 |
0.036 |
|
35–44 |
0.375 |
0.588 |
−0.213 |
0.038 |
|
≥45 |
0.209 |
0.386 |
−0.177 |
0.048 |
|
Gender |
Economically active |
Not economically active |
|
|
|
Female |
0.549 |
0.861 |
−0.312 |
0.006 |
|
Male |
0.092 |
0.339 |
−0.247 |
0.178 |
Source: Table prepared by authors from study results.
Married or in a common-law relationship.
Living with a single head of household likewise proved influential. For a participant who was average on all characteristics and lived in a single-headed household, having a male as the head of household significantly increased the predicted probability of respondents classifying their diet as unhealthy, by 0.427 (P = 0.000). However, the gender of the head of household for those who did not live in a family with a single head was not statistically significant (P = 0.432). This result adds context to the findings shown in Table 1 about the gender of the head of household, showing that gender matters for those with only a single head of household.
Moreover, the model predicts that for a respondent aged 18–24 years, being healthy reduced the predicted probability of perceiving they had an unhealthy diet by −0.167. While this effect is significant only at the 10% level (P = 0.087), the effect for the other age groups is significant at the 5% level, but it generally diminishes with age. The model also showed that the employment situation is important regardless of gender. For example, being a female who is economically active significantly reduced the predicted probability of having a perception of unhealthy eating, by an average of −0.312 (P = 0.006). In contrast, for male respondents the change was −0.247, but it was not significant (P = 0.178).
DISCUSSION
This study established that sociodemographic factors and food intake patterns in Jamaica significantly influence how individuals perceive their diets, which is in line with the findings of other studies (13, 18). It is instructive that consuming all of the foods and drinks that are commonly known to be less beneficial to health increased respondents’ probability of perceiving themselves as eating unhealthily, while consuming the healthier foods had the reverse effect. This suggests that there is some nutritional awareness regarding these foods and drinks and that health messages are being received, whether disseminated through the media, family or cultural interactions. This finding raises the question of how to convert knowledge into action. It highlights a need for greater insight into the barriers to healthy eating that appear more potent than the awareness of the need for change. The analysis of the survey results indicated that younger, less educated and lower-income respondents were more likely to consume some of the less healthful items, pointing to a need to target these subpopulations. Further, the results also suggest that changes in predicted probability are at least partially reflective of changes in diet quality. What is more, the predicted probability of a respondent perceiving that they consume an unhealthy diet is reduced when the respondent is male, economically active, in good health, married or in a common-law relationship and living in either the central or eastern region of Jamaica.
Other studies (13) have found no statistically significant differences between the self-perception of eating habits among males and females. Nonetheless, these results indicate that the male respondents may be overly optimistic when compared with the female respondents about the healthfulness of their diet and may, therefore, be more resistant to change (19, 20). Indeed, the results of the analyses of the joint effects (Table 3) are suggestive of this assertion, showing that the consumption of alcohol increases the predicted probability of having the perception of eating an unhealthy diet is less for male respondents (0.095) than for female respondents (0.221). Thus, the undue optimism of males may require special efforts to align their perceptions with their nutritional realities.
Additionally, the job situation variable (Economic activity, Table 1) speaks to the impact of economic factors on diet quality (21), and this, in turn, impacts the perception of one’s diet. Related investigations (18) have found a statistically significant difference in diet perception associated with this variable. Further, joint effects analyses (Table 3) indicate that economically active female respondents are less likely to perceive their diets as unhealthy. This improvement in a respondent’s economic situation (that is, moving from not being economically active to becoming economically active and from middle-income to high-income) seems to improve the quality of their diet and bring about a corresponding reduction in the predicted probability of the self-perception of eating an unhealthy diet. Therefore, any policy that enhances employment prospects and augments income may result in healthier eating choices.
The general health status of respondents was also associated with a reduced predicted probability of the perception of consuming an unhealthy diet. Persons with a health condition were more likely to judge their diets as unhealthy, which suggests a general awareness of the connection between diet and health (18, 22). Surprisingly, having a college degree was predicted to increase the probability of the perception of consuming an unhealthy diet. This result appears to contradict previous studies (23, 24) that showed a positive correlation between higher education and having a healthy diet. A possible explanation for this apparent divergence lies in the fact that the outcome variable in our model measures perceptions of diet quality. This perception may become more aligned with reality as education levels increase, even without a corresponding change in diet quality, a known possibility (25–29).
The statistical significance of the gender of the head of household for those living with a single head of household is instructive: it shows there is an increased likelihood of perceiving that an unhealthy diet is consumed when a male heads the home (Table 3). If these differences in perception reflect differences in actual diet quality, then the findings suggest there are gender differences in spending patterns that affect the household’s nutrition. Another study (30) found that the presence of females in the home, who tend to do most of the food preparation and are more health conscious (31, 32), improves the entire family’s welfare. Furthermore, in agreement with other findings (33, 34) that link marriage (or cohabitation) to improved diet quality, our results indicated the same. Further, joint effects analyses (Table 3) revealed that married or cohabiting female respondents experienced a larger reduction in their perception of unhealthy eating (−0.370) when compared with married or cohabiting men (−0.107). However, the reason for the observed difference is not apparent.
Nonetheless, the current study is limited by the fact that the sampling process was nonprobabilistic, so further research is needed to confirm these findings for the broader Jamaican population. Despite this, the results are based on a robust and well-accepted estimation process and provide policymakers with a better understanding of the factors that influence perceptions of diet quality in Jamaica, which are likely linked to a person’s actual diet. Further, the results suggest there is no knowledge deficit regarding healthy eating, but instead point to other barriers. We conclude that sociodemographic factors impact a person’s perceptions of the quality of their diet, and the impact can be negative or positive depending on the variable under consideration. Eating habits are connected with this perception, the nature of which varies according to what is consumed. Recommendations for policies to address these issues include identifying the barriers to healthy eating and implementing fiscal and social measures to reduce or eliminate these barriers. These measures should aim to make eating healthily simple, convenient and affordable. Further, these measures should target males, the economically vulnerable and young subpopulations, who are more inclined to consume low-quality foods.
Disclaimer.
Authors hold sole responsibility for the views expressed in the manuscript, which may not necessarily reflect the opinion or policy of the Revista Panamericana de Salud Pública/Pan American Journal of Public Health or the Pan American Health Organization (PAHO).
Acknowledgements.
The authors thank Dr Stanley Lalta, Dr Anton Cumberbatch, Mrs Patricia Edwards-Wescott, Mrs Haleema Ali-Sisbane and Mrs Kimoy Worrell for their support.
Funding Statement
Financial support for this study was provided by the International Development Research Centre. The sponsor did not influence in any way the design of the study, the data collection, the analysis or the writing of these results.
Footnotes
Authors’ contributions.
All authors contributed to conceiving and conceptualizing the original idea, designing the research, collecting and analyzing the data, interpreting the results, and writing and reviewing the research paper. All authors reviewed and approved the final version.
Conflicts of interest.
None declared.
Funding.
Financial support for this study was provided by the International Development Research Centre. The sponsor did not influence in any way the design of the study, the data collection, the analysis or the writing of these results.
REFERENCES
- 1.World Health Organization . Noncommunicable diseases. Geneva: World Health Organization; 2021. [cited 2022 Jan 13]. Internet. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases. [Google Scholar]; World Health Organization. Noncommunicable diseases [Internet]. Geneva: World Health Organization; 2021 [cited 2022 Jan 13]. Available from: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases
- 2.Pan American Health Organization . Noncommunicable diseases: key facts. Washington (DC): Pan American Health Organization; 2021. [cited 2022 Jan 20]. Internet. Available from: https://www.paho.org/en/topics/noncommunicable-diseases. [Google Scholar]; Pan American Health Organization. Noncommunicable diseases: key facts [Internet]. Washington (DC): Pan American Health Organization; 2021 [cited 2022 Jan 20]. Available from: https://www.paho.org/en/topics/noncommunicable-diseases
- 3.Ministry of Health and Wellness . Chronic non-communicable diseases: the Non-Communicable Disease and Injury Prevention Unit. Kingston: Ministry of Health and Wellness; 2021. [cited 2021 Aug 11]. Internet. Available from: https://www.moh.gov.jm/programmes-policies/chronic-non-communicable-diseases/ [Google Scholar]; Ministry of Health and Wellness. Chronic non-communicable diseases: the Non-Communicable Disease and Injury Prevention Unit [Internet]. Kingston: Ministry of Health and Wellness; 2021 [cited 2021 Aug 11]. Available from: https://www.moh.gov.jm/programmes-policies/chronic-non-communicable-diseases/
- 4.Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al. The global economic burden of noncommunicable diseases. Geneva: World Economic Forum; 2011. [Google Scholar]; Bloom DE, Cafiero ET, Jané-Llopis E, Abrahams-Gessel S, Bloom LR, Fathima S, et al. The global economic burden of noncommunicable diseases. Geneva: World Economic Forum; 2011.
- 5.Hodges P-G. NCDs must be seen as an economic problem – Dr. Tufton. Kingston: Jamaica Information Service; 2021. [cited 2022 Jan 24]. Internet. Available from: https://jis.gov.jm/ncds-must-be-seen-as-an-economic-problem-dr-tufton/ [Google Scholar]; Hodges P-G. NCDs must be seen as an economic problem – Dr. Tufton [Internet]. Kingston: Jamaica Information Service; 2021 [cited 2022 Jan 24]. Available from: https://jis.gov.jm/ncds-must-be-seen-as-an-economic-problem-dr-tufton/
- 6.Daniels ME, Jr., Donilon TE, Bollyky TJ, Tuttle CM. The emerging global health crisis: noncommunicable diseases in low- and middle-income countries. New York: Council on Foreign Relations; 2014. [Google Scholar]; Daniels ME Jr., Donilon TE, Bollyky TJ, Tuttle CM. The emerging global health crisis: noncommunicable diseases in low- and middle-income countries. New York: Council on Foreign Relations; 2014.
- 7.Marquez PV, La Foucade A, Theodore K, Gabriel S, Scott E, Laptiste C, et al. Trinidad and Tobago: tobacco taxation and impact of policy reforms. Washington (DC): World Bank Group; 2018. [Google Scholar]; Marquez PV, La Foucade A, Theodore K, Gabriel S, Scott E, Laptiste C, et al. Trinidad and Tobago: tobacco taxation and impact of policy reforms. Washington (DC): World Bank Group; 2018.
- 8.Etienne CF. Advancing the economics of noncommunicable diseases in the Americas. Rev Panam Salud Publica. 2018;42:e94. doi: 10.26633/RPSP.2018.94. [DOI] [PMC free article] [PubMed] [Google Scholar]; Etienne CF. Advancing the economics of noncommunicable diseases in the Americas. Rev Panam Salud Publica. 2018;42:e94. [DOI] [PMC free article] [PubMed]
- 9.La Foucade A, Metivier C, Gabriel S, Scott E, Theodore K, Laptiste C. The potential for using alcohol and tobacco taxes to fund prevention and control of noncommunicable diseases in Caribbean Community countries. Rev Panam Salud Publica. 2018;42:e192. doi: 10.26633/RPSP.2018.192. [DOI] [PMC free article] [PubMed] [Google Scholar]; La Foucade A, Metivier C, Gabriel S, Scott E, Theodore K, Laptiste C. The potential for using alcohol and tobacco taxes to fund prevention and control of noncommunicable diseases in Caribbean Community countries. Rev Panam Salud Publica. 2018;42:e192. [DOI] [PMC free article] [PubMed]
- 10.La Foucade A, Gabriel S, Scott E, Metivier C, Theodore K, Cumberbatch A, et al. Increased taxation on cigarettes in Grenada: potential effects on consumption and revenue. Rev Panam Salud Publica. 2018;42:e195. doi: 10.26633/RPSP.2018.195. [DOI] [PMC free article] [PubMed] [Google Scholar]; La Foucade A, Gabriel S, Scott E, Metivier C, Theodore K, Cumberbatch A, et al. Increased taxation on cigarettes in Grenada: potential effects on consumption and revenue. Rev Panam Salud Publica. 2018;42:e195. [DOI] [PMC free article] [PubMed]
- 11.Caprara G. Mediterranean-type dietary pattern and physical activity: the winning combination to counteract the rising burden of non-communicable diseases (NCDs) Nutrients. 2021;13:429. doi: 10.3390/nu13020429. [DOI] [PMC free article] [PubMed] [Google Scholar]; Caprara G. Mediterranean-type dietary pattern and physical activity: the winning combination to counteract the rising burden of non-communicable diseases (NCDs). Nutrients. 2021;13:429. [DOI] [PMC free article] [PubMed]
- 12.Wang DD, Li Y, Afshin A, Springmann M, Mozaffarian D, Stampfer MJ, et al. Global improvement in dietary quality could lead to substantial reduction in premature death. J Nutr. 2019;149:1065–1074. doi: 10.1093/jn/nxz010. [DOI] [PMC free article] [PubMed] [Google Scholar]; Wang DD, Li Y, Afshin A, Springmann M, Mozaffarian D, Stampfer MJ, et al. Global improvement in dietary quality could lead to substantial reduction in premature death. J Nutr. 2019;149:1065-74. [DOI] [PMC free article] [PubMed]
- 13.Lake AA, Hyland RM, Rugg-Gunn AJ, Wood CE, Mathers JC, Adamson AJ. Healthy eating: perceptions and practice (the ASH30 study) Appetite. 2007;48:176–182. doi: 10.1016/j.appet.2006.08.065. [DOI] [PubMed] [Google Scholar]; Lake AA, Hyland RM, Rugg-Gunn AJ, Wood CE, Mathers JC, Adamson AJ. Healthy eating: perceptions and practice (the ASH30 study). Appetite. 2007;48:176-82. [DOI] [PubMed]
- 14.Rodriguez-Sabate C, Morales I, Sanchez A, Rodriguez M. The multiple correspondence analysis method and brain functional connectivity: its application to the study of the non-linear relationships of motor cortex and basal ganglia. Front Neurosci. 2017;11:345. doi: 10.3389/fnins.2017.00345. [DOI] [PMC free article] [PubMed] [Google Scholar]; Rodriguez-Sabate C, Morales I, Sanchez A, Rodriguez M. The multiple correspondence analysis method and brain functional connectivity: its application to the study of the non-linear relationships of motor cortex and basal ganglia. Front Neurosci. 2017;11:345. [DOI] [PMC free article] [PubMed]
- 15.Pregibon D. Goodness of link tests for generalized linear models. Appl Stat. 1980;29(1):15–24. [Google Scholar]; Pregibon D. Goodness of link tests for generalized linear models. Appl Stat. 1980;29(1):15-24.
- 16.Pregibon D. Logistic regression diagnostics. Ann Stat. 1981;9(4):705–724. [Google Scholar]; Pregibon D. Logistic regression diagnostics. Ann Stat. 1981;9(4):705-24.
- 17.Long JS, Freese J. Regression models for categorical dependent variables using Stata. 3rd edition. College Station (TX): Stata; 2014. [Google Scholar]; Long JS, Freese J. Regression models for categorical dependent variables using Stata. 3rd edition. College Station (TX): Stata; 2014.
- 18.Boustani NM, Guiné RPF. Food choice motivations and perception of a healthy diet in a developing Mediterranean country. Open Agric. 2020;5:485–495. [Google Scholar]; Boustani NM, Guiné RPF. Food choice motivations and perception of a healthy diet in a developing Mediterranean country. Open Agric. 2020;5:485-95.
- 19.Bishow J, Blaylock J, Variyam JN. Matching perception and reality in our diets. Food Rev. 1998;202:16–20. [Google Scholar]; Bishow J, Blaylock J, Variyam JN. Matching perception and reality in our diets. Food Rev. 1998;202:16-20.
- 20.Sparks P, Shepherd R, Wieringa N, Zimmermanns N. Perceived behavioural control, unrealistic optimism and dietary change: an exploratory study. Appetite. 1995;24:243–255. doi: 10.1016/s0195-6663(95)99787-3. [DOI] [PubMed] [Google Scholar]; Sparks P, Shepherd R, Wieringa N, Zimmermanns N. Perceived behavioural control, unrealistic optimism and dietary change: an exploratory study. Appetite. 1995;24:243-55. [DOI] [PubMed]
- 21.Henry FJ, Eyre S, Caines D, Lawrence B. Obesity and food economics in the Caribbean. Nutr Food Technol Open Access. 2016;2:8–11. [Google Scholar]; Henry FJ, Eyre S, Caines D, Lawrence B. Obesity and food economics in the Caribbean. Nutr Food Technol Open Access. 2016;2:8-11.
- 22.Boca GD. Factors influencing consumer behavior in sustainable fruit and vegetable consumption in Maramures County, Romania. Sustainability. 2021;13(4):1812. [Google Scholar]; Boca GD. Factors influencing consumer behavior in sustainable fruit and vegetable consumption in Maramures County, Romania. Sustainability. 2021;13(4):1812.
- 23.Azizi Fard N, De Francisci Morales G, Mejova Y, Schifanella R. On the interplay between educational attainment and nutrition: a spatially-aware perspective. EPJ Data Sci. 2021;10:18. [Google Scholar]; Azizi Fard N, De Francisci Morales G, Mejova Y, Schifanella R. On the interplay between educational attainment and nutrition: a spatially-aware perspective. EPJ Data Sci. 2021;10:18.
- 24.Rippin HL, Hutchinson J, Greenwood DC, Jewell J, Breda JJ, Martin A, et al. Inequalities in education and national income are associated with poorer diet: pooled analysis of individual participant data across 12 European countries. PLoS One. 2020;15(5):e0232447. doi: 10.1371/journal.pone.0232447. [DOI] [PMC free article] [PubMed] [Google Scholar]; Rippin HL, Hutchinson J, Greenwood DC, Jewell J, Breda JJ, Martin A, et al. Inequalities in education and national income are associated with poorer diet: pooled analysis of individual participant data across 12 European countries. PLoS One. 2020;15(5):e0232447. [DOI] [PMC free article] [PubMed]
- 25.van Buul VJ, Bolman CAW, Brouns FJPH, Lechner L. Back-of-pack information in substitutive food choices: a process-tracking study in participants intending to eat healthy. Appetite. 2017;116:173–183. doi: 10.1016/j.appet.2017.04.036. [DOI] [PubMed] [Google Scholar]; van Buul VJ, Bolman CAW, Brouns FJPH, Lechner L. Back-of-pack information in substitutive food choices: a process-tracking study in participants intending to eat healthy. Appetite. 2017;116:173-83. [DOI] [PubMed]
- 26.Ferrão AC, Guiné RPF, Correia P, Ferreira M. Influence of environmental and political determinants on food choices in a sample of Portuguese population. Curr Nutr Food Sci. 2019;16:689–697. [Google Scholar]; Ferrão AC, Guiné RPF, Correia P, Ferreira M. Influence of environmental and political determinants on food choices in a sample of Portuguese population. Curr Nutr Food Sci. 2019;16:689-97.
- 27.Guiné R, Ferrão AC, Ferreira M, Correia P, Cardoso AP, Duarte J, et al. The motivations that define eating patterns in some Mediterranean countries. Nutr Food Sci. 2019;49:1126–1141. [Google Scholar]; Guiné R, Ferrão AC, Ferreira M, Correia P, Cardoso AP, Duarte J, et al. The motivations that define eating patterns in some Mediterranean countries. Nutr Food Sci. 2019;49:1126-41.
- 28.Harrington J, Fitzgerald AP, Layte R, Lutomski J, Molcho M, Perry IJ. Sociodemographic, health and lifestyle predictors of poor diets. Public Health Nutr. 2011;14:2166–2175. doi: 10.1017/S136898001100098X. [DOI] [PubMed] [Google Scholar]; Harrington J, Fitzgerald AP, Layte R, Lutomski J, Molcho M, Perry IJ. Sociodemographic, health and lifestyle predictors of poor diets. Public Health Nutr. 2011;14:2166-75. [DOI] [PubMed]
- 29.Mullie P, Clarys P, Hulens M, Vansant G. Dietary patterns and socioeconomic position. Eur J Clin Nutr. 2010;64:231–238. doi: 10.1038/ejcn.2009.145. [DOI] [PubMed] [Google Scholar]; Mullie P, Clarys P, Hulens M, Vansant G. Dietary patterns and socioeconomic position. Eur J Clin Nutr. 2010;64:231-8. [DOI] [PubMed]
- 30.Felker-Kantor E, Wood CH. Female-headed households and food insecurity in Brazil. Food Secur. 2012;4(4):607–617. [Google Scholar]; Felker-Kantor E, Wood CH. Female-headed households and food insecurity in Brazil. Food Secur. 2012;4(4):607-17.
- 31.Bärebring L, Palmqvist M, Winkvist A, Augustin H. Gender differences in perceived food healthiness and food avoidance in a Swedish population-based survey: a cross sectional study. Nutr J. 2020;19:140. doi: 10.1186/s12937-020-00659-0. [DOI] [PMC free article] [PubMed] [Google Scholar]; Bärebring L, Palmqvist M, Winkvist A, Augustin H. Gender differences in perceived food healthiness and food avoidance in a Swedish population-based survey: a cross sectional study. Nutr J. 2020;19:140. [DOI] [PMC free article] [PubMed]
- 32.Wolfson JA, Ishikawa Y, Hosokawa C, Janisch K, Massa J, Eisenberg DM. Gender differences in global estimates of cooking frequency prior to COVID-19. Appetite. 2021;161:105117. doi: 10.1016/j.appet.2021.105117. [DOI] [PMC free article] [PubMed] [Google Scholar]; Wolfson JA, Ishikawa Y, Hosokawa C, Janisch K, Massa J, Eisenberg DM. Gender differences in global estimates of cooking frequency prior to COVID-19. Appetite. 2021;161:105117. [DOI] [PMC free article] [PubMed]
- 33.Silveira B, Novaes J, Reis N, Lourenço L, Capobiano A, Leal A, et al. Sociodemographic and lifestyle factors are associated with diet quality in cardiometabolic risk subjects. J Food Nutr Res. 2019;7:141–147. [Google Scholar]; Silveira B, Novaes J, Reis N, Lourenço L, Capobiano A, Leal A, et al. Sociodemographic and lifestyle factors are associated with diet quality in cardiometabolic risk subjects. J Food Nutr Res. 2019;7:141-7.
- 34.Bawazeer NM, Al-Qahtani SJ, Alzaben AS. The association between dietary patterns and socio-demographic and lifestyle characteristics: a sample of Saudi Arabia. Curr Res Nutr Food Sci. 2021;9:1046–1057. [Google Scholar]; Bawazeer NM, Al-Qahtani SJ, Alzaben AS. The association between dietary patterns and socio-demographic and lifestyle characteristics: a sample of Saudi Arabia. Curr Res Nutr Food Sci. 2021;9:1046-57.