

Abstract
Cancer has become the most common cause of death in China. Owing to rapid economic development, improved livelihood, and shifts in risk factors, cancer epidemiology has experienced substantial changes during the past several decades. In this review, we aim to describe the current cancer epidemiology of the main types of cancer in China, report major risk factors associated with cancer development, and summarize the contributions of the Chinese government to controlling the cancer burden. A total of 4,064,000 new cases were diagnosed in China in 2016. The most frequent types are lung cancer (828,100; 20.4%), colorectal cancer (408,000; 10.0%), and gastric cancer (396,500; 9.8%). Lung (657,000; 27.2%), liver (336,400, 13.9%), and stomach (288,500; 12.0%) cancers are the 3 most deadly cancers in the general population. The 5-year survival rate for cancer has dramatically increased in recent decades. However, liver and particularly pancreatic cancers still have the poorest prognosis. The main modifiable risk factors associated with cancer development include infectious agents, smoking, alcohol consumption, obesity, unhealthful dietary habits, and inadequate physical activity. The Chinese government has made unremitting efforts to decrease the cancer burden, including cancer education and investment in cancer screening programs.
Keywords: Cancer burden, risk factor, prevention, China
Introduction
Cancer, with its chronic development and tendency to be fatal, has become one of the leading causes of death in China1. Over the past several decades, China has experienced groundbreaking economic development, transitioning from an agrarian economy to an economic superpower. The standard of living and health resources have dramatically improved, and lifestyles have become increasingly urbanized and westernized. In addition, the multiple levels of government in China have continually engaged in cancer prevention and control efforts, such as implementing educational programs and screening for harmful cancers. The patterns of cancer epidemiology have changed dramatically.
Cancer epidemiology information is critical for providing effective and timely guidance in establishing healthcare policies and intervention measures. Therefore, cancer epidemiology data require timely updating. In this review, we aim to describe the current trends in cancer epidemiology, report the relevant risk factors for various cancers, and highlight China’s efforts to ease the burden of cancer in recent decades.
To provide convincing evidence, we extracted relevant data from published articles in several electronic databases (e.g., PubMed, China National Knowledge Infrastructure, and Google Scholar), books, and official websites, such as the People’s Republic of China, the National Bureau of Statistics, National Health Commission of the People’s Republic of China, and the World Health Organization (WHO). Search terms included, but were not limited to, “cancer epidemiology”, “cancer burden”, “incidence”, “mortality”, “contribution”, “cancer prevention”, and “risk factors”.
Cancer epidemiology
Incidence trends
According to the estimates of the National Cancer Center (NCC) of China1, approximately 4,064,000 newly diagnosed cancer cases were reported in 2016, thus resulting in a crude incidence rate of 293.9/100,000. The age-standardized incidence rate (ASIR) in the world standard population for all cancer cases combined was 186.5/100,000. Men had a higher crude incidence rate or ASIR than women for most types of cancer (Figure 1). The most frequently diagnosed cancer types were those of the lung, colorectum, stomach, liver, and breast, accounting for 20.4%, 10.0%, 9.8%, 9.6%, and 7.5%, respectively, and representing 57.3% of all cancers combined (Table 1). The most common cancer in men was lung cancer (549,800; 24.6%), which was followed by liver cancer (288,800; 12.9%), stomach cancer (276,300; 12.4%), colorectal cancer (238,500; 10.7%), and esophageal cancer (184,500; 8.3%). In contrast, the most frequent malignancy in women was female breast cancer (306,000; 16.7%), and lung cancer (278,300; 15.2%) was the second most prevalent, and was followed by colorectal cancer (169,500; 9.3%) and thyroid cancer (152,600; 8.3%)1. The ratio of frequency is >1 for most cancers in men and women (excluding sex-specific malignancies, e.g., cancers of the prostate and female breast), except for cancers of the gallbladder, brain, and thyroid (0.9, 0.9, and 0.3, respectively). The highest ratio is for laryngeal cancer (10.7).
Figure 1.

Crude and age-standardized incidence of cancer by sex (A. female, B. male). Data were extracted from Cancer incidence and mortality in China, 20161.
Table 1.
The most frequent cancers in China by sex, 2016
| Site | Overall |
Men |
Women |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Cases | Percentage (%) | Rank | Cases | Percentage (%) | Rank | Cases | Percentage (%) | Rank | |
| All sites | 4,064,000 | 100.0 | – | 2,234,300 | 100.0 | – | 1,829,600 | 100.0 | – |
| Lung | 828,100 | 20.4 | 1 | 549,800 | 24.6 | 1 | 278,300 | 15.2 | 2 |
| Colon-rectum | 408,000 | 10.0 | 2 | 238,500 | 10.7 | 4 | 169,500 | 9.3 | 3 |
| Stomach | 396,500 | 9.8 | 3 | 276,300 | 12.4 | 3 | 120,200 | 6.6 | 5 |
| Liver | 388,800 | 9.6 | 4 | 288,800 | 12.9 | 2 | 100,000 | 5.5 | 7 |
| Female breast | 306,000 | 7.5 | 5 | – | – | – | 306,000 | 16.7 | 1 |
| Esophagus | 252,500 | 6.2 | 6 | 184,500 | 8.3 | 5 | 68,000 | 3.7 | 10 |
| Thyroid | 202,600 | 5.0 | 7 | 50,000 | 2.2 | 12 | 152,600 | 8.3 | 4 |
| All other sites | 173,600 | 4.3 | 8 | 90,900 | 4.1 | 6 | 82,700 | 4.5 | 8 |
| Cervix | 119,300 | 2.9 | 9 | – | – | – | 119,300 | 6.5 | 6 |
| Brain, CNS | 109,000 | 2.7 | 10 | 50,500 | 2.3 | 11 | 58,500 | 3.2 | 11 |
| Pancreas | 100,400 | 2.5 | 11 | 57,000 | 2.6 | 9 | 43,400 | 2.4 | 13 |
| Lymphoma | 89,900 | 2.2 | 12 | 51,600 | 2.3 | 10 | 38,300 | 2.1 | 14 |
| Leukemia | 85,800 | 2.1 | 13 | 49,400 | 2.2 | 13 | 36,400 | 2.0 | 15 |
| Bladder | 82,300 | 2.0 | 14 | 64,200 | 2.9 | 8 | 18,000 | 1.0 | 18 |
| Prostate | 78,300 | 1.9 | 15 | 78,300 | 3.5 | 7 | – | – | – |
| Kidney | 75,800 | 1.9 | 16 | 48,000 | 2.1 | 14 | 27,800 | 1.5 | 17 |
| Uterus | 71,100 | 1.7 | 17 | – | – | – | 71,100 | 3.9 | 9 |
| Ovary | 57,200 | 1.4 | 18 | – | – | – | 57,200 | 3.1 | 12 |
| Gallbladder | 55,700 | 1.4 | 19 | 26,400 | 1.2 | 17 | 29,300 | 1.6 | 16 |
| Lip, oral, cavity, and pharynx | 52,200 | 1.3 | 20 | 36,200 | 1.6 | 16 | 16,100 | 0.9 | 19 |
| Nasopharynx | 52,000 | 1.3 | 21 | 37,400 | 1.7 | 15 | 14,700 | 0.8 | 20 |
| Bone | 25,800 | 0.6 | 22 | 14,900 | 0.7 | 19 | 10,900 | 0.6 | 21 |
| Larynx | 25,700 | 0.6 | 23 | 23,500 | 1.1 | 18 | 2,200 | 0.1 | 24 |
| Other thoracic organs | 13,100 | 0.3 | 24 | 7,600 | 0.3 | 20 | 5,500 | 0.3 | 22 |
| Melanoma of skin | 7,000 | 0.2 | 25 | 3,500 | 0.2 | 21 | 3,500 | 0.2 | 23 |
| Testis | 3,400 | 0.1 | 26 | 3,400 | 0.2 | 22 | – | – | |
Cancer incidence and mortality in China, 20161.
The crude incidence rates for all cancers gradually increased in men and women from 2000 to 2015. However, the total cancer incidence rate in both sexes combined significantly decreased after age standardization2. Specifically, for both sexes, a downward trend in ASIR was seen for digestive tract cancer, including esophageal cancer, stomach cancer, and liver cancer. Lung cancer, colorectal cancer, stomach cancer, breast cancer, and thyroid cancer remained the most common cancers in China1,3.
Individually, the ASIR in men showed a stable trend over the past several decades. A substantial increase in prostate cancer incidence was observed, with an average annual percentage change of 7.1% from 2000 to 2016, particularly between 2000 and 2005 (annual percentage change of 12.5%)1. The incidence rates of leukemia and cancers of the colorectum, brain, pancreas, and bladder showed upward trends. Cancer incidence after age standardization was on a rise by 2.3% per year in women1. Trends for cancers of the esophagus, stomach, and liver steadily decreased during the same period. However, the ASIRs for colorectal cancer, uterine cancer, cervical cancer, and lung cancer have increased generally. Notably, the incidence of thyroid cancer rapidly increased, and its average annual percentage change was estimated to be 20.6% from 2007 to 20161.
Mortality trends
The cancer mortality ranking estimated by the NCC is shown in Table 2. In 2016, 2,413,500 cancer deaths were recorded in China, with a crude mortality rate of 174.6/100,000. The age-standardized mortality rate (ASMR) in the world standard population for all cancers combined was 105.2/100,000. Men had a significantly higher ASMR than women (138.1/100,000 vs. 74.0/100,000)1. The mortality rate by sex is shown in Figure 2. The highest numbers of cancer deaths were those for lung cancer (657,000; 27.2%), with a crude mortality rate of 47.5/100,000, liver cancer (336,400; 13.9%), stomach cancer (288,500; 12.0%), colorectal cancer (195,600; 8.1%), and esophageal cancer (193,900; 8.0%), representing 69.2% of all cancer deaths. Approximately 29.7% of all deaths from cancer were ascribed to lung cancer in men. The second most common cancer in men was liver cancer (249,600; 16.3%), which was followed by stomach cancer (200,200; 13.1%), esophageal cancer (142,300, 9.3%), and colorectal cancer (114,500; 7.5%). The leading causes of cancer death in women were lung cancer (202,300; 22.9%), stomach cancer (88,400; 10.0%), liver cancer (86,800; 9.8%), colorectal cancer (81,000; 9.2%), and breast cancer (71,700; 8.1%). The ratio of mortality of frequency for men to women was <1 for gallbladder cancer (0.9) and thyroid cancer (0.6), and the highest ratio was found for laryngeal cancer (7.4).
Table 2.
Leading causes of death in China by sex, 2016
| Site | Overall |
Men |
Women |
||||||
|---|---|---|---|---|---|---|---|---|---|
| Deaths | Percentage (%) | Rank | Deaths | Percentage (%) | Rank | Deaths | Percentage (%) | Rank | |
| All sites | 2,413,500 | 100.0 | – | 1,530,700 | 100.0 | – | 882,800 | 100.0 | – |
| Lung | 657,000 | 27.2 | 1 | 454,700 | 29.7 | 1 | 202,300 | 22.9 | 1 |
| Liver | 336,400 | 13.9 | 2 | 249,600 | 16.3 | 2 | 86,800 | 9.8 | 3 |
| Stomach | 288,500 | 12.0 | 3 | 200,200 | 13.1 | 3 | 88,400 | 10.0 | 2 |
| Colon–rectum | 195,600 | 8.1 | 4 | 114,500 | 7.5 | 5 | 81,000 | 9.2 | 4 |
| Esophagus | 193,900 | 8.0 | 5 | 142,300 | 9.3 | 4 | 51,600 | 5.8 | 6 |
| All other sites | 93,400 | 3.9 | 6 | 53,500 | 3.5 | 6 | 39,900 | 4.5 | 7 |
| Pancreas | 87,900 | 3.6 | 7 | 49,800 | 3.3 | 7 | 38,100 | 4.3 | 8 |
| Female breast | 71,700 | 3.0 | 8 | – | – | – | 71,700 | 8.1 | 5 |
| Brain, CNS | 58,500 | 2.4 | 9 | 32,600 | 2.1 | 9 | 25,900 | 2.9 | 11 |
| Leukemia | 55,700 | 2.3 | 10 | 32,400 | 2.1 | 10 | 23,200 | 2.6 | 12 |
| Lymphoma | 51,500 | 2.1 | 11 | 31,000 | 2.0 | 11 | 20,500 | 2.3 | 14 |
| Gallbladder | 41,400 | 1.7 | 12 | 19,500 | 1.3 | 14 | 22,000 | 2.5 | 13 |
| Cervix | 37,200 | 1.5 | 13 | – | – | – | 37,200 | 4.2 | 9 |
| Bladder | 33,700 | 1.4 | 14 | 26,200 | 1.7 | 12 | 7,500 | 0.9 | 18 |
| Prostate | 33,600 | 1.4 | 15 | 33,600 | 2.2 | 8 | – | – | – |
| Ovary | 27,200 | 1.1 | 16 | – | – | – | 27,200 | 3.1 | 10 |
| Kidney | 26,900 | 1.1 | 17 | 17,100 | 1.1 | 16 | 9,800 | 1.1 | 16 |
| Nasopharynx | 26,700 | 1.1 | 18 | 19,700 | 1.3 | 13 | 7,000 | 0.8 | 19 |
| Lip, oral, cavity, and pharynx | 25,800 | 1.1 | 19 | 18,900 | 1.2 | 15 | 6,900 | 0.8 | 20 |
| Bone | 18,400 | 0.8 | 20 | 10,700 | 0.7 | 18 | 7,700 | 0.9 | 17 |
| Uterus | 17,100 | 0.7 | 21 | – | – | – | 17,100 | 1.9 | 15 |
| Larynx | 14,300 | 0.6 | 22 | 12,500 | 0.8 | 17 | 1,700 | 0.2 | 23 |
| Thyroid | 8,300 | 0.3 | 23 | 3,100 | 0.2 | 20 | 5,200 | 0.6 | 21 |
| Other thoracic organs | 6,800 | 0.3 | 24 | 4,300 | 0.3 | 19 | 2,500 | 0.3 | 22 |
| Melanoma of skin | 3800 | 0.2 | 25 | 2,100 | 0.1 | 21 | 1,700 | 0.2 | 24 |
| Testis | 900 | 0.0 | 26 | 900 | 0.1 | 22 | – | – | – |
Cancer incidence and mortality in China, 20161.
Figure 2.

Crude and age-standardized mortality of cancer by sex (A. female, B. male). Data were extracted from Cancer incidence and mortality in China, 20161.
According to estimates from the National Bureau of Health Statistics, the 4 leading causes of death in China from 2000 to 2020 were cancer, heart conditions, cerebrovascular disease, and respiratory disease (Table 3). In urban areas, cancer remains the major cause of death, whereas in rural regions, it has overtaken respiratory diseases and become the leading cause of death4. Furthermore, the mortality rank for major cancer types has changed according to the 3 nationwide retrospective sampling surveys of causes of death5. Table 4 lists the 10 most common cancers in China over the past 3 periods (1973–1975, 1990–1992, and 2004–2005). In the first and second National Retrospective Sampling Survey of Death Causes, stomach cancer was the most deadly cancer (accounting for 23.0% and 23.2% of all cancer deaths, respectively). However, in the third National Retrospective Sampling Survey of Death Causes, lung cancer became the most common cause of death (accounting for 22.7% of all cancer deaths). The 5 leading causes of cancer-associated death have gradually become lung cancer, liver cancer, stomach cancer, esophageal cancer, and colorectal cancer6.
Table 3.
Leading causes of death in China
| Year | Rural (%) |
Urban (%) |
||||||
|---|---|---|---|---|---|---|---|---|
| Cancer | Heart conditions | Cerebrovascular disease | Respiratory disease | Cancer | Heart conditions | Cerebrovascular disease | Respiratory disease | |
| 2000 | 18.4 | 12.4 | 18.4 | 23.1 | 24.4 | 17.7 | 21.3 | 13.3 |
| 2001 | 17.7 | 13.1 | 19.0 | 22.5 | 24.9 | 17.6 | 20.4 | 13.4 |
| 2002 | 20.7 | 14.3 | 17.3 | 15.6 | 23.5 | 14.6 | 17.5 | 15.6 |
| 2003 | 25.3 | 12.0 | 23.8 | 18.7 | 25.5 | 14.4 | 20.0 | 14.6 |
| 2004 | 23.7 | 12.5 | 14.9 | 13.3 | 23.9 | 18.8 | 19.1 | 13.1 |
| 2005 | 20.3 | 11.8 | 21.2 | 23.5 | 22.9 | 17.9 | 21.2 | 12.6 |
| 2006 | 25.1 | 13.9 | 20.4 | 16.4 | 27.3 | 17.1 | 17.7 | 13.1 |
| 2007 | 24.8 | 14.8 | 20.6 | 17.2 | 28.5 | 16.3 | 18.0 | 13.1 |
| 2008 | 25.4 | 14.1 | 21.7 | 16.9 | 27.1 | 19.7 | 19.6 | 11.9 |
| 2009 | 24.3 | 17.2 | 23.2 | 15.0 | 27.0 | 20.8 | 20.4 | 10.5 |
| 2010 | 23.1 | 17.9 | 23.4 | 14.2 | 26.3 | 20.9 | 20.2 | 11.0 |
| 2011 | 23.6 | 19.4 | 21.7 | 13.3 | 27.8 | 21.3 | 20.2 | 10.6 |
| 2012 | 23.0 | 18.1 | 20.6 | 15.8 | 26.8 | 21.5 | 19.6 | 12.3 |
| 2013 | 22.4 | 21.9 | 22.9 | 11.5 | 25.5 | 21.6 | 20.3 | 12.4 |
| 2014 | 23.0 | 21.7 | 22.9 | 12.1 | 26.2 | 22.1 | 20.4 | 12.0 |
| 2015 | 23.2 | 21.8 | 23.2 | 12.1 | 26.4 | 22.0 | 20.6 | 11.8 |
| 2016 | 22.9 | 22.2 | 23.3 | 12.0 | 26.1 | 22.6 | 20.6 | 11.2 |
| 2017 | 23.1 | 22.7 | 23.2 | 11.6 | 26.1 | 23.0 | 20.6 | 10.9 |
| 2018 | 23.0 | 23.5 | 23.2 | 11.2 | 26.0 | 23.3 | 20.5 | 10.8 |
| 2019 | 23.3 | 23.8 | 22.9 | 10.8 | 25.7 | 23.7 | 20.6 | 10.4 |
| 2020 | 23.1 | 24.5 | 23.5 | 9.1 | 25.4 | 24.6 | 21.3 | 8.7 |
National Bureau of Statistics of China.
Table 4.
Major causes of cancer-associated death from 1973 to 2005
| 1973–1975 (year) |
1990–1992 (year) |
2004–2005 (year) |
|||
|---|---|---|---|---|---|
| Site | Proportion (%) | Site | Proportion (%) | Site | Proportion (%) |
| Stomach | 23.0 | Stomach | 23.2 | Lung | 22.7 |
| Esophagus | 22.3 | Liver | 18.8 | Liver | 19.3 |
| Liver | 15.1 | Lung | 16.2 | Stomach | 18.2 |
| Cervix | 7.6 | Esophagus | 16.1 | Esophagus | 11.2 |
| Lung | 7.4 | Colorectum | 4.9 | Colorectum | 5.2 |
| Colorectum | 5.3 | Leukemia | 3.4 | Leukemia | 2.8 |
| Leukemia | 3.8 | Cervix | 1.8 | Brain | 2.3 |
| Nasopharynx | 2.8 | Nasopharynx | 1.6 | Breast | 2.1 |
| Breast | 2.0 | Breast | 1.6 | Pancreas | 1.9 |
| Brain | 1.9 | Bladder | 0.9 | Bone | 1.3 |
| Others | 8.8 | Others | 11.5 | Others | 13.0 |
Three National Retrospective Sampling Survey of Death Causes6.
Regarding the ASMR in men, a steadily descending trend has been observed for all cancer types combined, with an annual percentage change of 1.2%1. The mortality decreased significantly for cancers of the esophagus, stomach, and liver. Additionally, upward trends in mortality were observed for prostate cancer, pancreatic cancer, brain cancer, and leukemia. In women, the ASMR for esophageal, stomach, and liver cancers also decreased dramatically during this period, whereas the rates for cervical and thyroid cancers showed increasing trends. The trend in the ASMR for cancers of the colorectum, brain, and uterus remained stable1,3.
Survival trends
Figure 3 illustrates the prognosis for the major types of cancer. The age-standardized 5-year survival rate was estimated to be 40.5% in 2012–2015, representing a substantial increase with respect to 2003–2005 (30.9%)7. Women had better prognosis than men (47.8% vs. 33.9%). The age-standardized 5-year survival rate for overall cancers combined in urban areas was higher than that in rural areas (46.7% vs. 33.6%)7.
Figure 3.
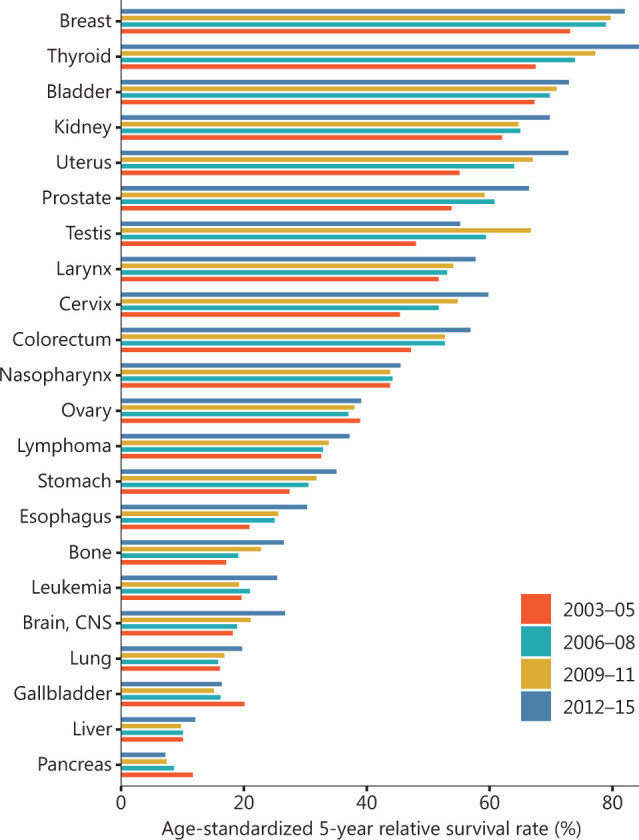
Age-standardized 5-year relative survival rates for the common cancers. Data were extracted from Changing cancer survival in China during 2003–2015: a pooled analysis of 17 population-based cancer registries7.
The age-standardized 5-year survival rate substantially varied for individual cancers. The best prognosis across the 4 periods was observed for thyroid cancer (67.5% in 2003–2005, 73.9% in 2006–2008, 77.2% in 2009–2011, and 84.3% in 2012–2015). Breast cancer had the second highest 5-year survival rate (82.0%) and was followed by bladder cancer (72.9%) in 2012–2015. The lowest 5-year age-standardized survival rate (7.2%) was found for pancreatic cancer (Figure 3)7. In urban areas, the 5-year age-standardized survival rate increased from 39.5% in 2003–2005 to 46.7% in 2012–2015, with a 2.2% average change. In contrast, greater growth in the 5-year standardized survival rate was observed in rural than urban areas: the rate increased from 21.8% in 2003–2005 to 33.6% in 2012–2015, with a 3.9% average change7.
Etiology and underlying modifiable risk factors
Infectious agents
Infectious agents generally include viruses, bacteria, and parasites, which can result in cancer or increase cancer risk. The most common infectious causes associated with cancer development are hepatitis B/C virus (HBV/HCV), aflatoxin exposure, Helicobacter pylori (H. pylori), human papillomavirus (HPV), and Epstein-Barr virus, which are risk factors for liver cancer, gastric cancer, cervical cancer, and nasopharyngeal cancer, respectively.
HBV and HCV are the predominant established risk factors for liver cancer in China. Approximately 53.2% of liver cancer deaths in China have been attributed to HBV infection, and 17.0% of deaths have been attributed to HCV infection8. The main infectious risk factors for liver cancer also include exposure to dietary aflatoxins. The population attributable risk of aflatoxin-associated liver cancer has been estimated to be 25% in China9. H. pylori has been classified as a class I carcinogen by the WHO10. A case-control study has shown that 78.5% of non-cardia gastric cancer and 62.1% of gastric cardia cancer cases are attributable to H. pylori infection11. The overall prevalence rate of H. pylori reached 55% among Chinese residents12. Although a slowly downward trend in the prevalence rate of H. pylori in China has been observed, the decline has not been sufficient to affect the incidence of gastric cancer13. Of the more than 100 identified HPV types, HPV-16 and HPV-18 were categorized as human carcinogens in 1995 by the International Agency for Research on Cancer14. The national overall prevalence of HPV infection showed a slightly decreasing trend from 16.4% in 2003 to 17.3% in 201615, and approximately 97.4% of deaths caused by cervical cancer in China are attributable to HPV infection16. In addition, several epidemiological studies have suggested that HPV infection is associated with the development of not only cervical cancer but also other types of cancer, including head and neck squamous cell carcinoma, oral, pharyngeal, and laryngeal cancers, and skin cancer17–19.
In general, infectious factors play major roles in the development and progression of various cancers, and approximately one-third of cancer cases in China are attributable to infection. In 2018, 780,000 of the 2.2 million new infection-attributable cases worldwide were in China20.
Alcohol
Alcohol consumption is considered a primary risk factor for cancer mortality worldwide. Alcohol consumption has been classified as a human carcinogen, and is known to generate reactive oxygen species, impair the body’s ability to break down nutrients, and increase the estrogen levels in the blood21. According to WHO estimates, 4.4% and 1.0% of deaths from cancer in men and women, respectively, are attributable to alcohol consumption in China22. A meta-analysis of 26 observational studies has indicated that alcohol consumption is significantly associated with increased risk of liver cancer, esophageal squamous cell carcinoma, and stomach cancer23. Alcohol consumption can also increase the risk of cancer in a dose-responsive manner24. Even at extremely low levels of consumption, alcohol has been found to increase the risk of head-and-neck cancers and esophageal squamous cell carcinoma25. A systematic analysis from the Global Burden of Disease Study has suggested that the optimal level of alcohol consumption for minimizing harm is zero26, thus suggesting that no safe level of alcohol consumption exists. The number of liters of alcohol consumed by the Chinese population 15 years of age or above has stably increased from 1960 to 201522. The prevalence rates of heavy episodic drinking in men and women (older than 15 years) are 36.3% and 8.6%, respectively, significantly higher than those in other countries22. Thus, the interventions and policies for the control of alcohol consumption should be reinforced.
Tobacco
A substantial number of studies have shown that tobacco use is associated with increased risk of many cancer types, such as lung cancer, liver cancer, stomach cancer, and esophageal cancer27–29. Tobacco products can produce multiple carcinogens, such as nicotine and volatile organic compounds, which cause complex mutations in critical cancer genes30. A population-based cohort study conducted in Austria has indicated that current smokers, compared with people who have never smoked, have greater risk of cancers of the lung (hazard ratio [HR] = 17.66, 95% CI, 14.65–21.29), larynx (HR = 11.29, 95% CI, 5.49–23.20), head and neck (HR = 2.53, 95% CI, 1.87–3.41), esophagus (HR = 3.84, 95% CI, 2.33–6.35), liver (HR = 4.07, 95% CI, 2.55–6.51), bladder (HR = 3.08, 95% CI, 2.00–4.73), pancreas (HR = 2.68, 95% CI, 1.93–3.71), and colorectum (HR = 1.31, 95% CI, 1.09–1.57)28. A nationwide prospective study in China recruiting 0.5 million adults has suggested that smoking significantly elevates the risk of lung cancer (risk ratio [RR] = 2.51, 95% CI, 2.18–2.90), liver cancer (RR = 1.32, 95% CI, 1.12–1.54), stomach cancer (RR = 1.34, 95% CI, 1.16–1.55), and esophageal cancer (RR = 1.47, 95% CI, 1.24–1.73)31. Furthermore, a positive dose-response relationship with smoking intensity and duration has been observed for most cancers32–34. Second-hand smoke, including environmental exposure to tobacco smoke, is also classified as a known human carcinogen by a series of regulatory agencies and governmental authorities35. Studies have indicated that passive smoking can increase the risk of cancer among people who do not smoke36–39.
China is the largest producer and consumer of tobacco worldwide. More than 300 million smokers live in China, and over 700 million non-smokers are exposed to second-hand smoke at least once per day each week40. Despite the initiation of tobacco control policies and educational activities, only minor effects have been observed on the smoking prevalence in China. Six nation-wide epidemiological surveys of smoking status, conducted in 1984, 1996, 2002, 2010, 2015, and 2018, have shown that the prevalence rate of smoking remains high, although a slight decrease was observed from 33.9% to 26.6%41. Data from the National Health Service Surveys have also indicated that the implementation of tobacco control policies in China has not been effective in decreasing smoking prevalence: the proportion of current smokers was 26.0% in 2003, 24.9% in 2008, and 25.2% in 201342. Thus, actions to strengthen the tobacco surveillance system are urgently needed.
Diet
Many epidemiological studies have reported the association between cancer outcomes and dietary factors43–45. A Mediterranean diet, associated with longevity and high quality of life, has been shown to significantly decrease the risk of cancer incidence and mortality46. Vegetable consumption has been identified to have a protective role against cancer. Compared with non-vegetarians, vegetarians have a statistically significantly lower overall cancer risk44. Moreover, vegan diets have been found to decrease overall cancer incidence by 16% in both sexes and to decrease female-specific cancer incidence by 34%47. Raw garlic consumption has been inversely associated with the development of liver cancer among individuals negative for HBV48. The Women’s Health Initiative Randomized Trial has indicated that a low-fat dietary pattern, characterized by high vegetable, fruit, and grain intake, can decrease the risk of death from breast cancer in postmenopausal women43. However, a prospective cohort study has suggested no association between dietary fat and liver cancer risk49.
Moreover, some methods of preserving and cooking food can influence cancer risk50. People who prefer salty food, and salt-preserved meat and fish, generally have a higher risk of gastric cancer51. A recent meta-analysis of 11 case-control and cohort studies has indicated that a high intake of salt increases the risk of gastric cancer dramatically (odds ratio = 2.05, 95% CI, 1.60-2.62)52. Consumption of processed meat may increase the risk of breast cancer45. Red meat intake has been found to increase the risk of overall cancer by 31% and the risk of breast cancer by 83%53. Dietary exposure to aflatoxin, derived mainly from grain mildew, is the primary etiologic factor influencing liver cancer in China. A widespread change in dietary habits from consumption of maize to rice, and changes in storage methods, have effectively decreased aflatoxin contamination in food in China, thus decreasing liver cancer burden50,54. Chinese-style salted fish has been classified as a carcinogen by the International Agency for Research on Cancer55. However, a recent population-based case-control study in Southern China has shown no association between consumption of hard Chinese-style salted fish and nasopharyngeal carcinoma56. Dietary habits in different regions of China are diverse, and thus the evidence of other dietary factors contributing to cancer development is currently insufficient57.
Physical activity
Strong evidence indicates that regular physical activity, particularly at high intensity, may negatively affect the risk of several cancers58. Physical activity decreases the risk of cancer by lowering levels of sex hormones, decreasing insulin sensitivity, and increasing colonic peristalsis59. Individuals with the highest level of recreational or occupational physical activity, compared with those with the lowest level, have a 15% lower risk of bladder cancer, according to a systematic literature review and meta-analysis of 15 studies60. A prospective cohort study in 73,049 Chinese women has also suggested that exercise at or above the recommended level is associated with a 27% lower risk of breast cancer than lower levels of exercise61. A negative statistical association between ovarian cancer risk and physical activity has been reported in a study conducted in Southern China62. A case-control study based on data from eastern and southern China has also reported that physical activity is beneficial in decreasing the risk of prostate cancer63. In comparison, a sedentary lifestyle has emerged as a risk factor for several site-specific cancers. Physical inactivity is responsible for 8.9% of the colorectal cancer burden in men and 9.0% of that in women64. A positive statistical association between ovarian cancer risk and sitting time has been reported in a quantitative meta-analysis65. China had a high prevalence of insufficient activity in adolescents in 2016 (84.3%), indicating a slight decrease from 85.4% in 200166. Boys have been found to have higher activity than girls (prevalence rates of insufficient activity of 80.1% and 89.1%, respectively)66. Policy actions to improve physical activity should be prioritized, particularly policies targeted to girls.
Overweight and obesity
Overweight and obesity can cause long-lasting inflammation and oxidative stress67. According to estimates, 11.9% and 13.1% of the cancer burdens in men and women, respectively, are attributable to obesity68. Robust evidence has shown that obesity increases the risk of endometrial cancer, esophageal adenocarcinoma, and cancers of the colorectum, postmenopausal breast, prostate, and kidney69. A prospective cohort of 68,253 Chinese women has indicated that obesity increases the risk of overall cancer (HR = 1.36, 95% CI = 1.21–1.52), postmenopausal breast cancer (HR = 2.43, 95% CI = 1.73–3.40), endometrial cancer (HR = 5.34, 95% CI = 3.48–8.18), liver cancer (HR = 1.93, 95% CI = 1.14–3.27), and epithelial ovarian cancer (HR = 2.44, 95% CI = 1.37–4.35)70. Moreover, a meta-analysis of more than 10 million participants from 24 prospective studies has found a positive association between high body mass index (BMI) and gastric cardia cancer71. A BMI-dependent increase in the risk of developing liver cancer has been reported in a systematic review of 28 prospective studies72. In addition, obesity leads to a high risk of development of type 2 diabetes and thus increases the risk of colorectal cancer73.
Obesity has become a major public health problem in China, with prevalence values of 34.3% for overweight (BMI: 24.0–27.9 kg/m2) and 16.4% for obesity (BMI: 28.0 kg/m2 or higher) in adults (≥18 years), according to the Chronic Disease and Nutrition Surveillance 2015–2019 survey74. By 2030, the prevalence rate of overweight and obesity is expected to reach 65.3% in adults, equivalent to 790 million people75. The high rates of obesity and overweight are driven by a combination of factors including economic growth, socio-cultural norms, and substantial changes in dietary patterns74. National prevention and control policies toward obesity have been insufficient, and thus this issue requires more government attention75.
Cancer prevention and control
To control the cancer burden, the Chinese government has made substantial efforts over the past decades. A series of policies were initiated in different periods according to social development and requirements. The main strategies for decreasing cancer burden have focused mainly on primary and secondary prevention, as shown in Figure 4.
Figure 4.

Measures for cancer prevention and control in China.
Governmental guidance
To guide cancer prevention in an orderly and effective manner, China has issued the “National Cancer Prevention and Control Plan (1986–2000)”, the first programmatic documentation of cancer prevention and control in China76. Cancer prevention has been strongly emphasized. The release of the National Cancer Prevention and Control Program (2004–2010) by the Chinese Ministry of Health endeavored to establish a national cancer registry system, enhance health education at the population level, and expand screening coverage for the principal cancers, particularly in rural areas observing obvious achievement in narrowing the urban-rural gap of the worse cancer incidence77. To address increases in non-communicable diseases and advance public health development, the National Program for Chronic Disease Prevention and Treatment (2012–2015)78 and China’s Cancer Prevention and Treatment Three-Year Action Plan (2015–2017)79 were initiated collaboratively by the Chinese government. Expanding the coverage of services for timely detection and treatment of frequently occurring cancers, emphasis is placed on the management of high-risk populations and the promotion of healthful lifestyles (e.g., tobacco cessation) in these 2 documents.
On October 25, 2016, the Chinese government enacted the “Healthy China 2030” strategy, jointly issued and implemented by the Central Committee of the Communist Party of China and the State Council, drafting a blueprint for cancer control80. In 2019, the Healthy China Action Plan (2019–2022) was officially implemented in accordance with the “Healthy China 2030” strategy81. The guidelines aim to improve cancer screening by increasing screening coverage and the early detection rates of major cancers in high-incidence areas. In addition, the promotion of healthful eating, physical activity, and other health initiatives is emphasized. The policies and programmatic documents issued in past decades have provided effective guidance and indications for cancer prevention in various regions, thus reflecting the government’s attention to cancer prevention and control.
Primary prevention
Primary prevention efforts are considered the most cost-effective strategy to curb the cancer burden. These efforts are aimed at decreasing exposure to risk factors associated with cancer development and increasing the resistance of the population to addressing cancer risk—a high priority aspect in cancer control. Among all efforts, vaccination and educational interventions targeting risk factors are the major preventive measures.
Vaccination
Several vaccines are available targeting several specific cancers caused by viruses. Hepatitis B vaccine has high efficacy in preventing the development of liver cancer. This vaccine is administered to newborns at 0 months of age (or within 24 h of birth), 1 month, and 6 months82,83. To increase hepatitis B vaccine coverage, the central government of China initiated several programmatic documents and policies, such as waiving vaccine administration and purchase costs84. In 2002, the hepatitis B vaccine was incorporated into the Expanded Program of Immunization, and a Global Alliance for Vaccines and Immunization was also implemented to ensure the vaccine’s availability in China’s poorest provinces and counties85. Encouragingly, the coverage rate of 3 doses of the hepatitis B vaccine has markedly increased, from 70.7% in 1999 to 99.7% in 201286. According to the national serological surveys conducted in 1992 and 2006, the infection rate of HBV has significantly decreased from 9.8% to 7.2%84, thus suggesting that the vaccination program for the control of the transmission of HBV in China has made great achievements.
The HPV vaccine is expected to decrease cervical cancer incidence and thus eliminate cervical cancer87. The WHO Cervical Cancer Elimination Modelling Consortium has reported that elimination could occur between 2059 and 2102 when girls vaccinated only in all countries88. Currently, the first Chinese HPV vaccine, Cecolin, has gained prequalification from WHO89. However, the HPV vaccine coverage in China remains unsatisfactory. A survey conducted at Peking University in China involving 884 college students has indicated that only 9.5% of the female students had received the vaccine90. Many misunderstandings regarding HPV and HPV vaccines persist among the public, thus suggesting that limited knowledge regarding the HPV vaccine is the primary barrier to acceptance of the vaccine91. Beyond limited awareness, high price may be another important reason limiting vaccination coverage. Generally, HPV vaccines cost as much as $271–450 (RMB: 1806–2999) for the 3 doses; this high cost makes the HPV vaccine inaccessible for most people, particularly women living in rural areas92. To increase HPV vaccine coverage, health promotion campaigns associated with the HPV vaccine are required. Public media also should take responsibility for disseminating knowledge regarding the HPV vaccine in a simple manner to help more people to learn about its importance.
Behavioral interventions
Behavioral interventions refer to the provision of behavioral education and correcting actions that can increase the risk of cancer. The main health initiatives in China include health education, promoting healthful diets, fitness, and tobacco control. The NCC, the Chinese Center for Disease Control and Prevention, the Chinese Anti-Cancer Association, and other institutions or organizations produce several themed publicity events every year across the entire country93, to publicize essential information for cancer prevention and control, and enhance public awareness and acceptance of cancer prevention. These organizations also provide scientific guidance to the public for developing healthful diets through media or books.
At present, China’s tobacco control strategy is focused mainly on adolescents, passive smokers (particularly women and children), and current smokers. To address tobacco use, the following measures have been implemented according to the Ottawa Charter: (1) enacting of public policies, such as banning the sale of cigarettes to those under 18 years of age; (2) elimination of exposure to second-hand tobacco smoke in all workplaces, public places, family environments, and public transportation; and (3) implementation of standardized tobacco packaging with large graphic or text warnings about the harms of smoking/tobacco use to health on all packages94. To limit the transmission of H. pylori, a comprehensive national prevention strategy had been implemented in China, including promoting good hygiene and handwashing, and the use of serving chopsticks and spoons95. Salt is an essential component of the human diet, however, high intake can significantly increase the risk of stomach cancer96. The WHO has called for all countries to decrease their intake of salt to less than 5 g/day by the year 202597. The Healthy Lifestyle Campaign for All, initiated by the Disease Control Bureau of the Ministry of Health in 200798, focused on a balanced diet and physical activity. A series of salt control and educational initiatives were subsequently launched. The results of Chronic Disease and Nutrition Surveillance performed in 31 provinces (autonomous regions and municipalities) from 2015 to 2019 has described the achievements of salt reduction initiatives in 2020: the per capita daily consumption was 9.3 grams of salt, 1.2 grams lower than that in 201599. These accomplishments indicate improved health awareness among the public.
Cancer registry
Cancer epidemiology, which includes cancer incidence, morbidity, mortality, and survival, is crucial to provide scientific information for cancer prevention and control. As the basis of the cancer control programs, the cancer registry plays a crucial role in cancer epidemic surveillance, evaluation of cancer control programs, and guidance for anti-cancer strategies. In China, cancer surveillance registration emerged in the 1960s in 3 demonstration sites: Qidong (population-based causes of death registry in 1958), Linxian (esophageal cancer incidence registry in 1959), and Shanghai (population-based cancer registry in 1963)100. The system was designed primarily to collect data on cancer incidence, mortality, and survival, as well as the population distribution in each region, and to further describe the burden of cancer. The cancer registration system developed very slowly at the beginning of its establishment. To enhance the management of the surveillance system, the Reporting Manual of Cancer Registration was released in 1982 by the Office of National Central Cancer Registry. In 2002, the National Central Cancer Registry was launched under the supervision of the former Ministry of Health, and was responsible for systematically collecting, analyzing, and interpreting cancer data. In 2008, to improve the standard of public health service, the cancer registration program was incorporated into the Central Subsidies for Local Transfer Payments by the Ministry of Finance combined with the former Ministry of Health. With strong support from the Chinese government, the national cancer surveillance network has rapidly developed. By 2009, 149 cancer registries had been established, accounting for 10% of the national population100. Every year, the NCC estimates the numbers of new cancer cases and deaths in China according to the collected data, thus providing key evidence for the formulation of policies. By the end of 2020, cancer registration covered 1152 counties, accounting for approximately 40% of the national population (598 million)1.
Cancer screening
The risk factors associated with cancer development are diverse, and thus decreasing cancer burden through only primary prevention is difficult. A substantial number of high-quality epidemiological studies have shown that screening for certain types of cancer may effectively decrease cancer incidence/mortality through enabling early detection and lesion removal in asymptomatic at-risk populations101–103. Four large-scale population-based organized cancer screening programs in mainland China have been initiated since 2005: Early Detection and Early Treatment of Cancer in Rural Cancer (2005), Early Detection and Early Treatment of Cancer in Huaihe Areas (2007), Cervical Cancer and Breast Cancer Screening Program for Women in Rural Areas (also called Two Cancer Screening; 2009), and Cancer Screening Program in Urban China (2012), to provide free screening services for people at high risk and those who are living in high-risk areas. The screening includes the 8 most common cancers in China: those of the lung, stomach, liver, colorectum, esophagus, cervix, breast, and nasopharynx104. The Chinese government has greatly expanded the coverage of cancer screening programs. From 2009 to 2018, the coverage of Two Cancer Screening expanded from 200 counties (cities, districts) to more than 1,700 counties, providing free cervical cancer screening for 85 million women and breast cancer screening for 20 million women105. Esophageal cancer, gastric cancer, and liver cancer were all incorporated into 3 national screening programs. As of 2018, 3.7 million high-risk individuals were identified, and a total of 0.2 million individuals had received free screening for upper gastrointestinal cancer in rural high-risk areas, thus yielding an early detection rate of 75.1% and a treatment rate of 85.7%106.
Beyond the programs supported by the central government, regional screening programs have also been implemented in several areas. In 2017, “Combined Screening for Common Cancers” was initiated in the Tianjin Municipal area, thus providing screening for lung cancer, breast cancer, gastric cancer, and liver cancer. The joint screening program for common cancers has been piloted in 48 communities and towns in 6 districts and Jizhou districts, and more than 150,000 residents have received cancer screening services107. Colorectal cancer screening at no cost is offered to residents in Zhejiang Province every 5 years108. Beyond the organized cancer screening programs, opportunistic screening may serve as an alternative, given the increasing health awareness of the public, the high accessibility of medical services, and improvements in service quality. Since 2019, the number of demonstration sites for opportunistic screening have increased. By the end of 2020, 997 units in rural areas have provided opportunistic screening services for upper gastrointestinal cancer109.
Expenditures and national insurance for cancer control
In recent years, the central government of China has paid great attention to the implementation of cancer screening, and funding for cancer screening has rapidly grown in recent decades. Since 2005, 280 million RMB each year has been invested by the central government to support the screening programs in the rural high-risk, Huaihe, and urban areas106. In addition, China’s government has invested more than 600 million RMB to screen for breast cancer and cervical cancer, and 19 provinces (municipalities and districts) achieved full coverage of screening for these 2 cancer types in 2020 through combined funding from multiple local governments110.
High expenditure and financial burden are important obstacles to the accessibility of cancer medical treatment. The Chinese government has launched 6 rounds of national drug price negotiation since 2016 to lower the costs for innovative drugs, particularly for anticancer drugs111. Recent price negotiation with pharmaceutical companies for medications covered by national basic health insurance was conducted in December 2021 by China’s National Healthcare Security Administration. Among the 117 drugs under negotiation, 74 were successfully added to the 2021 National Reimbursement Drug List, thus resulting in a 61.7% price decrease112. Moreover, 18 of the 74 newly added drugs were anti-cancer medicines, thereby greatly alleviating the personal financial burden of cancer treatment among Chinese residents. Beyond increasing insurance coverage for anti-cancer drugs, basic reimbursement services for examinations, treatment, and other costs for major diseases have steadily increased113. With the help of national subsidies, disadvantaged residents have gained access to convenient health services.
Limitations and challenges in cancer prevention
Geographical differences in diverse modifiable cancer risk factors have resulted in cancer burdens that vary across regions in China, thus leading to substantial difficulties in primary cancer prevention. Health educational campaigns in different regions should be improved and directed well. In addition, the HPV vaccine has not been covered in national immunization in China, thus limiting the number of vaccinations. Therefore, a larger budget should be allocated to cancer prevention in the future.
In general, because cancer occurrence is influenced by many risk factors, screening among the general population is not cost-effective. Risk-adapted screening strategies have been used for most current cancer screening in China114,115. By considering the epidemiological characteristics of the population and related biological markers or genetic factors, the risk prediction model provides an effective method for focusing coverage on high-risk individuals precisely. With the growth of big data and biological information, more accurate biomarkers have been identified, such as circulating tumor DNA116. Therefore, the established risk prediction models should be updated in the future. Additionally, how to choose accurate risk prediction models and set suitable cut-off values for the risk scores used in screening will be future research priorities to improve screening efficiency.
In conclusion, current epidemiological data indicate that cancer remains the major factor threatening health in China. Clear incremental trends in the incidence of thyroid and breast cancer in women, and colorectal and prostate cancer in men, have been observed. The great improvements in living conditions, particularly in rural areas of China, progress in health awareness, and shifts in risk factors are thought to be the main reasons for the dramatic changes in cancer burden observed in the past several decades. Hence, the central government and multidisciplinary institutions require strategies to strengthen existing measures in cancer prevention, screening, diagnosis, and management.
Acknowledgments
We thank Yiwen Yu at the Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, for editing the language of the main text.
Grant support
This study was supported by grants from the Sanming Project of Medicine in Shenzhen (Grant No. SZSM201911015).
Conflict of interest statement
No potential conflicts of interest are disclosed.
Author contributions
Conceived and designed the analysis: Wanqing Chen, Ji Peng, Changfa Xia and Lin Lei.
Collected the data: Fan Yang, Xinxin Yan, Shaoli Zhang, Maomao Cao.
Contributed data or analysis tools: He Li, Dianqin Sun, Siyi He.
Wrote the paper: Maomao Cao.
References
- 1.Zheng R, Zhang S, Zeng H, Wang S, Sun K, Chen R, et al. Cancer incidence and mortality in China, 2016. J Natl Cancer Center. 2022;2:1–9. doi: 10.1016/j.jncc.2022.02.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Wei W, Zeng H, Zheng R, Zhang S, An L, Chen R, et al. Cancer registration in China and its role in cancer prevention and control. Lancet Oncol. 2020;21:e342–9. doi: 10.1016/S1470-2045(20)30073-5. [DOI] [PubMed] [Google Scholar]
- 3.Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–32. doi: 10.3322/caac.21338. [DOI] [PubMed] [Google Scholar]
- 4.National Bureau of Statistics of China. [[Cited 2022 April 5]];China Statistical Yearbook. Available from: http://www.stats.gov.cn/tjsj/ndsj/
- 5.Sun D, Li H, Cao M, He S, Lei L, Peng J, et al. Cancer burden in China: trends, risk factors and prevention. Cancer Biol Med. 2020;17:879–95. doi: 10.20892/j.issn.2095-3941.2020.0387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Tong-hai L. Mortality and constitution of the top 10 of most common cancers in China. China Cancer. 2010;19:801–2. [Google Scholar]
- 7.Zeng H, Chen W, Zheng R, Zhang S, Ji JS, Zou X, et al. Changing cancer survival in China during 2003-15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6:e555–67. doi: 10.1016/S2214-109X(18)30127-X. [DOI] [PubMed] [Google Scholar]
- 8.Cao M, Ding C, Xia C, Li H, Sun D, He S, et al. Attributable deaths of liver cancer in China. Chin J Cancer Res. 2021;33:480–9. doi: 10.21147/j.issn.1000-9604.2021.04.05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Liu Y, Chang CC, Marsh GM, Wu F. Population attributable risk of aflatoxin-related liver cancer: systematic review and meta-analysis. Eur J Cancer. 2012;48:2125–36. doi: 10.1016/j.ejca.2012.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Yang JY, Kim JB, Lee P, Kim SH. Evodiamine Inhibits Helicobacter pylori Growth and Helicobacter pylori-Induced Inflammation. Int J Mol Sci. 2021;22:3385. doi: 10.3390/ijms22073385. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yang L, Kartsonaki C, Yao P, de Martel C, Plummer M, Chapman D, et al. The relative and attributable risks of cardia and non-cardia gastric cancer associated with Helicobacter pylori infection in China: a case-cohort study. Lancet Public Health. 2021;6:e888–96. doi: 10.1016/S2468-2667(21)00164-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Nagy P, Johansson S, Molloy-Bland M. Systematic review of time trends in the prevalence of Helicobacter pylori infection in China and the USA. Gut Pathog. 2016;8:8. doi: 10.1186/s13099-016-0091-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Li M, Sun Y, Yang J, de Martel C, Charvat H, Clifford GM, et al. Time trends and other sources of variation in Helicobacter pylori infection in mainland China: a systematic review and meta-analysis. Helicobacter. 2020;25:e12729. doi: 10.1111/hel.12729. [DOI] [PubMed] [Google Scholar]
- 14.Chelimo C, Wouldes TA, Cameron LD, Elwood JM. Risk factors for and prevention of human papillomaviruses (HPV), genital warts and cervical cancer. J Infect. 2013;66:207–17. doi: 10.1016/j.jinf.2012.10.024. [DOI] [PubMed] [Google Scholar]
- 15.Zhu B, Liu Y, Zuo T, Cui X, Li M, Zhang J, et al. The prevalence, trends, and geographical distribution of human papillomavirus infection in China: the pooled analysis of 1.7 million women. Cancer Med. 2019;8:5373–85. doi: 10.1002/cam4.2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Chen W, Xia C, Zheng R, Zhou M, Lin C, Zeng H, et al. Disparities by province, age, and sex in site-specific cancer burden attributable to 23 potentially modifiable risk factors in China: a comparative risk assessment. Lancet Glob Health. 2019;7:e257–69. doi: 10.1016/S2214-109X(18)30488-1. [DOI] [PubMed] [Google Scholar]
- 17.Hübbers CU, Akgül B. HPV and cancer of the oral cavity. Virulence. 2015;6:244–8. doi: 10.1080/21505594.2014.999570. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Smola S. Immunopathogenesis of HPV-associated cancers and prospects for immunotherapy. Viruses. 2017;9:254. doi: 10.3390/v9090254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Dogantemur S, Ozdemir S, Uguz A, Surmelioglu O, Dagkiran M, Tarkan O, et al. Assessment of HPV 16, HPV 18, p16 expression in advanced stage laryngeal cancer patients and prognostic significance. Braz J Otorhinolaryngol. 2020;86:351–7. doi: 10.1016/j.bjorl.2019.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.de Martel C, Georges D, Bray F, Ferlay J, Clifford GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020;8:e180–90. doi: 10.1016/S2214-109X(19)30488-7. [DOI] [PubMed] [Google Scholar]
- 21.National Cancer Institute. [[Cited 2022 April 10]];Alcohol and Cancer Risk. Available from: https://www.cancer.gov/about-cancer/causes-prevention/risk/alcohol/alcohol-fact-sheet.
- 22.World Health Organization. [[Cited 2022 April 10]];Global status report on alcohol and health (2018) Available from: https://www.who.int/publications/i/item/9789241565639.
- 23.He F, Sha Y, Wang B. Relationship between alcohol consumption and the risks of liver cancer, esophageal cancer, and gastric cancer in China: meta-analysis based on case-control studies. Medicine. 2021;100:e26982. doi: 10.1097/MD.0000000000026982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Li N, Deng Y, Zhou L, Tian T, Yang S, Wu Y, et al. Global burden of breast cancer and attributable risk factors in 195 countries and territories, from 1990 to 2017: results from the Global Burden of Disease Study 2017. J Hematol Oncol. 2019;12:140. doi: 10.1186/s13045-019-0828-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Praud D, Rota M, Rehm J, Shield K, Zatoński W, Hashibe M, et al. Cancer incidence and mortality attributable to alcohol consumption. Int J Cancer. 2016;138:1380–7. doi: 10.1002/ijc.29890. [DOI] [PubMed] [Google Scholar]
- 26.GBD 2016 Alcohol Collaborators. Alcohol use and burden for 195 countries and territories, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2018;392:1015–35. doi: 10.1016/S0140-6736(18)31310-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Hansen MS, Licaj I, Braaten T, Lund E, Gram IT. The fraction of lung cancer attributable to smoking in the Norwegian Women and Cancer (NOWAC) Study. Br J Cancer. 2021;124:658–62. doi: 10.1038/s41416-020-01131-w. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Weber MF, Sarich PEA, Vaneckova P, Wade S, Egger S, Ngo P, et al. Cancer incidence and cancer death in relation to tobacco smoking in a population-based Australian cohort study. Int J Cancer. 2021;149:1076–88. doi: 10.1002/ijc.33685. [DOI] [PubMed] [Google Scholar]
- 29.Pang Q, Qu K, Zhang J, Xu X, Liu S, Song S, et al. Cigarette smoking increases the risk of mortality from liver cancer: a clinical-based cohort and meta-analysis. J Gastroenterol Hepatol. 2015;30:1450–60. doi: 10.1111/jgh.12990. [DOI] [PubMed] [Google Scholar]
- 30.Hecht SS, Hatsukami DK. Smokeless tobacco and cigarette smoking: chemical mechanisms and cancer prevention. Nat Rev Cancer. 2022;22:143–55. doi: 10.1038/s41568-021-00423-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Chen Z-M, Peto R, Iona A, Guo Y, Chen Y-P, Bian Z, et al. Emerging tobacco-related cancer risks in China: a nationwide, prospective study of 0.5 million adults. Cancer. 2015;121:3097–106. doi: 10.1002/cncr.29560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ansary-Moghaddam A, Huxley R, Barzi F, Lawes C, Ohkubo T, Fang X, et al. The effect of modifiable risk factors on pancreatic cancer mortality in populations of the Asia-Pacific region. Cancer Epidemiol Biomarkers Prev. 2006;15:2435–40. doi: 10.1158/1055-9965.EPI-06-0368. [DOI] [PubMed] [Google Scholar]
- 33.McLaughlin JK, Lindblad P, Mellemgaard A, McCredie M, Mandel JS, Schlehofer B, et al. International renal-cell cancer study. I. Tobacco use. Int J Cancer. 1995;60:194–8. doi: 10.1002/ijc.2910600211. [DOI] [PubMed] [Google Scholar]
- 34.Praud D, Rota M, Pelucchi C, Bertuccio P, Rosso T, Galeone C, et al. Cigarette smoking and gastric cancer in the Stomach Cancer Pooling (StoP) Project. Eur J Cancer Prev. 2018;27:124–33. doi: 10.1097/CEJ.0000000000000290. [DOI] [PubMed] [Google Scholar]
- 35.Besaratinia A, Pfeifer GP. Second-hand smoke and human lung cancer. Lancet Oncol. 2008;9:657–66. doi: 10.1016/S1470-2045(08)70172-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Ni X, Xu N, Wang Q. Meta-analysis and systematic review in environmental tobacco smoke risk of female lung cancer by research type. Int J Environ Res Public Health. 2018;15:1348. doi: 10.3390/ijerph15071348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Hackshaw AK, Law MR, Wald NJ. The accumulated evidence on lung cancer and environmental tobacco smoke. BMJ. 1997;315:980–8. doi: 10.1136/bmj.315.7114.980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Ding Y, Yu C, Han Z, Xu S, Li D, Meng X, et al. Environmental tobacco smoke and pancreatic cancer: a case-control study. Int J Clin Exp Med. 2015;8:16729–32. [PMC free article] [PubMed] [Google Scholar]
- 39.Chang ET, Liu Z, Hildesheim A, Liu Q, Cai Y, Zhang Z, et al. Active and passive smoking and risk of nasopharyngeal carcinoma: a population-based case-control study in Southern China. Am J Epidemiol. 2017;185:1272–80. doi: 10.1093/aje/kwx018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.World Health Organization. [[Cited 2022 April 5]];Tobacco in China. Available from: https://www.who.int/china/health-topics/tobacco.
- 41.Wang C. An advanced coursebook of tobacco medicine. Peking Union Medial College Press. 2021:35–6. [Google Scholar]
- 42.Wang M, Luo X, Xu S, Liu W, Ding F, Zhang X, et al. Trends in smoking prevalence and implication for chronic diseases in China: serial national cross-sectional surveys from 2003 to 2013. Lancet Respir Med. 2019;7:35–45. doi: 10.1016/S2213-2600(18)30432-6. [DOI] [PubMed] [Google Scholar]
- 43.Chlebowski RT, Aragaki AK, Anderson GL, Pan K, Neuhouser ML, Manson JE, et al. Dietary modification and breast cancer mortality: long-term follow-up of the women’s health initiative randomized trial. J Clin Oncol. 2020;38:1419–28. doi: 10.1200/JCO.19.00435. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Aune D, Giovannucci E, Boffetta P, Fadnes LT, Keum N, Norat T, et al. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality-a systematic review and dose-response meta-analysis of prospective studies. Int J Epidemiol. 2017;46:1029–56. doi: 10.1093/ije/dyw319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Anderson JJ, Darwis NDM, Mackay DF, Celis-Morales CA, Lyall DM, Sattar N, et al. Red and processed meat consumption and breast cancer: UK Biobank cohort study and meta-analysis. Eur J Cancer. 2018;90:73–82. doi: 10.1016/j.ejca.2017.11.022. [DOI] [PubMed] [Google Scholar]
- 46.Sofi F, Cesari F, Abbate R, Gensini GF, Casini A. Adherence to Mediterranean diet and health status: meta-analysis. BMJ. 2008;337:a1344. doi: 10.1136/bmj.a1344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Tantamango-Bartley Y, Jaceldo-Siegl K, Fan J, Fraser G. Vegetarian diets and the incidence of cancer in a low-risk population. Cancer Epidemiol Biomarkers Prev. 2013;22:286–94. doi: 10.1158/1055-9965.EPI-12-1060. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Liu X, Baecker A, Wu M, Zhou JY, Yang J, Han RQ, et al. Raw garlic consumption and risk of liver cancer: a population-based case-control study in Eastern China. Nutrients. 2019;11:2038. doi: 10.3390/nu11092038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Ji X, Wang J, Li Z, Shen Q, Tuo J, Bi J, et al. Dietary fat intake and liver cancer risk: a prospective cohort study in Chinese women. Cancer Biol Med. 2021;19:370–83. doi: 10.20892/j.issn.2095-3941.2020.0633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Chen JG, Zhang SW. Liver cancer epidemic in China: past, present and future. Semin Cancer Biol. 2011;21:59–69. doi: 10.1016/j.semcancer.2010.11.002. [DOI] [PubMed] [Google Scholar]
- 51.Strumylaite L, Zickute J, Dudzevicius J, Dregval L. Salt-preserved foods and risk of gastric cancer. Medicina (Kaunas) 2006;42:164–70. [PubMed] [Google Scholar]
- 52.Ge S, Feng X, Shen L, Wei Z, Zhu Q, Sun J. Association between habitual dietary salt intake and risk of gastric cancer: a systematic review of observational studies. Gastroenterol Res Pract. 2012;2012:808120. doi: 10.1155/2012/808120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Diallo A, Deschasaux M, Latino-Martel P, Hercberg S, Galan P, Fassier P, et al. Red and processed meat intake and cancer risk: results from the prospective NutriNet-Santé cohort study. Int J Cancer. 2018;142:230–7. doi: 10.1002/ijc.31046. [DOI] [PubMed] [Google Scholar]
- 54.Szymañska K, Chen JG, Cui Y, Gong YY, Turner PC, Villar SP, et al. TP53 R249S mutations, exposure to aflatoxin, and occurrence of hepatocellular carcinoma in a cohort of chronic hepatitis B virus carriers from Qidong, China. Cancer Epidemiol Biomarkers Prev. 2009;18:1638–43. doi: 10.1158/1055-9965.EPI-08-1102. [DOI] [PubMed] [Google Scholar]
- 55.Secretan B, Straif K, Baan R, Grosse Y, El Ghissassi F, Bouvard V, et al. A review of human carcinogens – Part E: tobacco, areca nut, alcohol, coal smoke, and salted fish. Lancet Oncol. 2009;10:1033–4. doi: 10.1016/s1470-2045(09)70326-2. [DOI] [PubMed] [Google Scholar]
- 56.Barrett D, Ploner A, Chang ET, Liu Z, Zhang CX, Liu Q, et al. Past and recent salted fish and preserved food intakes are weakly associated with nasopharyngeal carcinoma risk in adults in Southern China. J Nutr. 2019;149:1596–605. doi: 10.1093/jn/nxz095. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Key TJ, Bradbury KE, Perez-Cornago A, Sinha R, Tsilidis KK, Tsugane S. Diet, nutrition, and cancer risk: what do we know and what is the way forward? BMJ. 2020;368:m511. doi: 10.1136/bmj.m511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Murray JM, Coleman HG, Hunter RF. Physical activity and cancer risk: Findings from the UK Biobank, a large prospective cohort study. Cancer Epidemiol. 2020;68:101780. doi: 10.1016/j.canep.2020.101780. [DOI] [PubMed] [Google Scholar]
- 59.Hardman AE. Physical activity and cancer risk. Proc Nutr Soc. 2001;60:107–13. doi: 10.1079/pns200076. [DOI] [PubMed] [Google Scholar]
- 60.Keimling M, Behrens G, Schmid D, Jochem C, Leitzmann MF. The association between physical activity and bladder cancer: systematic review and meta-analysis. Br J Cancer. 2014;110:1862–70. doi: 10.1038/bjc.2014.77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Pronk A, Ji BT, Shu XO, Chow WH, Xue S, Yang G, et al. Physical activity and breast cancer risk in Chinese women. Br J Cancer. 2011;105:1443–50. doi: 10.1038/bjc.2011.370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Lee AH, Su D, Pasalich M, Wong YL, Binns CW. Habitual physical activity reduces risk of ovarian cancer: a case-control study in southern China. Prev Med. 2013;57(Suppl):S31–3. doi: 10.1016/j.ypmed.2012.11.009. [DOI] [PubMed] [Google Scholar]
- 63.Reulen RC, de Vogel S, Zhong W, Zhong Z, Xie LP, Hu Z, et al. Physical activity and risk of prostate and bladder cancer in China: The South and East China case-control study on prostate and bladder cancer. PLoS One. 2017;12:e0178613. doi: 10.1371/journal.pone.0178613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Gu M-J, Huang Q-C, Bao C-Z, Li Y-J, Li X-Q, Ye D, et al. Attributable causes of colorectal cancer in China. BMC Cancer. 2018;18:38. doi: 10.1186/s12885-017-3968-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Biller VS, Leitzmann MF, Sedlmeier AM, Berger FF, Ortmann O, Jochem C. Sedentary behaviour in relation to ovarian cancer risk: a systematic review and meta-analysis. Eur J Epidemiol. 2021;36:769–80. doi: 10.1007/s10654-020-00712-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Guthold R, Stevens GA, Riley LM, Bull FC. Global trends in insufficient physical activity among adolescents: a pooled analysis of 298 population-based surveys with 1·6 million participants. Lancet Child Adolesc Health. 2020;4:23–35. doi: 10.1016/S2352-4642(19)30323-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Ellulu MS, Patimah I, Khaza’ai H, Rahmat A, Abed Y. Obesity and inflammation: the linking mechanism and the complications. Arch Med Sci. 2017;13:851–63. doi: 10.5114/aoms.2016.58928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Avgerinos KI, Spyrou N, Mantzoros CS, Dalamaga M. Obesity and cancer risk: emerging biological mechanisms and perspectives. Metabolism. 2019;92:121–35. doi: 10.1016/j.metabol.2018.11.001. [DOI] [PubMed] [Google Scholar]
- 69.De Pergola G, Silvestris F. Obesity as a major risk factor for cancer. J Obes. 2013;2013:291546. doi: 10.1155/2013/291546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Liu Y, Warren Andersen S, Wen W, Gao YT, Lan Q, Rothman N, et al. Prospective cohort study of general and central obesity, weight change trajectory and risk of major cancers among Chinese women. Int J Cancer. 2016;139:1461–70. doi: 10.1002/ijc.30187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Chen Y, Liu L, Wang X, Wang J, Yan Z, Cheng J, et al. Body mass index and risk of gastric cancer: a meta-analysis of a population with more than ten million from 24 prospective studies. Cancer Epidemiol Biomarkers Prev. 2013;22:1395. doi: 10.1158/1055-9965.EPI-13-0042. [DOI] [PubMed] [Google Scholar]
- 72.Sohn W, Lee HW, Lee S, Lim JH, Lee MW, Park CH, et al. Obesity and the risk of primary liver cancer: a systematic review and meta-analysis. Clin Mol Hepatol. 2021;27:157–74. doi: 10.3350/cmh.2020.0176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Ren X, Zhang X, Zhang X, Gu W, Chen K, Le Y, et al. Type 2 diabetes mellitus associated with increased risk for colorectal cancer: evidence from an international ecological study and population-based risk analysis in China. Public Health. 2009;123:540–4. doi: 10.1016/j.puhe.2009.06.019. [DOI] [PubMed] [Google Scholar]
- 74.Pan XF, Wang L, Pan A. Epidemiology and determinants of obesity in China. Lancet Diabetes Endocrinol. 2021;9:373–92. doi: 10.1016/S2213-8587(21)00045-0. [DOI] [PubMed] [Google Scholar]
- 75.Wang Y, Zhao L, Gao L, Pan A, Xue H. Health policy and public health implications of obesity in China. Lancet Diabetes Endocrinol. 2021;9:446–61. doi: 10.1016/S2213-8587(21)00118-2. [DOI] [PubMed] [Google Scholar]
- 76.National Office for Cancer Prevention and Control. National Cancer Control and Prevention Plan (1986–2000) China Cancer. 1985;9:336–7. [Google Scholar]
- 77.Chen X-Z, Liu Y, Wang R, Zhang W-H, Hu J-K. Improvement of cancer control in mainland China: epidemiological profiles during the 2004–10 National Cancer Prevention and Control Program. Lancet. 2016;388:S40. [Google Scholar]
- 78.Chinese Center for Disease Control and Prevention. [[Cited 2022 April 5]];China National Plan for NCD Prevention and Treatment (2012-2015) Available from: https://www.chinacdc.cn/en/ne/201207/t20120725_64430.html.
- 79.Bureau for Cancer Prevention and Control. [[Cited 2022 April 5]];China’s Cancer Prevention and Treatment Three-Year Action Plan (2015-2017) Available from: http://www.nhc.gov.cn/jkj/s5878/201509/656437bc5c7e4cd0afb581de85be998a.shtml.
- 80.The Central Government of the People’s Republic of China. [[Cited 2022 April 5]];Healthy China 2030. Available from: http://www.gov.cn/zhengce/2016-10/25/content_5124174.htm.
- 81.Bureau of Cancer Prevention and Control. [[Cited 2022 April 5]];Healthy China Action Plan (2019-2022) Available from: http://www.nhc.gov.cn/jkj/s5878/201909/2cb5dfb5d4f84f8881897e232b376b60.shtml.
- 82.Qu C, Chen T, Fan C, Zhan Q, Wang Y, Lu J, et al. Efficacy of neonatal HBV vaccination on liver cancer and other liver diseases over 30-year follow-up of the Qidong hepatitis B intervention study: a cluster randomized controlled trial. PLoS Med. 2014;11:e1001774. doi: 10.1371/journal.pmed.1001774. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Cao M, Fan J, Lu L, Fan C, Wang Y, Chen T, et al. Long term outcome of prevention of liver cancer by hepatitis B vaccine: Results from an RCT with 37 years. Cancer Lett. 2022;536:215652. doi: 10.1016/j.canlet.2022.215652. [DOI] [PubMed] [Google Scholar]
- 84.Liang X, Bi S, Yang W, Wang L, Cui G, Cui F, et al. Epidemiological serosurvey of hepatitis B in China – declining HBV prevalence due to hepatitis B vaccination. Vaccine. 2009;27:6550–7. doi: 10.1016/j.vaccine.2009.08.048. [DOI] [PubMed] [Google Scholar]
- 85.Liao X, Liang Z. Strategy vaccination against Hepatitis B in China. Hum Vaccin Immunother. 2015;11:1534–9. doi: 10.4161/21645515.2014.980206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Bureau for Cancer Prevention and Control. [[Cited 2022 April 5]];Great Achievements for the Contol of Hepatitis B. Available from: http://www.nhc.gov.cn/jkj/s3582/201307/518216575e544109b2caca07fca3b430.shtml.
- 87.Ribassin-Majed L, Lounes R, Clémençon S. Efficacy of vaccination against HPV infections to prevent cervical cancer in France: present assessment and pathways to improve vaccination policies. PLoS One. 2012;7:e32251. doi: 10.1371/journal.pone.0032251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Brisson M, Kim JJ, Canfell K, Drolet M, Gingras G, Burger EA, et al. Impact of HPV vaccination and cervical screening on cervical cancer elimination: a comparative modelling analysis in 78 low-income and lower-middle-income countries. Lancet. 2020;395:575–90. doi: 10.1016/S0140-6736(20)30068-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.ECNS.cn. [[Cited 2022 April 15]];China’s first domestic HPV vaccine earns WHO prequalification. Available from: http://www.ecns.cn/news/2021-10-18/detail-ihasacat0472343.shtml.
- 90.Liu Y, Di N, Tao X. Knowledge, practice and attitude towards HPV vaccination among college students in Beijing, China. Hum Vaccin Immunother. 2020;16:116–23. doi: 10.1080/21645515.2019.1638727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ji M, Huang Z, Ren J, Sun X, Wagner AL. Chinese vaccine providers’ perspectives on the HPV vaccine. Glob Pediatr Health. 2020;7:2333794X20967592. doi: 10.1177/2333794X20967592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Yin Y. HPV vaccination in China needs to be more cost-effective. Lancet. 2017;390:1735–6. doi: 10.1016/S0140-6736(17)32606-5. [DOI] [PubMed] [Google Scholar]
- 93.China Anti-Cancer Association. [[Cited 2022 June 10]];National Cancer Week. Available from: http://www.caca.org.cn/system/2020/03/27/020025350.shtml.
- 94.The Central Government of China. [[Cited 2022 April 5]];Healthy China Action (2019-2030) Available from: http://www.gov.cn/xinwen/2019-07/15/content_5409694.htm.
- 95.Ding S-Z, Du Y-Q, Lu H, Wang W-H, Cheng H, Chen S-Y, et al. Chinese consensus report on family-based Helicobacter pylori infection control and management (2021 Edition) Gut. 2022;71:238–53. doi: 10.1136/gutjnl-2021-325630. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Peleteiro B, Lopes C, Figueiredo C, Lunet N. Salt intake and gastric cancer risk according to Helicobacter pylori infection, smoking, tumour site and histological type. Br J Cancer. 2011;104:198–207. doi: 10.1038/sj.bjc.6605993. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Cappuccio FP, Capewell S, Lincoln P, McPherson K. Policy options to reduce population salt intake. BMJ. 2011;343:d4995. doi: 10.1136/bmj.d4995. [DOI] [PubMed] [Google Scholar]
- 98.Zhang N, Ma G. Childhood obesity in China: trends, risk factors, policies and actions. Global Health J. 2018;2:1–13. [Google Scholar]
- 99.People’s Republic of China. [[Cited 2022 April 7]];Report on Chinese Residents’ Chronic Diseases and Nutrition 2020. Available from: http://www.gov.cn/xinwen/2020-12/24/content_5572983.htm.
- 100.National Cancer Center. Chinese Guideline for Cancer Registration: People’s Medical Publishing House; 2016 [Google Scholar]
- 101.Aberle DR, Adams AM, Berg CD, Black WC, Clapp JD, Fagerstrom RM, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395–409. doi: 10.1056/NEJMoa1102873. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Duffy SW, Vulkan D, Cuckle H, Parmar D, Sheikh S, Smith RA, et al. Effect of mammographic screening from age 40 years on breast cancer mortality (UK Age trial): final results of a randomised, controlled trial. Lancet Oncol. 2020;21:1165–72. doi: 10.1016/S1470-2045(20)30398-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Ding R, Xiao Y, Mo M, Zheng Y, Jiang Y-Z, Shao Z-M. Breast cancer screening and early diagnosis in Chinese women. Cancer Biol Med. 2022;19:450–67. doi: 10.20892/j.issn.2095-3941.2021.0676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Cao M, Li H, Sun D, He S, Yu Y, Li J, et al. Cancer screening in China: The current status, challenges, and suggestions. Cancer Lett. 2021;506:120–7. doi: 10.1016/j.canlet.2021.02.017. [DOI] [PubMed] [Google Scholar]
- 105.Bureau for Maternal and Child Helath. [[Cited 2022 April 5]];Report on China’s development of maternal and child health (2019) Available from: http://www.nhc.gov.cn/fys/s7901/201905/bbd8e2134a7e47958c5c9ef032e1dfa2.shtml.
- 106.National Health Commission of the People’s Republic of China. [[Cited 2022 April 5]];Response to the Question suggested by the Second Session of the 13th National Committee of the Chinese People’s Political Consultative Conference. Available from: http://www.nhc.gov.cn/wjw/tia/202009/6c18078d53e847b3afc50f412cd5df93.shtml.
- 107.Tianjin Municipal People’s Government. [[Cited 2022 April 5]];The interim data of the joint screening project for common malignant tumors. Available from: http://www.tj.gov.cn/sy/tjxw/202108/t20210806_5526832.html.
- 108.The People’s Government of Zhejiang Province. [[Cited 2022 April 5]];Notice of the implementation plan of the “three exemptions and three benefits” health action for urban and rural residents in Zhejiang Province. Available from: http://www.zj.gov.cn/art/2021/11/26/art_1229530772_2376859.html.
- 109.National Helath Commission of the People’s Republic of China. [[Cited 2022 April 8]];Response to the Question suggested by The Fourth Session of the 13th National Committee of the Chinese People’s Political Consultative Conference. Available from: http://www.nhc.gov.cn/wjw/tia/202201/84ec994244ff4b1883c9556712c1a608.shtml.
- 110.National Health Commission of the People’s Republic of China. [[Cited 2022 April 8]];Response to Recommendation No. 8901 of the Fourth Session of the Thirteenth National People’s Congress 2021. Available from: http://www.nhc.gov.cn/wjw/jiany/202112/0c05b5bc81cc4786975384fdb44cf7a4.shtml.
- 111.Sun Y, Zhu Z, Zhang J, Han P, Qi Y, Wang X, et al. Impacts of national drug price negotiation on expenditure, volume, and availability of targeted anti-cancer drugs in China: an interrupted time series analysis. Int J Environ Res Public Health. 2022;19:4578. doi: 10.3390/ijerph19084578. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 112.The Central Government of the People’s Republic of China. [[Cited 2022 June 8]];74 drugs to be added to national insurance list. Available from: http://english.www.gov.cn/statecouncil/ministries/202112/07/content_WS61aeb805c6d09c94e48a1cbd.html.
- 113.The Central Government of the People’s Republic of China. [[Cited 2022 June 8]];Reimbursement ratio for major disease increased to 60% Available from: http://www.gov.cn/xinwen/2019-05/12/content_5390775.htm.
- 114.National Clinical Research Center for Digestive Diseases, Chinese Society of Digestive Endoscopology, Chinese Society of Health Management, Chinese Digestive Endoscopist Committee of Chinese Endoscopist Association, Health Management and Physical Examination Committee of Digestive Endoscopy of Chinese Endoscopist Association, National Quality Control Center for Digestive Endoscopy, Society of Oncological Endoscopy of China, et al. China experts consensus on the protocol of early gastric cancer screening (2017, Shanghai) Chin J Dig Endosc. 2018;35:77–83. [Google Scholar]
- 115.General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer (2022 edition) J Clin Hepatol. 2022;38:288–303. [Google Scholar]
- 116.Luo H, Zhao Q, Wei W, Zheng L, Yi S, Li G, et al. Circulating tumor DNA methylation profiles enable early diagnosis, prognosis prediction, and screening for colorectal cancer. Sci Transl Med. 2020;12:eaax7533. doi: 10.1126/scitranslmed.aax7533. [DOI] [PubMed] [Google Scholar]