

Abstract
Objectives.
We intended to assess the effectiveness of all three FDA approved COVID-19 vaccines at preventing SARS-CoV-2 infection and COVID-19 hospitalization in a large cohort of individuals on immunosuppressants for a diverse range of conditions.
Methods.
We studied the effectiveness of BNT162b2 (Pfizer–BioNTech), mRNA-1273 (Moderna) and Ad26.COV2.S (Johnson & Johnson–Janssen) vaccines among individuals who take immunosuppressants (including disease-modifying antirheumatic drugs (DMARD), and glucocorticoids) by comparing vaccinated (n=97,688) and unvaccinated (n=42,094) individuals in the Michigan Medicine healthcare system from January 1 to December 7, 2021, using Cox proportional hazards modelling with time-varying covariates.
Results.
Among vaccinated and unvaccinated individuals, taking immunosuppressants increased the risk of SARS-CoV-2 infection (adjusted hazard ratio[aHR]=2.17, 95% CI: [1.69-2.79] for fully vaccinated and aHR=1.40, 95% CI: [1.07-1.83] for unvaccinated). Among individuals taking immunosuppressants we found: (I) vaccination reduced the risk of SARS-CoV-2 infection (aHR=0.55, 95% CI: [0.39-0.78]) (II) the BNT162b2 and mRNA-1273 vaccines were highly effective at reducing the risk of SARS-CoV-2 infection (n=2046, aHR=0.59, 95% CI: [0.38-0.91] for BNT162b2; n=2064, aHR=0.52, 95% CI: [0.33-0.82] for mRNA-1273); (III) with a smaller sample size (n=173), Ad26.COV2.S vaccine protection did not reach statistical significance (aHR=0.34, 95% CI: [0.09-1.30], p=0.17); (IV) receiving a booster dose reduced the risk of SARS-CoV-2 infection (aHR=0.42, 95% CI: [0.24-0.76]).
Conclusions.
The mRNA-1273 and BNT162b2 vaccines are effective in individuals who take immunosuppressants. However, individuals who are vaccinated but on immunosuppressants are still at higher risk of SARS-CoV-2 infection and COVID-19 hospitalization than the broader vaccinated population. Booster doses are effective and crucially important for individuals on immunosuppressants.
Keywords: SARS-CoV-2, COVID-19, Vaccination, Immunosuppressant, EHR
INTRODUCTION
The BNT162b2 (Pfizer–BioNTech), mRNA-1273 (Moderna), and Ad26.COV2.S (Johnson & Johnson–Janssen) vaccines are currently the only COVID-19 vaccines with emergency use authorization (EUA) from the US Food and Drug Administration (FDA) since December, 2020. All three vaccines were found to be safe and effective in clinical trials prior to approval. However, these trials excluded individuals who were immunocompromised (1,2,3). Since approval, the vaccines have been highly effective at preventing SARS-CoV-2 infection and severe illness (4), but there is still limited evidence regarding vaccine effectiveness in immunosuppressed individuals. Studies have shown that COVID-19 vaccines have reduced immunogenicity in immunosuppressed individuals compared to immunocompetent individuals (5,6,7,8). In the limited epidemiological research thus far, the approved vaccines appear to be less effective in immunosuppressed individuals relative to the general population (9)(10)(11). However, these studies were all limited by either small sample size, individuals with a specific condition, a single vaccine, or a short study period before the Delta variant became dominant and booster dose approved.
Our objective was to assess the effectiveness of all three FDA approved COVID-19 vaccines at preventing SARS-CoV-2 infection and hospitalization in a large cohort of individuals who were taking immunosuppressants [here after referred to as “immunosuppressed individuals”] compared to individuals not taking immunosuppressants [here after: “immunocompetent individuals”] for a diverse range of conditions. We reviewed electronic health records (EHR) at Michigan Medicine from January 1 to December 7, 2021. On August 12th, 2021, the CDC recommended a booster dose 28 days following their second dose for immunocompromised of the mRNA-1273 and BNT162b2 vaccines (12). Thus, our study period covers the Delta variant and provided sufficient follow-up data to study the effect of booster dose of mRNA vaccines for immunosuppressed individuals.
An immunosuppressed individual was defined as anyone taking conventional synthetic disease-modifying antirheumatic drugs (csDMARDs), targeted synthetics DMARDs(tsDMARDs), biologic DMARDs (bDMARDs), or glucocorticoids (see Supplement for a complete list of medications) for at least 6 months prior to the baseline date. Immunocompetent individuals were defined as those who did not take any immunosuppressants for at least 6 months prior to the baseline date. A booster dose for immunosuppressed individuals was defined as a third dose for BNT162b2 and mRNA-1273 recipients or a second dose for Ad26.COV2.S recipients. We made comparisons to evaluate vaccine effectiveness in immunosuppressed subjects. We also compared vaccine effectiveness among different types of immunosuppressants and conducted sensitivity analyses by excluding cancer patients who might be immunosuppressed due to disease or cancer treatment.
METHODS
Patient Selection.
Using the CDC definition, we defined an individual as fully vaccinated two weeks after a second dose of the BNT162b2 or mRNA-1273 vaccine or two weeks after a single dose of the Ad26.COV2.S vaccine (13). There were a total of 195,581 individuals in the EHR system who had an active primary care physician (UM-PCP) at Michigan Medicine and had been seen at a UM primary care location within the past 18 months. We excluded 41,062 individuals who were under 18, partially vaccinated, had a prior history of COVID-19, or had received a vaccine not approved in the US. A total of 154,519 individuals were included in the final analysis. Baseline date was defined as the date of full vaccination for vaccinated individuals, and January 1st, 2021, for unvaccinated individuals. The study was approved by the University of Michigan Institutional Review Board (HUM00164771) with a waiver of consent given the use of de-identified electronic health record data.
Time-to-event Outcomes and Covariates.
The primary outcomes were SARS-CoV-2 infections or COVID-19 hospitalization from January 1 to December 7, 2021. We identified SARS-CoV-2 infection based on laboratory test results and the 10th version International Classification of Diseases (ICD-10) code U07.1. Date of infection was identified using test collection date where possible, and diagnosis date where test date was not available. COVID-19 hospitalization was identified using chart review (n=51) where data was available and using ICD-10 codes (n=171) J12.82, M35.81, and J18 where chart review data was not available. Detailed criteria are provided in Supplement 1. Demographics included age, gender and race. Charlson Comorbidity Index (CCI) (14) was calculated from ICD-10 diagnosis codes within one year before the baseline date. We did not have sufficient follow-up to assess the effect of a booster dose in the immunocompetent group. Therefore, we censored individuals at the date of receiving a third dose for BNT162b2 and mRNA-1273 recipients or a second dose for Ad26.COV2.S recipients in the analysis including immunocompetent subjects.
Statistical Analysis.
We assessed the effectiveness of the vaccines by comparing fully vaccinated and unvaccinated individuals within the immunosuppressed and immunocompetent groups, based on two time scales: (1) based on calendar time, and (2) based on time from vaccination. We also assessed the effectiveness of a booster dose in immunosuppressed individuals using calendar time.
Calendar date analysis.
We used data from April 1 to December 7 to compare vaccine effectiveness and data from August 12 to December 7 to compare effect of booster dose of vaccine. The later start date was necessary to compare vaccine groups in the same time period. The Ad26.COV2.S vaccine was not approved for use until late February, meaning there was an insufficient number of individuals fully vaccinated with Ad26.COV2.S until April. The Kaplan-Meier method was used to estimate cumulative incidence curves for each group. In this analysis, the vaccinated individuals were considered unvaccinated until they received their first dose. A Cox model with a time-varying covariate (i.e., full vaccination or booster dose) was used to estimate the effect after controlling for age (under 31, 31-50, 51-64, or over 65), gender (male vs. female), race (Caucasian, African American, or other/unknown), and CCI (0, 1-2, 3-4, or 5+).
Time-from-vaccination analysis.
In this analysis, we used data from January 1st to December 7th, 2021, to assess the effectiveness of each vaccine based on time from vaccination. The effectiveness of the vaccine in immunocompetent and immunosuppressed individuals was assessed using time-to-event outcomes, defined as the time from full vaccination to SARS-CoV-2 infection or COVID-19 hospitalization, analyzed separately. The Kaplan-Meier method was used to estimate the cumulative incidence of SARS-CoV-2 infection and hospitalized infection and the log-rank test was used for comparisons between groups. Multivariable Cox regression models were used to compare groups, adjusting for age, gender, race, and CCI. To avoid the complexity of selecting a baseline date for these individuals, unvaccinated individuals were not included in this analysis.
In the Cox analyses, we reported adjusted hazard ratios (aHR), 95% confidence interval (CI), and p-value. To quantify the relative difference in risk between vaccines, we also estimated the covariate-adjusted cumulative incidence of SARS-CoV-2 infections in each group to assess the absolute difference in risk between vaccines. Specifically, we created a pseudo-population of identical population characteristics as the study individuals for each group and then averaged the predicted values of cumulative incidence. All statistical analyses were performed using R v4.0.2 (R Core Team, Vienna).
RESULTS
Patient Characteristics.
The characteristics of fully vaccinated immunosuppressed individuals (n=4,283), unvaccinated immunosuppressed individuals (n=1,253), fully vaccinated immunocompetent individuals (n=93,405) and unvaccinated immunocompetent individuals (n=40,841) are shown in Table 1. The median age was 59 for fully vaccinated immunosuppressed individuals, 49 for unvaccinated immunosuppressed individuals, 52 for fully vaccinated immunocompetent individuals, and 39 for unvaccinated immunocompetent individuals. The study population was majority female (63.9% and 62.2% in the immunosuppressed group for fully vaccinated and unvaccinated, respectively; 58% and 57.2% in the immunocompetent group for fully vaccinated and unvaccinated, respectively); and predominantly white (80.8% and 77.5% in the immunosuppressed group for fully vaccinated and unvaccinated, respectively; 78% and 71.7% in the immunosuppressed group for fully vaccinated and unvaccinated, respectively). The gender and race distributions were well balanced among the four groups. In the fully vaccinated group, the distribution of vaccine type was well balanced between immunosuppressant and immunocompetent individuals.
Table 1.
Patient characteristics.
| Characteristic | Fully vaccinated group (Case group) N = 97688 | Unvaccinated group (Control group) N = 42094 | ||
|---|---|---|---|---|
| Immunosuppressed, N = 4283 (4.4%) |
Immunocompetent, N = 93405 (95.6%) |
Immunosuppressed, N = 1253 (3.0%) |
Immunocompetent, N = 40841 (97.0%) |
|
| Age Median (IQR) | 59 (46 – 69) | 52(36 – 65) | 49 (35 – 62) | 39 (28 – 54) |
| Gender No. (%) | ||||
| - Male | 1591 (37.1%) | 39814 (42.6%) | 474 (37.8%) | 17472 (42.8%) |
| - Female | 2692 (63.9%) | 53588 (58.0%) | 779 (62.2%) | 23369 (57.2%) |
| Race No. (%) | ||||
| - Caucasian | 3462 (80.8%) | 72872 (78.0%) | 971 (77.5%) | 29275 (71.7%) |
| - African American | 446 (10.4%) | 6910 (7.4%) | 189 (15.1%) | 5758 (14.1%) |
| - Other/Unknown | 375 (8.8%) | 13623 (14.6%) | 93 (7.4%) | 5808 (14.2%) |
| Vaccine Type No. (%) | ||||
| - BNT162b2 | 2046 (47.8%) | 53178 (56.9%) | N/A | N/A |
| - mRNA-1273 | 2064 (48.2%) | 35256 (37.7%) | N/A | N/A |
| - Ad26.COV2.S | 173 (4.1%) | 4971 (5.4%) | N/A | N/A |
| SARS-CoV-2 infections No. (%) | 119 (2.8%) | 1146 (1.3%) | 85 (6.8%) | 1470 (3.6%) |
| COVID-19 hospitalizations No. (%) | 15 (0.35%) | 45 (0.05%) | 7 (0.56%) | 155 (0.38%) |
Compare Risk of Infection between Immunosuppressant and Immunocompetent Individuals.
Among fully vaccinated and unvaccinated individuals, immunosuppressed individuals had a higher risk of SARS-CoV-2 infection (p < 0.001 by log-rank; Figure 1A) compared to immunocompetent individuals. Results remain significant after adjusting for age, gender, race, and CCI in vaccinated individuals (aHR=2.17, 95% CI:[1.69-2.79], p<0.0001) and unvaccinated individuals (aHR=1.40, 95% CI:[1.07-1.83], p=0.0075) We also found that among fully vaccinated individuals, taking immunosuppressants led to a higher risk of COVID-19 hospitalization (aHR=4.86, 95% CI: [2.24-10.56], p<0.0001).
Figure 1.
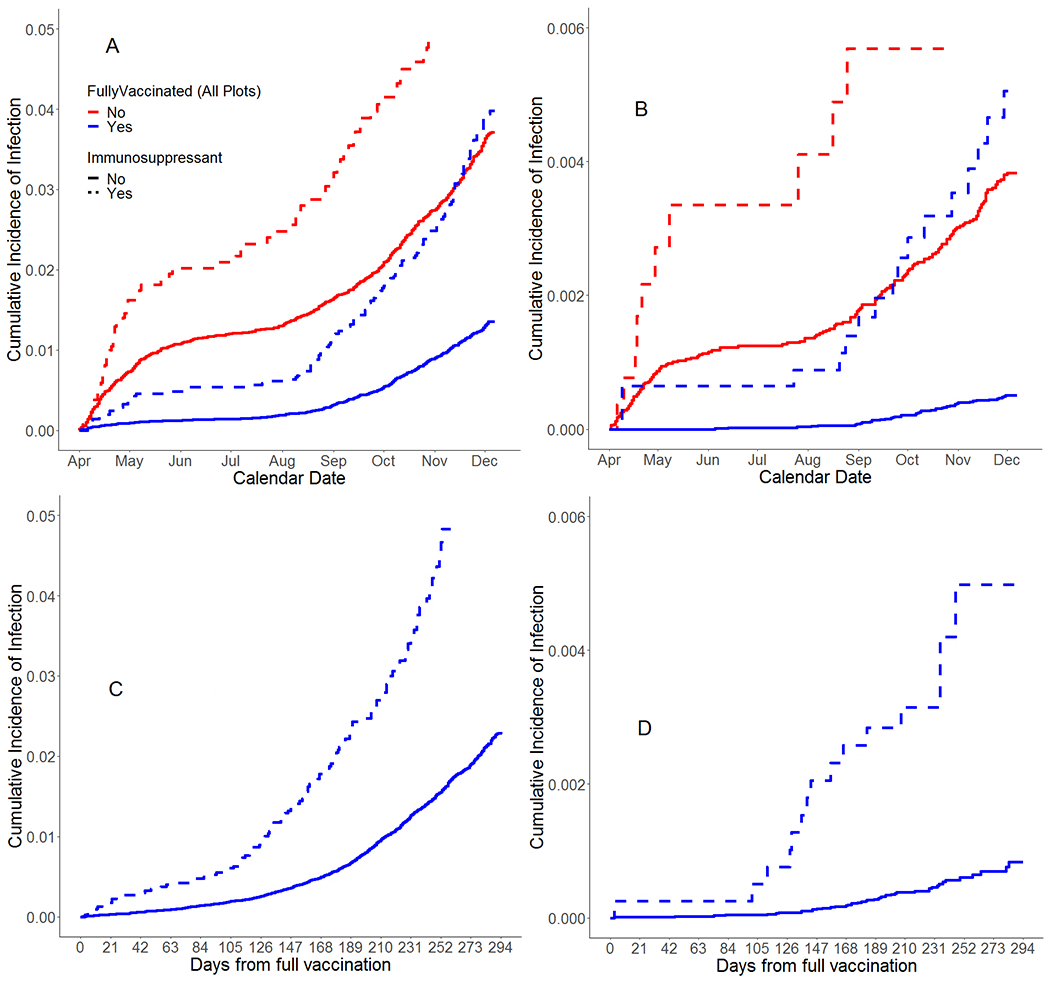
Unadjusted cumulative incidence curves of SARS-CoV-2 infection (A) and COVID-19 hospitalization (B) based on calendar time. Unadjusted CI curves of SARS-CoV-2 infection (C) and COVID-19 hospitalization (D) based on vaccination time.
Vaccine Effectiveness in Immunosuppressed Individuals.
Based on the calendar time analysis, fully vaccinated immunosuppressed individuals had a lower incidence of SARS-CoV-2 infection and COVID-19 hospitalization compared to unvaccinated immunosuppressed individuals (p<0.001 by log-rank; Figure 1A, 1B). The result remained the same for the immunocompetent individuals. Vaccination reduced risk of infection in immunosuppressed individuals based on multivariable Cox regression adjusted for age, gender, race, and CCI (aHR=0.55, 95% CI: [0.39-0.78], p<0.0001). The result remained the same for the immunocompetent individuals (aHR=0.35, 95% CI: [0.32-0.39], p<0.0001; Table 2). Full vaccination was associated with lower risk for COVID-19 hospitalization for immunocompetent individuals (aHR=0.11, 95% CI: [0.07-0.16], p<0.0001); but it did not reach statistical significance for immunosuppressed individuals, which is likely due to low power (only 15 had COVID-19 hospitalization among them). We estimated the covariate-adjusted cumulative incidence of SARS-CoV-2 infections per 100,000 for April to June, July to September, and October to December to be 1423,1366, and 2753 for unvaccinated immunosuppressed individuals; 1020, 979, and 1978 for unvaccinated immunocompetent individuals; 785, 753, and 1525 for the fully vaccinated immunosuppressed individuals; and 362, 348, and 705 for the fully vaccinated immunocompetent individuals, respectively.
Table 2.
Multivariable Cox regression for comparing immunosuppressed vs immunocompetent group based on calendar time
| SARS-CoV-2 infections | COVID-19 hospitalization | |||
|---|---|---|---|---|
| Variable | HR (95% CI) | p-value | HR (95% CI) | p-value |
| Unvaccinated (Immunosuppressed vs Immunocompetent) | 1.398 (1.068 – 1.829) | 0.0075 | 0.951 (0.435 – 2.080) | 0.9984 |
| Fully vaccinated (Immunosuppressed vs Immunocompetent) | 2.173 (1.690 – 2.794) | < 0.0001 | 4.861 (2.238 – 10.56) | < 0.0001 |
| Immunocompetent (Fully vaccinated vs Unvaccinated) | 0.354 (0.319 – 0.392) | < 0.0001 | 0.105 (0.067 – 0.162) | < 0.0001 |
| Immunosuppressed (Fully vaccinated vs Unvaccinated) | 0.550 (0.387 – 0.781) | 0.0001 | 0.534 (0.196 – 1.452) | 0.3724 |
| Age | ||||
| - Under 31 | Ref | Ref | Ref | Ref |
| - 31 – 50 | 1.497 (1.351 – 1.659) | < 0.0001 | 1.560 (0.970 – 2.509) | 0.0668 |
| - 51 – 64 | 1.481 (1.324 – 1.657) | < 0.0001 | 3.119 (1.961 – 4.961) | < 0.0001 |
| - Over 65 | 1.243 (1.096 – 1.411) | 0.0007 | 4.550 (2.829 – 7.320) | < 0.0001 |
| Gender | ||||
| - Female | Ref | Ref | Ref | Ref |
| - Male | 0.864 (0.804 – 0.929) | < 0.0001 | 1.419 (1.109 – 1.816) | 0.0054 |
| Race | ||||
| - Caucasian | Ref | Ref | Ref | Ref |
| - African American | 0.867 (0.774 – 0.972) | 0.0147 | 1.408 (0.995 – 1.991) | 0.0531 |
| - Other/unknown | 0.548 (0.481 – 0.624) | < .0001 | 0.875 (0.570 – 1.341) | 0.5397 |
| Charlson Comorbidity Index | ||||
| - >= 5 | Ref | Ref | Ref | Ref |
| - 3 – 4 | 0.876 (0.712 – 1.078) | 0.2118 | 0.478 (0.290 – 0.791) | 0.0040 |
| - 1 – 2 | 0.699 (0.587 – 0.832) | <0.0001 | 0.433 (0.293 – 0.640) | < 0.0001 |
| - 0 | 0.468 (0.396 – 0.554) | <0.0001 | 0.187 (0.126 – 0.276) | <0.0001 |
Based on the days-from-vaccination analysis, immunosuppressed individuals had a higher incidence of SARS-CoV-2 infection and COVID-19 hospitalization compared to immunocompetent individuals (p< 0.001 by log-rank; Figure 1C, 1D). The immunosuppressed individuals remained at a higher risk of SARS-CoV-2 infection (aHR=2.41, 95% CI: [1.98-2.92], p<.0001) and COVID-19 hospitalization (aHR=3.47, 95% CI: [1.89-6.37], p<.0001) in multivariable Cox regression adjusted for age, gender, race, and CCI. We estimated the covariate-adjusted cumulative incidence of SARS-CoV-2 infections per 100,000 for 3-month, 6-month, and 9-month after full vaccination to be 362, 1438, and 4396 for immunosuppressed individuals; and 151, 601, and 1855 for immunocompetent individuals, respectively.
Vaccine Effectiveness by Vaccine Type in Immunosuppressed individuals.
In the analysis compared the three vaccines with unvaccinated controls, we found that all three vaccines were highly effective at preventing SARS-CoV-2 infection and COVID-19 hospitalization for immunocompetent individuals. For immunosuppressed individuals, there was a significantly lower risk of SARS-CoV-2 infection compared to unvaccinated control for BNT162b2 recipients (aHR=0.59, 95% CI: [0.38-0.91], p=0.0098; Figure 2) and mRNA-1273 recipients (aHR=0.52, 95% CI: [0.33-0.82], p=0.0015); but we did not find statistically significant vaccine protection for the much smaller sample of Ad26.COV2.S recipients (aHR=0.34, 95% CI: [0.09-1.30], p=0.17). It is likely that this effect didn’t reach statistical significance due to low power. Given the estimated HR of 0.35 and current sample size, we found that the power is only 35% at a 0.05 significance level, using a two-sided test based on Cox proportional hazards regression. Because of the small sample size and number of events, there was insufficient statistical certainty when comparing vaccine effectiveness against COVID-19 hospitalizations for immunosuppressed individuals.
Figure 2.
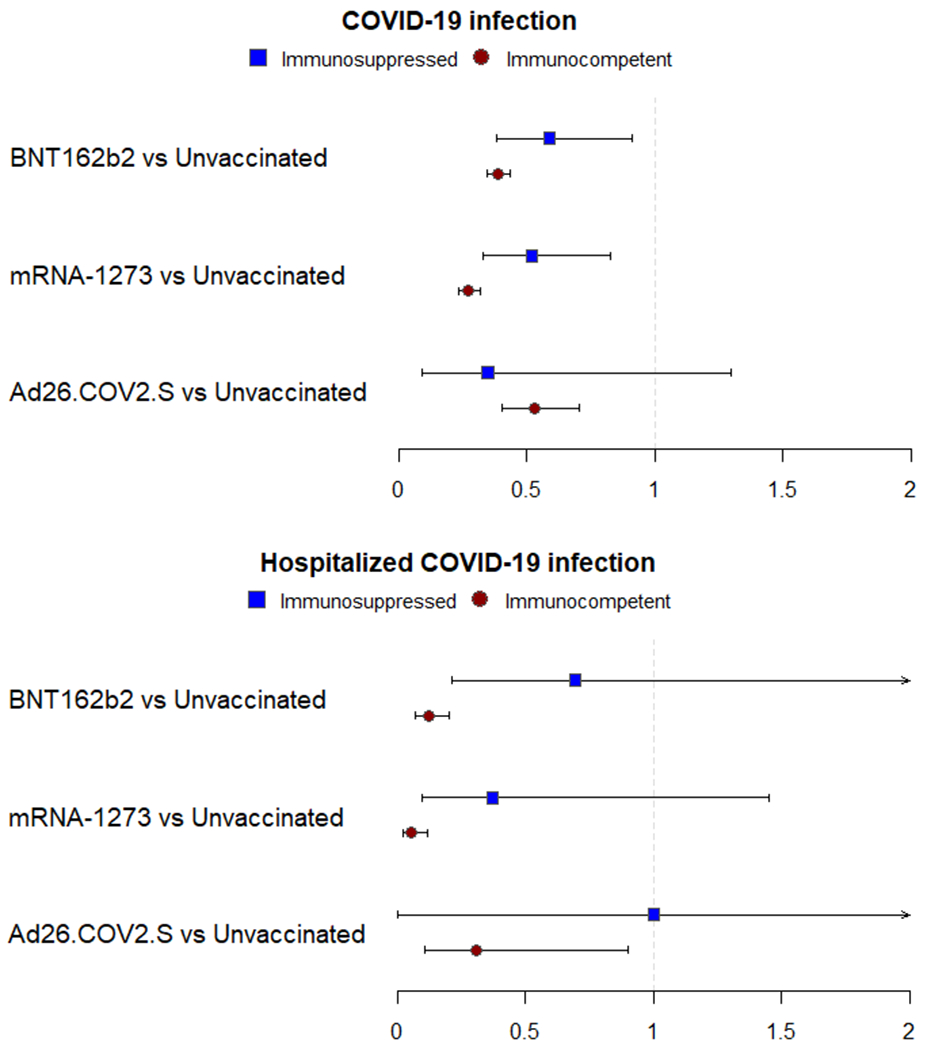
Hazard ratios for SARS-CoV-2 infection and COVID-19 hospitalization for each vaccine group compared to the unvaccinated group among immunosuppressed and immunocompetent individuals. Comparisons using multivariable Cox Model adjusting for age, gender, race, and CCI.
Effectiveness of Booster Dose in Immunosuppressed Individuals.
Figure 1A shows that the incidence of SARS-CoV-2 infection increased dramatically for fully vaccinated immunosuppressed individuals after late August, and that their cumulative incidence increased over the unvaccinated immunocompetent individuals by late November, suggesting their immunity waned faster than the general population. In this analysis, individuals were censored at the date of receiving a booster dose; therefore, we conducted a further analysis to study the effectiveness of the booster dose in immunosuppressed individuals.
We compared individuals who had a booster dose (n=1650, 38.5%) versus individuals before taking or who did not take the booster dose (n=2633, 61.5%). We found that fully vaccinated immunosuppressed individuals who had a booster dose had a lower incidence of SARS-CoV-2 infection compared to fully vaccinated immunosuppressed individuals who did not (p < 0.001 by log-rank; Figure 3). This result remained significant in multivariable Cox regression after adjusting for age, gender, race, and CCI (aHR=0.42, 95% CI: [0.24-0.76], p=0.0037).
Figure 3.
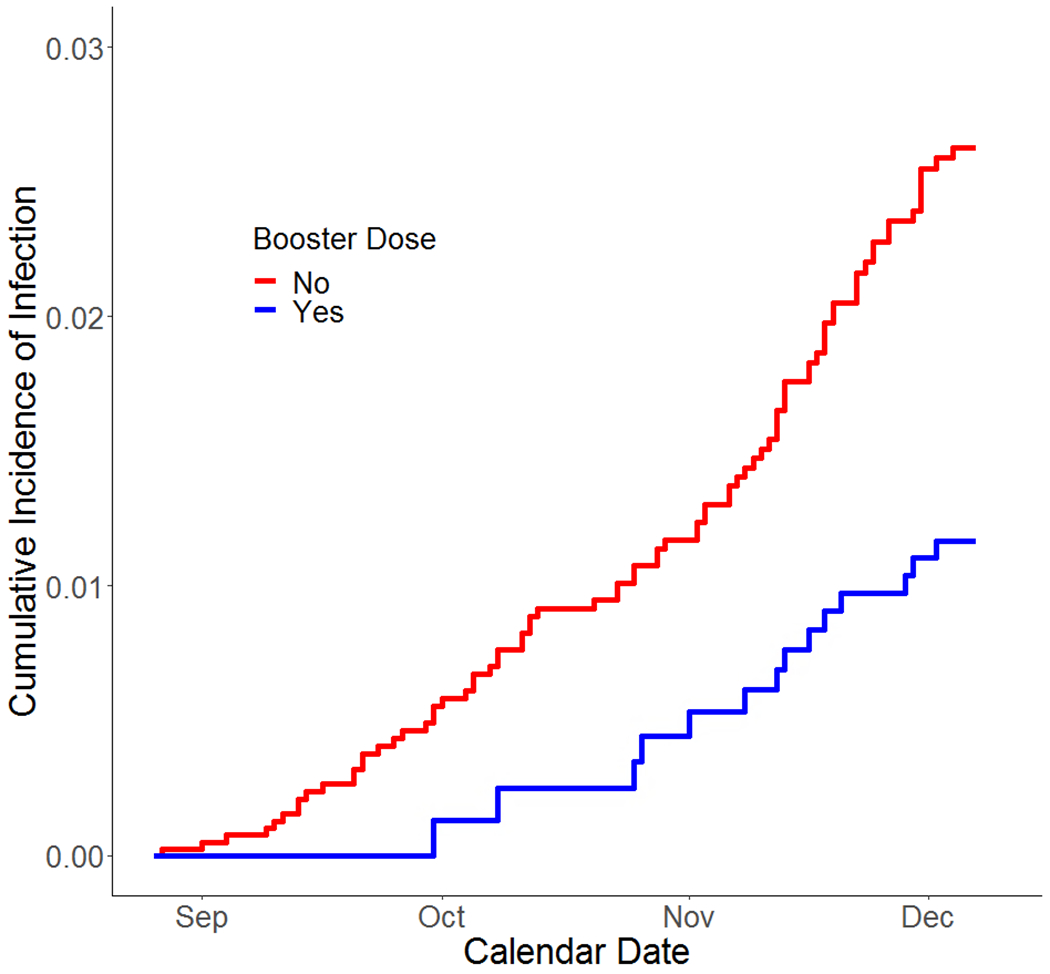
Unadjusted CI curves of SARS-CoV-2 infection in immunosuppressed individuals who took a booster dose or not based on calendar time.
Sensitivity Analysis.
We studied a comprehensive list of immunosuppressant drugs used to treat patients with autoimmune disease or who had transplantation. However, individuals who did not take these medications might also be in an immunosuppressive condition; for instance, cancer individuals who were immunosuppressed due to the disease or taking immunosuppressive cancer therapy. In addition, transplant patients may have lower exposure to SARS-CoV-2 infection due to shielding or risk avoidant behavior. Thus, we conducted sensitivity analyses by excluding patients who had these conditions.
We first excluded patients who had a history of cancer, who were identified from the ICD-10 diagnosis codes in the one year before the baseline date (n=750 (13.6%) immunosuppressed and n=207 (3.9%) immunocompetent). We further excluded patients who had a transplant (n=550 (9.9%) immunosuppressed and n=500 (0.4%) immunocompetent) and performed the same analyses again. Conclusions remained the same on vaccine effectiveness and comparisons between immunosuppressed and immunocompetent individuals based on the two time scales (data not shown).
Vaccine Effectiveness by Immunosuppressant Type.
Among the 4283 fully vaccinated immunosuppressed individuals, there were 674 (15.7%) individuals who were only treated with csDMARDs, 265 (6.2%) individuals who were only treated with bDMARDs (combined tsDMARDs and bDMARDs), 210 (4.9%) individuals who were treated with both csDMARDs and bDMARDs, and 1528 (35.7%) individuals who were only treated with glucocorticoids. We excluded the individuals who were treated with both DMARDs and glucocorticoids (1606, 37.5%). Based on the calendar time analysis and time-from-vaccination analysis, we found no significant differences in SARS-CoV-2 infection between these types of immunosuppressants. (Figure in Supplement)
DISCUSSION
We found that immunosuppressed individuals who had received one of the three approved COVID-19 vaccines were at substantially lower risk of SARS-CoV-2 infection compared to those who were unvaccinated. Specifically, we found that BNT162b2 and mRNA-1273 vaccines were highly effective at preventing SARS-CoV-2 infection in immunosuppressed individuals. However, due to the small sample size, the statistical power to detect the effectiveness of the Ad26.COV2.S vaccine was only 35%; if the sample size was increased by 10 times (close to the same size for BNT162b2 or mRNA-1273), the power would be over 95%. Overall, these results are highly reassuring, given concerns that reduced immune response would lead to lower vaccine effectiveness in immunosuppressed individuals and the lack of data from the clinical trials conducted prior to vaccine approval. We also found that booster doses were highly effective at reducing risk of infection and hospitalization within this group. Giving a booster dose to immunosuppressed individuals who have not yet received one is crucially important.
We also observed an increase in incidence of infection among all individuals after July 1st, once the Delta variant became the dominant variant in the United States (see Figure 1A). This increase appears to be larger for vaccinated immunosuppressed individuals compared to other vaccinated individuals. Based on the analysis using time from vaccination (see Figure 1C comparing immunocompetent and immunosuppressed individuals who are vaccinated), this could be explained by vaccine-induced immunity waning more quickly for immunosuppressed individuals. It is also possible that the Delta variant affected vaccine-induced immunity differently for immunosuppressed compared to immunocompetent individuals. Regardless of the explanation, this underlines the importance of immunosuppressed individuals receiving booster shots, as their immunity due to vaccination appears to be reduced later in the study period and is likely to wane further in the coming months. It also indicates that public health officials should expect that the immunity conferred by booster shots will wane more quickly for immunosuppressed individuals and incorporate this into decision-making regarding approval of additional booster doses in the future.
In late December 2021, the Omicron variant rapidly increased in prevalence and now accounts for a majority of new SARS-CoV-2 infections. Although this study did not cover Omicron infections, the conclusions for immunosuppressed individuals are likely to remain the same. Vaccines will offer protection, but lower immunity after vaccination and rapidly waning immunity will put them at higher risk of SARS-CoV-2 infection and COVID-19 hospitalization compared to immunocompetent individuals.
Limitations of this study include having data from a single health institution, and underestimation of SARS-CoV-2 infection due to limitations in testing and reporting of tests received at outside sites. EHR data has limitations such as inaccuracy and missingness. Our determination of disease (such as cancer and transplantation) and calculation of comorbidity scores relied on ICD-10 codes, which may prone to errors (15). CCI, which we used to capture comorbidities, is not necessarily a comprehensive metric for determining patient health and may miss some prognostic factors for SARS-CoV-2 infection. Despite this limitation, the CCI is more accurate than using individual ICD10 codes (16).
Immunosuppressed subjects might interact more with the health system compared to immunocompetent subjects due to treatment of their underlying condition and vulnerability to other health problems, leading to more complete infection data for this group. To reduce the bias caused by this issue, we defined the study cohort to individuals who had an active primary care physician at the University of Michigan.
Furthermore, immunosuppressants are prescribed for a wide variety of medical conditions such as autoimmune diseases, pulmonary fibrosis, gastrointestinal or endocrine disorders. As a result, the degree of immunosuppression and medical vulnerability is not homogenous across all immunosuppressed patients. We conducted sensitivity analyses by excluding certain conditions or procedures, such as cancer and transplantation, but cannot fully determine whether higher infection rates for immunosuppressed individuals are due to immunosuppressant medications or the underlying conditions they are used to treat.
Despite these limitations, our results provide important information on vaccines effectiveness in immunosuppressed individuals. Vaccines are highly effective at preventing SARS-CoV-2 infections in this group, despite reduced effectiveness relative to the broader population. It is crucial that immunosuppressed individuals take boosters as soon as possible as they remain at elevated risk of SARS-CoV-2 infection and COVID-19 hospitalization than other vaccinated individuals.
Supplementary Material
KEY MESSAGES:
What is already known about this subject?
-
1.
The BNT162b2 vaccine is effective in immunocompromised individuals.
-
2.
Immunocompromised individuals who were fully vaccinated are at a higher risk of SARS-CoV-2 infection compared to the wider vaccinated population.
What does this study add?
-
3.
The BNT162b2 and mRNA-1273 vaccines are effective in a wide range of individuals who take immunosuppressants, but vaccinated individuals in this group remain at higher risk compared to the wider vaccinated population.
-
4.
Booster doses are effective at preventing SARS-CoV-2 infections for individuals who take immunosuppressants.
How might this impact on clinical practice or future developments?
-
5.
Patients who take immunosuppressants should become fully vaccinated and get a booster dose to gain protection against SARS-CoV-2 infections.
ACKNOWLEDGMENTS and AFFILIATIONS
We thank the University of Michigan Data Office for assistance with data extraction from electronic medical records and Dr. Kirsten Herold for editing the writing.
Research reported in this publication was supported by the National Institute Of Allergy And Infectious Diseases of the National Institutes of Health under Award Number R01AI158543. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Footnotes
The authors have declared that no conflict of interest exists.
REFERENCES
- 1.Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. New England Journal of Medicine 2021; 384:403–416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. New England Journal of Medicine 2020; 383:2603–2615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Sadoff J, Gray G, Vandebosch A, et al. Safety and efficacy of single-dose Ad26.COV2.S vaccine against Covid-19. New England Journal of Medicine 2021; 384:2187–2201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.CDC. COVID-19 Vaccines Effectiveness. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/how-they-work.html. Updated Aug 16, 2021. Accessed Oct 28, 2021.
- 5.Boyarsky BJ, Werbel WA, Avery RK, et al. Antibody response to 2-dose SARS-COV-2 mRNA vaccine series in solid organ transplant recipients. JAMA. 2021;325(21):2204–2206. doi: 10.1001/jama.2021.7489 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hallett et al. SARS-CoV-2 messenger RNA vaccine antibody response and reactogenicity in heart and lung transplant recipients. The Journal of Heart and Lung Transplantation. 2021. 10.1016/j.healun.2021.07.026 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Deepak P, Kim W, Paley MA et al. Effect of Immunosuppression on the Immunogenicity of mRNA Vaccines to SARS-CoV-2: A Prospective Cohort Study. Ann Intern Med. 2021. Aug 31:M21–1757. doi: 10.7326/M21-1757. Epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Dooling K, Evidence to Recommendation Framework: An Additional Dose of mRNA COVID-19 Vaccine Following a Primary Series in Immunocompromised People. Advisory Committee on Immunization Practices. August 13, 2021. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2021-08-13/02-COVID-Dooling-508.pdf [Google Scholar]
- 9.Chodick Gabriel et al. , The Effectiveness of the Two-Dose BNT162b2 Vaccine: Analysis of Real-World Data, Clinical Infectious Diseases 2021; ciab438, 10.1093/cid/ciab438 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Khan Nabeel, Mahmud Nadim, Effectiveness of SARS-CoV-2 Vaccination in a Veterans Affairs Cohort of Patients with Inflammatory Bowel Disease With Diverse Exposure to Immunosuppressive Medications, Gastroenterology, Volume 161, Issue 3, 2021, Pages 827–836, ISSN 0016-5085, 10.1053/j.gastro.2021.05.044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Tenforde Mark W. et al. , Effectiveness of Severe Acute Respiratory Syndrome Coronavirus 2 Messenger RNA Vaccines for Preventing Coronavirus Disease 2019 Hospitalizations in the United States, Clinical Infectious Diseases 2021, ciab687, 10.1093/cid/ciab687 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.CDC. COVID-19 Vaccines for Moderately to Severely Immunocompromised People. https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations/immuno.html. Updated November 23, 2021. Accessed November 24, 2021.
- 13.CDC. Science Brief: COVID-19 Vaccines and Vaccination. https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/fully-vaccinated-people.html. Updated July 27, 2021. Accessed August 25, 2021.
- 14.Charlson ME, Pompei P, Ales KL, & MacKenzie CR A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. Journal of chronic diseases 1987;40(5), 373–383. [DOI] [PubMed] [Google Scholar]
- 15.Hersh WR, Weiner MG, Embi PJ, et al. Caveats for the use of operational electronic health record data in comparative effectiveness research. Med Care. 2013;51(8 suppl 3):S30–S37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Austin SR, Wong YN, Uzzo RG, Beck JR, Egleston BL. Why Summary Comorbidity Measures Such As the Charlson Comorbidity Index and Elixhauser Score Work. Med Care. 2015;53(9):e65–e72. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.