

Abstract
Although the outcome after myocardial infarction depends on the time to treatment, a delay between symptom onset and treatment is common. Apple Watch, a popular wearable device, provides the ability to perform an electrocardiogram. We review the progress made in using the Apple Watch to record multiple electrocardiogram leads for diagnosing myocardial infarction. Although the data are encouraging, many limitations remain, and more research is needed. Nevertheless, the Apple Watch could eventually serve as a self-check tool for patients who have chest pains or other symptoms of myocardial infarction, thus substantially decreasing the time to treatment and improving the outcome after myocardial infarction.
Keywords: Apple Watch, echocardiography/diagnosis, heart attack, myocardial infarction
About every 40 seconds, someone in the United States (US) has a myocardial infarction (MI).1 The outcomes after MI depend on the time that elapses before treatment begins. More than half of individuals who have an MI die in an emergency room or before reaching a hospital within an hour of symptom onset.2 The benefit of early treatment of MI is clear: survival rates increase by up to 50% if reperfusion is achieved within one hour of symptom onset and by 23% if achieved within 3 hours.3–5 Therefore, immediate treatment is essential. Without it, patients have higher rates of mortality and severe complications caused by increased infarct size, including cardiogenic shock, arrhythmias, and heart failure.6
To receive immediate diagnosis and treatment, patients need to seek medical attention as soon as symptoms develop. Unfortunately, in the US, the median time from symptom onset to hospital arrival ranges from 1.5 to 6 hours.7 Educating patients about the symptoms of MI is a highly recommended strategy for reducing the time to treatment.7,8 Although chest pain is a characteristic feature of MI, up to one-third of patients may not have this symptom, which can increase the difficulty of identifying the acute onset of MI.8 This may be why studies assessing this strategy have shown no reduction in delay time.8,9
The first diagnostic step for confirming MI is the traditional 12-lead electrocardiogram (ECG), which requires specific equipment and professional training to record and interpret. In 2018, Apple Inc. launched the Apple Watch series 4, touting its ability to record an ECG. If the ECG function of the Apple Watch, one of the most popular wearable devices globally, could provide a reliable analysis of MI risk when symptoms develop, it could then send a clear signal to the user to seek medical attention, thereby minimizing the delay in diagnosis and treatment.
Apple Watch's Electrocardiographic Function
The Apple Watch uses one positive electrode (on the back of the watch) and one negative electrode (at the digital crown) to record a single-lead ECG. In this simple procedure, the watch is worn on the left wrist, and the wearer launches the ECG application on the watch and touches the digital crown of the watch with a right-hand finger. The watch then makes a 30-second recording to generate a bipolar signal from the voltage differences between the left and right arms, simulating a conventional ECG lead I recording. Then, the ECG application can perform a rhythm analysis and classify the recording as sinus rhythm, bradycardia, tachycardia, atrial fibrillation, or inconclusive.10 Because the watch provides only single-lead information, Apple clearly indicates that it cannot be used to detect MI.10,11
Expanding Use of Apple Watch's Electrocardiographic Function
In the clinical setting, a 12-lead ECG is currently needed to diagnose MI. Many studies12–15 have examined the possibility of using the Apple Watch to record multiple leads to meet this requirement for a clinical diagnosis of MI.
Limb Leads I, II, and III
Electrocardiographic leads I, II, and III are an integral part of the standard 12-lead ECG in routine clinical applications. The Apple Watch can record lead I, and, according to the Einthoven triangle, it could acquire leads II and III by using different parts of the body.15 The watch could be placed on the left lower abdomen, the left thigh, or the left ankle, and lead II could be recorded by placing the right index finger on the crown of the watch; lead III could be recorded in the same manner by placing the left index finger on the crown (Fig. 1). The left lower abdomen has been shown to provide the best quality signal.13 Several studies12–18 have verified the overall accuracy of this approach and its comparability to the standard 12-lead ECG, and they have shown the signal's tracing quality and the duration and amplitude of waves generated by the Apple Watch to be suitable for diagnosis. Cardiologists have been able to correctly allocate in blinded fashion more than 90% of Apple Watch ECG signals to the corresponding standard ECG leads.15,17,18 These results suggest that the recording of leads I through III by the Apple Watch is accurate and highly comparable to their recording on a standard ECG.
Fig. 1.
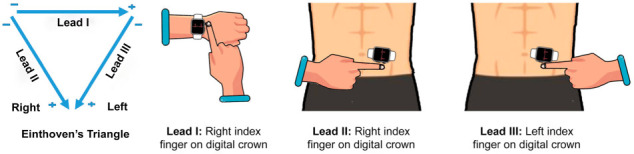
Illustration shows the Einthoven triangle and how to use the Apple Watch to record leads I through III.
From Behzadi A, Sepehri Shamloo A, Mouratis K, Hindricks G, Arya A, Bollmann A. Feasibility and reliability of smartwatch to obtain 3-lead electrocardiogram recordings. Sensors (Basel) 2020;20(18):5074.13 Used under the terms of the Creative Commons CC-BY license.
Precordial Leads V1 Through V6
Precordial leads (V1–V6) are also part of the standard 12-lead ECG and are important for identifying and locating an MI. During recording of the 12-lead ECG, the precordial leads are created by subtracting the potential at the Wilson central terminal (WCT) from the potential at each precordial electrode.19 The WCT is the average potential of the 3 limb potentials, R, L, and F. When an Apple Watch is placed in the same position as the precordial electrodes, it can also generate similar ECG signals; however, the reference point is the right or left arm for Apple Watch precordial recordings.20 Therefore, the resulting P-QRS-T waveforms are not identical to those of the corresponding leads generated by the WCT reference. If the watch is placed on the chest with the left finger touching the crown, the signals are designated CL1 through CL6. Accordingly, with the right finger touching the crown, the watch will generate CR1 to CR6 signals (Fig. 2). In most previous studies in which the Apple Watch was used to record precordial signals, CR signals were generated.14,21 These findings suggest that CR leads recorded by the Apple Watch correspond correctly to standard V leads.
Fig. 2.

Photographs show how to position the Apple Watch for obtaining precordial electrocardiograms. The precordial leads are recorded as CR1 through CR6, corresponding, respectively, to the locations of V1 (4th intercostal space right parasternal), V2 (4th intercostal space left parasternal), V3 (between V2 and V4), V4 (5th intercostal space midclavicular line), V5 (5th intercostal space anterior axillary line), and V6 (5th intercostal space midaxillary line).
From Spaccarotella CAM, Polimeni A, Migliarino S, Principe E, Curcio A, Mongiardo A, et al. Multichannel electrocardiograms obtained by a smartwatch for the diagnosis of ST-segment changes. JAMA Cardiol 2020;5(10):1176-80.21 Used under the terms of the Creative Commons CC-BY license.
However, considering the reference difference between the standard 12-lead ECG and the Apple Watch, the accuracy of the Apple Watch in detecting MI may be affected if the watch is following the 12-lead ECG threshold. For example, in one study that compared the CR/CL signals with the standard V leads, the sensitivity of CR/CL leads in detecting ST-segment elevation myocardial infarction (STEMI) was slightly lower.22 Therefore, further study is needed to ascertain whether the Apple Watch ECG needs exclusive criteria to detect MI accurately.
Another method to generate precordial lead signals using the Apple Watch has been proposed.17 This approach is similar to the CR recording, but requires using the left hand to enclose the right wrist. The ECG signal recorded through this approach is identical to that of the standard ECG. However, this method is more complicated for patients to use, and no other studies of this approach have been published.
Augmented Vector Leads aVL, aVR, and aVF
Augmented vector leads aVL, aVR, and aVF are also part of the standard 12-lead ECG. Using the Apple Watch, a bipolar system, to generate the augmented vector leads is difficult because it cannot create 2 negative poles.23 Although some methods are available for producing such signals on the Apple Watch, no peer-reviewed studies have been published that describe or compare their accuracy with that of the standard ECG.
Apple Watch in Detecting Myocardial Infarction
As discussed above, the Apple Watch can reliably produce a 9-lead ECG that includes leads I, II, and III and precordial leads similar to V1 through V6. Based on these findings, several reports12,14,24,25 and a study21 have been published on the use of the Apple Watch in detecting MI or acute coronary syndrome. The published research is limited, mostly in the form of case reports (Table I). In the most extensive study to date,21 Spaccarotella and colleagues enrolled 100 patients, including 54 patients with STEMI and 27 with non-STEMI. In that study, Apple Watch had a sensitivity of 93% and specificity of 95% for detecting STEMI, compared with a sensitivity of 94% and specificity of 92% for detecting non-STEMI.
TABLE I.
Studies of the Apple Watch in Detecting Myocardial Infarction
| Reference | Report Type | No. of Patients | Leads Recorded | Patient Type |
|---|---|---|---|---|
| Avila CO12 (2019) | Case report | 2 | I, II, and III | STEMI |
| Stark K, et al.25 (2020) | Case report | 1 | I | STEMI |
| Spaccarotella CAM, et al.21 (2020) | Prospective study | 100 | CR1–CR6,* I, II, and III | STEMI (n=54); non-STEMI (n=27); healthy controls (n=19) |
| Drexler M, et al.24 (2020) | Case report | 1 | I | Angina |
| Cobos Gil MA14 (2020) | Case report | 2 | CR1–CR6,* I, II, and III | STEMI (n=1); non-STEMI (n=1) |
CR = chest-right arm; STEMI = ST-elevation myocardial infarction
*Corresponding to conventional leads V1 through V6.
Although these published reports support the idea that the Apple Watch can detect the ST change during ischemic onset, the small test population undermines the reliability of the results. Larger-scale clinical trials are needed to examine how accurately the Apple Watch can not only rule in, but also rule out, an MI; no studies to date have addressed this aspect. Therefore, despite encouraging early results, studies of the Apple Watch for detecting MI are still in the proof-of-concept stage, with many limitations that need to be examined before the watch can be widely used to detect MI.
Technical Limitations
Technical differences between the Apple Watch ECG and the standard 12-lead ECG, such as the way in which precordial leads are recorded and described, may change the diagnostic criteria for MI. However, in the largest study so far,21 researchers clearly used the terminology of V1 through V6 instead of CR1 through CR6. Authors may omit the difference intentionally to make this concept more popular, but more work is necessary to define the criteria for the Apple Watch ECG. In addition, it is possible that the patient may record CL rather than CR signals; the effect of this scenario on the diagnosis of MI is unknown and needs further clarification.
Except in the case of the precordial leads, the Apple Watch ECG records leads asynchronously (sequentially); in contrast, the standard ECG can record multiple leads simultaneously. This difference can make J-point detection more difficult. In a study comparing the QT interval measured on asynchronous ECG leads versus on a standard ECG, clinically important differences (>20 ms) were observed in nearly 25% of the study population.26 Again, no studies have examined the differences between asynchronous and synchronous ECG acquisition, and all previous studies have used standard ECG criteria in Apple Watch–acquired ECGs. Data are needed to assess this type of comparison.
Study Protocol Limitations
Using the Apple Watch to detect MI is not meant to replace the standard 12-lead ECG. Rather, the Apple Watch could serve as a new MI screening tool for people at home or in other environments. In addition to ensuring the accuracy of the results, we need to focus on the patient experience and the convenience of using this approach. In the above-mentioned study of 100 patients,21 each patient needed to record 9 leads (I, II, III, and CR1–CR6) with the Apple Watch. This procedure may pose 2 challenges for patients. First, the process for acquiring the ECG is time-consuming. In the study by Spaccarotella's group,21 the average recording time was 5.73 minutes. In an emergency, an approximately 6-minute test involving 9 recording maneuvers may be too long and complicated. Second, patients without any knowledge of ECG recording may have difficulty recording all 9 leads accurately. Even professional staff can make mistakes by placing the chest electrodes (precordial leads) in the wrong place.27 Displacement of precordial leads can affect the ECG morphology and lead to a misdiagnosis.28,29 The issue of where patients should place the Apple Watch when recording an ECG has not been previously addressed. In most studies, the recording was performed or supervised by physicians, not patients. Moreover, no studies have compared results of recordings made by patients with those made by physicians. Accordingly, the reliability of the Apple Watch as a home tool for detecting MI is unknown. In a retrospective study of the use of artificial intelligence simulation, 3 asynchronous ECG leads (I, II, and V5) were able to detect MI, and 4 leads (I, II, V2, and V5) were an even better predictor.30 Although no studies based on these conclusions have been performed in humans, these results provide a potential direction for an Apple Watch study. Developing an easier self-check protocol that requires only 3 or 4 recordings may help regular users avoid mistakes and save time.
Future Challenges
Apple Watch is not the only wearable device on the market with an ECG function. Many similar products are available, such as the Fitbit Watch and the Galaxy Watch. These devices are ushering in a new era of consumer-driven health monitors. Although other mobile ECG devices such as the KardiaMobile 6L can provide more professional recordings, the popularity of the Apple Watch and other similar devices offers an important advantage. An estimated 20% of US residents currently own a wearable device, and the global market is expected to grow at a compound annual growth rate of 25%, reaching $70 billion by 2025.31 The expansion of telehealth during the COVID-19 pandemic further accelerated adoption of wearable devices. Thus, any healthcare breakthroughs based on these devices will benefit a large population. The Apple Watch and other wearable devices provide a powerful platform for tracking one's personal health status through functions that include recording ECGs; monitoring heart rate, oxygen saturation, and blood pressure; and applying other emerging techniques (e.g., biosensors for troponin32 and glucose33). This platform may offer a comprehensive solution for MI detection. For example, SmartCardia, a device that records ECGs and monitors multiple vital signs, has achieved 90% accuracy in detecting MI.34 With their panoply of functions and with further study, these wearable devices may improve diagnostic accuracy even more.
Despite this promise, achieving the goal of early MI detection relies on the awareness of the users and their long-term behaviors. Finding an effective way to educate a large population on how to use these smart devices and the importance of using them daily is challenging. In a clinical trial reported in 2016,35 investigators questioned the value of wearable devices in improving clinical outcomes without incentives. In a large population, improving MI outcomes with a wearable device may be difficult without widespread education on its correct use, even with a good MI detection plan.
Conclusion
The Apple Watch shows promise for detecting MI. Current studies have shown that it can record multiple-lead ECG signals and detect the ST change during MI. However, there are still many limitations to achieving the objective of early MI detection, and more clinical data are needed. Future work should aim at making the ECG recording procedure less complex. With further research, we believe that the Apple Watch and other wearable devices can play a prominent role in promoting heart health.
Acknowledgments
The authors thank Rebecca A. Bartow, PhD, of the Department of Scientific Publications at the Texas Heart Institute, for editorial support.
Funding Statement
Funding/support: None
Footnotes
Conflict of interest disclosures: None
References
- 1.Center for Disease Control and Prevention Heart attack symptoms, risk, and recovery. [Internet]. Available from: https://www.cdc.gov/heartdisease/heart_attack.htm [cited 2022 January 10; accessed 2022 June 6]
- 2.Thom T, Haase N, Rosamond W, Howard VJ, Rumsfeld J, Manolio T et al. Heart disease and stroke statistics--2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation . 2006;113(6):e85–151. doi: 10.1161/CIRCULATIONAHA.105.171600. [DOI] [PubMed] [Google Scholar]
- 3.De Luca G, Suryapranata H, Ottervanger JP, Antman EM. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: every minute of delay counts. Circulation . 2004;109(10):1223–5. doi: 10.1161/01.CIR.0000121424.76486.20. [DOI] [PubMed] [Google Scholar]
- 4.Gersh BJ, Stone GW, White HD, Holmes DR. Pharmacological facilitation of primary percutaneous coronary intervention for acute myocardial infarction is the slope of the curve the shape of the future? JAMA . 2005;293(8):979–86. doi: 10.1001/jama.293.8.979. [DOI] [PubMed] [Google Scholar]
- 5.Simoons ML, Serruys PW, van den Brand M, Res J, Verheugt FW, Krauss XH et al. Early thrombolysis in acute myocardial infarction: limitation of infarct size and improved survival. J Am Coll Cardiol . 1986;7(4):717–28. doi: 10.1016/s0735-1097(86)80329-1. [DOI] [PubMed] [Google Scholar]
- 6.Krumholz HM, Normand ST, Wang Y. Twenty-year trends in outcomes for older adults with acute myocardial infarction in the United States. JAMA Netw Open . 2019;2(3):e191938. doi: 10.1001/jamanetworkopen.2019.1938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Moser DK, Kimble LP, Alberts MJ, Alonzo A, Croft JB, Dracup K et al. Reducing delay in seeking treatment by patients with acute coronary syndrome and stroke: a scientific statement from the American Heart Association Council on cardiovascular nursing and stroke council. Circulation . 2006;114(2):168–82. doi: 10.1161/CIRCULATIONAHA.106.176040. [DOI] [PubMed] [Google Scholar]
- 8.Finn JC, Bett JH, Shilton TR, Cunningham C, Thompson PL. Patient delay in responding to symptoms of possible heart attack: can we reduce time to care? Med J Aust . 2007;187(5):293–8. doi: 10.5694/j.1326-5377.2007.tb01247.x. [DOI] [PubMed] [Google Scholar]
- 9.Hand M, Brown C, Horan M, Simons-Morton D. The National Heart Attack Alert Program: progress at 5 years in educating providers, patients, and the public and future directions. J Thromb Thrombolysis . 1998;6(1):9–17. doi: 10.1023/A:1008868020782. [DOI] [PubMed] [Google Scholar]
- 10.Apple Take an ECG with the ECG app on Apple Watch. [Internet]. Available from: https://support.apple.com/en-us/HT208955 [cited 2022 January 10; accessed 2022 June 6]
- 11. De novo classification request for ECG app. [Internet]. Available from: https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN180044.pdf [cited 2022 January 10; accessed 2022 June 6]
- 12.Avila CO. Novel use of Apple Watch 4 to obtain 3-lead electrocardiogram and detect cardiac ischemia. Perm J . 2019;23:19–025. doi: 10.7812/TPP/19-025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Behzadi A, Sepehri Shamloo A, Mouratis K, Hindricks G, Arya A, Bollmann A. Feasibility and reliability of smartwatch to obtain 3-lead electrocardiogram recordings. Sensors (Basel) . 2020;20(18):5074. doi: 10.3390/s20185074. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cobos Gil MA. Standard and precordial leads obtained with an Apple Watch. Ann Intern Med . 2020;172(6):436–7. doi: 10.7326/M19-2018. [DOI] [PubMed] [Google Scholar]
- 15.Samol A, Bischof K, Luani B, Pascut D, Wiemer M, Kaese S. Recording of bipolar multichannel ECGs by a smartwatch: modern ECG diagnostic 100 years after Einthoven. Sensors (Basel) . 2019;19(13):2894. doi: 10.3390/s19132894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Frisch DR. A novel technique to expand the electrocardiographic recording capability from an Apple Watch. Am J Med . 2019;132(8):940–1. doi: 10.1016/j.amjmed.2019.03.005. [DOI] [PubMed] [Google Scholar]
- 17.Samol A, Bischof K, Luani B, Pascut D, Wiemer M, Kaese S. Single-lead ECG recordings including Einthoven and Wilson leads by a Smartwatch: a new era of patient directed early ECG differential diagnosis of cardiac diseases? Sensors (Basel) . 2019;19(20):4377. doi: 10.3390/s19204377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Samol A, Bischof K, Luani B, Pascut D, Wiemer M, Kaese S. Patient directed recording of a bipolar three-lead electrocardiogram using a smartwatch with ECG function. J Vis Exp . 2019;(154) doi: 10.3791/60715. [DOI] [PubMed] [Google Scholar]
- 19.Gargiulo GD. True unipolar ECG machine for Wilson central terminal measurements. BioMed Res Int . 2015;2015:586397. doi: 10.1155/2015/586397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Baquero GA, Banchs JE, Ahmed S, Naccarelli GV, Luck JC. Surface 12 lead electrocardiogram recordings using smart phone technology. J Electrocardiol . 2015;48(1):1–7. doi: 10.1016/j.jelectrocard.2014.09.006. [DOI] [PubMed] [Google Scholar]
- 21.Spaccarotella CAM, Polimeni A, Migliarino S, Principe E, Curcio A, Mongiardo A et al. Multichannel electrocardiograms obtained by a smartwatch for the diagnosis of ST-segment changes. JAMA Cardiol . 2020;5(10):1176–80. doi: 10.1001/jamacardio.2020.3994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Lindow T, Engblom H, Khoshnood A, Ekelund U, Carlsson M, Pahlm O. Chest-lead ST-J amplitudes using arm electrodes as reference instead of the Wilson central terminal in smartphone ECG applications: Influence on ST-elevation myocardial infarction criteria fulfillment. Ann Noninvasive Electrocardiol . 2018;23(5):e12549. doi: 10.1111/anec.12549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Wilkinson-Stokes M. Einthoven and precordial lead accuracy of smartwatch-acquired electrocardiographs: a review of the literature. Australasian Journal of Paramedicine . 2020:17. [Google Scholar]
- 24.Drexler M, Elsner C, Gabelmann V, Gori T, Munzel T. Apple Watch detecting coronary ischaemia during chest pain episodes or an apple a day may keep myocardial infarction away. Eur Heart J . 2020;41(23):2224. doi: 10.1093/eurheartj/ehaa290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Stark K, Czermak T, Massberg S, Orban M. Watch out for ST-elevation myocardial infarction: a case report of ST-elevation in single-lead electrocardiogram tracing of a smartwatch. Eur Heart J Case Rep . 2020;4(6):1–4. doi: 10.1093/ehjcr/ytaa353. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Holkeri A, Eranti A, Kentta TV, Noponen K, Haukilahti MAE, Seppanen T et al. Experiences in digitizing and digitally measuring a paper-based ECG archive. J Electrocardiol . 2018;51(1):74–81. doi: 10.1016/j.jelectrocard.2017.09.007. [DOI] [PubMed] [Google Scholar]
- 27.Rudiger A, Schob L, Follath F. Influence of electrode misplacement on the electrocardiographic signs of inferior myocardial ischemia. Am J Emerg Med . 2003;21(7):574–7. doi: 10.1016/j.ajem.2003.08.007. [DOI] [PubMed] [Google Scholar]
- 28.Kania M, Rix H, Fereniec M, Zavala-Fernandez H, Janusek D, Mroczka T et al. The effect of precordial lead displacement on ECG morphology. Med Biol Eng Comput . 2014;52(2):109–19. doi: 10.1007/s11517-013-1115-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Rajaganeshan R, Ludlam CL, Francis DP, Parasramka SV, Sutton R. Accuracy in ECG lead placement among technicians, nurses, general physicians and cardiologists. Int J Clin Pract . 2008;62(1):65–70. doi: 10.1111/j.1742-1241.2007.01390..x. [DOI] [PubMed] [Google Scholar]
- 30.Han C, Song Y, Lim HS, Tae Y, Jang JH, Lee BT et al. Automated detection of acute myocardial infarction using asynchronous electrocardiogram signals-preview of implementing artificial intelligence with multichannel electrocardiographs obtained from smartwatches: retrospective study. J Med Internet Res . 2021;23(9):e31129. doi: 10.2196/31129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Polaris Market Research Healthcare analytics market share, size, trends, industry analysis report. [Internet]. Available from https://www.polarismarketresearch.com/industry-analysis/healthcare-analytics-market [cited 2022 January 10; accessed 2022 June 6]
- 32.Redon P, Shahzad A, Iqbal T, Wijns W. Development of a new detection algorithm to identify acute coronary syndrome using electrochemical biosensors for real-world long-term monitoring. Bioengineering (Basel) . 2021;8(2):28. doi: 10.3390/bioengineering8020028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Pontius K, Semenova D, Silina YE, Gernaey KV, Junicke H. Automated electrochemical glucose biosensor platform as an efficient tool toward on-line fermentation monitoring: novel application approaches and insights. Front Bioeng Biotechnol . 2020;8:436. doi: 10.3389/fbioe.2020.00436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Sopic D, Aminifar A, Aminifar A, Atienza D. Real-time event-driven classification technique for early detection and prevention of myocardial infarction on wearable systems. IEEE Trans Biomed Circuits Syst . 2018;12(5):982–92. doi: 10.1109/TBCAS.2018.2848477. [DOI] [PubMed] [Google Scholar]
- 35.Finkelstein EA, Haaland BA, Bilger M, Sahasranaman A, Sloan RA, Nang EEK, Evenson KR. Effectiveness of activity trackers with and without incentives to increase physical activity (TRIPPA): a randomised controlled trial. Lancet Diabetes Endocrinol . 2016;4(12):983–95. doi: 10.1016/S2213-8587(16)30284-4. [DOI] [PubMed] [Google Scholar]