

Abstract
The extent to which treatment of speech errors that are phonetic in nature (i.e., distortions) produces generalization to untrained sounds is not well understood. This case study reports a child referred for treatment of a velarized distortion of American English /ɹ/, who also demonstrated an inconsistent velarized distortion of /l/. Acoustic analysis revealed evidence of a covert contrast between /ɹ/ and /l/ prior to treatment. Ultrasound biofeedback treatment and perceptual training targeted /ɹ/ only, but progress was tracked for both /ɹ/ and /l/. Substantial improvements in perceptually rated accuracy and significant changes in acoustic features were observed for both sounds, indicating generalization. These results highlight that generalization from trained to untrained sounds is possible for children with residual speech errors characterized by phonetic distortions.
Keywords: speech sound disorders, generalization, covert contrast, rhotics
Introduction
Generalization is an important consideration for effective and efficient speech therapy. Substantial literature has been devoted to maximizing clinical outcomes in speech therapy by focusing on treatment strategies that facilitate rapid and widespread generalization in children with speech sound disorders (Barlow & Gierut, 2002; Gierut et al., 2010; Hoffman, 1983; Powell & McReynolds, 1969; Powell, 1991). Generalization may be observed in several ways, including generalization from trained to untrained words or word positions (Hoffman, 1983; Preston et al., 2014). Ideally, generalization across speech sounds is preferred to effect maximal change. Cases of generalization between cognates (e.g., from voiceless to voiced obstruents), within a manner class (e.g., from one fricative to another), and across manner classes following implicational hierarchies of complexity or markedness (e.g., from affricates to fricatives) have been reported in previous literature (Gierut, 1990; Gierut et al., 1996; Gierut & Morrisette, 2011). However, these findings generally come from studies of children with phonological disorders, whose errors often represent substitutions of one contrastive phoneme for another. There is less evidence to support generalization across speech sounds in children who demonstrate errors that are phonetic in nature (i.e., distortions). This may be attributable to the fact that phonetic distortions are commonly conceptualized as motoric rather than phonological in origin. As generalization across sounds could potentially decrease the treatment time required for children with multiple phonetic distortions, this is an area of significant clinical relevance.
Generalization may be enhanced by heightened awareness of speech sounds. For example, explicit training in self-monitoring has been shown to facilitate generalization (Koegel et al., 1986a; Shriberg & Kwiatkowski, 1987). Providing opportunities for self-monitoring may allow children to become more active participants in the treatment process. Successful self-monitoring is thought to require adequate metalinguistic awareness, including an accurate linguistic representation of the intended form and an understanding of how this may differ from one’s own habitual productions (Hagood & Dun 1985). One means of increasing metalinguistic awareness of speech is to provide visual models and feedback representing the child’s articulatory gestures; it is possible that such visualizations may aid generalization of those gestures to untrained speech sounds.
Visual articulatory feedback can be provided with several technologies, including ultrasound visual feedback (UVF), which provides a display of tongue movement in real time. This approach has been shown to be an efficacious treatment modality for children with speech sound disorders, including those with distortions of American English /ɹ/ (Preston et al., 2014, 2017, 2018; Sugden et al., 2019). This is considered a particularly challenging sound to remediate clinically, due in large part to the complex tongue shape required for correct production. It is also important to note that tongue and lip positions for the correct production of /ɹ/ vary greatly between individual speakers and are dependent on the size and shape of each individual’s vocal tract, as well as the phonetic context in which the sound is being produced (Guenther et al., 1999; Mielke et al., 2016). Cuing strategies for treatment must thus be highly individualized. UVF enables explicit and concrete cuing related to each part of the tongue, including elevation of the tongue tip/blade, posterior retraction of the tongue root, and elevation of the sides of the dorsum (Preston et al., 2020). Failure to execute any of these elements during /ɹ/ production may result in a distortion of the sound. During treatment, UVF can be utilized to point out these specific movements to enhance clinicians’ and clients’ understanding of the articulatory requirements for accurate production of speech sounds. As children with /ɹ/ distortions learn the phonetic characteristics of the sound, it is plausible that such knowledge may heighten awareness of misarticulations of phonetically similar sounds such as /l/, as both /ɹ/ and /l/ require a complex tongue shape (Gick, et al., 2007).
Treatment outcomes may also be enhanced if a covert contrast is present between misarticulated sounds, as opposed to a true substitution or phoneme collapse. Covert contrasts are productions which are acoustically (and articulatorily) distinct, but are neutralized in most listeners’ perceptions. Covert contrasts may be detected through acoustic analysis (Baum & McNutt, 1990; Forrest et al., 1990; Li et al., 2009; Maxwell & Weismer, 1982; Tyler et al., 1990) as well as other instrumental methods (Cleland et al., 2017; Gibbon, 1990). For children with speech disorders, it is believed that the presence of a covert contrast indicates a level of phonological knowledge beyond what is apparent to typical listeners (Tyler et al., 1990). Covert contrasts are reported to be a positive prognostic indicator, as children who demonstrate a covert contrast often make more rapid progress in treatment as compared to children who demonstrate a phoneme collapse (Gibbon et al., 1993; Tyler et al., 1993). No study to date has examined the impact of covert contrasts on generalization in treatment, although it is plausible that generalization could be enhanced by the heightened level of phonological knowledge which a covert contrast may represent.
Purpose
The present study investigates generalization learning in a case report of a child for whom several of the above-discussed factors are relevant. The participant exhibited residual errors impacting American English /ɹ/ and /l/, which were both produced with a perceptually identical velarized distortion. However, acoustic analysis revealed a covert contrast between /ɹ/ and /l/. This child participated in a treatment research study for /ɹ/ errors that included UVF and self-monitoring of productions. The present study used acoustic and perceptual measures to examine changes in the treated sound, /ɹ/, as well as generalization to the untrained /l/. To our knowledge, no study to date has addressed the impact of a covert contrast on generalization between speech errors that are phonetic in nature.
Method
Participant
Larry (pseudonym) was a 9-year-old male referred by a local speech-language pathologist for a treatment study on remediation of /ɹ/ (reported in Preston, Hitchcock & Leece, 2020). Larry had received no previous speech therapy prior to the study. This study was carried out in accordance with the recommendations of the Syracuse University Institutional Review Board.
Larry’s performance on several standardized tasks suggested language and cognitive abilities broadly within normal limits. His scores were average on the Peabody Picture Vocabulary Test-4 (Dunn & Dunn, 2007) (standard score: 100), Clinical Evaluation of Language Fundamentals–5 (Wiig et al., 2013): Formulated Sentences (scaled score: 10) and Recalling Sentences (scaled score: 9). Larry passed a hearing screening at 500, 1000, 2000, 5000 Hz bilaterally at 20 dBHL.
Articulation skills were below age expectations on both the Goldman-Fristoe Test of Articulaton-2 (Goldman & Fristoe, 2000) (percentile rank: 5) and the Linguisystems Articulation Test (Bowers & Huisingh, 2008) (percentile rank <1). On these tasks, his errors consisted of a somewhat unusual velarized distortion of /ɹ/ and /l/ (i.e., both sounds produced with a single velar constriction of the oral cavity) on all erred productions. No other sound errors were noted. When in error, his distortions on both /ɹ/ and /l/ in syllable onsets were perceived to be highly similar in nature; thus, to the clinician, there was a perceptual merger of /ɹ/ and /l/. During a stimulability assessment (Miccio, 2002), 11 different syllables with /ɹ/ were elicited through direct imitation three times each, and Larry was unsuccessful at imitating /ɹ/ in any context (score: 0/33).
Treatment Procedures
This case study is drawn from a larger group study investigating treatment conditions that affect /ɹ/ production (Preston et al., 2020). Larry received 14 sessions of speech therapy using ultrasound biofeedback to address errors affecting /ɹ/. Sessions were approximately one hour in length and were scheduled twice per week for 7 weeks. The second author, a certified SLP, delivered the treatment. Larry did not receive any outside treatment targeting /ɹ/ while enrolled in the study.
Each session began with a pre-practice period during which Larry completed a 50-item researcher-developed speech perception training module. Using a format broadly modeled after SAILS (Rvachew et al., 2004), Larry listened to recorded productions of single words with /ɹ/ in various word positions spoken by children with typical speech as well as children with distorted /ɹ/ productions. He indicated via mouse click whether he thought the /ɹ/ in each word was produced correctly or not; each module was approximately balanced in its representation of correct and incorrect productions, as determined by consensus across expert listeners. He received reinforcement for responses that matched the judgment of expert listeners, and he received corrective feedback when his response did not match the expert listeners. Tokens could be replayed up to five times before a judgement was made. Larry completed seven different 50-item training modules twice each over the course of the 14 treatment sessions.
Following the pre-practice perceptual training, Larry practiced various syllables, words, and sentences containing /ɹ/ for 162 trials per session. The Challenge Point Program (CPP; McAllister et al., 2020; McAllister Byun et al., 2015), a researcher-developed open-source program, was used to guide stimulus presentation and feedback delivery. The CPP software prompted adaptive changes in feedback type (knowledge of performance or knowledge of results), feedback rate, or linguistic complexity based on Larry’s accuracy in the previous block of 6 productions, with only one change made per block. The levels of linguistic complexity included nonword syllables, one-syllable words, one-syllable words with a competing phoneme (/l/ or /w/), two-syllable words, two syllable words with /l/ or /w/, carrier phrases, and sentences. At higher levels of complexity, the CPP software prompted a reduction in clinician-provided knowledge of performance and knowledge of results feedback. To encourage self-monitoring, the software also prompted Larry to judge his own /ɹ/ accuracy before receiving feedback from the SLP on a randomly selected 50% of trials.
Sagittal ultrasound images from an Echo Blaster 128 (Telemed, n.d.) were used to cue Larry to produce /ɹ/ by raising his tongue blade, lowering his tongue dorsum, and retracting the tongue root (Preston et al., 2020). Larry was cued to make a bunched /ɹ/, as this shape was judged to be more conducive to /ɹ/ productions that were perceived as accurate by the treating SLP. During sessions 1–7, Larry practiced a small number of both prevocalic and postvocalic /ɹ/ contexts (i.e., /ɪɹ, ɛɹ, ɹɑ, ɹe/) using the ultrasound biofeedback for 88% of trials each session. During sessions 8–14, Larry practiced a larger number of targets (i.e., /ɪɹ, ɛɹ, ɑɹ, ɔɹ, ɹe, ɹaɪ, ɹɑ, ɹu, ɝ/ and the ultrasound biofeedback was provided for 44% of trials. Importantly, no cueing for /l/ production was provided in treatment.
Assessment of Changes
Changes in speech production were monitored using probes in which the participant read 25 words containing /ɹ/ onset singletons and 25 words containing /l/ onset singletons. Probe words remained consistent throughout the course of the study. Audio recordings of these probes were collected using a Sennheiser MKE2 lavalier microphone recorded into Praat (Boersma & Weenink, 2017) as WAV files and sampled at 44.1 kHz using 16 bit quantization. Probe recordings were collected three times before treatment to assess baseline performance, once at the midpoint of treatment (after 7 sessions), one week after the final treatment session, and two months later.
Acoustic analysis
For each probe recording, Praat textgrids were used to mark the target words and point tiers were created in which the onset of the /ɹ/ or /l/ segment was marked. The point marked was approximately 15 msec after the onset of voicing as evident in the acoustic waveform, with adjustments made to ensure there were recognizable formants in the spectrogram (e.g., for a handful of productions with breathy onsets). Values for F1, F2 and F3 were then automatically extracted using the following settings in Praat: positive maximum formant set to 6,500 Hz, positive window length set to 0.025 seconds, positive time step set to 0.01, and maximum number of formants set to 5. To assess the reliability of the extracted acoustic measurements, a randomly selected subset of tokens representing 20% of the full sample was re-measured manually. A t test for paired samples showed no significant difference in the two sets of F1, F2, and F3 measurements.
Perceptual Ratings
Four graduate student listeners independently scored each production with regard to the accuracy of the /ɹ/ or /l/ segment. The graduate students were native speakers of English who had training in phonetics. Words from each time point (baseline, midpoint, post-treatment) were presented to listeners in random order. The participant’s productions were combined with those of other participants and randomized so listeners did not accommodate to a single speaker’s patterns. Each word was scored with a binary rating (0 = inaccurate or 1 = perceptually correct) based on the audio recording only. Raters were blind to other raters’ scores and to the time point of elicitation. Fleiss’ kappa, which was calculated to determine reliability across multiple raters, was estimated at 0.81 (95% CI, 0.78 to 0.84). The final data represent the average of the four listeners’ ratings. Upon review of the productions characterized as inaccurate, there was consensus among the authors that the distortions of both /ɹ/ and /l/ were best characterized as velarized distortions.
Results
Figure 1 shows the average of four listeners’ perceptual ratings of /ɹ/ and /l/ in onset position for three baseline assessments prior to treatment (B1-B3), at the midpoint of treatment (M), one week post-treatment (P1), and two months post-treatment (P2). Both sounds showed substantial improvement in perceived accuracy.
Figure 1: Perceptual ratings for word-initial /ɹ/ and /l/.
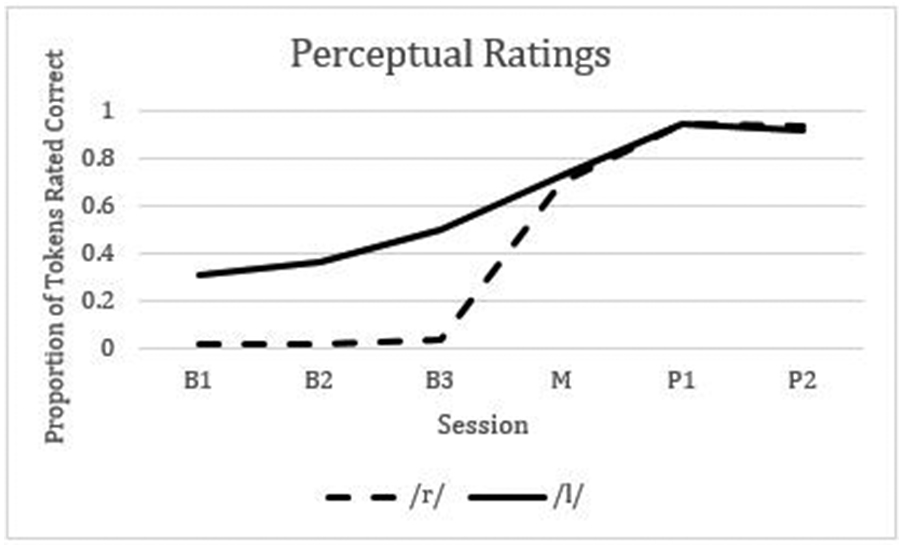
Note. B = Baseline, M = Midpoint, P = Post-treatment.
Acoustic analyses were carried out on the first three formants (F1, F2, F3), as these formants characterize correct and distorted productions of /ɹ/ and /l/. Spectrograms of representative pre- and post-treatment /ɹ/ and /l/ tokens are shown in Figure 2, and the mean values of the first three formants are shown in Figure 3. Results of a paired t-test revealed a significant drop in F3-F2 distance for /ɹ/ from baseline to post-treatment (t(24) = 10.45, p < .001), which is an acoustic indicator of more accurate /ɹ/ productions (Campbell et al., 2017; Shriberg et al., 2001). For /l/, a paired t-test revealed a significant increase in F2-F1 distance from baseline to post-treatment (t(24) = −7.76, p <.001), which corresponds to a shift from dark (velarized) to light (alveolar) /l/ productions (Recasens & Espinosa, 2005; Sproat, Richard & Fujimura, 1993). The acoustic results, therefore, align with the perceptual results showing an increase in perceptually rated correct productions.
Figure 2. Spectrograms of pretreatment /l/ and /ɹ/ in “lock” (A) and “rock” (B), post-treatment “lock” (C) and “rock” (D).

Figure 3: Mean formant values for word-initial /ɹ/ (3A) and /l/ (3B) across time points.
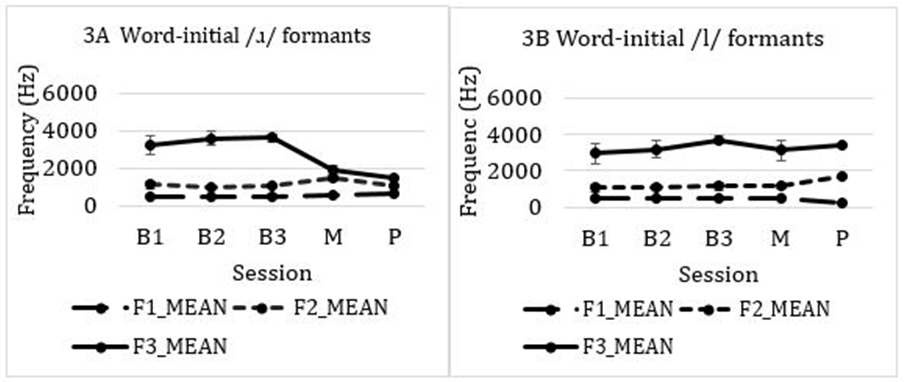
Note. B = Baseline, M = Midpoint, P = Post-treatment. Circles represent mean, error bars represent standard deviations.
Finally, because Larry’s distorted productions of both /ɹ/ and /l/ before treatment were perceived to be similar velarized distortions, a 2 (phoneme) x 3 (formant) ANOVA was used to compare formant values pooled across baseline sessions for tokens that were perceived by the majority of listeners to be incorrect. The results indicated a significant phoneme x formant interaction (F [2,107] = 6.79, p <0.001). Post-hoc analyses indicated no pre-treatment differences between /ɹ/ and /l/ in F1 (t(112) = .05, p = 0.96) or F2 (t(112) = .0.88, p = 0.38), but a slightly higher F3 for /ɹ/ than for /l/ (t(112) = 2.47, p = 0.015). This suggests that, even though the distortions of the two phonemes were perceived by listeners to be similar, there was an underlying acoustic difference evident in F3 in Larry’s distorted productions, indicating a covert contrast.
Discussion
This study examined across-phoneme generalization in a child who produced /ɹ/ and /l/ with a phonetically similar velarized distortion. Although only /ɹ/ was targeted in treatment, a significant change in acoustic features and perceptually-rated accuracy was observed for both /ɹ/ and /l/. This indicates that generalization across liquid phonemes can occur in children with phonetic distortions, at least in contexts similar to this instance involving covert contrast. To our knowledge, this is the first study addressing this type of generalization between /ɹ/ and /l/. Because this is only a single case, however, further research on generalization is clearly warranted.
A velarized distortion of both /ɹ/ and /l/ was perceived pre-treatment, which suggested a phonemic merger of the sounds; however, acoustic analysis revealed a covert contrast with regard to F3 values. This acoustic distinction indicates that Larry had a greater degree of pre-treatment phonological knowledge than perceptual evaluation would suggest. Even though he had not yet mastered the correct motor routines to produce an easily perceptible distinction, the acoustic difference that he produced between /ɹ/ and /l/ demonstrates that he had some level of awareness of a phonological contrast between these sounds. It has been suggested that having greater productive phonological knowledge of a target sound may lead to more rapid progress within treatment (Elbert et al., 1984; Gierut et al., 1987). It is possible that this higher degree of underlying knowledge was responsible for the fact that improvement was observed not only on the treated sound /ɹ/, but also the untreated sound /l/.
The inclusion of UVF in treatment may have encouraged greater understanding of the phonetic features of /ɹ/, which could have aided in the generalization of trained articulatory actions to untrained speech sounds. Specifically, lowering the dorsum of the tongue for a more accurate production of /ɹ/ may have generalized to a lower dorsum during production of /l/, contributing to the shift from dark (velarized) to light (alveolar) productions in onsets. Combined with Larry’s phonological knowledge of the contrast between /ɹ/ and /l/, the heightened awareness of articulatory movements for /ɹ/ provided by UVF may have increased his ability to generalize across liquid phonemes to achieve correct production of the untreated sound /l/. It is also important to note that Larry’s pre-treatment accuracy for /l/ was higher than his pre-treatment accuracy for /ɹ/, indicating an awareness of correct production of this sound prior to treatment. This may have also played a role in his ability to correct this error without direct treatment.
Finally, the self-monitoring training component of treatment may have enhanced Larry’s awareness of correct and incorrect sound productions, which could also have contributed to his improved accuracy for untrained as well as trained sounds (Koegel et al., 1986b). The results highlight that generalization to untrained sounds is possible not only for children with phonological disorders, but also children with residual speech errors characterized by phonetic distortions of speech sounds.
This study provides further evidence for the use of UVF in the treatment of speech errors that are phonetic in nature. Larry’s understanding of the articulatory movements necessary for accurate production of /ɹ/ may have been enhanced by this additional visual feedback, which may have been a factor in his ability to generalize across sounds. Generalization across liquid phonemes, as found in this study, has not previously been reported in a child with phonetic distortions. Clinically, clinicians may consider incorporating self-monitoring into the treatment of speech sound errors such as those observed in this case report, as this may have been another factor which enhanced generalization. Future studies investigating the impact of these two factors, UVF and self-monitoring, on generalization across treated and untreated sounds would be beneficial in guiding clinical decision making and treatment planning.
Acknowledgements:
Research reported in this publication was supported by the National Institute on Deafness and Other Communication Disorders of the National Institutes of Health under Award Number R15DC016426 (J. Preston, PI) and R01DC013668 (D. Whalen, PI). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
Declaration of Interest:
The authors report no conflict of interest.
Contributor Information
Caitlin V. Raaz, Department of Audiology and Speech Language Sciences, University of Northern Colorado, Greeley, CO
Megan C. Leece, Department of Communication Sciences & Disorders, Syracuse University, Syracuse, NY
Tara McAllister, Department of Communication Sciences & Disorders, New York University, New York, NY.
Jonathan L. Preston, Department of Communication Sciences & Disorders, Syracuse University, Syracuse, NY
References & Links
- Barlow JA, & Gierut JA (2002). Minimal pair approaches to phonological remediation. Seminars in Speech and Language, 23(1), 57–68. https://www.thieme-connect.com/DOI/DOI?10.1055/s-2002-24969 [DOI] [PubMed] [Google Scholar]
- Baum SR, & McNutt JC (1990). An acoustic analysis of frontal misarticulation of /s/ in children. Journal of Phonetics. [Google Scholar]
- Boersma P, & Weenink D (2017). Praat: doing phonetics by computer (Version 6.0.19) [Computer software] (v. 6.0.32). http://www.praat.org/ [Google Scholar]
- Bowers L, & Huisingh R (2008). LinguiSystems Articulation Test (LAT). Linguisystems. [Google Scholar]
- Campbell H, Harel D, Hitchcock E, & McAllister Byun T (2017). Selecting an acoustic correlate for automated measurement of American English rhotic production in children. International Journal of Speech-Language Pathology, 1–9. 10.1080/17549507.2017.1359334 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cleland J, Scobbie JM, Heyde C, Roxburgh Z, & Wrench AA (2017). Covert contrast and covert errors in persistent velar fronting. Clinical Linguistics & Phonetics, 31(1), 35–55. [DOI] [PubMed] [Google Scholar]
- Dunn LM, & Dunn DM (2007). Peabody Picture Vocabulary Test (4th ed.). Pearson. [Google Scholar]
- Elbert M, Dinnsen DA, & Powell TW (1984). On the prediction of phonologic generalization learning patterns. Journal of Speech and Hearing Disorders. 10.1044/jshd.4903.309 [DOI] [PubMed] [Google Scholar]
- Forrest K, Weismer G, Hodge M, Dinnsen DA, & Elbert M (1990). Statistical analysis of word-initial/k/and/t/produced by normal and phonologically disordered children. Clinical Linguistics & Phonetics, 4(4), 327–340. [Google Scholar]
- Gick B, Bacsfalvi P, Bernhardt BM, Oh S, Stolar S, & Wilson I (2007, June). A motor differentiation model for liquid substitutions in children's speech. In Proceedings of Meetings on Acoustics 153ASA (Vol. 1, No. 1, p. 060003). Acoustical Society of America. [Google Scholar]
- Gibbon F (1990). Lingual activity in two speech-disordered children’s attempts to produce velar and alveolar stop consonants: evidence from electropalatographic (EPG) data. International Journal of Language & Communication Disorders, 25(3), 329–340. [DOI] [PubMed] [Google Scholar]
- Gibbon F, Dent H, & Hardcastle W (1993). Diagnosis and therapy of abnormal alveolar stops in a speech-disordered child using electropalatography. Clinical Linguistics & Phonetics, 7(4), 247–267. [Google Scholar]
- Gierut JA (1990). Differential learning of phonological oppositions. Journal of Speech and Hearing Research. 10.1044/jshr.3303.540 [DOI] [PubMed] [Google Scholar]
- Gierut JA, Elbert M, & Dinnsen DA (1987). A functional analysis of phonological knowledge and generalization learning in misarticulating children. Journal of Speech and Hearing Research. 10.1044/jshr.3004.432 [DOI] [PubMed] [Google Scholar]
- Gierut Judith A., & Morrisette ML (2011). Effect size in clinical phonology. Clinical Linguistics and Phonetics, 25(11–12), 975–980. 10.3109/02699206.2011.601392 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gierut Judith A., Morrisette ML, Hughes MT, & Rowland S (1996). Phonological Treatment Efficacy and Developmental Norms. Language Speech and Hearing Services in Schools, 27(3), 215. 10.1044/0161-1461.2703.215 [DOI] [Google Scholar]
- Gierut Judith A, Elbert M, & Dinnsen DA (1987). A functional analysis of phonological knowledge and generalization learning in misarticulating children. Journal of Speech and Hearing Research, 30(4), 462–479. http://jslhr.pubs.asha.org/article.aspx?articleid=1778354 [DOI] [PubMed] [Google Scholar]
- Gierut Judith A, Morrisette M. ichel. L., Hughes MT, & Rowland S (1996). Phonological treatment efficacy and developmental norms. Language, Speech, and Hearing Services in Schools, 27(3), 215–230. [Google Scholar]
- Gierut Judith A, Morrisette ML, & Ziemer SM (2010). Nonwords and Generalization in Children With Phonological Disorders. Am J Speech Lang Pathol, 19(2), 167–177. 10.1044/1058-0360(2009/09-0020) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldman R, & Fristoe M (2000). Goldman Fristoe 2 Test of Articulation (Second). American Guidance Service. [Google Scholar]
- Guenther FH, Espy-Wilson CY, Boyce SE, Matthies ML, Zandipour M, & Perkell JS (1999). Articulatory tradeoffs reduce acoustic variability during American English /r/ production. The Journal of the Acoustical Society of America, 105(5), 2854–2865. 10.1121/1.426900 [DOI] [PubMed] [Google Scholar]
- Hagood L, & Dunn C (1985). Self-monitoring in phonological acquisition. Paper Presented at the Child Phonology Meeting, Purdue University, West Lafayette. [Google Scholar]
- Hoffman PR (1983). Interallophonic generalization of /r/ training. Journal of Speech & Hearing Disorders, 48(2), 215–221. http://jshd.asha.org/cgi/content/abstract/48/2/215 [DOI] [PubMed] [Google Scholar]
- Koegel LK, Koegel RL, & Ingham JC (1986a). Programming rapid generalization of correct articulation through self-monitoring procedures. Journal of Speech & Hearing Disorders, 51(1), 24–32. http://jshd.asha.org/cgi/content/abstract/51/1/24 [DOI] [PubMed] [Google Scholar]
- Koegel LK, Koegel RL, & Ingham JC (1986b). Programming Rapid Generalization of Correct Articulation through Self-Monitoring Procedures. J Speech Hear Disord, 51(1), 24–32. http://jshd.asha.org/cgi/content/abstract/51/1/24 [DOI] [PubMed] [Google Scholar]
- Li F, Edwards J, & Beckman ME (2009). Contrast and covert contrast: The phonetic development of voiceless sibilant fricatives in English and Japanese toddlers. Journal of Phonetics, 37(1), 111–124. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Maxwell EM, & Weismer G (1982). The contribution of phonological, acoustic, and perceptual techniques to the characterization of a misarticulating child’s voice contrast for stops. Applied Psycholinguistics, 3(1), 29–43. [Google Scholar]
- McAllister Byun T, Hitchcock ER, & Ortiz JA (2015). Challenge Ultrasound (Version 1.585) [Computer Software] (v. 1.585). [Google Scholar]
- McAllister T, Hitchcock ER, & Ortiz JA (2020). Computer-assisted challenge point intervention for residual speech errors. Perspectives of the ASHA Special Interest Groups, 1–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Miccio AW (2002). Clinical problem solving: Assessment of phonological disorders. American Journal of Speech-Language Pathology, 11(3), 221–229. 10.1044/1058-0360(2002/023) [DOI] [Google Scholar]
- Mielke J, Baker A, & Archangeli D (2016). Individual-level contact limits phonological complexity: Evidence from bunched and retroflex /ɹ/. Language, 92(1), 101–140. 10.1353/lan.2016.0019 [DOI] [Google Scholar]
- Powell J, & McReynolds L (1969). A procedure for testing position generalization from articulation training. Journal of Speech, Language, and Hearing Research, 12(3), 629–645. 10.1044/jshr.1203.629 [DOI] [PubMed] [Google Scholar]
- Powell TW (1991). Planning for Phonological Generalization: An Approach to Treatment Target Selection. Am J Speech Lang Pathol, 1(1), 21–27. http://ajslp.asha.org/cgi/content/abstract/1/1/21 [Google Scholar]
- Preston JL, Hitchcock ER, & Leece MC (2020). Auditory Perception and Ultrasound Biofeedback Treatment Outcomes for Children With Residual /ɹ/ Distortions: A Randomized Controlled Trial. 10.23641/asha [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preston JL, McAllister T, Phillips E, Boyce S, Tiede M, Kim JS, & Whalen DH (2018). Treatment for residual rhotic errors with high- and low-frequency ultrasound visual feedback: A single-case experimental design. Journal of Speech, Language, and Hearing Research, 61(8), 1875–1892. 10.1044/2018_JSLHR-S-17-0441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preston JL, Benway NR, Leece MC, Hitchcock ER, & McAllister T (2020). Tutorial: Motor-Based Treatment Strategies for/r/Distortions. Language, Speech, and Hearing Services in Schools, 51(4), 966–980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preston JL, McCabe P, Rivera-Campos A, Whittle JL, Landry E, & Maas E (2014). Ultrasound visual feedback treatment and practice variability for residual speech sound errors. Journal of Speech Language and Hearing Research, 57(6), 2102–2115. 10.1044/2014_JSLHR-S-14-0031 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Recasens D, & Espinosa A (2005). Articulatory, positional and coarticulatory characteristics for clear /l/ and dark /l/: evidence from two Catalan dialects. Journal of the International Phonetic Association, 35(1), 1–25. https://doi.org/DOI: 10.1017/S0025100305001878 [DOI] [Google Scholar]
- Rvachew S, Nowak M, & Cloutier G (2004). Effect of phonemic perception training on the speech production and phonological awareness skills of children with expressive phonological delay. American Journal of Speech-Language Pathology, 13(3), 250–263. 10.1044/1058-0360(2004/026) [DOI] [PubMed] [Google Scholar]
- Shriberg LD, Flipsen P ., Karlsson HB ., & McSweeny JL (2001). Acoustic phenotypes for speech-genetics studies: an acoustic marker for residual /ɝ/ distortions. Clinical Linguistics and Phonetics, 15(8), 631–650. [DOI] [PubMed] [Google Scholar]
- Shriberg LD, & Kwiatkowski J (1987). A retrospective study of spontaneous generalization in speech-delayed children. Language, Speech, and Hearing Services in Schools, 18(2), 144–157. 10.1044/0161-1461.1802.144 [DOI] [Google Scholar]
- Sproat Richard & Fujimura O (1993). Allophonic variation in English /l/ and its impact for phonetic implementation. Journot of Phonetics, 291–311. [Google Scholar]
- Sugden E, Lloyd S, Lam J, & Cleland J (2019). Systematic review of ultrasound visual biofeedback in intervention for speech sound disorders. International Journal of Language & Communication Disorders, 54(5), 705–728. [DOI] [PubMed] [Google Scholar]
- Telemed. (n.d.). EchoBlaster 128. Telemed. [Google Scholar]
- Tyler AA, Edwards ML, & Saxman JH (1990). Acoustic validation of phonological knowledge and its relationship to treatment. Journal of Speech and Hearing Disorders, 55(2), 251–261. 10.1044/jshd.5502.251 [DOI] [PubMed] [Google Scholar]
- Tyler AA, Figurski GR, & Langsdale T (1993). Relationships between acoustically determined knowledge of stop place and voicing contrasts and phonological treatment progress. Journal of Speech Language and Hearing Research, 36(4), 746. 10.1044/jshr.3604.746 [DOI] [PubMed] [Google Scholar]
- Wiig EH, Semel EM, & Secord W (2013). CELF-5 : Clinical Evaluation of Language Fundamentals. In Clinical Evaulation of Language Fundamentals (Fifth). Pearson. [Google Scholar]