

Abstract
Objective
This study aimed to assess the technical feasibility, efficacy, and safety of the safe triangular working zone (STWZ) approach applied in percutaneous vertebroplasty (PV) for spinal metastases involving the posterior part of the vertebral body.
Materials and Methods
We prospectively enrolled 87 patients who underwent PV for spinal metastasis involving the posterior part of the vertebral body, with or without the STWZ approach, from January 2019 to April 2022. Forty-nine patients (27 females and 22 males; mean age ± standard deviation [SD], 57.2 ± 11.6 years; age range, 31–76 years) were included in group A (with STWZ approach), accounting for 54 vertebrae. Thirty-eight patients (18 females and 20 males; 59.1 ± 10.9 years; 29–81 years) were included in group B (without STWZ approach), accounting for 57 vertebrae. Patient demographics, procedure-related variables, and pain relief as assessed using the visual analog scale (VAS) were collected at different time points. Tumor recurrence in the vertebrae after PV was analyzed using Kaplan–Meier curves.
Results
The STWZ approach was successful from T1 to L5 without severe complications. Cement filling was satisfactory in 47/54 (87.0%) and 25/57 (43.9%) vertebrae in groups A and B, respectively (p < 0.001). Cement leakage was not significantly different between groups A and B (p = 1.000). Mean VAS score ± SD before and 1 week and 1, 3, 6, 9, and 12 months after PV were 7.6 ± 1.8, 4.2 ± 2.0, 2.7 ± 1.9, 1.9 ± 1.5, 1.7 ± 1.4, 1.7 ± 1.1, and 1.6 ± 1.3, respectively, in group A and 7.2 ± 1.7, 4.0 ± 1.3, 3.4 ± 1.6, 2.4 ± 1.2, 1.8 ± 1.0, 1.4 ± 0.5, and 1.7 ± 0.9, respectively, in group B. Kaplan–Meier analysis showed a lower tumor recurrence rate in group A than in group B (p = 0.001).
Conclusion
The STWZ approach may represent a new, safe, alternative/auxiliary approach to target the posterior part of the vertebral body in the PV for spinal metastases.
Keywords: Percutaneous vertebroplasty, Puncture approach, Spinal metastases
INTRODUCTION
Percutaneous vertebroplasty (PV) is a well-established technique for the treatment of benign and malignant compression fractures, as well as for the consolidation and palliation of osteoporotic vertebral compression fractures and painful lytic tumors [1,2].
In the PV approach, transpedicular and extrapedicular approaches are the two traditional methods for the needle to be applied to the affected vertebral body. However, under certain conditions, these traditional approaches cannot meet the demand if polymethylmethacrylate (PMMA) does not effectively fill the vertebral body. The transpedicular approach is limited in that it may not be possible to place needles in appropriate locations because of the constrained puncture angle [3]. Furthermore, it is difficult to apply the transpedicular PV approach when the vertebra has short and narrow pedicles.
Some researchers have improved the transpedicular approach by developing the extrapedicular approach, which increases the puncture angle [4,5]. However, the extrapedicular approach might cause fracture of the transverse process and injury to the ligament complex and segmental artery [6,7]. Moreover, the extrapedicular approach may lead to more serious complications, such as pulmonary embolism and compression of neural structures [8,9].
Considering the feeding angle of the needle, the location of the vertebral body and the related targeted area, improvement and appropriate placement of the needle during surgery are needed [10]. The safe triangular working zone (STWZ) is bordered anteriorly by the exiting root, inferiorly by the proximal plate of the lower lumbar segment, posteriorly by the proximal articular process of the vertebra, and medially by the traversing nerve root and dural sac [11,12]. The STWZ is widely used to access critical structures in a variety of spinal procedures and transforaminal epidural injections [13].
We assumed that the STWZ would be a useful approach when there is a need to target the posterior vertebra. For the first time, we applied the STWZ approach in treating spinal metastases to target the posterior part of the vertebral body to obtain appropriate placement of the needle and achieve satisfactory filling of the cement. This study aimed to assess the technical feasibility, efficacy, and safety of PV using the STWZ approach for spinal metastases involving the posterior part of the vertebral body.
MATERIALS AND METHODS
Patient Inclusion
This prospective, non-randomized, observational study was conducted at a single center. Approval was obtained from the Institutional Review Board (IRB No. 2018-0214). The patient was informed of the risk of nerve or vascular damage in the STWZ approach if the surgery was performed. Informed consent was obtained from all patients before the procedure.
From January 2019 to April 2022, 109 patients were enrolled consecutively and underwent PV of the spine in a digital subtraction angiography (DSA; Siemens Biplannar Artiz) room. The inclusion criteria were as follows: patients aged > 18 years who had malignant disease clinically diagnosed in conjunction with either a CT and MRI scan and had pain with a visual analog scale score (VAS) above 4. Patients who had the following conditions were considered to undergo the STWZ approach: 1) tumor involving the posterior part of the vertebral body, 2) the tumor covered the entire vertebra, and 3) the vertebral body was severely damaged (> 50% degree of osteolytic destruction) [14]. To compare the efficiency of this approach, under the same conditions, the other patients underwent PV using traditional approaches (transpedicular or extrapedicular approach) without STWZ assistance. The exclusion criteria were as follows: life expectancy < 1 month, irreversible coagulopathy, active infection, neurological deficit, mechanical instability, or risk from anesthesia. After further excluding 22 patients lost to follow-up after PV, 49 patients (with 54 vertebrae) in the STWZ approach group (group A) and 38 patients (with 57 vertebrae) in the non-STWZ group (group B) were finally included. Figure 1 shows the patient flowchart in this study.
Fig. 1. Patient flow diagram.

STWZ = safe triangular working zone
Patient Preparation before PV
The procedure was performed under sterile conditions. Blood pressure, heart rate, electrocardiography, and pulse oximetry were continuously monitored. The patient was placed in a prone position on a radiolucent operating table. Two fluoroscopic machines were used for simultaneous anteroposterior projections (APs) and lateral projections (LPs) of the spine. After preparing the skin and draping the patient, the treated vertebra was centered on the fluoroscope. The appropriate access point, puncture angle, and distance from the skin to the lesion were determined in advance based on the CT or MR images. Preoperative MR or CT imaging was used to evaluate the proper distance and puncture angle to avoid the nerve root. PV was performed by physicians with 10–20 years of experience. All patients who underwent PV were assigned specific clinico-radiological criteria in accordance with the CIRSE guidelines for vertebral augmentation [15].
STWZ Approach Process
During the puncture process, the transpedicular and/or extrapedicular approaches were performed first, and the STWZ approach was performed subsequently, forming group A. If transpedicular and/or extrapedicular approaches were performed without the STWZ approach, the patients were included in group B. The enrolled patients (or their family members) made informed decisions regarding the use of the STWZ approach after receiving explanations from the practitioner. Transpedicular and extrapedicular approaches were performed according to a previous article [5]. The steps involved in the STWZ technique are shown in Figure 2.
Fig. 2. Diagrams (A to F) showing the steps involved in the technique to perform PV via the STWZ approach.

A. Local anesthesia administered via the STWZ approach targeted the posterior point of the periosteum. B. In the LP view, the disposable coaxial biopsy needle with a blunt core needle was carefully advanced until it approached the vertebral body posteriorly, and the patient’s response was continuously monitored. C. The EV catheter needle replaced the blunt core needle coaxially. D, E. The bevel needle sheath was punctured through the EV, then the EV was removed with the inner needle inserted. F. With the help of a hammer, the bevel needle was guided toward the target zone or adjusted to many angles within the vertebral body. LP = lateral projection, PV = percutaneous vertebroplasty, STWZ = safe triangular working zone approach
First step: under fluoroscopy guidance, 1% lidocaine was administered after reaching the periosteum of the posterior part of the vertebral body via the STWZ.
Second step: in the LP view, a disposable coaxial biopsy needle (Bard Peripheral Vascular Inc.) with a blunt core needle was carefully advanced until it approached the posterior vertebral body. During penetration of the STWZ, the patient’s responses and feelings were continuously monitored. If the patient felt a sharp electronic shock-like sensation, the direction of the needle was changed accordingly. This procedure ensures that the puncture route acts in the STWZ area and that the blunt needle does not damage the nerve root. This procedure also provides a safe route for the next step, as it leaves the exiting nerve root course superiorly, laterally, and anteriorly.
Third step: the inner needle trocar of the EV catheter needle (HAKKO ELASTER) was removed from the tail and the blunt core needle was coaxially changed. The EV remained, and disposable coaxial biopsy needle trocars were drawn back.
Fourth step: a bevel needle sheath (Cook Inc.) was punctured through the EV, then the EV was removed with the inner needle inserted. Using a hammer, the bevel needle was guided toward the target zone at a designated angle or adjusted to other angles within the vertebral body.
After removing the inner needle, commercially available PMMA (SimplexP; HowmedicaOsteonics) was carefully injected into the vertebral body under continuous fluoroscopic monitoring. The injection was stopped if it became difficult because of high resistance or when the cement reached the posterior vertebral wall or entered the extraosseous space.
Outcome Evaluation
Immediately after the procedure, standard anterior and lateral radiographs were obtained to assess cement distribution, cement leakage, or other possible local complications. The patients were observed overnight and discharged during the following few days if the clinical course was uneventful. Patients were followed up clinically in the first week, first month, and every 3 months after PV. Technical success and complications, such as wound infections, nerve injuries, and pulmonary embolism, were recorded for all patients.
The patients were clinically examined by two physicians who gathered initial and follow-up data before the procedure, and outcome measures were repeated at fixed times of 1 week and 1, 3, 6, 9, and 12 months after the procedure. The pre-specified primary outcome measures were modified using a VAS score ranging from 0 (no pain) to 10 (worst pain ever) at different time points: short-term (1 week), medium-term (1–3 months), and long-term (6–12 months) [16].
Clinical Data Collection
For each group’s patient and procedure, the patients’ sex, age, and diagnosis were collected, and the involved vertebral level and previous radiotherapy given at the treated site were recorded. The involved vertebral levels were T1–L5 (i.e., 17 vertebral levels); therefore, we divided them into four group, each with four contiguous levels of vertebrae, except for the first group, which was assigned one extra vertebra (T1–5, T6–9, T10–L1, and L2–5). In addition, the technique used to access the target vertebra, technical success, complications, leakage of cement (including paravertebral, epidural, intervertebral disc, neural canal, and paravertebral vessel leakage), and the amount of bone cement used were analyzed. Postprocedural pain relief was evaluated using the VAS and compared with the baseline level of pain.
CT or X-ray was performed within 2 days to assess cement leakage. The distribution of cement filling the vertebral body after vertebroplasty was assessed using standard anterior and lateral radiographs. The vertebral body was divided into nine equal sections on the AP and LP, including one central and eight peripheral sections. If the cement was observed in every section, the filling was considered satisfactory. If any section was cement-free, the filling was considered unsatisfactory [17].
Statistical and Quantitative Assessments
Dichotomous and categorical data are reported as numbers (percentages). Continuous data are reported as mean ± standard deviation (SD) and range. Kaplan–Meier analysis was performed to investigate tumor recurrence in the targeted vertebra after vertebroplasty. Fisher’s exact test or the Mann–Whitney U test was used for quantitative variables. Statistical significance was set at p < 0.05. All statistical analyses were performed using R software (version 4.0.2; http://www.r-project.org).
RESULTS
Patients
The population included 45 female and 42 male patients referred for PV in T1 to L5; the clinical characteristics of all the patients are shown in Table 1. In group A, 54 vertebrae were treated in 49 patients (27 females and 22 males; mean age ± SD, 57.2 ± 11.6 years; age range, 31–76 years). In group B, 57 vertebrae were treated in 38 patients (18 females and 20 males; mean age ± SD, 59.1 ± 10.9 years; age range, 29–81 years). There were no significant differences between the two groups in age, sex, or various vertebral variables, except for the treated vertebral level, as shown in Table 1. The primary origins of the spinal metastases found in the included patients are shown in Figure 3.
Table 1. Demographics and Baseline Characteristics.
| Parameters | Group A | Group B | P | ||
|---|---|---|---|---|---|
| Patient parameters | |||||
| Number | 49 | 38 | |||
| Age in year, mean ± SD (range) |
57.2 ± 11.6 (31–76) | 59.1 ± 10.9 (29–81) | 0.441 | ||
| Sex | 0.617 | ||||
| Female | 27 (55.1) | 18 (47.4) | |||
| Male | 22 (44.9) | 20 (52.6) | |||
| Vertebra parameters | |||||
| Number | 54 | 57 | |||
| Treated vertebra level | 0.002 | ||||
| T1–T5 | 6 (11.1) | 20 (35.1) | |||
| T6–T9 | 6 (11.1) | 13 (22.8) | |||
| T10–L1 | 19 (35.2) | 13 (22.8) | |||
| L2–L5 | 23 (42.6) | 11 (19.3) | |||
| Included reason | 0.148 | ||||
| I1 | 24 (44.4) | 20 (35.1) | |||
| I2 | 8 (14.8) | 19 (33.3) | |||
| I3 | 20 (37.0) | 17 (29.8) | |||
| I4 | 2 (3.7) | 1 (1.8) | |||
| Indication for PV | 0.413 | ||||
| Pathologic fracture | 29 (53.7) | 36 (63.2) | |||
| Painful tumor | 25 (46.3) | 21 (36.8) | |||
| Rupture of the posterior vertebral wall | 1.000 | ||||
| No | 24 (44.4) | 25 (43.9) | |||
| Yes | 30 (55.6) | 32 (56.1) | |||
| Previous radiotherapy | 0.400 | ||||
| No | 40 (74.1) | 47 (82.5) | |||
| Yes | 14 (25.9) | 10 (17.5) | |||
Data are presented as the number of patients or vertebrae with the corresponding percentages in parentheses, unless specified otherwise. I1 indicates the tumor occurred in the posterior part of the vertebral body, I2 indicates the tumor covered the entire vertebra, I3 indicates the vertebral body was severely damaged, and I4 indicates the tumor relapsed in the posterior part of the vertebral body. PV = percutaneous vertebroplasty, SD = standard deviation
Fig. 3. Primary origin of vertebral tumors in all included patients.
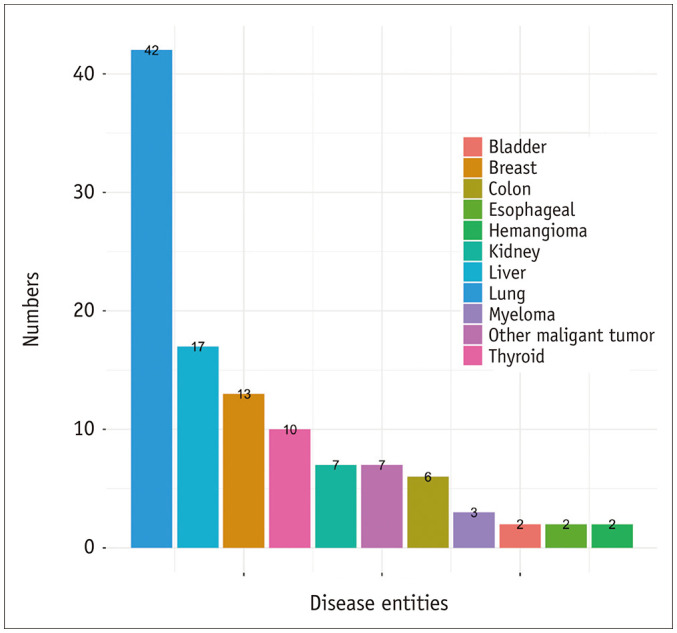
The number on top of the bar indicates the number of certain tumor types, the different colors represent the different tumor types.
Safety, Application, and Feasibility of STWZ Approach
The STWZ approach was technically successful and well-tolerated in all patients. No damage to the surrounding tissue (nerve damage or spinal damage) was observed. No severe complications related to STWZ were observed. The incidence of complications did not differ between groups (Table 2). Examples of vertebrae treated with the STWZ approach are shown in Figures 4 and 5.
Table 2. The Indicators Related to PV in Group A and B.
| Parameters | Group A (n = 54) |
Group B (n = 57) |
P | |
|---|---|---|---|---|
| The number of needle puncture | < 0.001 | |||
| Median (min, max) | 3.0 (1.0, 5.0) |
2.0 (1.0, 3.0) |
||
| The volume of cement injected, mL | 0.186 | |||
| Mean ± SD | 6.0 ± 1.4 | 5.7 ± 1.5 | ||
| Median (min, max) | 6.0 (2.0, 10.0) |
6.0 (2.0, 9.0) |
||
| The cement filling | < 0.001 | |||
| Satisfied | 47 (87.0) | 25 (43.9) | ||
| Unsatisfied | 7 (13.0) | 32 (56.1) | ||
| The leakage of cement (no, yes) | 1, 53 | 1, 56 | 1.000 | |
| Paravertebral leakage | 15, 39 | 19, 38 | 0.368 | |
| Intervertebral disc leakage | 43, 11 | 37, 20 | 1.000 | |
| Neural canal leakage | 43, 11 | 36, 21 | 1.000 | |
| Paravertebral vessel leakage | 18, 36 | 12, 45 | 1.000 | |
| The analgesic used after PV (no, yes) | 43, 11 | 51, 6 | 0.240 | |
| Complications | 0.065 | |||
| Fever | 8 (14.8) | 3 (5.3) | ||
| Stomach upset | 0 (0) | 1 (1.8) | ||
| Pain | 3 (5.6) | 0 (0) | ||
| Admission length after the PV, day | 0.433 | |||
| Mean ± SD | 4.6 ± 3.2 | 4.2 ± 2.3 | ||
| Median (min, max) | 4.0 (0, 14.0) |
4.0 (0, 10) |
||
Data represent the number of vertebrae with the corresponding percentages in parentheses, unless specified otherwise. PV = percutaneous vertebroplasty, SD = standard deviation
Fig. 4. Example patient.

A-D. Sagittal CT view (A1, A2) and axial T2-weighted MR image (B1, B2) show the lumbar spine in a 70-year-old male who suffered spinal pain after screw fixation and fracture of the L4 vertebra following metastasis from lung cancer with rupture of the posterior wall (A1 to B1 for preoperative imaging; A2 to B2 for postoperative imaging). C1, C2 and D1, D2 show the digital subtraction angiography scan, A2 to B2 show the cement covering the vertebra and tumor, B2 image shows that the tumor is smaller after vertebroplasty than before, with relief of the spinal pain. The arrows indicate the safe triangular working zone approach.
Fig. 5. Example patient.

A-F. MRI scans of tumors occurring in the posterior vertebral body in a 46-year-old male with adenocarcinoma of the liver with bone metastases (A, B). STWZ was performed to target the bone metastasis tumor (C, D) with radiofrequency ablation and achieved satisfactory cement fulfillment (E, F). The arrows indicate the STWZ approach. STWZ = safe triangular working zone
The procedure-related parameters are listed in Table 2. The PMMA filling quality was satisfactory in 47/54 (87.0%) and unsatisfactory in 7/54 (13.0%) in group A, and satisfactory in 25/57 (43.9%) and unsatisfactory in 32/57 (56.1%) in group B (p < 0.001, group A vs. group B). The difference in cement leakage between groups A and B was not significant (p = 1.000) (Table 2).
Efficacy of the Procedure
The VAS score showed pain relief at 1 and 3 months in groups A (both p < 0.001) and B (both p < 0.001) relative to baseline (Fig. 6). The VAS scores before and 1 week and 1, 3, 6, 9, and 12 months after PV were 7.6 ± 1.8, 4.2 ± 2.0, 2.7 ± 1.9, 1.9 ± 1.5, 1.7 ± 1.4, 1.7 ± 1.1, and 1.6 ± 1.3, respectively, in group A; and 7.2 ± 1.7, 4.0 ± 1.3, 3.4 ± 1.6, 2.4 ± 1.2, 1.8 ± 1.0, 1.4 ± 0.5, and 1.7 ± 0.9, respectively, in group B. There was no difference in VAS scores between groups A and B during follow-up (Table 3).
Fig. 6. VAS score in groups A and B.

A. VAS at baseline (VAS 0) and after 1 and 3 months (VAS 1 and VAS 3) in group A. B. VAS at baseline (VAS 0) and after 1 and 3 months (VAS 1 and VAS 3) in group B. C. The improvement in VAS scores are shown for both groups. For the included patients, a new baseline was established before the procedure, and follow-up was performed at 1, 3, 6, 9 and 12 months after percutaneous vertebroplasty in groups A (red) and B (blue). *p < 0.001 in comparison with baseline (preoperation). VAS = visual analog scale
Table 3. Summary of VAS Score Results.
| Parameter | Group A | Group B | P | |
|---|---|---|---|---|
| Pre-procedural | 7.6 ± 1.8 | 7.2 ± 1.7 | 0.236 | |
| Post-procedural | ||||
| 1 week | 4.2 ± 2.0 | 4.0 ± 1.3 | 0.491 | |
| 1 month | 2.7 ± 1.9 | 3.4 ± 1.6 | 0.052 | |
| 3 months | 1.9 ± 1.5 | 2.4 ± 1.2 | 0.124 | |
| 6 months | 1.7 ± 1.4 | 1.8 ± 1.0 | 0.525 | |
| 9 months | 1.7 ± 1.1 | 1.4 ± 0.5 | 0.406 | |
| 12 months | 1.6 ± 1.3 | 1.7 ± 0.9 | 0.747 | |
Data are mean ± standard deviation.
Recurrence after PV
The Kaplan–Meier curve is shown in Figure 7. A total of 54 and 57 vertebrae were studied in groups A and B, respectively. There were four and 18 cases of vertebral recurrence in groups A and B, respectively. The median time to recurrence in group A was 19.0 ± 5.1 (95% confidence interval [CI]: 9.1, 28.9) months. The tumor recurrence rate was statistically different between the two groups (χ2 = 10.6, p = 0.001, log-rank test; Fig. 7).
Fig. 7. Kaplan–Meier curve shows the cumulative proportion of vertebral recurrence after vertebroplasty.
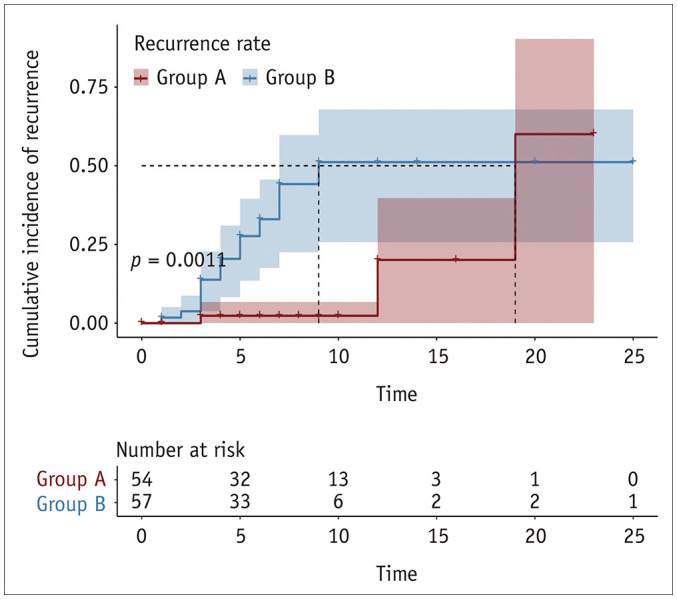
Group A (red) had lower tumor recurrence rate in the vertebrae than group B (blue).
DISCUSSION
In this study, we reported our 3-year experience with the STWZ approach in 54 vertebrae undergoing PV with STWZ assistance mainly because of underlying spinal metastases. The STWZ approach was successfully established and targeted the posterior part of the vertebral body, and it could be an alternative or auxiliary puncture method over wide vertebral levels.
Based on our clinical experience, the STWZ approach could be performed alternatively or additionally in PV: 1) if the traditional approach (transpedicular or extrapedicular approach) was not available because of vertebral deformation, or if the cement or internal fixation nail did not allow extra space for traditional punctures, 2) if the tumor occurred or relapsed in the vertebral body in the posterior part of the vertebral body, 3) if the distribution of cement was not adequate to cover the tumor as much as possible for the tumor covering the entire vertebral body, or 4) if destruction of the vertebra provided great opportunities for extravasation.
Compared with the traditional approach, STWZ yields several different theoretical advantages. STWZ could create a new approach for PV targeting the posterior part of the vertebral body. It is well known that the hypotenuse of the Kambin triangle is the exiting nerve root and that the base is the superior endplate of the caudal vertebra [18]. Our approach first used the STWZ as a puncture approach to target the posterior part of the vertebral body and successfully reached the target point.
In daily practice, if the disruption of a vertebral body provides a great opportunity to cement, we would perform bilateral transpedicular combined with the STWZ approach. The STWZ could act as an additional approach for injection when a channel leaks directly to the intradistal space, or spinal canal leakage is likely to occur without increasing the risk of injury to the nearby structure and cement leakage.
The average volume of the bone cement used in this study was 6.0 ± 1.4 mL and 5.7 ± 1.5 mL in groups A and B, respectively, which was close to the volumes reported [19]. Nonetheless, the cement leakage rate in group A was 98.1%, without any clinical complications. The rate of leakage increased with cement volume [20,21], was higher than that in other published studies [22,23], and had no difference when compared with that in group B.
The STWZ could also adjust the puncture angle in the posterior part of the vertebral body and the direction to enter the vertebra. Bone cement diffuses across the midline; both sides of the vertebra can increase stiffness significantly, and biomechanical balance of stress on both sides is achieved [24]. The extrapedicular approach of the transverse process increases the puncture angle [5,25]; however, the limitations of the skin entry point and injury to the ligament complex and segmental artery make the application of this approach relatively limited [6,7]. Furthermore, Wang et al. [26] reported that the Kambin triangle approach is safe and effective and has excellent cement distribution in osteoporotic vertebral compression fractures. Compared with the traditional approach (group B), cement filling was better in the STWZ approach (group A, p < 0.001) without increasing the risk of cement leakage. Thus, the STWZ approach might act as a supplement when it is difficult to apply or achieve satisfactory cement filling using transpedicular and extrapedicular approaches.
The STWZ approach can target the area of the posterior vertebral body when tumor recurrence occurs in that area. With the STWZ approach, a lower recurrence rate was achieved when compared with the traditional approach (p = 0.001). Biopsy and radiofrequency ablation can be performed via STWZ. Therefore, this approach could be associated with other diagnoses and treatments during the same procedure. During the puncture process, the patient’s perception of radiation pain was determined to ensure the safety of the puncture, which was used to minimize injury to the nerve root. Every patient in our cohort underwent local anesthesia to ensure timely feedback from the patient, which is also an important part of safely using the STWZ approach.
The limitation of this study is that a small number of patients were followed up. Even after contacting them via telephone, some patients were lost to follow-up. Another limitation of this study is that some patients had multiple comorbidities, complex medical histories including concomitant treatments, or rapid progression, which may have negatively affected the evaluation of the analgesic effect of PV. Finally, we performed this study in a single center and did not divide the two groups in a randomized manner; we did not evaluate the STWZ approach alone compared with traditional approaches, which would cover the true benefits or complications of the STWZ approach. Further studies are warranted using the STWZ approach alone.
In conclusion, this study demonstrated the technical feasibility, safety, and efficacy of PV using the STWZ approach to target the posterior part of the vertebral body in the treatment of spinal metastases. The STWZ approach can be an alternative or auxiliary puncture method to perform PV, and is applicable to various vertebral levels.
Footnotes
Conflicts of Interest: The authors have no potential conflicts of interest to disclose.
- Conceptualization: Bi Cong Yan, Yan Feng Fan, Qing Hua Tian, Tao Wang, Chun Gen Wu.
- Data curation: Bi Cong Yan, Yan Feng Fan, Qing Hua Tian, Zhi Long Huang, Hong Mei Song, Ying Li.
- Formal analysis: Bi Cong Yan.
- Funding acquisition: Chun Gen Wu.
- Investigation: Bi Cong Yan, Yan Feng Fan.
- Methodology: Bi Cong Yan, Yan Feng Fan, Qing Hua Tian, Ying Li, Chun Gen Wu.
- Project administration: all authors.
- Resources: Bi Cong Yan, Yan Feng Fan, Tao Wang, Zhi Long Huang, Hong Mei Song.
- Software: Bi Cong Yan, Yan Feng Fan.
- Supervision: Chun Gen Wu.
- Validation: Chun Gen Wu.
- Visualization: Bi Cong Yan, Yan Feng Fan.
- Writing—original draft: Bi Cong Yan, Yan Feng Fan.
- Writing—review & editing: Ying LI, Chun Gen Wu.
Funding Statement: None
Availability of Data and Material
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.
References
- 1.Health Quality Ontario. Vertebral augmentation involving vertebroplasty or kyphoplasty for cancer-related vertebral compression fractures: a systematic review. Ont Health Technol Assess Ser. 2016;16:1–202. [PMC free article] [PubMed] [Google Scholar]
- 2.Tsoumakidou G, Too CW, Koch G, Caudrelier J, Cazzato RL, Garnon J, et al. CIRSE guidelines on percutaneous vertebral augmentation. Cardiovasc Intervent Radiol. 2017;40:331–342. doi: 10.1007/s00270-017-1574-8. [DOI] [PubMed] [Google Scholar]
- 3.Kallmes DF, Schweickert PA, Marx WF, Jensen ME. Vertebroplasty in the mid- and upper thoracic spine. AJNR Am J Neuroradiol. 2002;23:1117–1120. [PMC free article] [PubMed] [Google Scholar]
- 4.Robinson Y, Heyde CE, Försth P, Olerud C. Kyphoplasty in osteoporotic vertebral compression fractures--guidelines and technical considerations. J Orthop Surg Res. 2011;6:43. doi: 10.1186/1749-799X-6-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ringer AJ, Bhamidipaty SV. Percutaneous access to the vertebral bodies: a video and fluoroscopic overview of access techniques for trans-, extra-, and infrapedicular approaches. World Neurosurg. 2013;80:428–435. doi: 10.1016/j.wneu.2012.09.005. [DOI] [PubMed] [Google Scholar]
- 6.Heo DH, Cho YJ. Segmental artery injury following percutaneous vertebroplasty using extrapedicular approach. J Korean Neurosurg Soc. 2011;49:131–133. doi: 10.3340/jkns.2011.49.2.131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ryu KS, Huh HY, Jun SC, Park CK. Single-balloon kyphoplasty in osteoporotic vertebral compression fractures: far-lateral extrapedicular approach. J Korean Neurosurg Soc. 2009;45:122–126. doi: 10.3340/jkns.2009.45.2.122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Padovani B, Kasriel O, Brunner P, Peretti-Viton P. Pulmonary embolism caused by acrylic cement: a rare complication of percutaneous vertebroplasty. AJNR Am J Neuroradiol. 1999;20:375–377. [PMC free article] [PubMed] [Google Scholar]
- 9.Ratliff J, Nguyen T, Heiss J. Root and spinal cord compression from methylmethacrylate vertebroplasty. Spine (Phila Pa 1976) 2001;26:E300–E302. doi: 10.1097/00007632-200107010-00021. [DOI] [PubMed] [Google Scholar]
- 10.Deramond H, Depriester C, Galibert P, Le Gars D. Percutaneous vertebroplasty with polymethylmethacrylate. Technique, indications, and results. Radiol Clin North Am. 1998;36:533–546. doi: 10.1016/s0033-8389(05)70042-7. [DOI] [PubMed] [Google Scholar]
- 11.Tumialán LM, Madhavan K, Godzik J, Wang MY. The history of and controversy over Kambin’s triangle: a historical analysis of the lumbar transforaminal corridor for endoscopic and surgical approaches. World Neurosurg. 2019;123:402–408. doi: 10.1016/j.wneu.2018.10.221. [DOI] [PubMed] [Google Scholar]
- 12.Fanous AA, Tumialán LM, Wang MY. Kambin’s triangle: definition and new classification schema. J Neurosurg Spine. 2020;32:390–398. doi: 10.3171/2019.8.SPINE181475. [DOI] [PubMed] [Google Scholar]
- 13.Lee J, Jo D, Song S, Park D, Kim D, Oh J. Effect of needle tip position on contrast media dispersion pattern in transforaminal epidural injection using Kambin’s triangle approach. J Pain Res. 2020;13:2869–2878. doi: 10.2147/JPR.S270450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Trumm CG, Jakobs TF, Zech CJ, Helmberger TK, Reiser MF, Hoffmann RT. CT fluoroscopy-guided percutaneous vertebroplasty for the treatment of osteolytic breast cancer metastases: results in 62 sessions with 86 vertebrae treated. J Vasc Interv Radiol. 2008;19:1596–1606. doi: 10.1016/j.jvir.2008.08.014. [DOI] [PubMed] [Google Scholar]
- 15.Filippiadis DK, Binkert C, Pellerin O, Hoffmann RT, Krajina A, Pereira PL. Cirse quality assurance document and standards for classification of complications: the cirse classification system. Cardiovasc Intervent Radiol. 2017;40:1141–1146. doi: 10.1007/s00270-017-1703-4. [DOI] [PubMed] [Google Scholar]
- 16.Comstock BA, Sitlani CM, Jarvik JG, Heagerty PJ, Turner JA, Kallmes DF. Investigational vertebroplasty safety and efficacy trial (INVEST): patient-reported outcomes through 1 year. Radiology. 2013;269:224–231. doi: 10.1148/radiol.13120821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Saliou G, Kocheida el M, Lehmann P, Depriester C, Paradot G, Le Gars D, et al. Percutaneous vertebroplasty for pain management in malignant fractures of the spine with epidural involvement. Radiology. 2010;254:882–890. doi: 10.1148/radiol.09081698. [DOI] [PubMed] [Google Scholar]
- 18.Hoshide R, Feldman E, Taylor W. Cadaveric analysis of the Kambin’s Triangle. Cureus. 2016;8:e475. doi: 10.7759/cureus.475. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Belkoff SM, Mathis JM, Jasper LE, Deramond H. The biomechanics of vertebroplasty. The effect of cement volume on mechanical behavior. Spine (Phila Pa 1976) 2001;26:1537–1541. doi: 10.1097/00007632-200107150-00007. [DOI] [PubMed] [Google Scholar]
- 20.Sun HB, Jing XS, Liu YZ, Qi M, Wang XK, Hai Y. The optimal volume fraction in percutaneous vertebroplasty evaluated by pain relief, cement dispersion, and cement leakage: a prospective cohort study of 130 patients with painful osteoporotic vertebral compression fracture in the thoracolumbar vertebra. World Neurosurg. 2018;114:e677–e688. doi: 10.1016/j.wneu.2018.03.050. [DOI] [PubMed] [Google Scholar]
- 21.Li Q, Long X, Wang Y, Guan T, Fang X, Guo D, et al. Clinical observation of two bone cement distribution modes after percutaneous vertebroplasty for osteoporotic vertebral compression fractures. BMC Musculoskelet Disord. 2021;22:577. doi: 10.1186/s12891-021-04480-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Amoretti N, Diego P, Amélie P, Andreani O, Foti P, Schmid-Antomarchi H, et al. Percutaneous vertebroplasty in tumoral spinal fractures with posterior vertebral wall involvement: feasibility and safety. Eur J Radiol. 2018;104:38–42. doi: 10.1016/j.ejrad.2018.04.010. [DOI] [PubMed] [Google Scholar]
- 23.Barragán-Campos HM, Vallée JN, Lo D, Cormier E, Jean B, Rose M, et al. Percutaneous vertebroplasty for spinal metastases: complications. Radiology. 2006;238:354–362. doi: 10.1148/radiol.2381040841. [DOI] [PubMed] [Google Scholar]
- 24.Chen B, Li Y, Xie D, Yang X, Zheng Z. Comparison of unipedicular and bipedicular kyphoplasty on the stiffness and biomechanical balance of compression fractured vertebrae. Eur Spine J. 2011;20:1272–1280. doi: 10.1007/s00586-011-1744-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Zhuo Y, Liu L, Wang H, Li P, Zhou Q, Liu Y. A modified transverse process-pedicle approach applied to unilateral extrapedicular percutaneous vertebroplasty. Pain Res Manag. 2021;2021:6493712. doi: 10.1155/2021/6493712. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wang YF, Shen J, Li SY, Yu X, Zou TM. Kambin triangle approach in percutaneous vertebroplasty for the treatment of osteoporotic vertebral compression fractures. Medicine (Baltimore) 2019;98:e17857. doi: 10.1097/MD.0000000000017857. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated or analyzed during the study are available from the corresponding author on reasonable request.