

Abstract
This report describes an intra-abdominal mass caused by progesterone-containing controlled internal drug release (CIDR) devices in the abdominal cavity of a 28-month-old Japanese Black heifer presenting with infertility. Rectal examination revealed a mass containing a cartilage-like object in the pelvic cavity. Computed tomography revealed a mass containing two T-shaped foreign bodies. Laparotomy was performed to remove the mass containing the foreign bodies. The heifer was healthy at discharge seven days post-surgery. This case adds CIDR device as a new etiology for intra-abdominal masses. Furthermore, it highlights the usefulness of CT in diagnosing deep abdominal lesions.
Keywords: computed tomography, controlled internal drug release (CIDR) device, heifer, intra-abdominal mass, small intestine
Cattle do not sort their feed fastidiously; this characteristic along with the peculiar structure of the ruminant forestomach predisposes them to foreign body lesions [14]. The most common foreign body disease is traumatic reticuloperitonitis (TRP). Although TRP incidence has decreased over the past decades, the recently reported incidence rate stands at 2–10% [6, 16, 17]. The leading cause of TRP is the ingestion of sharp metal objects, such as nails and wire fragments, that penetrate the secondary stomach wall [2, 9, 11, 13, 15]. These sharp objects can easily penetrate the tarpaulin covering the silage and accidentally get mixed in the feed. Rare incidents of alimentary tract perforation caused by tire wires or metal components of the mixer wagon have also been reported [6,7,8, 12]. The occurrence of gastrointestinal diseases caused by trichobezoars [1, 3] or non-magnetic foreign bodies, such as feeding nipples [5], is rare [9, 13, 18] and is reported to cause duodenal obstruction.
A controlled internal drug release (CIDR) device is an intravaginal device containing progesterone mainly used for estrus synchronization or treating reproductive disorders in cattle. The head of the CIDR device is T-shaped so that it verges into the vaginal wall, and the tail is connected to a wire protruding from the vagina that is used to remove it. Its structure is such that it does not easily fall from the vagina. In rare cases, animals might get interested in the protruding wire and might pull on it with the tongue or horn, or the device might spontaneously fall off.
This report highlights the fact that if an animal accidentally ingests a CIDR device, it can pass through the esophagus and rumen, reach the small intestine, and, in the worst-case scenario, perforate it, resulting in an intra-abdominal mass. In such case, Computed tomography (CT) is also helpful in investigating foreign bodies deep in the abdominal wall. This is the first report of CT preoperative diagnosis of jejunal perforation and the formation of an intra-abdominal mass secondary to a CIDR device in the abdominal cavity. Written informed consent was obtained from the owner for publication of this case report and the accompanying images.
A 28-month-old Japanese Black cow, weighing 438 kg, was referred to the Veterinary Teaching Hospital, University of Miyazaki, for infertility. A cartilage-like object was found around the uterus horns on rectal palpation. At admission to the hospital, the heifer presented with no abnormal activity or appetite. The heifer was fed in the pen and allowed free access to water at all times. The heart rate was 64 beats per minute, respiratory rate was 32 breaths per minute, and rectal temperature was 38.9°C.
The laboratory tests, including complete blood count and serum biochemical profile, were within the normal range. On rectal examination, there were soft feces in the rectum. Although no abnormality was palpated on the dorsal surface of the vagina and uterus, a mass (approximately 20 × 20 cm) was palpated between the cranioventral side of the cervix and the uterine horn. Both ovaries were adherent to the connective tissue around the mass, making it difficult to palpate the entire mass. However, the object, as wide as a calf rib with a cartilage-like texture, was palpated. The mass was not completely adhered to the uterus, and therefore, the uterus was movable. No abnormality was noted in the inner vaginal wall on vaginal examination.
Rectal ultrasonography (10.0-MHz linear probe, MyLab One VET, Esaote, Maastricht, the Netherlands) confirmed a foreign body of over 15 cm in length, with high echogenicity, under the uterine horn (Fig. 1). Ultrasonography (5.0-MHz convex probe, iViz air, FUJIFILM, Tokyo, Japan) through the right abdominal wall did not reveal dilation of the small intestine or colon.
Fig. 1.
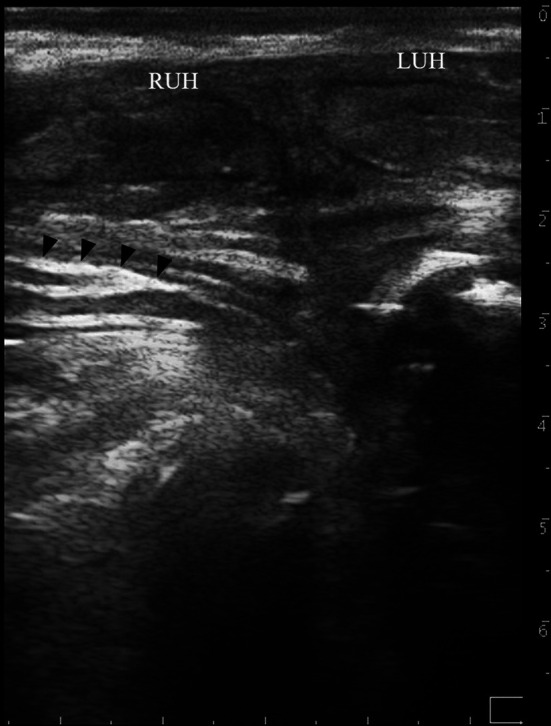
Transrectal horizontal ultrasonographic image of the uterus and foreign body. Ultrasonography (10.0 MHz linear probe) in a 28-month-old Japanese Black heifer revealed a mass extending from the cervical ventral side to the uterine horn. A line of high echogenicity (black arrowheads) is visible under the uterine horn. RUH, right uterus horn; LUH, left uterine horn.
CT was performed to obtain detailed information on the size, shape, and properties of the mass and foreign body. The heifer was sedated with an intravenous injection of 2% xylazine hydrochloride (0.2 mg/kg, Selactar, Bayer, Tokyo, Japan). An endotracheal tube was inserted, and anesthesia was maintained with isoflurane (Isoflurane, Pfizer, Tokyo, Japan) in oxygen. The heifer was then restrained in the right recumbent position and underwent scanning using a 16-detector row helical CT unit (Aquilion LB, Canon Medical Systems Corp., Ohtawara, Japan). A CT examination revealed a mass between the cranioventral side of the cervix and the right uterine horn. While the boundary of the mass was not clear and the size could not be confirmed, two cartilage-like, T-shaped foreign bodies at different angles were observed around the mass (Fig. 2). The CT values of the mass were −62.1 ± 22.8 Hounsfield units (HU) (ROI=500 mm2) and −93.3 ± 29.0 HU (ROI=528 mm2), which suggested fat-containing tissue, and 60.0 ± 28.2 HU (ROI=1,056 mm2) and 45.9 ± 35.2 HU (ROI=1,056 mm2), which suggested soft-tissue. The CT value of the foreign bodies was approximately 100 HU. Although it was not possible to determine the nature of the mass from the CT values, the shape on the CT images and the absence of a CIDR devices inserted into the vagina of the cow and her cohabitant strongly suggested that the foreign bodies were CIDR devices.
Fig. 2.

Reconstructed computed tomography images of the two intra-abdominal foreign bodies. The T-shaped, cartilage-like foreign body is seen around the mass (white arrowheads). Each foreign body is shown in a different cross-section for easy recognition. One is shown in the sagittal plane (A) and the other in the coronal plane (B). Cr, cranial; Cd, caudal.
Laparotomy was performed to remove the mass and foreign bodies from the abdominal cavity. The heifer fasted for 36 hr before the surgery. An intramuscular injection of a compound drug containing 200,000 units of benzylpenicillin procaine and 250 mg of dihydrostreptomycin sulfate (0.05 mL/kg, Mycillin Sol, Meiji-Seika Pharma, Tokyo, Japan) was administered to prevent perioperative infection. Flunixin meglumine (2 mg/kg, Forvet50, MSD, Tokyo, Japan) was given for pain relief. The general anesthesia procedure was the same as described above. Prior CT had shown a foreign body at the right ventral side of the uterus horn, the heifer was placed in the left lateral recumbent position. Local anesthesia with 2% lidocaine hydrochloride (20 mL, Xylocaine, Aspen Japan, Tokyo, Japan) was administered subcutaneously around the right flank area. A 20 cm long incision was made on the skin of the right flank, and the abdominal cavity was exposed. A blue vessel-like structure was visible in the abdominal cavity underneath the peritoneum (Fig. 3A). Detailed exploration of the abdominal cavity was performed, and no signs of peritonitis were noted. Delineation of the entire mass was nearly impossible due to its adherence to the ovary and surrounding pelvic tissues, making it challenging to perform an en-bloc resection. The blue blood vessel-like structure in the intra-abdominal cavity turned out to be the tail wire of the CIDR device (CIDR tail). The T-shaped CIDR device head (CIDR head) was embedded in the connective tissue surrounding the mass. The CIDR head was carefully peeled from the connective tissue and removed. In addition, another CIDR device was palpated between the mass and the surrounding connective tissue (Fig. 3B). When the mass was pulled close to the incision, the jejunum and mesentery were found to be adherent to the mass, and the CIDR head appeared to be inside the adherent jejunum. The straight part of the CIDR body had perforated the intestinal wall and was surrounded by the mesentery. The CIDR tail penetrated through the mesentery into the ventral uterine mass. The adherent mass and jejunum were separated using a vessel sealing device (LigaSure™ Smart Jaw; Medtronic, Dublin, Ireland). A white pus-like fluid appeared at the pore when the CIDR tail was pulled out from the mass. A 7 French (Fr) tube was inserted into the pore, and the fluid was aspirated. The intra-abdominal mass was then washed with a warm normal saline solution mixed with Mycillin solution. The pore was subsequently sealed with LigaSure to prevent leakage of the contents. The collected fluid was cultured aerobically and anaerobically using conventional methods, but no bacterial growth was observed. A part of the jejunum was incised to remove the CIDR device from the intestinal cavity (Fig. 4). The jejunum incision was closed with polydioxanone synthetic absorbable monofilament suture material (USP 2–0, PDS, Johnson & Johnson, Tokyo, Japan) in two layers of simple sutures, following the Lembert suture pattern. After washing the intestinal surface and the abdominal cavity with a warm normal saline solution, the peritoneum, and muscular layer were closed using synthetic, absorbable, multifilament polyglycolic acid suture material (USP 3+4, Opepolyx, Alfresa Pharma, Osaka, Japan) in a continuous suture pattern. The subcutaneous tissue was closed with continuous sutures using polyglactin 910, synthetic absorbable multifilament suture material (USP 0, Vicryl, Johnson & Johnson). The skin incision was closed with intradermal buried sutures using the same suture thread used for the subcutaneous tissue. Postoperatively, the heifer was administered cefazolin sodium (4 mg/kg, Cefazolin-Chu, Fujita Pharmaceutical, Tokyo, Japan) and flunixin meglumine intravenously for four days. Feed was withheld for approximately 24 hr postoperatively, and it gradually increased after that. Appetite and vigor steadily improved, and the heifer was discharged 7 days after the surgery. Currently, the heifer is in good general condition and became pregnant three months after surgery.
Fig. 3.

Intraoperative views of the right flank area. When the right flank area incised and the peritoneum was exposed, a blood vessel-like structure was visualized in the abdominal cavity behind the peritoneum (A; arrowheads). This was the tail wire part of a controlled internal drug release (CIDR) device. When the mass was pulled closer to the incision site, the small intestine and mesentery were found to be adherent to it, and the head of a second CIDR device was inside the adherent jejunum (B; dotted line). Dr, dorsal; Vt, ventral; Cr, cranial; Cd, caudal.
Fig. 4.
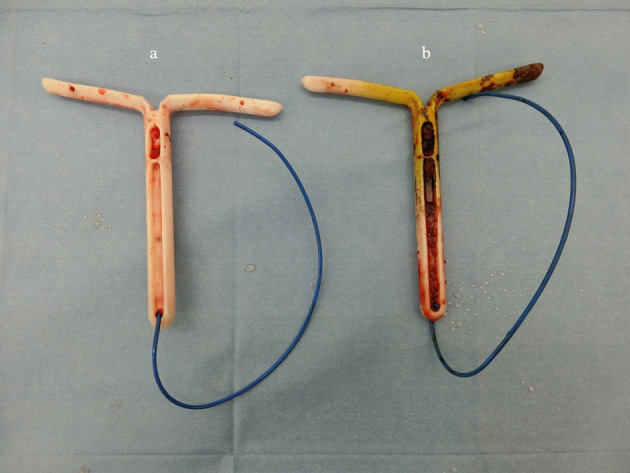
The controlled internal drug release (CIDR) devices removed from the heifer. The CIDR devices after removal from the abdominal cavity (a) and jejunum (b).
This case is different from previously reported cases in terms of clinical symptoms and laboratory findings of foreign body disease [1,3,4,5,6,7, 15] because there was no colic, anorexia, fever, weight loss, or markedly diminished fecal output. Moreover, dilated intestinal loops were absent on transrectal palpation. In cases of abomasal or proximal jejunum obstruction, blood tests reveal findings suggestive of regurgitation of the abomasal contents [3, 4, 10]; however, no hematological abnormalities were observed in the present case. We suspect that typical clinical symptoms were absent in this case because of the shape of the CIDR device. It did not completely obstruct the gastrointestinal tract, allowing the contents to pass normally. Furthermore, it is assumed that the injury was insufficient to impair the small intestine motility.
We suspect that inflammation and granuloma were the host animal’s normal reactions to the presence of foreign bodies, ultimately resulting in the formation of a mass in the abdominal cavity. The CT findings strongly support this theory as the CT value of the foreign bodies was consistent with that of cartilage or mild calcification. There were severe adhesions around the uterine horns and ovaries, and it is unclear whether this was the cause of infertility, but since the patient became pregnant after the CIDR devices was removed, the CIDR devices was likely the cause of infertility.
There have been no previous reports of accidental ingestion of CIDR devices. In this case, 2 weeks after CIDR device insertion, 2 heifers’ CIDR devices could not be seen in their vaginas. CT scan showed two Y-shaped foreign bodies like CIDR devices in one of the cow’s abdominal cavity, and laparotomy was performed based on this information, which revealed two CIDR devices in the abdominal cavity as per preoperative diagnosis. The exact route by which the CIDR devices had entered the abdominal cavity is unknown, although oral ingestion is considered likely, based on the condition of the vaginal wall by the internal examination, and the surrounding female genitalia at the time of laparotomy.
This case report shows that despite its T-shaped head, if one or more CIDR devices are accidentally ingested by such a large animal, the device(s) might pass through the esophagus and rumen, subsequently reaching the small intestine, where the CIDR device could perforate the intestinal wall leading to possible abdominal mass formation and other gastrointestinal disorders.
Currently, CT examination of cattle has several challenges, such as difficulty in transportation, economic constraints, and the need for general anesthesia. However, CT can reveal intricate details of foreign bodies and masses embedded deep in the abdominal cavity that are difficult to examine by conventional radiography or ultrasonography. Therefore, if a cow is suspected of ingesting a foreign body like a CIDR device, CT can help with diagnosis, select optimal treatment, and assess the risks involved in surgical intervention.
CONFLICT OF INTEREST
The authors declare that they have no competing interests.
Acknowledgments
The authors wish to acknowledge Dr. Yoshihiko OGATA for his support for treatment after discharge. We thank the staff and student assistants at the University of Miyazaki for caring for the heifer during operation and hospitalization.
REFERENCES
- 1.Abutarbush SM, Radostits OM. 2004. Obstruction of the small intestine caused by a hairball in 2 young beef calves. Can Vet J 45: 324–325. [PMC free article] [PubMed] [Google Scholar]
- 2.Andersen G, Gillund P. 1980. Traumatic indigestion among slaughter cattle: its occurrence and pathological effects. Norsk Vet 92: 93–97. [Google Scholar]
- 3.Anderson DE, Ewoldt JM. 2005. Intestinal surgery of adult cattle. Vet Clin North Am Food Anim Pract 21: 133–154. doi: 10.1016/j.cvfa.2004.12.010 [DOI] [PubMed] [Google Scholar]
- 4.Braun U, Steiner A, Götz M. 1993. Clinical signs, diagnosis and treatment of duodenal ileus in cattle. Schweiz Arch Tierheilkd 135: 345–355. [PubMed] [Google Scholar]
- 5.Braun U, Schnetzler C, Previtali M, Gerspach C, Schmid T. 2011. Duodenal ileus caused by a calf feeding nipple in a cow. BMC Vet Res 7: 2. doi: 10.1186/1746-6148-7-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cramers T, Mikkelsen KB, Andersen P, Enevoldsen C, Jensen HE. 2005. New types of foreign bodies and the effect of magnets in traumatic reticulitis in cows. Vet Rec 157: 287–289. doi: 10.1136/vr.157.10.287 [DOI] [PubMed] [Google Scholar]
- 7.Daniel R, Smith G. 2008. Suspected bovine reticuloperitonitis associated with the metal components of a mixer wagon. Vet Rec 162: 563–564. doi: 10.1136/vr.162.17.563-a [DOI] [PubMed] [Google Scholar]
- 8.Harwood D. 2004. Alimentary tract perforation in cattle caused by tyre wire. Vet Rec 154: 574–575. [PubMed] [Google Scholar]
- 9.Jagos P. 1969. The characteristics of foreign bodies in traumatic inflammations of cattle. Acta Vet Brno 38: 545–552. [Google Scholar]
- 10.Lejeune B, Lorenz I. 2008. Ultrasonographic findings in 2 cows with duodenal obstruction. Can Vet J 49: 386–388. [PMC free article] [PubMed] [Google Scholar]
- 11.Maddy KT. 1954. Incidence of perforation of the bovine reticulum. J Am Vet Med Assoc 124: 113–115. [PubMed] [Google Scholar]
- 12.Monies B. 2004. Alimentary tract perforation in cattle caused by tyre wire. Vet Rec 154: 735. [PubMed] [Google Scholar]
- 13.Neumann N. 1979. Untersuchungen über das Vorkommen von Netzmagen-Fremdkörpern bei Schlachtrindern in Bayern. Dr Med Vet Thesis. pp 1–120. University of Munich, German (in German).
- 14.Poulsen JS. 1976. Prevention of traumatic indigestion in cattle. Vet Rec 98: 149–151. doi: 10.1136/vr.98.8.149 [DOI] [PubMed] [Google Scholar]
- 15.Roth L, King JM. 1991. Traumatic reticulitis in cattle: a review of 60 fatal cases. J Vet Diagn Invest 3: 52–54. doi: 10.1177/104063879100300111 [DOI] [PubMed] [Google Scholar]
- 16.Starke A, Rehage J. 2000. Diagnose und Therapie bei abszedierender Reticuloperitonitis traumatica. Tierarztl Prax 28: 93–95. [Google Scholar]
- 17.Waldner CL, Kennedy RI, Rosengren L, Clark EG. 2009. A field study of culling and mortality in beef cows from western Canada. Can Vet J 50: 491–499. [PMC free article] [PubMed] [Google Scholar]
- 18.Warislohner S. 2017. Reticuloperitonitis traumatica beim Rind-eine Analyse von 503 Krankengeschichten. Dr Med Vet Thesis. University of Zurich, Switzerland (in German).