

Abstract
This paper investigates the effects of prenatal exposure to extreme temperatures on birth outcomes—specifically, the log of birth weight and an indicator for low birth weight—using a nationally representative dataset in rural China. During the span of our data (i.e., 1991–2000), indoor air-conditioning was not widely available and migration was limited, allowing us to address identification issues endemic in the climate change literature related to adaptation and location sorting. We find substantial heterogeneity in the effects of extreme temperature exposure on birth outcomes. In particular, prenatal exposure to heat waves has stronger negative effects than exposure to cold spells on survivors.
Keywords: Climate change, Cold weather, Heat waves, Birth weight, Low birth weight, China
JEL Codes: I15, Q54, Q51
1. Introduction
Climate change has induced more frequent yet largely unpredictable extreme weather events, such as days of extreme temperatures (heat waves and polar vortices), precipitation (flooding and drought), and windstorm variation (hurricanes) (IPCC 2014). In response to the increasing number of extreme weather events, there is a growing body of literature examining the impact of exposure to these events at various stages of the lifecycle.1 In particular, in utero exposure to extreme temperatures has been shown to affect birth outcomes (Deschênes, Greenstone and Guryan 2009; Andalon et al. 2016; Ha et al. 2017), as well as adult welfare outcomes, including educational attainments (Hu and Li 2019), disabilities (Wilde et al. 2017), annual earnings (Isen, Rossin-Slater and Walker 2017), and depression symptoms (Adhvaryu et al. 2017).
In this paper, we investigate the effects of prenatal exposure to extreme temperatures on birth outcomes – specifically, birth weight and the incidence of low birth weight (LBW) – using a large representative dataset in rural China. Our paper contributes to the literature in several dimensions.
First, our paper adds to the emerging literature in epidemiology that examines the impact of prenatal exposure to ambient temperature on birth outcomes; see, the important recent survey by Strand, Barbett and Tong (2011), by introducing new evidence in the important context of China (the largest developing country). Strand et al. (2011) surveys eight studies that examine the impact of early extreme temperature exposure on birth weight, but only one of these studies is in a developing country context (i.e., Elter et al. (2004) in the context of Turkey).
Further, because the administrative records from which our data is drawn cover a wide range of regions in China, a geographically expansive nation with varying climatic conditions, we are also able to explore the potential nonlinear effects of in utero exposure to extreme temperatures on birth outcomes. While some recent studies in the literature have simultaneously investigated the effects of exposure to both ends of the temperature extremes (e.g., Isen, Rossin-Slater and Walker 2017; Ha et al. 2017; Wilde et al. 2017; Deschênes, Greenstone and Guryan 2009; Barreca, Deschênes and Guldi 2018; Karlsson and Ziebarth 2018), almost all of these studies are in the context of developed nations. An important exception is Elter et al. (2004) who consider the impact of outdoor ambient temperatures in summer and winter on birth weight in the context of Turkey. The authors find that cold exposure during the middle trimester is associated with LBW. However, Elter et al. (2004)’s sample is relatively small (N = 3333) and there are concerns over insufficient power to detect small effects due to hot temperatures.
Importantly, information on gestational age in our data also allows us to examine, following the seminal work by Deschênes, Greenstone and Guryan (2009), the number of days within each trimester of the gestation period during which a woman is exposed to either extreme cold or hot weather. Hence, like Deschênes, Greenstone and Guryan (2009), our work allows for a finer treatment variable that more precisely targets the birth effects of gestational exposure to extreme temperatures.
Investigating the effects from both ends of the temperature extremes is important since there has been a lack of consensus on the relative importance of cold versus hot temperature exposure in the absence of mitigation. While there is a large body of literature evaluating the health burden of heat waves as the shift of temperature distribution makes extreme heat events more frequent, severe, and long-lasting (Bobb et al. 2014; CDC 2018; Gasparrini et al. 2015; Gosling et al. 2009; Isen, Rossin-Slater and Walker 2017; Carolan-Olah and Frankowska 2014; Adhvaryu et al. 2017), cold spells are recently found to cause more deaths (Seltenrich 2015). The different mechanisms through which cold spells and heat waves may affect human health have also been of interest (Seltenrich 2015).
Second, importantly, we focus on a rural sample in order to exploit the institutional aspects that are unique to the Chinese context to circumvent the identification challenges in isolating the biological effects of temperature extremes. Our clean study context makes sure that the adaptation/mitigation effect is largely absent.2 For example, indoor air-conditioning (AC) can be used as an ex post strategy to cope with hot weather. Barreca et al. (2016) find in the U.S. context that, from 1960 onward, there was a 70% decline in the mortality impact of days with mean temperatures exceeding 80 °F, virtually all of which could be explained by the diffusion of residential AC. The diffusion of AC was not a concern in our sample period 1991–2000 since the number of AC units per 100 households in rural China was minimal (only around 1.32 even by the end of 2000 according to China Statistical Yearbook 2001).
Another potentially serious threat to identification is ex ante residential sorting. If concerned pregnant mothers migrate to regions with less frequent extreme temperatures for the sake of their offspring’s health, then we cannot confidently tell whether our findings on birth outcomes reflect differences in the unobserved characteristics of pregnant mothers in our treatment and control groups or the direct impact of in utero temperature exposure. However, the average rural pregnant mother’s ability to engage in residential sorting was severely restricted in China by the residential registry (hukou) system since the 1960s. Massive migration did not take off until 1997 (Meng 2012).3
The hukou restrictions imposed not only strong direct restrictions on the ability of pregnant rural mothers to migrate but also to access healthcare systems outside of their hukou. Residents with rural hukou living in urban areas during the sample period were not entitled to the health care enjoyed by their urban counterparts. Most migrants thus chose to give birth in their hometowns as they could not afford to pay for child delivery in urban hospitals.4
Based on the matched dataset of birth records and daily prenatal temperature exposure, we find that heat waves are associated with a decrease in birth weight. Spending an additional day in the gestation period with a temperature above 28 °C, relative to a day in the 0–4 °C range, leads to a reduction in birth weight by 0.050 percent (1.66 grams), which accounts for 2.36% of the gender gap and 2.16% of the educational gap in birth weight. Similarly, exposure to an additional hot day above 28 °C during gestation increases the probability of LBW by 0.035 percentage points (1.05 percent of the mean incidence of LBW in the sample), which accounts for 3.18% of the gender gap and 2.30% of the education gap in the rate of LBW.5 However, we find no significantly detrimental effect on birth weight for survived newborns who are exposed to extremely cold days in utero. The latter is consistent with the literature suggesting that indoor heating reduces adverse health effects, including winter mortality (Chirakijja, Jayachandran and Ong 2019; Iparraguirre 2015).6
In the 1980s, the population-weighted total number of days with a mean temperature above 28 °C was 233 days, which rapidly increased to 261 days in our sample during the 1990s. Our estimates indicate that 28 additional such hot days may have caused 1.4 percent (46.5 grams) additional damage to birth weight a decade later.7 Put in perspective, based on findings in the literature, this estimated impact of extreme heat exposure in utero on birth weight would lead, in expectation, to about a 0.080 centimeter decrease in height, a 0.126 percentage point decrease in the probability of high school completion, a 0.126% decrease in earnings (Black, Devereux and Salvanes 2009), a 0.007 standard deviation reduction in mathematics scores (Figlio et al. 2014), and a 0.146% decline in permanent income (Bharadwaj, Lundbord and Rooth 2017). However, these long-term projections should be interpreted with caution as they may not be quantitatively accurate or appropriate given different contexts.
Finally, our paper also contributes to several other strains of work in the health and development literature. Our emphasis on in utero exposure to environmental stressors on birth outcomes relates to work on Barker (1992)’s “fetal origins hypothesis” (e.g., Almond and Currie 2011). This literature suggests that early exposure to stressors such as malnutrition (Meng and Qian 2009; Tan, Tan and Zhang 2015), family income shocks (Adhvaryu et al. 2017), and maternal stress (Persson and Ross-Slater 2014) have both short- and long-term effects on offspring. More broadly, our work relates to the new family investment models developed by Heckman and coauthors (Cunha, Heckman and Schennach 2010; Heckman and Mosso 2014) that examine parental investment responses to initial child disadvantages. These models emphasize the importance of reinforcing and compensatory responses to the perpetuation of initial shocks on future outcomes.
The rest of the paper is organized as follows. We describe our data and empirical methodology in sections 2 and 3, respectively. We present our baseline and robustness results in section 4. Section 5 concludes.
2. Data
The birth record data are collected by China’s National Disease Surveillance Points (DSP) system, which includes 145 counties in 31 provinces (autonomous regions and municipalities), using multistage cluster probability sampling to cover a 1% nationally representative sample of the Chinese population (Yang et al. 2005). The data contain demographic information on the child, including the exact date and county of birth, sex, birth weight, birth order, and gestational week.8 The data also provide demographic information on the parents, including their age at the birth of the child, ethnicity, education, and occupation. Table A1 presents summary statistics for these key characteristics in our analytical sample.
We focus primarily on the 864,757 live singleton births during 1991–2000 in rural areas of 31 Chinese provinces. Due to there being 174,424 missing values for birth weight and 53,300 missing values for other household demographics, the final dataset includes 637,033 live singleton births.9 We interpolate the missing gestational age by 39 weeks in the analysis. From the gestational age we infer the date of “conception” and measure the three trimesters of the pregnancy relative to that date.10 Specifically, we assign weeks 1–13 after conception to trimester 1, weeks 14–26 to trimester 2, and weeks 27–39 to trimester 3.11 As a robustness check below, we also report results for the subset of observations with gestational age values.12
The weather data are provided by the China National Meteorological Data Service Center (CMDC) under the National Meteorological Information Center of China. It contains consecutive daily weather records of 824 monitoring stations along with their longitudes and latitudes in China. The key variable for our analysis is the daily mean temperature. The dataset also provides a rich set of climate controls, such as precipitation, wind speed, sunshine duration and relative humidity.
To merge the birth data with the weather data, we calculate the average values of all the monitoring stations within 60 km to the centroid of each DSP county weighted by the inverse of the distance between the monitoring stations and the county centroid. When a county has no stations within 60 km, we match the county to the nearest station within 100 km.13
Figure 1 displays the spatial distribution of DSPs and weather stations. The weather stations are evenly distributed in China and could be well matched with the DSPs. We construct the number of days for which the daily mean temperature falls into one of 10 temperature bins, i.e., <−4 °C, −4–0 °C, 0–4 °C, 4–8 °C, 8–12 °C, 12–16 °C, 16–20 °C, 20–24 °C, 24–28 °C, and >28 °C during the 39 gestational weeks in our sample.14 Figure 2 depicts the distribution of daily mean temperature during the gestation period newborns in our sample are exposed. The vertical axis represents the average number of days that an expectant mother spends in each temperature bin while pregnant. The average number of days is 19.5 for the 0–4 °C range, 9.8 for the below −4 °C bin, and 19.0 for the above 28 °C bin. In the subsequent analysis, the number of days in each temperature bin is calculated separately for each trimester of the gestation period to allow for substantial flexibility and nonlinear relationships between birth outcomes and temperature exposure.
Figure 1: Distribution of DSPs and monitoring stations.
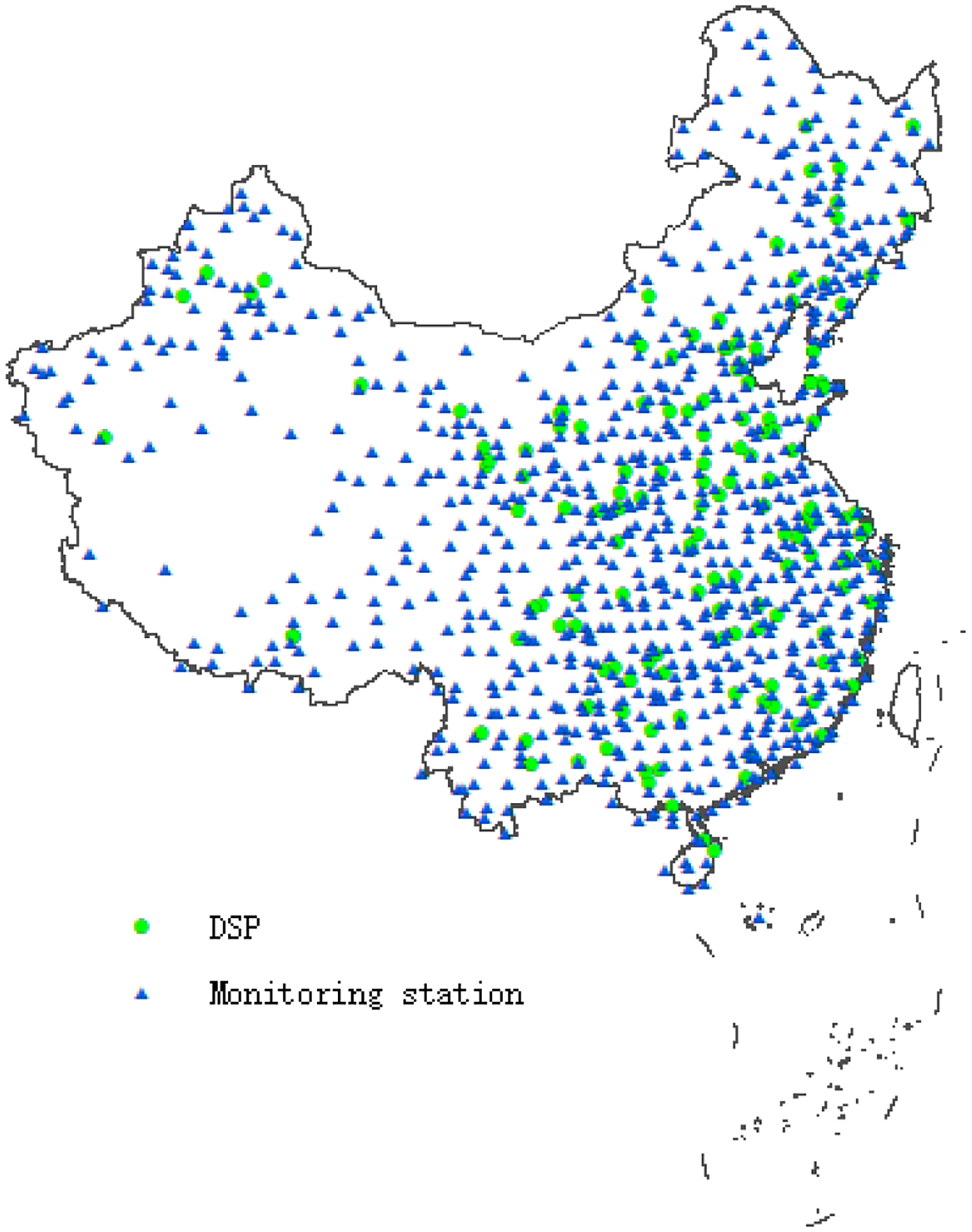
Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: This figure is plotted using ArcMap 10.5.1.
Figure 2: Distribution of daily mean temperature exposure during the gestation period.

Source: China Meteorological Data Service Center.
3. Empirical strategy
Our baseline econometric specification is as follows:
| (1) |
where the dependent variable Yicyd is the birth outcome of child i conceived in county c on day d (1–366) of year y. The two birth outcomes we test for this paper are log form of birth weight15 and an indicator for LBW (i.e., less than 2,500 grams). The key variables of interest TEMPcydj are the number of days in the temperature bin j (from 1 to 10) during the 39 weeks after the conception for child i conceived in county c on day d of year y. We set the 0–4 °C temperature bin as the reference group in all the exercises. The vector Xicyd contains a set of demographic variables, including the child’s gender, birth order, maternal age and its square, and dummies for the maternal education. We also control for a vector of rich weather conditions Wcyd, involving the mean precipitation, wind speed, sunshine duration and relative humidity measured at the gestation period level. Finally, we control for county specific seasonality by including county × day of conception year fixed effect (δcd), and county level time trends (e.g., driven by economic growth over this period) by including county × linear conception year time trend (trendcy) and conception year fixed effects (ηy). εicyd is the error term.16
Furthermore, the model could be refined to estimate the effects of exposure by individual pregnancy trimester:
| (2) |
where TR1, TR2, and TR3 are the indicators for the first, second, and third trimesters during the pregnancy. This specification allows us to test whether the estimated effects are driven by particular periods of pregnancy, such as the first trimester, when the fetus may be more sensitive to environmental insults.
By conditioning on the full set of fixed effects listed above, the key parameters are identified by comparing children conceived in the same county on the same day in different years after excluding county-specific shocks across years. Due to the unpredictability of temperature fluctuations, it is reasonable to assume that this variation is orthogonal to the unobserved determinants of birth outcomes. We also ran parsimonious specifications by dropping the set of demographic controls.17 If temperature fluctuations are random, then our treatment variables should be orthogonal to confounders and hence our regression estimates should be consistent. The inclusion of covariates should serve to improve the efficiency of the estimators, but we would expect then the point estimates from the parsimonious exercises to be similar to those from our benchmark exercises. We do, in fact, find that this is the case.
4. Results
4.1. Baseline results
Throughout this section, our main estimation results are visually represented in Figures 3 and 4, while the full numerical results are presented in Tables A2 and A3.
Figure 3: Estimated impacts of temperature on birth outcomes during the gestation period.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: The figure plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin identified from the regressions in Columns (2) and (4) of Table A2. Panels A and B correspond to the two birth outcomes, log birth weight and LBW (i.e., <2,500 grams), respectively. The reference temperature bin is 0–4°C. All the coefficients are scaled by 100 to make them more readable. All regressions include county × day of conception year fixed effects, county × linear conception year time trend, and conception year fixed effects. Demographic controls include gender, birth order, maternal age and its square, and dummies for maternal education. Environmental controls include mean precipitation, mean wind speed, mean sunshine duration and mean humidity during the gestation period in square polynomial forms.
Figure 4: Estimated impacts of temperature on birth outcomes in each trimester.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: The figure plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin in each trimester from the regressions in Table A3. Panels A and B correspond to the two birth outcomes, log birth weight and LBW (i.e., <2,500 grams), respectively. The reference temperature bin is 0–24°C. All the coefficients are scaled by 100 to make them more readable. All regressions include county × day of conception year fixed effects, county × linear conception year time trend, and conception year fixed effects. Demographic controls include gender, birth order, maternal age and its square, and dummies for maternal education. Environmental controls include mean precipitation, mean wind speed, mean sunshine duration and mean humidity in each trimester in square polynomial forms.
Our baseline findings are presented in Figure 3, which plots the estimates associated with each temperature bin (TEMPcydj) in equation (1) for the two birth outcomes. Specifically, Panels A and B in Figure 3 provide estimated impacts for log birth weight and LBW, respectively. The reference temperature bin is the 0–4 °C bin. Hence, the plotted coefficients can be interpreted as the estimated effects of an additional day in the corresponding temperature bin during the gestation period on birth outcomes relative to the reference temperature category. The 90 and 95 percent confidence intervals are included in all the panels in Figure 3.
We now turn to a discussion of our main findings. Panel A of Figure 3 indicates a non-linear relationship between log birth weight and temperature, where a high temperature decreases birth weight. Specifically, an additional gestational day with a mean temperature above 28 °C, relative to a day in the 0–4 °C range, is associated with a reduction in the birth weight by 0.050 percent (1.66 grams).18 The economic size of this estimate is small but largely consistent with previous literature.19
Panel B of Figure 3 plots the estimated coefficients for LBW. As displayed in Panel B of Figure 3, exposure to an additional hot day above 28 °C statistically significantly (at the 5% level) increased the probability of LBW by 0.035 percentage points (1.05 percent of the mean incidence of LBW in the sample).20 Because having a LBW may indicate a preterm birth or intrauterine growth restriction (i.e., being smaller than the norm given the gestational age), we also examine the impact of exposure to extreme temperatures on small for gestational age (SGA),21 preterm,22 and gestational age in Columns (7) through (9) in Table A2. We do not find a strong effect of exposure to heat waves on these three outcomes.
We also test the statistical differences between coefficients on hot days versus other temperature bins for log birth weight and LBW, respectively. The differences between the hot temperature bin (>28 °C) and other temperature bins (i.e. <−4 °C, −4–0 °C, 4–8 °C, 8–12 °C, 12–16 °C, 16–20 °C, 20–24 °C, 24–28 °C) are all significant at the 10% level or even the 1% level. All these test results suggest larger damage to birth weight is associated with exposure to heat waves as compared to cold temperatures.
Finally, we examine if the timing of exposure to extreme temperatures during pregnancy has any heterogeneous effects across trimesters. Figure 4 shows the estimated coefficients associated with each temperature bin by trimester for log birth weight and LBW, respectively. As indicated by our previous analysis, the marginal effects of temperature bins are constant across the range 0–24 °C. Thus, we estimate a specification that aggregates exposure into five temperature bins (<−4 °C, −4–0 °C, 0–24 °C, 24–28 °C, and >28 °C) with the 0–24 °C as the reference group. We find similar effects in Figure 4 as we do in our benchmark case above (Figure 3) across the three trimesters for all birth outcomes. For log birth weight, the point estimates suggest that exposure to extreme hot weather (above 28 °C) leads to a statistically significant damage in the first and third trimesters, with exposure of heat waves in the third trimester resulting in the largest negative impact. However, there are no significant differences in effects of extreme hot temperatures across trimesters as revealed by Wald test results. For LBW, the effects of hot days (above 28 °C) are distinguished between trimester 2 and trimester 3 at the 10% significance level.
4.2. Placebo tests and robustness checks
As is standard in the literature, we conduct placebo tests to further support our identifying assumptions. The placebo tests assign false treatments; i.e., temperature exposure three trimesters (39 weeks) before the conception date and three trimesters (39 weeks) after the birth date, to observational units. Figure 5 presents the results for log birth weight (Panel A) and LBW (Panel B), respectively. Specifically, the left part of each panel plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin when matching temperature exposure in trimesters before conception. The right part is drawn based on the estimates after birth. The middle part replicates the baseline results for ease of comparison.
Figure 5: Placebo tests - Estimated impacts of temperature before conception and after birth.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: We match temperature exposure in three trimesters (39 weeks) before conception and after birth with birth outcomes to conduct these placebo tests. Specifically, the left part of each panel plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin when matching temperature exposure in trimesters before conception. The right part is drawn based on the estimates after birth. The middle part replicates the baseline results for ease of comparison. Panels A and B correspond to the two birth outcomes, log birth weight and LBW (i.e., <2,500 grams), respectively. The reference temperature bin is 0–24°C. All the coefficients are scaled by 100 to make them more readable. Other covariates and fixed effects are the same as those in Figure 3.
Neither pre-conception exposure nor postnatal exposure to extreme temperatures should affect log birth weight or LBW, unless the identified effect is driven by unobserved confounding factors or trends. In line with our expectations, the results from the placebo tests show that temperature exposure before conception and after birth do not have any significant effects on birth outcomes, and the magnitude of the coefficients are also small. Overall, the placebo tests lend us support that our empirical strategy is effective in identifying the causal impact of extreme temperature exposure on birth outcomes.23
Our baseline results are also robust to a wide variety of specification checks. Columns (1) through (4) of Table A4 indicate that the results are robust to controlling for different sets of fixed effects; including, county × conception month fixed effects or county × day of conception year × sex fixed effects instead of county × day of conception year fixed effects. Columns (5) through (6) show that migration is unlikely to significantly bias our estimates. Furthermore, while we use forward counting to match the temperature exposure in the baseline results, Columns (7) through (8) show that the results are qualitatively unchanged if we use backward counting instead as per Currie and Rossin-Slater (2013).
In addition, Column (9) of Table A4 also shows our results are still robust if we remove observations at 3,000 and 3,500 grams to address the heaping issues in birth weight (Figure A2). Finally, we also define the temperature bins using “feels like” temperatures, which take into account wind speeds, atmosphere pressure and relative humidity to assess how the human body actually feels temperature (Steadman 1984). As indicated by Figure A3, our main findings remain unchanged.
4.3. Heterogeneous effects
We explore possible heterogeneity in the effects of temperature exposure on birth weight across gender, geographic region, and socioeconomic status (SES) as measured by maternal education attainment. Figure 6 visualizes the results shown in Table A5 on heterogeneous effects by gender. Heat waves tend to impose larger negative effects on females than males in terms of LBW. However, the gender difference is not significant.
Figure 6: Estimated impacts of temperature on birth outcomes, by gender.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: The figure plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin identified from the regressions in Table A5 for males and females. Panels A and B correspond to the two birth outcomes, log birth weight and LBW (i.e., <2,500 grams), respectively. The reference temperature bin is 0–24°C. All the coefficients are scaled by 100 to make them more readable. Other covariates and fixed effects are the same as those in Figure 3.
There have been regional variations in the trends of number of heat waves during our sample period. Figure A4 shows the proportion of hot days (>28 °C) throughout each year over 10 years. Overall, in years with higher proportion of hot days, average birth weight is lower. There is some trend of rising number of hot days in north China, while no clear pattern is found for south China. Regarding average birth weight, northerners experience no clear trend, while southerners see an increasing trend. These simple graphs raise the possibility that while birth weight may indeed be negatively correlated with rising hot days in the aggregate, the correlation may be due to a composition effect or be driven by the experiences of parents in specific regions of the country. We explore this hypothesis systematically below.24
For the purposes of our analysis, it is necessary to get a sense of not just the heterogeneity in ambient temperature trends across regions, but the actual exposure of mothers to such temperatures. Nevertheless, Figure A4 certainly suggests that our model specification should include flexible county-specific time trends to account for such local variations in temperature patterns (which we do). In Figure A5, we plot the distribution of daily mean temperatures during the gestation period for the northern and southern regions of China divided by the Huai river.25 It is clearly the case that mothers from the southern region of China experience more high temperature days during pregnancy. It is therefore possible that the baseline results could be driven by these southern mothers because of their higher rates of exposure. Alternatively, it could be the case that southern mothers may exhibit natural adaptation to heat so that the baseline findings are instead driven by the experiences of northern mothers who are not as well adapted to extreme heat exposure.
Table A6 shows the results of our baseline regression split by region. While the point estimates show that the negative impact of extreme heat exposure on birth weight is larger for infants born in the north compared to the south, the point estimates are not significantly different across the two regions. Our benchmark findings are therefore unlikely to be driven by factors that imply regional heterogeneity for these effects.
In Table A7, we present results for our baseline regression for offspring of mothers with different levels of educational attainment; i.e., middle school or below versus high school or above. It seems that the impact of heat waves on birth weight is larger for newborns of less educated mothers, and the difference is significant for LBW.
4.4. Alternative hypotheses
Our findings that exposure to heat waves results in negative outcomes for birth weight stand in contrast with some existing work in the literature. For example, Wilde et al. (2017) find that a higher temperature at conception leads to better educational attainment and literacy, fewer disabilities, and lower child mortality. Andalon et al. (2016) find a positive and statistically significant association between APGAR scores and high-temperature shocks (events two or more SDs above the historical mean).
4.4.1. Selection into conception during heat waves based on SES
One argument for why we might expect exposure to heat waves to lead to positive birth outcomes (as opposed to what we found in this paper) is the possibility that heat waves may affect fertility patterns, for example, through falling sexual activity during heat waves (Buckles and Hungerman 2013; Barreca, Deschênes and Guldi 2018; Wilde et al. 2017). The effect may be disproportionally larger for parents of low SES if they are unable to shield against heat waves (by employing AC, for instance). Consequently, fertility may fall faster among lower SES families nine months after the heat wave, thereby raising the average SES among the pool of women conceiving children during heat waves. Naturally, children from more privileged backgrounds with fitter mothers are more likely to have better birth outcomes during heat waves.
In Panel A of Figure 7, we directly test whether there is any sorting into temperature exposure in terms of SES (as measured by maternal education) around the time of conception (specifically, within 30 days before conception). As opposed to Wilde et al. (2017) and others, we do not find a salient pattern that, in the Chinese context, higher SES mothers sort into higher temperature bins before conception. No AC installed for almost all families may explain this absence of maternal sorting by SES. As shown in Panel A of Figure 8, we find the number of extreme hot days (above 28 °C) during the gestation period is associated with higher SES at the 10% significance level. However, the significance disappears when we identify the relationship by trimester in Panel A of Figure A6. Therefore, we do not find strong evidence for the selection into conception during heat waves based on SES.
Figure 7: Mechanism tests – effects of temperature in the last 30 days before conception.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: The figure plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin identified from the regressions in Panel A of Table A8. Panels A, B and C correspond to the three birth outcomes, mother’s years of education, child being female and number of births at conception-county-month level, respectively. The reference temperature bin is 0–24°C. The coefficients in Panel A and Panel B are scaled by 100 to make them more readable. Panel A and Panel B control county × day of conception year fixed effects, county × linear conception year time trend, and conception year fixed effects. Panel C controls county × conception month fixed effects and conception year fixed effects. Other covariates include mean precipitation, mean wind speed, mean sunshine duration and mean humidity in the last 30 days before conception in square polynomial forms.
Figure 8: Mechanism tests – effects of temperature during the gestation period.

Source: China’s National Disease Surveillance Points system and China Meteorological Data Service Center.
Note: The figure plots the estimated coefficients with 90% and 95% confidence intervals associated with each temperature bin identified from the regressions in Panel B of Table A8. Panels A, B and C correspond to the three birth outcomes, mother’s years of education, child being female and number of births at conception-county-month level, respectively. The reference temperature bin is 0–24°C. The coefficients in Panel A and Panel B are scaled by 100 to make them more readable. Panel A and Panel B control county × day of conception year fixed effects, county × linear conception year time trend, and conception year fixed effects. Panel C controls county × conception month fixed effects and conception year fixed effects. Other covariates include mean precipitation, mean wind speed, mean sunshine duration and mean humidity during the gestation period in square polynomial forms.
4.4.2. In utero mortality selection as a result of exposure to extreme temperatures
A second potential reason why we might expect to find that extreme heat exposure leads to better birth outcomes (we find the opposite) is mortality selection in utero. Extreme temperature may increase fetal mortality directly through an adverse, direct biological effect or indirectly through reduced farm income, poor nutrition, and maternal health (Barreca 2017). This hypothesis implies that weaker fetuses are more likely to be selected out through the culling effect after exposure to extreme temperatures, while stronger fetuses tend to survive and are inherently healthier. One may therefore observe positive associations between extreme temperatures and birth outcomes when the culling effect dominates the scarring effect on the surviving babies. Several papers provide evidence about this channel. For example, Wilde et al. (2017) attribute the positive correlation between temperature at conception and later life outcomes largely to fetal selection. Importantly, such mortality selection is typically gender differentiated, as males tend to be more vulnerable to negative shocks. For example, Valente (2015) finds that, in the context of maternal stress, in utero shocks result in a decrease in the male-to-female sex ratio at birth.
Residents in rural China, rich or poor, often have some access to traditional forms of winter heating with varying quality (e.g., burning firewood or coal, but no centralized winter heating). This probably explains why we do not observe statistically significant impact of cold exposure on birth outcomes. However, it is true that Chinese families generally have limited options to shield against heat waves. For example, according to the China Statistical Yearbook 2001, the rate of AC ownership in China was a mere 1.32 units per 100 households in 2000. Nevertheless, do we observe a strong impact on mortality or gender selection implied by the above mortality selection mechanism?
While our data does not provide information on infant mortality or still births, as we can see from Panels C of Figure 7 and Figure 8, there appears to be negative correlation between the number of days of high temperature exposure both in the 30 days before conception and during the gestation period with the number of births at the conception-county-month level. This is also true when we look at the results at the trimester level, especially the first trimester; see, Panel C of Figure A6. However, the finding of larger negative correlation for 24–28 °C bin than for >28 °C bin deserves future investigation.
Panel B of Figure 8 shows that the number of days of extreme temperature exposure during the gestation period does not predict the gender of the child. In fact, Panel B of Figure 7 finds that the number of days of extreme heat exposure in the 30 days before conception increases the probability that the child is male (and not female, as expected). Meanwhile, the evidence for mortality selection at the trimester level is also mixed and therefore difficult to interpret in favor of the hypothesis. As Panel B of Figure A6 shows, babies who experience more days of extreme heat during gestation in the second trimester are likely to be born female. However, those experiencing more extreme heat days in the first trimester are more likely to be born male.
Taken together, these results suggest that the fetal mortality selection mechanism after being exposed to heat waves or cold spells is probably not strong in our context (China).26
5. Conclusion
The existing literature has focused on the economic burden imposed by a greater frequency of heat waves due to climate change on vulnerable populations. In this paper, we investigate the consequences of in utero exposure to extreme temperatures (both extreme cold and heat waves) on birth outcomes, i.e., log birth weight and LBW, using a large, nationally representative dataset in rural China. We find that in utero exposure to extreme cold has no impact on the birth outcomes of surviving children while exposure to heat waves yields significant negative effects. Lack of access to technological adaptation devices against heat, e.g., AC, is likely a key cause. If this is the case, the negative impact of exposure to heat waves might have become more muted in the past two decades with the diffusion of AC in rural China.
Supplementary Material
*.
The authors are grateful to the editor and three anonymous referees for their very valuable and insightful suggestions, which have substantially improved the quality of this work. The authors also acknowledge helpful comments from audiences at various conferences, seminars and workshops. Xi Chen is grateful for financial support from the James Tobin Research Fund at Yale Economics Department, Yale Macmillan Center Faculty Research Award (2017–2019), the U.S. PEPPER Center Scholar Award (P30AG021342, 2016–2018), NIH/NIA Career Development Award (K01AG053408, 2017–2021), and NIH/NIA Research Awards (R03AG048920). Chih Ming Tan thanks the Greg and Cindy Page Faculty Distribution Fund for financial support. Xin Zhang acknowledges financial support from the China Postdoctoral Science Foundation Grants (2017M620653 and 2018T110057) and the Fundamental Research Funds for the Central Universities. The authors declare that they have no conflict of interest.
Footnotes
A wide range of outcomes have been investigated, for example, birth outcomes (Currie and Rossin-Slater 2013), human capital formation (Graff Zivin, Hsiang and Neidell 2018), health, education, and socioeconomic outcomes (Maccini and Yang 2009), hospitalizations (Karlsson and Ziebarth 2018), the allocation of time (Graff Zivin, Joshua and Neidell 2010), and the mortality rate (Huynen et al. 2001; Deschênes and Moretti 2009; Anderson and Bell 2009; Deschênes and Greenstone 2011; Barreca 2012; Burgess et al. 2014). Also see Graff Zivin, Joshua and Neidell (2013), Dell, Jones and Olken (2014), and Heal and Park (2015) for comprehensive surveys.
In comparison, existing studies using more recent data or from developed nations often identify combined effects that involve the biological effect and the adaptation/mitigation effect (see a comprehensive review and discussion about isolating biological effect in Currie et al. 2014).
We run robustness checks where we replicate our benchmark exercises using the subsample of observations before the year 1997 just to make sure that migration is not driving our results. Our main findings remain qualitatively similar and robust (see Columns (5)–(6) in Table A4). Since using the subsample 1991–1997 leaves us 164,000 fewer newborn observations, in our main estimations we retain more sample by using the whole period 1991–2000.
As Sun (2015) points out, “Although the Ministry of Labor and Social Security provides health insurance plans to urban hukou residents, rural-to-urban migrants are excluded from public healthcare because of their rural hukou status (Wei 2006). Most migrants and their children have limited access to sanitation and other basic health facilities…. Private hospitalization, the only option available to migrants, is a costly luxury that most will not take on. More importantly, they do not wish to “waste” remittances, which are designated to go home and support family, for their own health problems (Grey 2008).”
The male-female gender gap is 70.44 grams for birth weight and 1.10% for LBW, while the gap between newborns to less educated mothers (primary school or below) and more educated mothers (college or above) is 76.79 grams for birth weight and 1.52% for LBW.
While these findings are unlikely to be driven by migration, we should cautiously interpret our results. Since we are unable to completely rule out the possibility that a small share of expectant mothers could respond to unusually hot time periods via temporary moving, there would potentially be selection bias.
Our identified effect on LBW is more sizable, which amounts to (1.05×28=) 29.4 percent increase in LBW, that is, 1.05 percent higher incidence of LBW per day of exposure to heat waves, for a total of 28 more days during 1991–2000. This more salient effect on LBW may stem from larger effects towards dragging those vulnerable newborns who are slightly above the LBW cut-off to below the cut-off.
The gestational week information is recorded according to the exact date of the mother’s last menstrual period. Figure A1 plots the distribution of gestational age at birth in our sample. The distribution of gestational age in our sample is similar to that in Dai et al. (2004), which confirms the accuracy of the gestational age measurement.
We run a linear probability model (LPM) model of the missing indicator (1 if the observation is missing from the estimation sample; 0 otherwise) on the 10 temperature bins. None of the coefficients are significant and the magnitudes are small, suggesting that the values are largely missing at random.
The mean of gestational age is 39.2 weeks while the mode is 40 weeks in our sample. It is a common practice to assign weather exposure based on the expected gestational length (i.e., mean value in our case) instead of the actual exposure because of the concern over endogenous gestational age (Deschênes, Greenstone and Guryan 2009; Currie and Rossin-Slater 2013). Our baseline results are robust if we match temperatures to birth outcomes during the 40 weeks after the conception. The result is available upon request.
Weeks 1–2 are usually before the conception even starts. To address this concern, we conduct a robustness check by assigning weeks 3–13 to trimester 1. Our result is robust to this change. The result is available upon request.
These results are reported in Columns (5) and (6) of Table A2. Again, consistent with the baseline results in Columns (1)–(4), we show no distinguishable effect of exposure to extreme cold temperatures (<−4 °C) but significant effect after exposure to heat waves (>28 °C).
The same approach is taken by Karlsson and Ziebarth (2018). The average matching distance in our sample is 32 km. Only 4.1% of our newborns are matched to weather stations beyond 60 km. Our matching radius is smaller than those used in Deschenes et al. (2009) and Deschenes and Greenstone (2011).
Our benchmark temperature bins are similar to those in Isen et al. (2017). We also define the temperature bins using daily maximum temperatures and daily minimum temperatures. Our main findings remain unchanged. The results are available upon requests.
Figure A2 displays the histogram of birth weight in our sample. As displayed in Figure A2, birth weight heaps mainly at 3,000 and 3,500 grams. Our results are still robust if we remove observations at 3,000 and 3,500 grams. Please see the result in Column (9) of Table A4.
We have experimented with many fixed effects specifications to capture local heterogeneity and seasonality. We report the baseline findings for these specifications in Table A9 of the Appendix. Our benchmark findings are qualitatively robust to these alternatives.
These results are reported in Columns (1) and (3) of Table A2.
We also run quantile regressions on birth weight. Our main findings still hold. The results are available upon requests.
For example, Deschênes, Greenstone and Guryan (2009) show that for all three trimesters, exposure to hot days (>85 °F or >29.4 °C) is associated with a statistically significant decline in birth weight ranging in magnitude from 0.003 to 0.009 percent per such day, relative to a day in the reference category (45–65 °F, or 7–18 °C). Our identified larger effect could be due to our lower reference temperatures than Deschênes, Greenstone and Guryan (2009).
The main results are robust if we examine the effect of cold spells and heat waves separately. An anonymous referee also suggested that the −4–0 °C category may be poorly powered and that it may be a good idea to combine the relevant temperature bins. Our baseline results are robust if we combine the <−4 °C and 0–4 °C bins together. In fact, after combining the two lower temperature bins, the estimates for hot temperatures are even more sizable across birth outcomes. These results are available upon request.
The variable SGA refers to babies whose birth weights are below the 10th percentile for each gestational age by gender using data from the China National Population-based Birth Defects Surveillance System; see, Table 2 in Dai et al. (2014) for the gestational age-specific birth weight percentiles for Chinese babies.
Preterm is defined as gestational age below 37 weeks.
As expected, statistical tests show that our treatment effects (during pregnancy) are significantly larger than the placebo estimates (before conception; after birth). However, the difference in LBW between our treatment effect (during pregnancy) and a placebo estimate (before conception) is imprecisely estimated, which deserves a cautious interpretation. We thank an anonymous referee for suggesting this test.
We thank an anonymous referee for making this important observation.
The lack of common support or overlap is an important concern when estimating the impact of extreme temperature exposure on birth outcomes. For example, when we investigate the impact of exposure to heat waves, are we only restricted to births in a region where temperatures are typically high? If so, the external validity of our findings may be called into question. As revealed in Figure A5, we find evidence for common support for both extreme heat and extreme cold across both regions in China—that is, across both regions, children have some likelihood of being exposed to both the highest (>28 °C) and lowest (<−4 °C) temperature bins while in utero.
Of course, it is possible that the muted gender-biased mortality selection may have to do with strong son preference in rural China, where mothers who know that they are bearing sons take better care of themselves or even reallocate resources from daughters to sons to compensate for sons’ losses (Gupta et al. 2003; Lhila and Simon 2008; Chen et al. 2013). We have no way of directly verifying this possibility.
Contributor Information
Xi Chen, Department of Health Policy and Management, Yale School of Public Health, New Haven, CT 06520, USA; Department of Economics, Yale University, New Haven, CT 06511, USA.
Chih Ming Tan, Department of Economics, College of Business and Public Administration, University of North Dakota, Grand Forks, ND 58202, USA.
Xiaobo Zhang, National School of Development, Peking University, 5 Yiheyuan Road, Beijing 100871, China; Division of Development Strategy and Governance, International Food Policy Research Institute, 1201 Eye Street, NW, Washington, DC 20005, USA.
Xin Zhang, School of Statistics, Beijing Normal University, Beijing 100875, China.
REFERENCES
- Adhvaryu Achyutu, Fenske James, Kala Namrata, and Nyshadham Anant. 2017. “Fetal Origins of Mental Health: Evidence from Africa.” Available at http://static1.1.sqspcdn.com/static/f/884336/27600991/1498048251633/AFKNMentalHealthMay2017.pdf?token=OKpEPTzjGnbt%2BoVS7CP%2BBW3lFIs%3D. Accessed October 18, 2018.
- Almond Douglas and Currie Janet. 2011. “Killing Me Softly: The Fetal Origins Hypothesis.” Journal of Economic Perspectives, 25 (3): 153–172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andalon Mabel, Rodríguez-Castelán Carlos, Viviane Sanfelice, Azevedo João Pedro and Daniel Valderrama. 2016. “Weather Shocks and Health at Birth in Colombia.” World Development, 82: 69–82. [Google Scholar]
- Anderson GB and Bell ML. 2009. “Weather-related mortality: how heat, cold, and heat waves affect mortality in the United States.” Epidemiology, 20(2): 205–213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barker David J. P. 1992. “The Fetal Origins of Adult Hypertension.” Journal of Hypertension, 10: 39–45. [PubMed] [Google Scholar]
- Barreca Alan. 2012. “Climate Change, Humidity, and Mortality in the United States.” Journal of Environmental Economics and Management, 63, 19–34. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barreca Alan. 2017. “Does hot weather affect human fertility?” IZA World of Labor 375, doi: 10.15185/izawol.375. [DOI] [Google Scholar]
- Barreca Alan, Clay Karen, Deschenes Olivier, Greenstone Michael, and Shapiro Joseph S.. 2016. “Adapting to Climate Change: The Remarkable Decline in the US Temperature-Mortality Relationship over the Twentieth Century.” Journal of Political Economy, 124(1): 105–159. [Google Scholar]
- Barreca A, Deschênes O and Guldi M 2018. “Maybe Next Month? Temperature Shocks and Dynamic Adjustments in Birth Rates.” Demography 55: 1269. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bharadwaj P, Lundbord P, Rooth D-O. 2017. “Birth weight in the long run.” Journal of Human Resources, 53(1): 189–231. [Google Scholar]
- Black S, Devereux P, Salvanes K 2009. “From the cradle to the labor market? The effect of birth weight on adult outcomes.” Quarterly Journal of Economics, 122(1), pp. 409–439. [Google Scholar]
- Bobb Jennifer F., Peng Roger D., Bell Michelle L. and Dominici Francesca. 2014. “Heat-related mortality and adaptation to heat in the United States.” Environmental Health Perspectives, 122(8):811–816. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Buckles KS. and Hungerman DM. 2013. “Season of Birth and Later Outcomes: Old Questions, New Answers.” The Review of Economics and Statistics, 95(3): 711–724. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burgess R, Deschenes O, Donaldson D and Greenstone M. 2014. “The Unequal Effects of Weather and Climate Change: Evidence from Mortality in India.” Available at https://pdfs.semanticscholar.org/8958/18edb2300f50ffe45417f3c065c722dd1ba4.pdf. Accessed January 9, 2020.
- Carolan-Olah M, Frankowska D. 2014. “High environmental temperature and preterm birth: a review of the evidence.” Midwifery, 30:50–59. [DOI] [PubMed] [Google Scholar]
- CDC. 2018. Climate Change and Extreme Heat Events. Atlanta, GA: U.S. Centers for Disease Control and Prevention. https://www.cdc.gov/climateandhealth/pubs/ClimateChangeandExtremeHeatEvents.pdf [Google Scholar]
- Chen Y, Li H, & Meng L 2013. “Prenatal Sex Selection and Missing Girls in China: Evidence from the Diffusion of Diagnostic Ultrasound.” Journal of Human Resources, 48(1), 36–70. [Google Scholar]
- Chirakijja J, Jayachandran S, Ong P. 2019. Inexpensive Heating Reduces Winter Mortality. NBER Working Paper No. 25681.
- Cunha Flavio, Heckman James J. and Schennach Susanne M.. 2010. “Estimating the Technology of Cognitive and Noncognitive Skill Formation.” Econometrica, 78 (3): 883–931. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Currie Janet, and Rossin-Slater Maya. 2013. “Weathering the Storm: Hurricanes and Birth Outcomes.” Journal of Health Economics, 32, 487–503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Currie Janet, Zivin Joshua Graff, Mullins Jamie, and Neidell Matthew. 2014. “What Do We Know About Short- and Long-Term Effects of Early-Life Exposure to Pollution?” Annual Review of Resource Economics 6(1): 217–247. [Google Scholar]
- Dai L, Deng C, Li Y, Zhu J, Mu Y, Deng Y, Mao M, Wang Y, Li Q, Ma S, Ma X and Zhang Y. 2014. “Birth Weight Reference Percentiles for Chinese.” PLoS ONE, 9(8): e104779. doi: 10.1371/journal.pone.0104779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Deschenes Olivier, and Moretti Enrico. 2009. “Extreme Weather Events, Mortality, and Migration.” The Review of Economics and Statistics, 91(4): 659–681. [Google Scholar]
- Deschenes Olivier, Greenstone Michael, and Guryan Jonathan. 2009. “Climate Change and Birth Weight.” American Economic Review: Papers & Proceedings, 99(2): 211–217. [DOI] [PubMed] [Google Scholar]
- Deschenes Olivier, and Greenstone Michael. 2011. “Climate Change, Mortality, and Adaptation: Evidence from Annual Fluctuations in Weather in the US.” American Economic Journal: Applied Economics, 3: 152–185. [Google Scholar]
- Dell Melissa, Jones Benjamin F., and Olken Benjamin A.. 2014. “What Do We Learn from the Weather? The New Climate-Economy Literature.” Journal of Economic Literature, 52(3): 740–798. [Google Scholar]
- Elter K, Ay Emine, Uyar Esra and Kavak Zehra N.. 2004. “Exposure to low outdoor temperature in the midtrimester is associated with low birth weight.” Aust N Z J Obstet Gynaecol, 44(6), pp. 553–557. [DOI] [PubMed] [Google Scholar]
- Figlio D, Guryan J, Karbownik K, Roth J 2014. “The effects of poor neonatal health on children’s cognitive development.” American Economic Review, 2014, 104(12), pp. 3921–3955. [DOI] [PubMed] [Google Scholar]
- Gasparrini A, Guo Y, Hashizume M, Kinney PL, Petkova EP, Lavigne E, Zanobetti A, Schwartz JD, Tobias A, Leone M, Tong S, Honda Y, Kim H, Armstrong BG 2015. “Temporal variation in heat–mortality associations: a multicountry study.” Environmental Health Perspectives, 123(11):1200–1207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gosling Simon N., Lowe Jason A., McGregor Glenn R., Pelling Mark and Malamud Bruce D.. 2009. “Associations between elevated atmospheric temperature and human mortality: a critical review of the literature.” Climate Change, 92(3):299–341. [Google Scholar]
- Zivin Joshua S. Graff, and Neidell Mathew. 2010. “Temperature and the Allocation of Time: Implications for Climate Change.” Journal of Labor Economics, 32(1): 1–26. [Google Scholar]
- Zivin Joshua S. Graff,, and Neidell Mathew. 2013. “Environment, Health, and Human Capital.” Journal of Economic Literature, 51(3): 689–730. [Google Scholar]
- Graff Zivin J, Hsiang SM, and Neidell M. 2018. “Temperature and Human Capital in the Short and Long Run.” Journal of the Association of Environmental and Resource Economists, 5(1):77–105. [Google Scholar]
- Grey W 2008. “Migrant Education in Beijing: Hukou and the Future of Human Capital Development.” Western Political Science Association Annual Meeting. [Google Scholar]
- Gupta MD, Zhenghua J, Bohua L, Zhenming X, Chung W, & Hwa-Ok B 2003. Why is Son Preference so Persistent in East and South Asia? A Cross-Country Study of China, India, and the Republic of Korea: The World Bank. [Google Scholar]
- Ha S, Liu D, Zhu Y, Kim SS, Sherman S and Mendola P. 2017. “Ambient Temperature and Early Delivery of Singleton Pregnancies.” Environmental Health Perspectives, 125 (3): 453–459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heal Geoffrey, and Park Jisung. 2015. Goldilocks Economies? Temperature Stress and the Direct Impacts of Climate Change. NBER Working Paper 21119.
- Heckman James J. and Mosso Stefano. 2014. “The Economics of Human Development and Social Mobility.” Annual Review of Economics, 6: 689–733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hu Zihan, and Li Teng. 2019. “Too hot to handle: The effects of high temperatures during pregnancy on adult welfare outcomes.” Journal of Environmental Economics and Management, 94: 236–253. [Google Scholar]
- Huynen Maud M.T.E., Martens Pim, Schram Dienke, Weijenberg Matty P., and Kunst Anton E.. 2001. “The Impact of Heat Waves and Cold Spells on Mortality Rates in the Dutch Population.” Environmental Health Perspectives, 109(5): 463–470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Iparraguirre J 2015. “Have winter fuel payments reduced excess winter mortality in England and Wales?” Journal of Public Health, 37(1): 26–33. [DOI] [PubMed] [Google Scholar]
- Isen A, Rossin-Slater M and Walker R 2017. “Relationship between season of birth, temperature exposure, and later life wellbeing.” Proceedings of the National Academy of Sciences of the United States of America, 114(51), 13447–13452. [DOI] [PMC free article] [PubMed] [Google Scholar]
- IPCC. 2014. Climate change 2014: synthesis report. Contribution of working groups I, II and III to the Fifth Assessment Report of the Intergovernmental Panel on Climate Change. technical report. Geneva: Intergovernmental Panel on Climate Change. [Google Scholar]
- Karlsson M and Ziebarth NR. 2018. “Population Health Effects and Health-Related Costs of Extreme Temperatures: Comprehensive Evidence from Germany.” Journal of Environmental Economics and Management, 91: 93–117. [Google Scholar]
- Lhila A, & Simon KI 2008. “Prenatal Health Investment Decisions: Does the Child’s Sex Matter?” Demography, 45(4), 885–905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maccini Sharon, and Yang Dean. 2009. “Under the Weather: Health, Schooling, and Economic Consequences of Early-Life Rainfall.” American Economic Review, 99(3): 1006–1026. [DOI] [PubMed] [Google Scholar]
- Meng Xin. 2012. “Labor Market Outcomes and Reforms in China.” Journal of Economic Perspectives, 26 (4): 75–102. [Google Scholar]
- Meng Xin and Qian Nancy. 2009. The Long-term Consequences of Famine on Survivors: Evidence from a Unique Natural Experiment Using China’s Great Famine. NBER Working Paper No. 14917.
- Persson Petra and Rossin-Slater Maya. 2014. Family Ruptures and Intergenerational Transmission of Stress. IFN Working Paper No. 1022.
- Seltenrich Nate. 2015. “Between Extremes: Health Effects of Heat and Cold.” Environmental Health Perspectives, 123(11): A275–A280. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Steadman Robert G. 1984. “A universal scale of apparent temperature.” Journal of Climate and Applied Meteorology, 23, 1674–1687. [Google Scholar]
- Strand Linn B., Barnett Adrian G., and Tong Shilu. 2011. “The influence of season and ambient temperature on birth outcomes: A review of the epidemiological literature.” Environmental Research, 111, 451–462. [DOI] [PubMed] [Google Scholar]
- Sun Meiping. 2015. “The Potential Causal Effect of Hukou on Health among Rural-to-Urban Migrants in China.” Available at http://www.columbia.edu/~ms4196/Hukou_system.pdf. Accessed January 9, 2020.
- Tan Chih Ming, Tan Zhibo and Zhang Xiaobo. 2015. “Sins of the Fathers: The Intergenerational Legacy of the 1959–61 Great Chinese Famine on Children’s Cognitive Development.” Available at https://ssrn.com/abstract=2409452. Accessed October 18, 2018. [DOI] [PubMed]
- Valente Christine. 2015. “Civil Conflict, Gender-specific Fetal Loss, and Selection: A New Test of the Trivers–Willard Hypothesis.” Journal of Health Economics, 39: 31–50. [DOI] [PubMed] [Google Scholar]
- Wei T 2006. “Many Migrant Workers Struggle with Medical Expenses in Big Cities.” Beijing Review, 14–19. [Google Scholar]
- Wilde Joshua, Apouey Benedicte H., and Jung Toni. 2017. “The Effect of Ambient Temperature Shocks During Conception and Early Pregnancy on Later Life Outcomes.” European Economic Review, 97: 87–107. [Google Scholar]
- Yang G, Hu J, Rao KQ, Ma J, Rao C, and Lopez AD 2005. “Mortality registration and surveillance in China: history, current situation and challenges.” Population health metrics, 3(1), 3. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.