

Abstract
Background:
Like diagnostic status, clinically-relevant thought remains overwhelmingly conceptualized in terms of discrete categories (e.g., worry; rumination; obsessions). However, definitions can vary widely. The area of perseverative thought (or clinically-relevant thought more broadly) would benefit substantially from a consensus-based, empirically-grounded taxonomy similar to the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017) or the “Big Five” for personality. This paper addresses three major barriers to establishing such a taxonomy: 1) a lack of research explicitly comparing categorical (subtype) versus dimensional models; 2) primary reliance on between-person measures rather than modeling at the level of the thought (within-person); 3) insufficient emphasis on replication and refinement.
Methods:
Participants included an unselected crowdsourced sample (790 observations from 286 participants) and an independent anxious-depressed replication sample (808 observations from 277 participants). Participants made dimensional ratings for three idiographic clinically-relevant thoughts on a range of features. Multilevel latent class analysis and multilevel exploratory factor analysis were applied to identify and extract natural patterns of covariation among features at the level of the thought, controlling for person-level tendencies.
Results:
A consistent five-dimension solution emerged across both samples and reliably outperformed the best-fitting categorical solution in terms of fit, replicability, and explanatory power. Identified dimensions were dyscontrol, self-focus, valence, interpersonal, and uncertainty.
Conclusions:
Findings support a five-factor latent structure of PT. Theoretical, empirical, and clinical implications and future directions are discussed.
Keywords: rumination, repetitive thought, worry, structure, transdiagnostic
General Scientific Summary:
Difficult-to-control thoughts are common across a wide range of psychological problems, including anxiety, depression, and related emotional mental health concerns. In clinical research and practice, these thoughts are often described in terms of mutually exclusive categories, such as “worry,” “obsessions,” or “rumination,” but these categories may not be the most accurate way to organize and define thoughts. In two independent samples, we show that thoughts do not naturally group into categories. Instead, we find five underlying dimensions (uncontrollability; valence; self-focus; interpersonal; and uncertainty) along which difficult-to-control thoughts differ.
The increased availability and application of latent variable modeling approaches within the clinical science literature has contributed to a growing shift away from a traditional “neo-Kraepelinian” model in which psychological disorders are conceptualized as discrete entities (e.g., Kotov et al., 2017; Wright et al., 2013), and toward multidimensional conceptualizations of psychopathology, such as the Hierarchical Taxonomy of Psychopathology (HiTOP; Kotov et al., 2017). The advances resulting from the quantitative empirical approach to psychopathology have generated considerable excitement and impact. Empirically-derived dimensional taxonomies offer a clear, actionable alternative to clinically- and empirically problematic categorical taxonomies (e.g., DSM-5; American Psychiatric Association [APA], 2013). This work is especially important given the major influence that a dominant taxonomy can exert over theory, research, and practice. Efforts to establish such taxonomies serve as a guiding framework for later research aimed at refining, extending, and validating instruments to assess the constructs represented therein (see e.g., the Big Five model of personality and its instrumentation, John et al., 2008; HiTOP, Kotov et al., 2017).
One taxonomy that stands to benefit considerably from an empirically-driven approach governs the classification of clinically-relevant thought, especially perseverative (i.e., recurrent, difficult-to-control) thought. Perseverative thought, also commonly referred to as repetitive thought, negative repetitive thought, or perseverative cognition, is a defining feature and well-documented mechanism of internalizing-related psychopathology (APA, 2013; Watkins, 2008). Early operationalizations of perseverative thought followed a disorder-specific framework, in which major thought classes or “types” were identified on the basis of salient features (e.g., those commonly observed in clinical contexts) and studied within the context of a specific disorder. For example, rumination is one prominent manifestation of perseverative thought that has been defined in several ways, most notably as persistent dwelling on the causes and consequences of one’s depressive symptoms (Nolen-Hoeksema et al., 2008). Similarly, worry, historically studied in the context of generalized anxiety disorder (GAD), has been defined as apprehensive and relatively uncontrollable thought about the future (Borkovec et al., 2004), while obsessions, typically studied within the context of obsessive-compulsive disorder (OCD), have been defined as intrusive and unwanted thoughts that are subjectively experienced as unacceptable (Turner et al., 1992). Within this framework, the existence of each of these “classes” or “types” of thought (e.g., worries; obsessions) was rarely challenged. Instead, thought classes were commonly defined a priori on the basis of one or two salient features (e.g., worry is by definition future-oriented), with the primary empirical challenge being one of identifying additional features that either frequently co-occurred with the features presumed central to the construct, or that reliably distinguished between a given thought class (e.g., worry) and other classes that were presumed related but distinct (e.g., obsessions). Table 1 summarizes the major thought classes covered in the present study, with an emphasis placed on the major thought features identified in leading theoretical and clinical definitions of each class.
Table 1.
Major Perseverative Thought “Types” with Example Theoretical Models and Definitions
| Model | Label | Definition | Valence | Content | Temporal | Form | Dyscontrol |
|---|---|---|---|---|---|---|---|
| Worry | |||||||
| DSM-5 (APA, 2013) | Worry | “apprehensive expectation” | Anxious | Forthcoming problems; Future events; Real-life concerns |
Future | N/A | N/A |
| Borkovec et al., (1983); Borkovec & Inz, (1990); Borkovec et al., (2004) | Worry | “a chain of thoughts and images, negatively affect-laden and relatively uncontrollable… an attempt to engage in mental problem-solving on an issue whose outcome is uncertain but contains the possibility of. negative outcomes” | Anxious | Uncertain outcomes | Future | Verbal-linguistic; Images identified in 1983 model but excluded thereafter |
Difficultly disengaging; Repetitive |
| Rumination | |||||||
| Martin & Tesser, (1996) | Rumination | “conscious thoughts that revolve around a common instrumental theme and recur in the absence of… environmental demands” | N/A | Unattained goals | Past; Present |
Verbal; Emotions; Images; Sensations |
Involuntary; Difficulty disengaging; Long-lasting |
| Nolen-Hoeksema (1991); Nolen-Hoeksema et al., (2008) | Rumination | “repetitively and passively focusing on the symptoms of distress… thinking perseveratively about one’s feelings and problems” | Negative; Sad |
Self-worth; Meaning; Loss; Feelings; Personal problems |
Past; Present |
N/A | Repetitive; Perseverative |
| Trapnell & Campbell, (1999); Treynor et al., (2003) | Brooding (rumination subtype) |
“passive comparison of problems with an unachieved standard” | Negative; Sad |
Personal problems; Unachieved goals |
N/A | N/A | Repetitive |
| Trapnell & Campbell, (1999); Treynor et al., (2003) | Reflection / Pondering (rumination subtype) | “purposeful self-analysis… cognitive problem solving to alleviate one’s depression symptoms” | Neutral | Self | Present | N/A | Voluntary |
| Feldman et al., (2008) | Positive rumination (rumination subtype) |
“…recurrent thoughts about positive self-qualities… affective experience, and one’s favorable life circumstances” | Happy; Proud |
Self; Affective experience; Favorable circumstances |
Present | Thoughts | Recurrent |
| Intrusive Memories | |||||||
| DSM-5 (APA, 2013) | Intrusive memories | “recurrent, involuntary, and intrusive memories of the traumatic event” | Distressing | Traumatic experience | Past | Memories | Recurrent; Involuntary; Intrusive |
| Ehlers et al., (2004) | Intrusive memories | “sensory impressions and emotional responses from the trauma that… lack a time perspective and a context” | Fearful | Traumatic experience | Past; Present |
Memories; Sensations |
Intrusive; Repetitive; Involuntary |
| Obsessions | |||||||
| DSM-5 (APA, 2013) | Obsessions | “recurrent and persistent thoughts, urges, or images that are…intrusive and unwanted, and… cause marked anxiety or distress” | Anxiety; Distress; Not pleasurable |
Varies | N/A | Thoughts; Urges; Images |
Intrusive; Unwanted; Involuntary |
| Turner et al., (1992) | Obsessions | “repetitive and intrusive thoughts, images, and impulses that are considered unacceptable” | Negative | Varies | N/A | Verbal; Images; Impulses |
Repetitive; Intrusive; Egodystonic |
| Post-Event Processing | |||||||
| Rachman et al., (2000) | Post-event processing | “a review of distressing or embarrassing events” | Anxious | Self-evaluation; Social |
Past | Memories | Recurrent; Intrusive |
As is evident upon close examination of Table 1, terminology, definitions, and proposed boundaries of these specific manifestations, classes, or types of perseverative thought vary considerably and remain longstanding matters of scientific debate (e.g., Harvey et al., 2004; Watkins 2008). We consider these debates in greater detail below (see Categorical Taxonomies of Perseverative Thought). However, a consensus has begun to emerge naming perseveration (i.e., inappropriate or involuntary repetition) as the central, shared characteristic that cuts across all of these manifestations, partially or fully accounting for the high comorbidity observed across supposedly distinct thought types and the strong relationship between perseverative thought and internalizing-related psychopathology (e.g., Ehring et al., 2011; Gustavson et al., 2018; Segerstrom et al., 2000; Spinhoven et al., 2011). Some transdiagnostic frameworks also identify negative valence as an additional defining feature of the shared transdiagnostic construct (e.g., Segerstrom et al., 2000); however, others explicitly exclude valence from their conceptualization, which allows for the inclusion of positive rumination (e.g., as occurs in the context of bipolar disorder and normative experiences such as limerence) under the broader perseverative thought umbrella (e.g., Ehring et al., 2011; Feldman et al., 2008; Watkins, 2008). Because positive rumination is implicated in emotion-related psychopathology (e.g., Feldman et al., 2008), and because it shares the primary defining feature of repetitiveness and subjective “stickiness” or uncontrollability that is identified across all major models of perseverative thought (e.g., Watkins, 2008), our operational definition of perseverative thought does not impose any requirements related to valence or content.
Therefore, in accordance with leading transdiagnostic frameworks (e.g., Brosschot et al., 2006; Ehring et al., 2011; Segerstrom et al., 2000), we operationalize perseverative thought as a transdiagnostic cognitive process that is defined by the subjective experience of repetitiveness or uncontrollability of mental activity. Within that operationalization, we allow that thoughts may be perseverative to a greater or lesser extent, but we exclude from our conceptualization even highly distressing or otherwise-salient thoughts that are not characterized by at least a minimal level of repetitiveness or “stickiness.” As in Ehring et al. (2011), we use the term perseverative thought because it highlights the defining feature of perseveration without imposing additional assumptions (e.g., valence; content). Because virtually all prominent models of perseverative thought emerge from a tradition of, and adhere closely to, anxious-distress and related affective phenomena (e.g., Harvey et al., 2004), we exclude from our conceptualization perseveration that may occur in the context of traumatic brain injury, psychotic disorders (e.g., delusions), developmental disorders (e.g., attention deficit-hyperactivity disorder). Instead, we limit our consideration of disorder-specific manifestations to major classes (types) listed in the diagnostic criteria for one or more “emotional” (i.e., anxiety, depressive, bipolar, obsessive-compulsive, and/or trauma- and stressor-related disorders), or considered a major feature or mechanism of those disorders (see Table 1). However, we suggest that an even broader framework that includes perseveration resulting from organic brain disease or injury and other atypical neurological presentations could be a potentially fruitful direction for future research.
Categorical Taxonomies of Perseverative Thought
Despite early theoretical and empirical support for a transdiagnostic framework (Ehring & Watkins, 2008; Harvey et al., 2004), and ongoing transdiagnostic work aimed at characterizing features that are shared across expressions of perseverative thought (e.g., Harvey et al., 2004; Ehring et al. 2011; Segerstrom et al., 2016; Szkodny & Newman, 2017), the prevailing clinical framework remains one of discrete “types” (classes) of thoughts (e.g., worry; obsessions; rumination; intrusive memories). The dominance of this categorical approach is evident by its utilization in DSM-5 (APA, 2013; see Table 1). A natural consequence of this approach is that perseverative thought “types” are often reified or treated as discrete and mutually exclusive, even when this is not the overt intention. For example, the DSM-5 requires that a given clinically-relevant thought be assigned to a single category (“this is a worry” or “this is an obsession”) in order to “count” toward the assignment of a clinical diagnosis. Additionally, although some frameworks allow a thought to be described as more or less severe within an assigned category, neither the DSM-5 nor any other frameworks to our knowledge allow a given clinically-relevant thought to be described as in-between categories (“somewhere between a worry and an obsession”) or to belong to multiple categories (“both a worry and an obsession”). Even within prominent transdiagnostic frameworks, only a few have considered the possibility of a multidimensional approach that allows predetermined categories to be transcended, while still retaining potentially important information about other clinically-relevant features of the thought (Segerstrom et al., 2016; Szkodny & Newman, 2017).
A further challenge of the prevailing categorical approach is that, even though virtually all frameworks define major classes of perseverative thought on the basis of various underlying features, such as valence, temporal orientation, level of construal, and controllability, there is little consensus about which of these features are considered definitional (i.e., necessary and sufficient) for a given thought type. Consequently, definitions and operationalizations within a given class can vary widely across research groups and clinical settings (see Table 1). As an illustrative example of the challenges of prevailing models, a leading definition of worry describes it as “a chain of thoughts and images, negatively affect-laden and relatively uncontrollable…” (Borkovec et al., 1983). Although later research suggested that verbal-linguistic processing was more commonly associated with these types of thoughts, and in fact might function to inhibit imagery (Borkovec & Inz, 1990), a revised consensus definition was never established. Can a thought that is predominantly imagery still be defined as a worry? What criteria are necessary and sufficient to “diagnose” a worry? The DSM-5 is arguably the consensus document to answer these questions, but it is even less specific than this leading empirical definition, defining worry only as “apprehensive expectation,” and referencing future- and problem-orientation in the section dedicated to differential diagnosis (APA, 2013).
Methodological and interpretative challenges also arise because certain features are embedded into the definitions of certain kinds of thought. For example, “worry” is future-focused by definition (Borkovec et al., 1983). Although researchers have typically been careful to remove references to features of interest when investigating other characteristics of these thoughts, participants themselves may apply their own culturally-informed schemas (e.g., about what it means for something to be a “worry”) when presented with these terms, complicating research into the nature and existence of such classes. Moreover, when features of interest are constrained in advance, either by researchers or participants (e.g., if examples of “worry” are pre-selected on the basis of high future-orientation and anxious arousal), finding related to those features are also necessarily constrained, in ways that may diverge from naturally-occurring patterns of covariation that might emerge in the absence of such constraints.
An even broader unanswered question is whether “worries” are a true class that exists in nature, being qualitatively distinct from other classes (e.g., “obsessions” or “brooding”), or whether these delineations represent artificial categories superimposed onto what are in reality one or more latent dimensions (e.g., repetitiveness, which may be empirically dissociable from future orientation and anxious valence). This question is more than theoretical; the ability to establish a direct relationship between specific features of a thought (e.g., intrusiveness) and the implications of those features for clinically-relevant outcomes (e.g., responsivity to exposure-based interventions) holds significant and as-yet untapped potential for advancing cognitive-behavioral intervention in this area. Meanwhile, inconsistencies, inaccuracies, and lack of clarity in the answers to these questions risk muddying the literature and impeding translation between research and clinical practice (e.g., Spitzer, 1976). Critically, some experimental research does point to potentially meaningful differences between theoretically-defined classes of perseverative thought. For example, a number of studies report differential effects of experimentally-induced worry versus rumination on a range of cognitive, affective, and biological outcomes (e.g., Cooney et al., 2010; Kim & Newman, 2019; Lewis et al., 2019; McLaughlin et al., 2007). However, without clear insight into the distinguishing features that drive these effects, it is difficult to translate these experimental findings into advances in theory or practice.
Dimensional Models of Perseverative Thought
Early support for a continuum of severity within a given perseverative thought class (worry, Ruscio et al., 2001; obsessions, Olatunji et al., 2008) came from the taxometric research literature. These studies reliably found that severity was distributed along a continuum, with no qualitative gap distinguishing “normal” versus “pathological” worry (Ruscio et al., 2001) or obsessions (Olatunji et al., 2008). However, these studies did not challenge the existence or nature of the types themselves. In other words, the studies confirmed that severity is distributed continuously, but they did not attempt to demarcate the boundaries that distinguish and define each thought type. Other studies have investigated the nature and boundaries between proposed types by asking participants to rate prototypical or idiographic examples of each type on the basis of various features (e.g., Watkins et al., 2005; Wells & Morrison, 1994) and comparing mean ratings. These studies yielded some consistent patterns, most reliably the finding that theoretically-defined worry and rumination differ primarily or exclusively in temporal orientation (Watkins et al., 2005; Kircanski et al., 2015). However, similar to the taxometric work in this area, these studies did not empirically challenge the existence of the classes themselves. Rather, these studies have mostly operated within the prevailing taxonomic framework, which in the empirical literature is a loosely organized array of “types” of thoughts with shared characteristics between them (e.g., Watkins, 2008).
Still other studies have explored hypothesized shared features and mechanisms of perseverative thought (sometimes called “transdiagnostic perseverative thought”) more directly by developing self-report measures that ask about the tendency to experience thoughts with those shared characteristics, rather than focusing on thoughts belonging to a specific subtype. For example, the Perseverative Thinking Questionnaire (PTQ; Ehring et al., 2011) was developed to assess the tendency to perseverate, minimizing references to peripheral features such as content and valence (e.g., “I get stuck on certain issues and can’t move on”; Ehring et al., 2011). Factor analyses favored a hierarchical structure with one higher-order factor and three lower-order factors. This structure included a “core PT” factor reflecting dyscontrol-related items which accounted for the preponderance of the variance in the scale’s relationship to existing measures, as well as factors for perceived unproductiveness and capture of mental capacity. Using a different approach, Segerstrom et al. (2016) derived a circumplex model of trait perseverative thought from existing self-report and daily diary measures of perseverative thought subtypes. The model identified valence (positive-negative) and purpose (searching-solving) as the major dimensions along which a given type of perseverative thought can be placed. Most recently, the Perseverative Cognitions Questionnaire (PCQ; Szkodny & Newman, 2017), was developed to test a six-dimensional model of trait perseverative thought. The proposed dimensions (dyscontrol; preparing for the future; dwelling on the past; expecting the worst; searching for causes/meaning; thinking discordant with ideal self) were supported in factor analyses across two large student samples.
Categorical approaches are also at odds with a growing empirical literature in healthy adults exploring underlying features of non-pathological spontaneous thought (e.g., Andrews-Hanna et al., 2013; Wang et al., 2018) and a clinical literature suggesting that shared variance between perseverative thought “types” accounts for the preponderance of variance in their relationship to anxiety, depression, and other forms of psychopathology (Arditte et al., 2016; Ehring & Watkins, 2008; Harvey et al., 2004; Topper et al., 2017). Several such studies conclude that trait measures of worry and rumination fit a bifactor model (e.g., Topper et al., 2014) or load with other perseverative thought subtypes to form a single factor (e.g., Arditte et al., 2016). However, although a few studies have used within-person momentary approaches to study mind-wandering in healthy adults (e.g., Andrews-Hanna et al., 2013), clinical research has overwhelmingly relied on individual difference (e.g., trait) measures, which assess a person’s usual levels of various subtypes of PT, rather than approaching classification at the level of the thoughts themselves. Consequently, it is not clear whether shared person-level variance reflects specific characteristics of the thoughts themselves, or nonspecific characteristics of the individual. This is an important limitation, because virtually all theoretical and clinical models allow that individuals experience many different “types” of thoughts, with many different severities, over the course of an hour, a day, or a lifetime.
Thus, despite considerable progress in the empirical literature, important gaps remain. One critical gap is that existing studies investigating the latent structure of perseverative thought have almost invariably done so at the level of the individual, rather than at the level of the thoughts themselves. Latent classes or dimensions that exist at the level of individual thoughts will be lost when averaged at the level of the person. For example, individuals who tend to experience higher rates of future-oriented thoughts (traditionally associated with worry) may also experience higher rates of sad thoughts (traditionally associated with rumination). However, that does not mean that a given thought that is more future-oriented will also tend to be sadder, once person-level tendencies are controlled. This consideration is especially important because endorsement rates for the various thought “types” are highly correlated (e.g., McEvoy et al., 2013).
One innovative early study (Segerstrom et al., 2003) approached classification at the level of the thought by inviting student participants to rate “something that has been on your mind lately” on a variety of unidimensional features (e.g., valence). Those descriptions were given to a second group of participants, who sorted them on the basis of similarity. The atheoretical, partially data-driven approach was a unique strength of this early study. However, there were also several limitations, including a non-nested statistical design (such that person-level characteristics were not controlled), an exclusively student sample, and the lack of an explicit comparison between a categorical versus dimensional latent structure. More recently, Kircanski et al. (2015) applied a combined theoretical and empirical approach to nested data in the context of an ecological momentary assessment study. In the study, women with generalized anxiety disorder and/or major depression responded to signals by first rating their level of worry and rumination, then rating those thoughts on a variety of theoretically-relevant features. The study had several noteworthy strengths, such as a multilevel design that focused on individual thoughts and unidimensional measurement of underlying features. However, it also shared some limitations with previous work, most centrally the decision to constrain analyses in line with theoretically-defined subtypes (i.e., worry and rumination were defined a priori; several dimensions were examined for only one subtype) and the lack of a direct comparison of a categorical versus dimensional latent structure.
Toward an Empirically-Derived Taxonomy of Perseverative Thought
Although previous studies of the nature and latent structure of perseverative thought offer strong preliminary support for a transdiagnostic approach to conceptualizing perseverative thought in terms of shared features, important questions and barriers to implementation remain. To address these questions, the present studies derive and compare a categorical (subtype; latent class) versus dimensional latent structure of perseverative thought using multilevel modeling, which allows classification at the level of the thought, versus the person. Other priorities included lifting a priori theoretical constraints, avoiding type-specific terminology in the recruitment and study materials, and assessing the replicability of the findings. This latter point was considered especially important for questions with proximal or immediate clinical implications, including questions that bear directly on classification and assessment, in light of the growing understanding and awareness of issues of replicability and transparency in clinical science (Tackett & Miller, 2019).
Leveraging methods adopted by the HiTOP framework (Kotov et al., 2017) and other data-driven classification efforts (e.g., Wright et al., 2013; Wright et al., 2015), we derived competing latent structures from feature ratings of idiographic (self-nominated) thoughts in two independent samples, including one unselected crowdsourced sample and a community sample of adults with elevated anxiety and/or depression. Participants self-nominated three thoughts that had “been on [their] mind a lot recently,” and rated each thought along a broad range of underlying features identified as potentially relevant to perseverative thought or any proposed subtypes. We selected these thought features based on a careful review of the theoretical, empirical, and clinical literatures, and, in keeping with the goal of developing a clinically-meaningful framework, our (L.S.H. and J.J.) own clinical training in differential diagnosis. Of particular interest were transdiagnostic models of perseverative thought (e.g., Segerstrom et al., 2000), major classes of thought included in the diagnostic criteria for one or more emotional disorders (e.g., worry; obsessions; intrusive memories), and classes widely considered a major feature or mechanism of those disorders (e.g., rumination; post-event processing). We identified for inclusion any thought feature that was included in the leading theoretical definition(s) for a given class; frequently studied with reference to a given class; considered theoretically or clinically important for a class; or used to distinguish between classes with at least some evidence of replicability. As an illustrative example, Langlois et al. (2000) asked participants to select a personally-relevant thought from a list of a priori-defined worries and obsessions and rate it on characteristics such as controllability (e.g., intrusiveness; difficulty disengaging), form (e.g., visual; verbal), and valence. We selected for inclusion any feature that reliably differentiated between classes in similar empirical studies (e.g., temporal orientation distinguishing between worry versus rumination; Kircanski et al., 2015; Watkins et al., 2005), that distinguished between outcomes within a class (e.g., worry in imagery versus verbal form; Leigh & Hirsch, 2011), or that was identified as a major defining characteristic of a class in at least one leading theoretical model (e.g., intrusiveness as a defining feature of obsessions; Turner et al., 1992).
Recognizing that there may be important characteristics not previously identified in the clinical literature, and because an overinclusive approach would still permit the emergence of a “true” latent structure, whereas an underinclusive approach might not, we also extracted other plausibly-relevant thought characteristics from the basic (non-clinical) cognitive neuroscience and mind wandering literatures (e.g., Andrews-Hanna et al., 2013), with a particular eye toward neurobiologically-dissociable facets of cognition. Thought features were selected with an eye toward unidimensionality and broad coverage for potentially-dissociable domains of process, form, and content. Although function is often represented in prominent theoretical models of perseverative thought, we conceptualize questions of causality (e.g., etiology; consequences) as empirically distinct from those of phenomenology and therefore did not attempt to assess those domains. We also limited our assessment of content to those domains represented in leading definitions of one or more forms of perseverative thought. We therefore excluded from our assessment content considered peripheral to the definition of a construct (e.g., we did not assess contamination content, because obsessions are typically defined on the basis of their intrusiveness, independent of content).
Finally, although the perseverative thought literature does not yet have an established and agreed-upon set of bordering constructs, we intentionally included two items that we would not expect to be endorsed in a well-specified framework, namely items related to mindfulness, which we conceptualize as in direct opposition to perseverative thought (e.g., Thompson et al., 2019). The complete list of features selected for inclusion is presented in Table 2. Feature ratings were subjected to a series of data-driven statistical approaches that were tailored to address some of the unique challenges and limitations of previous research in this area (see Data Analytic Plan).
Table 2.
Item Text and Descriptive Statistics for Individual and Composite Feature Ratings
| Study 1 | Study 2 | ||
|---|---|---|---|
| Descriptor | M (SD) | M (SD) | Text presented to participants |
| How ___ is the thought? | |||
| Repetitive | 2.27 (1.12) | 2.81 (1.07) | Repetitive (repeats over and over again) |
| Intrusive | 1.93 (1.37) | 2.59 (1.26) | Intrusive (comes into my mind when I don’t want it there) |
| Difficulty disengaging | 1.73 (1.36) | 2.53 (1.28) | Uncontrollable (hard to stop thinking about once I’ve started) |
| Abstractnesscomp | 0.99 (1.03) | 1.22 (1.05) | Abstract / Vague |
| Productive | 1.62 (1.32) | 1.31 (1.21) | Productive or helpful |
| Egosyntonica | – | 2.26 (1.3) | Consistent with how I see myself |
| What form did the thought take? | |||
| Visual | 2.35 (1.4) | 2.01 (1.48) | Images, like pictures, a TV show, or movie |
| Verbal | 2.21 (1.4) | 2.89 (1.25) | Words, like an internal monologue or audiobook |
| Memory | 0.99 (1.28) | 1.94 (1.56) | A memory that I am replaying |
| Impulsea | – | 1.62 (1.53) | An urge or impulse |
| The thought is about… | |||
| How I’m feeling | 2.17 (1.41) | 2.87 (1.25) | How I’m feeling |
| Personal task | 2.63 (1.5) | 2.77 (1.43) | Something I need to do |
| Personal problem | 1.88 (1.51) | 2.37 (1.5) | A personal problem |
| Analytical self-focus | 1.29 (1.37) | 2.15 (1.56) | Why I feel or act the way I do |
| Evaluative self-focuscomp | 1.45 (1.35) | 2.51 (1.37) | Self-critical thoughts / Evaluating myself or my performance |
| Socialcomp | 1.26 (1.35) | 1.93 (1.43) | A social interaction / My relationship with someone else |
| Something else | 0.90 (1.55) | 1.06 (1.64) | Something else |
| Past | 1.4 (1.43) | 2.03 (1.57) | Something that happened in the past |
| Present | 3.09 (1.2) | 3.32 (1.11) | Something that is happening now |
| Future | 3.43 (0.93) | 3.44 (1.07) | Something that could happen in the future |
| The thought made me feel… | |||
| Positivecomp | 2.02 (1.19) | 0.87 (1.13) | Happyb / Proudb |
| Angry | 1.96 (1.26) | 1.71 (1.48) | Angryb |
| Sad | 2.37 (1.42) | 2.38 (1.48) | Sadb |
| Guilty | 2.0 (1.26) | 1.81 (1.54) | Guiltyb |
| Anxiouscomp | 2.63 (1.23) | 2.64 (1.21) | Nervousb / Afraidb |
| Uncertain | 3.19 (1.37) | 2.81 (1.36) | Uncertain |
| Shamecompa | — | 1.57 (1.37) | Embarrassed / Ashamedb / Disgustedb |
Note. The full range (0 – 4) was represented for all items.
compComposite score.
Administered in Study 2 only.
Method
Feature Ratings
After providing consent and providing demographic information, participants nominated “three topics that have been on [their] mind a lot recently,” being “as specific as possible,” with no other instructions or suggestions as to how thoughts should be selected (adapted from Segerstrom et al., 2003). Participants rated each self-nominated thought according to the broad range of underlying features described above, including major facets of dyscontrol (intrusiveness; difficulty disengaging; repetitiveness) and other relevant features as described above (see Table 2). Theoretically-opposing features (e.g., future vs. past orientation) were rated separately.
Items were extracted directly from validated measures where possible (e.g., affect items were drawn primarily from the Positive and Negative Affect Schedule – Expanded Form; Watson & Clark, 1994; see Table 2). Where no validated measures existed, a well-documented challenge in this literature (Kircanski et al., 2015; see Discussion for further consideration of this issue), we (L.S.H. and J.J) drew on clinical expertise to describe the features in language that would typically be used in a clinical setting (e.g., egosyntonicity described as “consistent with how I see myself”). The lack of existing measures means there are no criteria against which to evaluate convergent and discriminant validity. However, the full range of scores were represented for all items.
In total, 23 items including 5 composites (see Data Analytic Plan) were submitted to analysis in Study 1. Seven additional items were added in Study 2 to provide more comprehensive coverage of domains theoretically linked to obsessions, intrusive recollections, and post-event processing. In the interest of prioritizing questions of replicability, the primary analyses for Study 2 included only those features that were assessed in Study 1. We then conducted follow-up analyses to examine the impact that any of these additional features had on the results (see Additional Items).
After completing the feature ratings, participants completed validated trait-level perseverative thought and symptom measures in a randomized order (see Trait and Symptom Measures).
Data Analytic Plan
Items were standardized and reduced prior to analysis to facilitate interpretation. Standardization occurred after removing those ineligible observations. To preserve unidimensionality, data reduction was limited to creating a composite score for highly correlated items (r ≥ |.60|) and was not implemented if theoretical models of perseverative thought made strong predictions about distinct contributions (i.e., intrusiveness versus difficulty disengaging). This latter decision was made to give leading theoretical models a “fair chance” to emerge from the data. We also excluded one poorly performing item (current sensations) and one composite item (specific/concrete) that was identified as theoretically and statistically redundant with another composite (vague/abstract; r = −.46 in Study 1). Observations (thoughts) were excluded from analyses if they failed a “minimum necessary” threshold to be plausibly considered an example of perseverative thought (i.e., for inclusion, thoughts were required to have a rating of greater than zero/“not at all” on at least one perseveration item [repetitive, intrusive, or difficult-to-control]).1 Of the five novel items, three were intercorrelated r = .59 – .83 and averaged prior to analysis.
For both studies, we estimated a dimensional model using maximum-likelihood multilevel (with robust standard errors) exploratory factor analysis with oblique (geomin) rotation at the within-person (i.e., thought) and between-persons level. We first identified the best-fitting solution for each level independently by estimating an unrestricted (i.e., fully saturated) structure at the other level (Ryu & West, 2009; Yuan & Bentler, 2007). We then ran a final model with the optimal number of factors specified at each level. Overall model fit statistics are reported using this latter model, which offers the most direct and conservative comparison to the multilevel latent class analysis fit statistics, while the structure is presented using estimates from the unrestricted analyses. Because the between-persons structure was not a focus of this study, these findings are presented in the Supplemental Materials. We estimated a categorical model using two-level mixture modeling with maximum-likelihood estimation and robust standard error estimates. Specifically, we estimated what has been termed a two-level random effects latent class analysis (Henry & Muthén, 2010; Vermunt, 2003).
We considered solutions between one and five factors (dimensions; at both the within- and between-persons levels) or classes (types) and compared the models on the basis of model fit (Akaike information criterion [AIC], Bayesian information criterion [BIC], where lower values reflect less discrepancy between model-predicted versus observed values, thereby indicating better fit), and replicability (visual examination and Tucker’s congruence coefficient; Tucker, 1951) within and across studies. For model comparisons, we used the information theory criteria (AIC, BIC) from the factor models with a structure simultaneously estimated at each level, because they provide a more conservative fit (i.e., they fit more poorly than the unrestricted models). Finally, linear multiple regression was used to examine the extent to which empirically-derived dimensions explained unique variance in established trait perseverative thought measures. Sample size was designed to exceed recent recommendations for stable covariance parameter estimation of N ≥ 250 (Schönbrodt & Perugini, 2013). Factor and latent class analyses were conducting using Mplus version 8 (Muthén & Muthén, 2017). Data preprocessing, correlation, and regression analyses were completed in R.
Study 1
Participants.
Participants (N = 286; 790 observations) were 52% women, 48% men, and 0.4% other gender; M age = 37.50, SD = 11.0; 84% White; 13% Black or African American; 5% Asian; 2% other; 10% Latino/a/x; 14% high school education or less; 43% Bachelor’s degree or higher (see Table 3). Participants were recruited via Amazon Mechanical Turk (mTurk) between March and April 2018, which precedes a possible quality decline beginning in Summer 2018 (Chmielewski & Kucker, 2019). Clinical data collected via mTurk at that time is generally of high quality and more representative of the general population compared to student samples and community samples from university communities (Chandler & Shapiro, 2016). To improve data quality and in keeping with best practices (Chandler et al., 2020), we restricted the sample to workers in the United States with at least a 99% previous task approval rating and excluded any participant who failed one or more of 17 attention checks (see Figure 1). Participants were paid $7 to complete the 55-minute study after endorsing an electronic waiver of consent. All procedures were IRB-approved for both studies.
Table 3.
Participant Characteristics
| Study 1 | Study 2 | |||||
|---|---|---|---|---|---|---|
| Measure | α | M(SD) | Range | α | M(SD) | Range |
| Perseverative Thought Measures | ||||||
| PTQ | 0.96 | 22.99 (12.76) | 0–51 | 0.93 | 35.33 (10.36) | 3–60 |
| PSWQ | 0.97 | 49.71 (18.05) | 16–80 | 0.93 | 61.8 (12.49) | 26–80 |
| RRS-10 Brooding | 0.85 | 9.87 (3.63) | 5–20 | 0.76 | 13.00 (3.48) | 6–20 |
| RRS-10 Reflection | 0.83 | 9.90 (3.36) | 5–20 | 0.72 | 11.79 (3.16) | 5–20 |
| RRQ Rumination | 0.96 | 38.06 (12.77) | 12–60 | 0.90 | 47.03 (8.15) | 19–60 |
| PCL-C Re-Experiencing | 0.91 | 8.74 (4.28) | 5–23 | 0.86 | 12.54 (4.94) | 5–25 |
| Y-BOCS-SR Obsession | 0.92 | 3.81 (4.43) | 0–18 | 0.92 | 7.20 (4.64) | 0–18 |
| Symptom Measures | ||||||
| DASS-21 | 0.96 | 25.54 (24.06) | 0–112 | 0.90 | 48.56 (21.80) | 8–106 |
| Depressiona,b | 0.94 | 8.22 (9.34) | 0–34 | 0.90 | 16.70 (10.70) | 0–42 |
| Anxietyc | 0.89 | 6.29 (8.00) | 0–38 | 0.82 | 13.04 (8.51) | 0–36 |
| Stressd | 0.91 | 11.03 (9.32) | 0 – 42 | 0.77 | 18.83 (7.76) | 0 – 38 |
| GAD-Q-IV | 0.85 | 4.70 (4.03) | 2 – 9.92 | 0.80 | 8.09 (3.61) | 0 – 13 |
| LSAS | --- | --- | --- | 0.97 | 58.52 (31.39) | 0 – 144 |
| PCL-C | 0.95 | 31.42 (14.59) | 17 – 77 | 0.91 | 44.52 (14.41) | 17 – 81 |
| Y-BOCS-SR | 0.91 | 7.15 (8.14) | 0 – 37 | 0.92 | 12.43 (8.78) | 0 – 35 |
Note. PTQ = Perseverative Thought Questionnaire; PSWQ = Penn State Worry Questionnaire; RRS-10 = Ruminative Responses Scale 10-item; RRQ = Rumination-Reflection Questionnaire; PCL-C = Post-Traumatic Stress Checklist-Civilian Version; Y-BOCS-SR = Yale Brown Obsessive-Compulsive Scale-Self Report; DASS-21 = Depression, Anxiety, and Stress Scale-21 item; GAD-Q-IV = Generalized Anxiety Disorder Questionnaire-IV; LSAS = Liebowitz Social Anxiety Scale.
DASS-21 depression subscale was administered without item 21 in Study 1. The error was corrected for Study 2.
≥ 10 inclusion threshold for Study 2;
≥ 2 inclusion threshold for Study 2;
≥ 7 inclusion threshold for Study 2 (all Antony et al., 1998).
Figure 1.
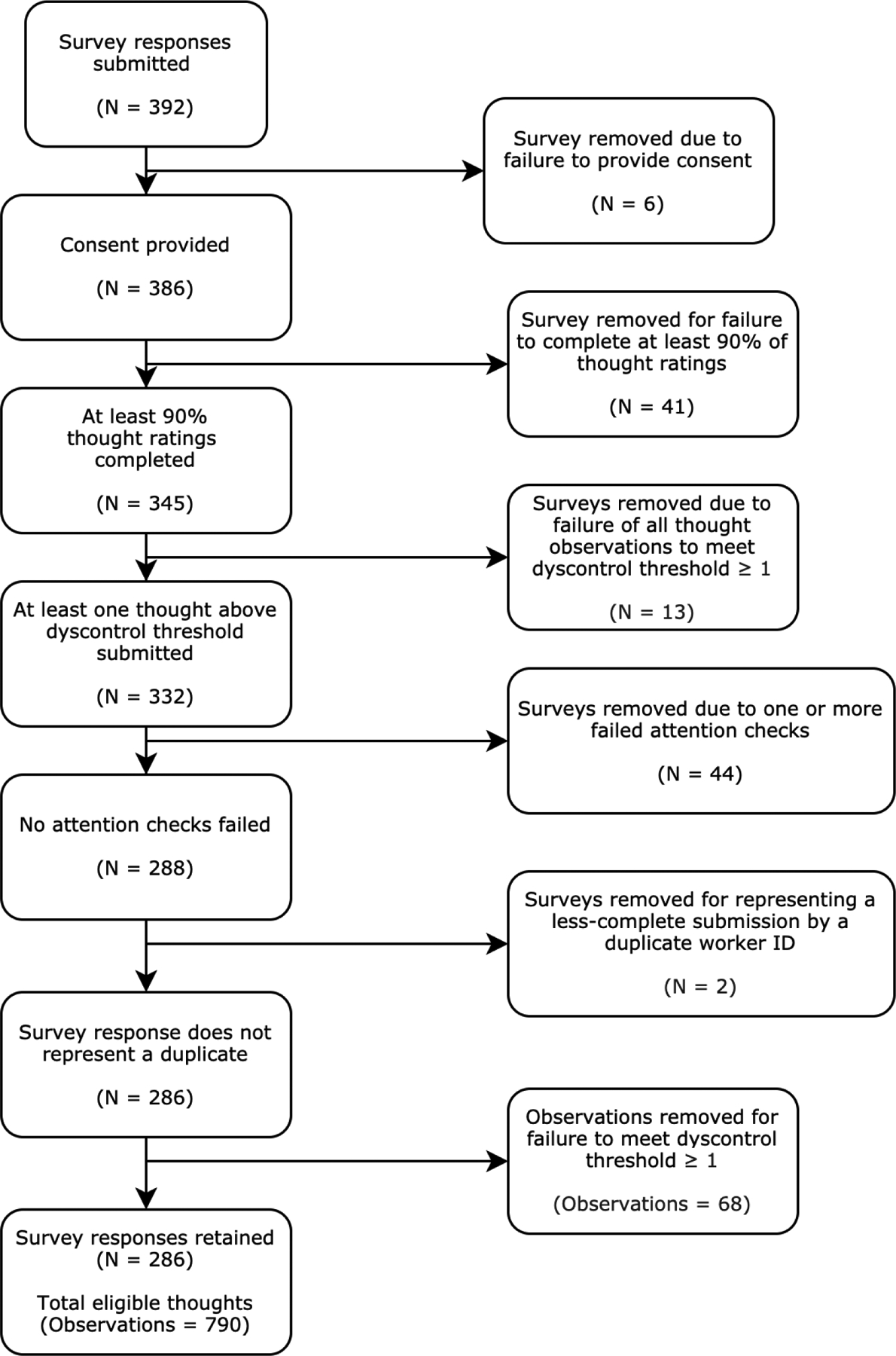
Diagram of Inclusion and Exclusion Criteria Applied for Study 1 Survey Responses
Trait and symptom measures.
The Perseverative Thought Questionnaire (PTQ; Ehring et al., 2011) is a 15-item measure of trait perseverative thought with strong psychometric features in non-clinical and clinical populations, including strong internal consistency and convergent validity vis-à-vis prominent measures of worry and rumination (Ehring et al., 2011). See Table 3 for descriptive statistics and internal consistency for all trait and symptom measures.
The Penn State Worry Questionnaire (PSWQ; Meyer et al., 1990) is a widely-used 16-item measure of trait worry with strong psychometric properties in unselected and clinical samples (Fresco et al., 2003).
The Ruminative Response Scale-10 item version (RRS-10; Treynor et al., 2003) includes two 5-item subscales: Brooding, defined as negative self-referential processing that is usually maladaptive, and Reflection, defined as analytical self-focus (e.g., seeking to understand one’s experiences) that is not necessarily maladaptive. The RRS-10 shows internal consistency and predictive validity similar to that of the original RRS (Treynor et al., 2003).
The Rumination subscale of the Rumination-Reflection Questionnaire (RRQ; Trapnell & Campbell, 1999) adopts a broader definition of rumination and includes 12 items related to self-criticism and mental rehearsal of past mistakes and failures. The subscale shows good test-retest reliability and convergent validity with related constructs (Trapnell & Campbell, 1999).
The Post-Traumatic Stress Checklist-Civilian Version (PCL-C; Weathers et al., 1993) is a 17-item self-report measure with strong psychometric properties for assessing trauma- and stressor-related symptoms in non-military samples. The PCL-C does not require the presence of a Criterion A trauma but instead refers to a “stressful experience from the past.” The 5-item Re-Experiencing subscale has good psychometric properties as a stand-alone measure of intrusive memories (Weathers et al., 1993).
The Obsession subscale of the Yale-Brown Obsessive-Compulsive Scale-Self Report version (Y-BOCS-SR; Baer et al., 1993) is a 5-item measure of obsession severity. The obsession subscale and Y-BOCS-SR more generally demonstrate good internal consistency, test-retest reliability and have been shown to discriminate between OCD and non-OCD patients (Steketee et al., 1996).
The Depression, Anxiety, and Stress Scale-21 item version (DASS-21; Henry & Crawford, 2005) is a well-validated short form of the DASS-42 for use in unselected and clinical samples as a measure of depression (Depression subscale), autonomic arousal and panic-like symptoms (Anxiety subscale), and chronic anxiety-related symptoms (Stress subscale).
The Generalized Anxiety Disorder Questionnaire-IV (GAD-Q-IV; Newman et al., 2002) is a validated self-report measure with 89% sensitivity and 83% specificity for a diagnosis of GAD. We used the recommended dimensional scoring which results in a cut-off of 5.7 for a GAD diagnosis.
Results.
Dimensional model.
Examination of the scree plot and fit statistics at the within-person level (specifying an unrestricted between-person structure) suggested that model fit improved substantially with the addition of each additional factor until a model with four within-person factors, which yielded acceptable fit (Confirmatory Fit Index [CFI] = 0.97; Standardized Root Mean Square Residual [SRMR] = 0.074; Root Mean Square Error of Approximation [RMSEA] < 0.01; AIC = 43,935; BIC = 44,551). Model fit further improved for all indices but the BIC with the addition of a fifth factor (CFI = 0.98; SRMR = 0.061; RMSEA < 0.01; AIC = 43,899; BIC = 44,605). Specifying a three-factor solution at the between-person level (see Supplemental Materials for additional discussion of the between-person structure) expectedly resulted in a relative decrement in fit relative to the unrestricted model, but the final model fit was still acceptable (CFI = 0.88; SRMR-within = 0.047; RMSEA = 0.047; AIC = 44,672; BIC = 45,794).
Results from the five-factor within-person solution (unrestricted between-person covariance) are presented in Figure 2 and Table 4. For both the four- and five-factor solutions, repetitiveness, intrusiveness, and difficulty disengaging loaded strongly on the first factor (dyscontrol). The second factor (self-focus) was characterized by relative elevations primarily in self-referential content, including evaluative and analytical self-focus, and task and personal problem and content. An interpersonal factor also emerged, with moderate loadings for past-focus, social/relationship content, and memory. The fourth factor consisted of a strong negative loading for positive affect, moderate positive loadings for sadness and anger, and modest negative loadings for productiveness and visual properties. Anxiety and uncertainty loaded with negative valence in the four-factor solution but formed a separate, fifth factor (uncertainty) in the five-factor solution. The five-factor solution also included a modest positive cross-loading for personal problem content that was not present in the four-factor solution.
Figure 2.
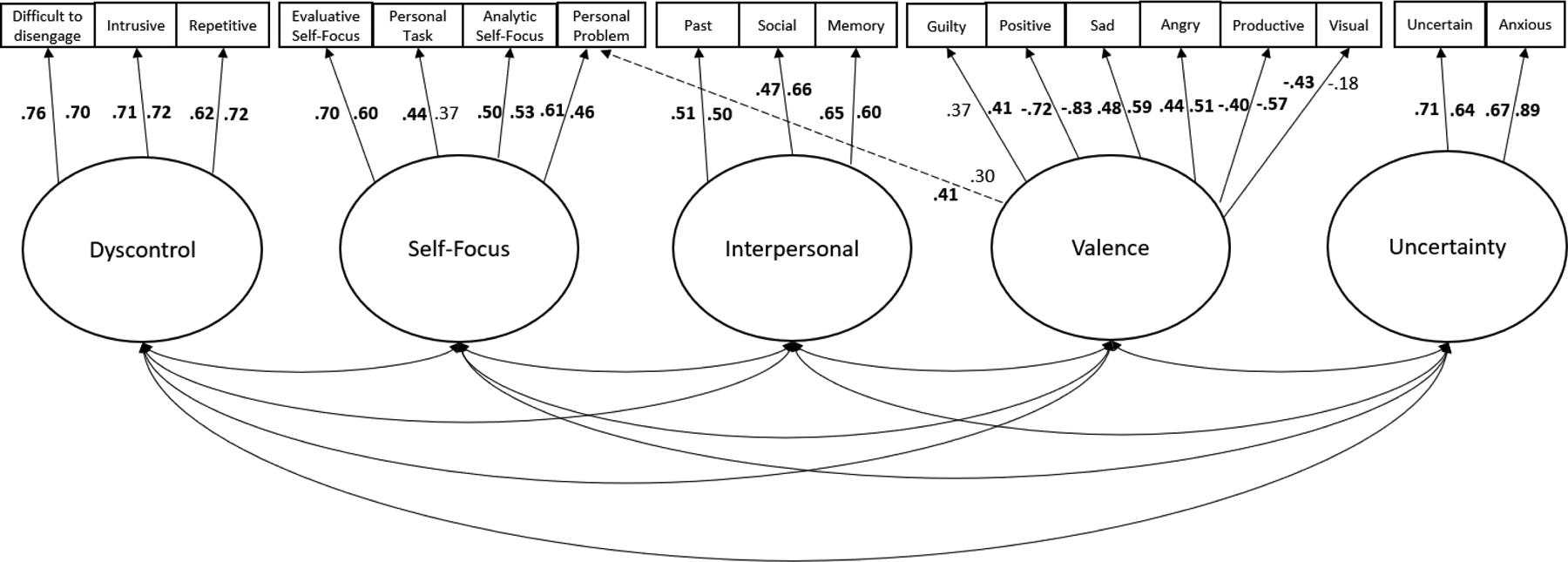
Multilevel Exploratory Factor Loadings for Study 1 and Study 2
Note. Five-factor latent structure. Factor loadings for Study 1 are placed to the left of each line. Factor loadings for Study 2 are placed to the right of each line. Significant factor loadings are in bold. Dotted lines reflect items that cross-loaded in one of the studies. For interpretability, factor covariances are presented separately in Table 4.
Table 4.
Five Factor Solution Factor Loadings for the Multilevel Exploratory Factor Analysis (MEFA)
| Item | Study 1 | Study 2 | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 1 | 2 | 3 | 4 | 5 | |
| Difficulty disengaging | 0.76 | 0.02 | 0.05 | −0.03 | 0.10 | 0.70 | 0.01 | 0.01 | 0.15 | 0.03 |
| Intrusiveness | 0.71 | 0.00 | 0.01 | 0.15 | 0.05 | 0.72 | 0.02 | 0.02 | 0.16 | 0.07 |
| Repetitive | 0.62 | 0.15 | −0.06 | 0.01 | −0.04 | 0.72 | 0.03 | −0.01 | −0.07 | −0.03 |
| Evaluative self-focusa | 0.09 | 0.70 | 0.15 | 0.01 | 0.04 | 0.24 | 0.60 | 0.02 | 0.02 | 0.00 |
| Personal problem | −0.01 | 0.61 | −0.05 | 0.41 | 0.00 | −0.10 | 0.46 | −0.01 | 0.30 | 0.01 |
| Analytical self-focus | −0.03 | 0.50 | 0.37 | −0.01 | 0.06 | 0.03 | 0.53 | 0.32 | 0.04 | −0.04 |
| Personal task | 0.08 | 0.44 | −0.39 | −0.05 | −0.07 | 0.04 | 0.37 | −0.38 | −0.23 | 0.07 |
| Past | 0.05 | 0.04 | 0.51 | 0.11 | −0.10 | 0.04 | 0.00 | 0.50 | 0.25 | −0.01 |
| Sociala | −0.15 | 0.01 | 0.47 | −0.17 | 0.02 | −0.09 | 0.13 | 0.66 | −0.07 | −0.01 |
| Memory | −0.01 | 0.06 | 0.65 | 0.01 | −0.14 | 0.10 | −0.02 | 0.60 | 0.10 | 0.03 |
| Positivea | 0.02 | 0.01 | 0.01 | −0.72 | −0.17 | −0.01 | −0.01 | 0.28 | −0.83 | 0.03 |
| Sad | 0.13 | −0.03 | 0.35 | 0.48 | 0.05 | 0.06 | 0.04 | 0.13 | 0.59 | 0.09 |
| Angry | 0.15 | −0.03 | 0.20 | 0.44 | −0.04 | −0.04 | 0.01 | 0.05 | 0.51 | 0.13 |
| Productive | −0.12 | 0.28 | −0.19 | −0.40 | −0.09 | −0.07 | 0.19 | −0.03 | −0.57 | −0.03 |
| Guilty | −0.01 | 0.38 | 0.07 | 0.37 | −0.02 | 0.08 | 0.25 | −0.03 | 0.41 | −0.02 |
| Visual | 0.14 | −0.14 | 0.33 | −0.43 | −0.04 | 0.05 | −0.17 | 0.30 | −0.18 | −0.03 |
| Uncertain | 0.03 | 0.01 | 0.02 | 0.10 | 0.71 | −0.04 | 0.03 | −0.02 | 0.07 | 0.64 |
| Anxiousa | 0.18 | −0.03 | −0.01 | 0.06 | 0.67 | 0.05 | −0.04 | −0.02 | −0.01 | 0.89 |
| Present | 0.07 | 0.16 | −0.09 | 0.27 | −0.08 | −0.02 | 0.14 | −0.01 | 0.02 | −0.02 |
| Future | 0.02 | 0.03 | −0.15 | −0.22 | 0.32 | 0.00 | 0.08 | −0.01 | −0.10 | 0.22 |
| How I’m feeling | 0.03 | 0.36 | 0.30 | −0.08 | 0.01 | 0.15 | 0.22 | 0.03 | 0.01 | −0.06 |
| Verbal | −0.01 | 0.10 | −0.02 | 0.19 | 0.10 | 0.10 | 0.29 | 0.28 | −0.05 | −0.02 |
| Abstractness | −0.08 | 0.06 | 0.08 | −0.22 | 0.27 | −0.24 | 0.16 | 0.13 | 0.03 | 0.10 |
| Factor Correlations | ||||||||||
| Factor 1 Dyscontrol | – | – | ||||||||
| Factor 2 Self-Focus | .15* | – | .34* | – | ||||||
| Factor 3 Interpersonal | .27* | −.03 | – | .20* | .19* | – | ||||
| Factor 4 Valence | .43* | −.07 | .14* | – | .41* | .27* | .25* | – | ||
| Factor 5 Uncertainty | .35* | −.06 | 0.13 | .48* | – | .29* | .05 | −.22* | .24* | – |
Note. Factor loadings ≥ .40 are in boldface.
Composite item.
p < .05.
Categorical model.
The multilevel latent class model consistently provided a worse fit to the data than a dimensional model, including when the categorical model was extrapolated out to an uninterpretably high number of classes (e.g., 9-class model AIC = 46,286; BIC = 47,436). The categorical results are not described further, but example solutions from each study are presented in the Supplemental Materials (Figures S1–S2) for illustrative purposes. All dimensional models were superior to the best-fitting categorical model (5-class model: AIC = 47,460; BIC = 48,142).
Correlation and regression analyses.
We next investigated the relationship of the empirically-derived dimensions to conventional trait perseverative thought measures. First, we summed the highest-loading items for each dimension and averaged them across thoughts within-person to approximate a “trait” rating for each dimension. We then conducted Pearson correlation and linear multiple regression analyses (Supplemental Tables S1and S2). Dyscontrol was strongly associated with transdiagnostic perseverative thought (r = .52) and intrusive memories (r = .52) and was only weakly related to reflection (r = .21). Uncertainty and Valence were each moderately associated with trait worry (r = .39 – .43, both p < .001). Associations between other dimensions and trait measures were small-to-moderate. Across analyses, average dimension scores explained 19 – 35% of the variance in trait PT. As expected, dyscontrol was the strongest and most consistent predictor across outcomes.
Discussion.
In direct comparisons, the dimensional model outperformed the categorical model in terms of model fit across all potentially viable class and factor solutions. This pattern of results suggests that a dimensional latent structure in which individual thoughts can be characterized along a series of underlying dimensions provides a better fit to the feature data, compared to a categorical structure in which thoughts are organized into “types.” Across analytic approaches, a 5-factor model provided the best fit to the data; we therefore focus our interpretation on these results.
Consistent with our conceptualization of dyscontrol as central to the perseverative thought construct, the three dyscontrol items loaded together on a single factor, which in turn significantly related to several perseveration-related outcomes in the regression analyses. The emergence of a self-focus dimension that included current concerns as well as analytical and evaluative self-focus was also noteworthy. This dimension correlated modestly with dyscontrol (r = .15) and was unrelated to valence (r = −.03). Although these features are broadly consistent with theoretically-defined rumination, the low correlation with the dyscontrol and valence dimensions challenges the suggestion that this factor could stand alone as a “rumination” dimension in its own right. Notably, personal problem content did modestly cross-load onto the negative valence factor, but this is likely driven by the “problem” aspect of the item, which is inherently negatively valenced, whereas the “personal” aspect is self-referential. Similarly, although the negative loading of visual properties on the valence factor was not expected, it is theoretically interpretable, as valence as a construct is not inherently visual. Finally, the emergence of a dimension characterized by strong positive loadings for anxious affect and uncertainty is also of interest. Notably, other features that have traditionally been linked to worry (future-orientation; abstract; verbal) did not load on this or any other factor.
Study 2
The aim of Study 2 was to replicate the findings from Study 1 in a community sample of adults with elevated anxiety and/or depression symptoms.
Participants.
Participants (N = 277; 808 observations) were 76% women, 21% men, 1% other gender; M age = 32.60, SD = 12.50; 90% White, 6% Black or African American, 6% Asian, 4% other; 5% Latino/a; 10% high school education or less; 60% Bachelor’s degree or higher (see Table 3 for clinical characteristics and Supplemental Table S3 for self-reported diagnostic status).
Participants were included if they scored within 1 SD (or higher) of the clinical M reported in Antony et al. (1998) for one or more corresponding DASS-21 subscales (e.g., within 1 SD of the MDD group M for the depression subscale). In the final sample, 83% of participants scored at or above well-established clinical cut-offs for one or more DSM-5 disorders characterized by perseverative thought, including generalized anxiety disorder (GADQ ≥ 7.67; 64%; Moore et al., 2014; Newman et al., 2002); major depressive disorder (DASS-depression ≥ 19; 39%; Weiss et al., 2015); obsessive-compulsive disorder (Y-BOCS-SR ≥ 16; 40%; Goodman et al., 1989); post-traumatic stress disorder (PCL-C ≥ 44; 52%; Ruggiero et al., 2003); and/or social anxiety disorder (LSAS ≥ 30; 78%; Mennin et al., 2002).
Most eligible participants (70%) were recruited via a National Institute of Health-funded Honest Broker participant registry housed within the recruiting university’s Clinical Translational Science Institute. The remainder of participants was recruited through social media, flyers, and listservs on the basis of self-identified anxiety and/or depressive disorder. As in Study 1, the study was described without reference to perseverative thought. Participants completed an electronic waiver of consent and received a $10 gift card as compensation.
Of note, there was a 12-hour period that was characterized by many identical and common-vocabulary open-text submissions, unusually fast completion times, and frequent attention check failures, all of which suggest the activity of bots rather than human participants. All responses from that time period were excluded, as were ten additional responses that showed a common agrammatical construction also suggestive of bots (using “your” in place of “my,” e.g., “Buy a car of your own”). See Figure 3 for detailed participant flow and reasons for exclusion.
Figure 3.
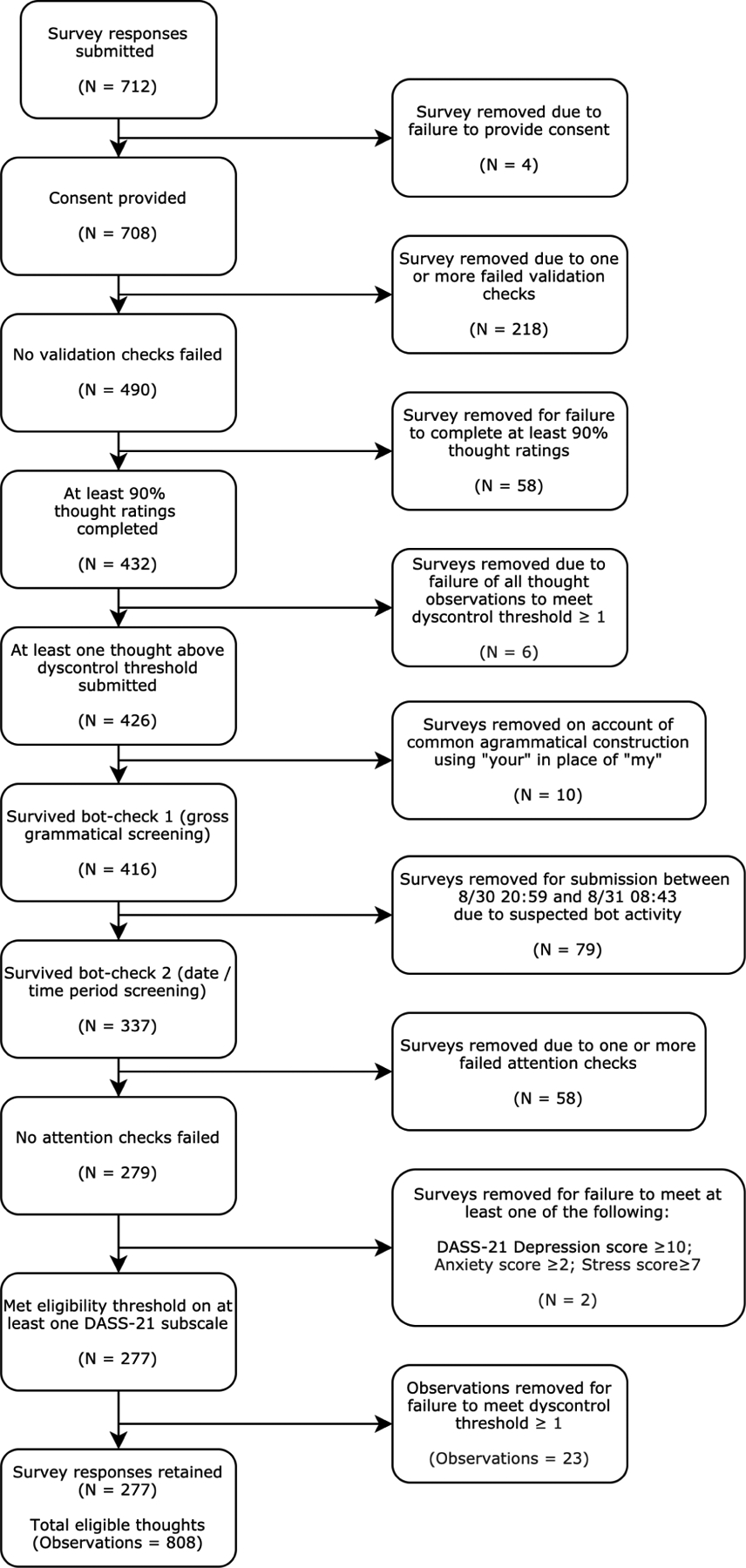
Diagram of Inclusion and Exclusion Criteria Applied for Study 2 Survey Responses
Trait and symptom measures.
Participants completed the following measures in addition to those described in Study 1.
The 9-item Post-Event Processing Questionnaire-Revised (PEPQ-R; McEvoy & Kingsep, 2006) is a short form of the PEPQ (Rachman et al., 2000) and assesses the tendency to experience repetitive, distressing, and interfering thoughts in response to anxiety-provoking social situations.
The Responses to Positive Affect Questionnaire (RPA; Feldman et al., 2008) was used to assess positive rumination (rumination in response to positive affect). The RPA has shown good convergent and discriminant validity with related measures (Feldman et al., 2008).
The Perseverative Cognitions Questionnaire (PCQ; Szkodny & Newman, 2017) assesses six theoretically-derived dimensions of perseverative thought and shows good convergent validity with other measures of repetitive thinking (Szkodny & Newman, 2017).
The Liebowitz Social Anxiety Scale (LSAS; Liebowitz, 1987) assesses past-week fear and avoidance of 24 common social situations. Internal consistency and convergent validity are strong in anxious samples (Fresco et al., 2001).
Results.
Dimensional model.
As in Study 1, a model estimated using an unrestricted between-person structures yielded acceptable fit for a four-factor (CFI = 0.92; SRMR = 0.04; RMSEA = 0.02; AIC = 46,546; BIC = 47,166) and five-factor (CFI = 0.95; SRMR = 0.03; RMSEA < 0.01; AIC = 46,382; BIC = 47,092; see Table 4) within-person solution. Model fit remained acceptable with the specification of a three-factor between-person structure (CFI = 0.92; SRMR-within = 0.04; AIC = 46,825; BIC = 47,952). The four-factor solution differed somewhat from the solution obtained in Study 1 (e.g., negative cross-loadings for anxiety and task content on the interpersonal factor; anxiety and uncertainty failed to load > .40 on the valence factor), and was less interpretable. By contrast, loading patterns for the five-factor solution were largely replicated, both visually and according to Tucker’s congruence coefficient (rc = .90 – .96 for Factors 1 – 4; rc = .89 for Factor 5; Lorenzo-Seva & ten Berge, 2006; see Figure 1).
Categorical model.
The dimensional model once again strongly outperformed the categorical model (5-class AIC = 48,871, BIC = 49,557), even when considering a model with an uninterpretably high number of classes (9-class model AIC = 47,683; BIC = 48,838). The categorical results therefore are not interpreted further.
Correlation and regression analyses.
As in Study 1, there was a moderate positive zero-order relationship between average dyscontrol and the trait measures included in Study 1, except RRS-Reflection (r = .09; see Supplemental Table S1). Of the remaining dimensions, self-focus and interpersonal content were again most strongly related to intrusive memories (r = .42 – .48, p < .001), while uncertainty was positively associated with transdiagnostic perseverative thought (r = .33) and trait worry (r = .28; all p < .001). Regression findings were also generally similar to Study 1 (see Supplemental Tables S2 and S4). As in Study 1, dyscontrol continued to emerge as the strongest and most reliable predictor.
Sensitivity analyses with additional items.
Model fit remained acceptable and was not substantially changed by the addition of the seven new items. Results are described further in the Supplemental Materials.
Discussion.
As in Study 1, a dimensional model provided a superior fit to the data compared to a latent class model. The factor solution for the dimensional model closely adhered to the solution obtained in Study 1 (all factors rc ≥ .89). Specifically, a five-factor model provided the strongest fit to the data and included dimensions for dyscontrol, self-focus, interpersonal content, valence, and uncertainty. A few differences emerged in the valence factor, but these were minor and improved interpretability; specifically, visual features and personal problem content no longer loaded > .40 (compared to loadings |.41 – .43| in Study 1) while guilt loaded .41 in Study 2 (versus .37 in Study 1). The modestly improved cohesiveness and interpretability of the valence factor in Study 2 may be related to the symptomatic nature of the sample. Similar to Study 1, mean scores across the five dimensions explained 19 – 35% of the variance in established trait measures of perseverative thought.
General Discussion
Despite a growing appreciation for the value of empirically-derived and dimensional taxonomies in clinical science, classification efforts for perseverative thought have been constrained by a longstanding diffuse and insufficiently-specified categorical (“type” or class-based) framework (e.g., APA, 2013). Although a large literature considers similarities and differences across types of perseverative thought, and despite advances from taxometric research (e.g., Ruscio et al., 2001; Olatunji et al., 2008), structural modeling studies (Arditte et al., 2016; Topper et al., 2014) and efforts to develop transdiagnostic measures (Ehring et al., 2011; Segerstrom et al., 2016; Szkodny & Newman, 2017), the existence of the types themselves at the latent level (i.e., discrete and mutually exclusive classes of clinically-relevant repetitive thought) has never been directly empirically challenged, nor tested against a viable alternative taxonomy. In the absence of empirical support, deference to a class-based taxonomy risks reification of artificial categories, while idiosyncratic adoption of incomplete and ad hoc transdiagnostic frameworks interferes with advances in theory and measurement. Collectively, the lack of a well-delineated framework from which to build a consensus-based, empirically-derived, and well-specified taxonomy of perseverative thought (akin to the Big Five model of personality; John et al., 2008) impedes collective advancement of the field and research-to-practice translation.
The present research therefore considered each of the following questions in turn: whether perseverative thought, broadly-defined, is most accurately described in terms of classes (types) or dimensions; how those classes or dimensions express themselves when released from theoretically-imposed constraints; and the extent to which those categories or dimensions align with established models and measures of perseverative thought. Across two studies, a dimensional model reliably outperformed a categorical model in terms of both statistical fit, interpretability, and replicability. Both studies yielded a five-factor within-person solution that provided a strong fit to the data, with dimensions related to cognitive dyscontrol, self-focus, interpersonal content, valence, and uncertainty.
The finding that dyscontrol reliably emerged across samples and as the strongest predictor of existing measures across a range of analytic approaches is consistent with a growing theoretical and empirical literature that identifies dyscontrol as the fundamental maladaptive feature of perseverative thought (e.g., Ehring et al., 2011). As in Ehring et al. (2011), dyscontrol items loaded separately from other potential core features such as unproductiveness, which in the present study loaded with valence (sadness; anger; low positive affect). The moderate relationship of this valence dimension to dyscontrol (r = .41 – .43) suggests that although the dimensions are separable, thoughts that were more unproductive, sad, and angry also tended to be experienced as more difficult to control. Notably, and in contrast to the major role these features play in distinguishing between obsessions and worry in clinical practice, intrusiveness and difficulty disengaging were highly correlated (r > .70), while repetitiveness showed a more moderate, but still robust, pattern of covariation. It would be premature to conclude from the present findings that there is no meaningful distinction between intrusiveness and impaired disengagement; however, the present findings do raise challenges for that distinction that will need to be directly addressed in intensive research with clinical samples.
A self-focus dimension consisting of analytical and evaluative self-focus (including self-criticism) and personal concerns also emerged across studies. This dimension corresponds to themes identified in several theoretical models of rumination (see Table 1) and suggests that self-referential processing may be most fruitfully viewed through a broad lens, rather than more narrowly as strictly related to self-analytical or self-evaluative processing. The absence of separate adaptive and maladaptive factors was also notable. Suggestively, Study 1 found a modest positive loading for guilt, but this loading was weaker in Study 2. We did not explore hierarchical structures in the present study, but it may be worthwhile for future research to explore whether clinically meaningful subdimensions for the current factors might emerge with additional indicators.
It is also notable that this self-focus dimension was only modestly related to dyscontrol (r = .15 – .34). This finding raises questions about the extent to which the dimension can be described as “rumination” or perseverative thought more broadly. One lens through which this finding might be interpreted is the “severity versus style” framework (e.g., Hopwood et al., 2011). In this case, dyscontrol may serve as a marker for the severity of PT, with elevations in other dimensions reflecting stylistic aspects that may have independent theoretical and clinical utility. That is, inability to control a thought reflects the core of this construct, with the other dimensions reflecting features that moderate the nature of the thought or its content. Finally, it will also be important for future research to consider the ways in which efforts to control thoughts might manifest and interact with subjective (perceived) and objective (behaviorally-indexed) cognitive dyscontrol within and across these dimensions.
The uncertainty dimension was somewhat less reliable than the first four dimensions and comprised only two indicators (one single indicator and one composite), so some caution is warranted in interpretation. Nevertheless, the dimension aligns in important respects with theoretical models of both worry and obsessions. Notably, we did not find support for a structural distinction between worry and obsessions (e.g., a dimension or class characterized by intrusiveness, negative valence, and egodystonicity, as in prototypical “obsessions,” versus a separate dimension or class characterized by future-orientation, verbal-linguistic form, and difficulty disengaging, as in prototypical “worry”). The use of an elevated symptom sample in Study 2, where more than a third of the sample endorsed clinically-significant obsessive-compulsive symptoms (Y-BOCS-SR ≥ 16) and more than half endorsed clinically-significant worry (PSWQ ≥ 65; Table 3) suggests that findings are not likely to be due to excessively mild or a restricted range of obsession severity (Y-BOCS-SR Obsessions M = 7.2, SD = 4.64, range = 0 – 18) or worry severity (PSWQ M = 61.8, SD = 12.49, range = 26 – 80). However, additional research with a true clinical sample will be essential.
It is also possible that the sample was sufficiently severe, but that conventionally obsessional thoughts were less likely to be nominated. Especially severe obsessional thoughts could be systematically underrepresented because participants may fear disclosure (e.g., because of social desirability concerns or magical thinking about potential consequences or implications of writing the thought). It is also possible that a different structure might emerge if only anxious thoughts were investigated or if hierarchical structures were considered. Adjusting study procedures to encourage reporting of traditionally-defined obsessions (e.g., by asking about “unwanted” thoughts) would be valuable for increasing confidence in the absence of an obsessional factor, and for guiding research into treatment prediction (i.e., mapping dimensional characteristics of presenting thoughts onto optimal interventions and outcomes).
These findings should also be considered in light of the studies’ other strengths and weaknesses. An important strength is the novelty of the present research, which is to our knowledge the first to apply contemporary data-driven multilevel modeling approaches to empirically derive and statistically compare categorical and dimensional structural models of perseverative thought. We are also among the first to approach classification at the level of the thought, which enabled us to control for person-level characteristics and covariation of proposed subtypes within individuals. However, the present study was limited in that participants only rated three thoughts, identified on the basis of being “on your mind a lot,” rather than in real-time and real-world contexts. This lower intensity of measurement was necessary and we believe well-justified in light of the early and exploratory nature of the present work; however, it will be important to examine the extent to which the findings replicate across contexts using ecological momentary assessment and other intensive measurement strategies. It will also be important for future research to describe and consider potential interactions between person-level and thought-level characteristics. Although these questions were largely beyond the scope of the present study, one goal for future research would also be to clarify how and under what circumstances general perseverative tendencies manifest as specific instances of PT.
Although we took several steps to ensure the robustness of our measurement approach, it is also important to acknowledge that, currently, there is no comprehensive measure or set of measures with known psychometric properties for assessing all potentially relevant characteristics of perseverative thought. Although in some respects this is a limitation of the present study, it is also an expected and arguably necessary condition of the problem that the present work aims to address. Much as the refinement of the Big Five and other personality models occurred in tandem with measure development and refinement (e.g., Digman, 1990), so too must refinement of a taxonomy of perseverative thought, and perhaps clinically-relevant cognition more broadly. Consequently, we view the present study as a critical foundation for an ongoing, iterative process of measure and model development and refinement, in which both lines of work independently and interactively move the field progressively closer to a comprehensive, detailed, and accurate representation of empirical truth.
The present findings should also be extended to treatment-seeking samples where perseverative thoughts are the presenting complaint or primary treatment target. There are many reasons to expect the present findings to generalize to clinical populations; for example, perseverative thought severity is distributed continuously in the population (Ruscio et al., 2001; Olatunji et al., 2008), and the vast majority (93%) of participants in Study 2 exceeded established clinical severity cut-offs for one or more anxiety, obsessive-compulsive, trauma- and stressor-related or depressive disorders. Nevertheless, there may be higher prevalence or salience of low-base-rate thoughts in treatment-seeking samples. The present findings suggest that this research would be a promising next step. An additional limitation is that the samples were largely White and cisgender. Recent empirical work suggests that the between-person latent structure of perseverative thought does not differ cross-culturally (e.g., Zainal, Newman, & Hong, in press); however, minority stress and related experiences may impact the expression of perseverative thought more broadly, and therefore warrant further consideration. The present study also only included content to the extent that it was needed to provide a fair test of leading theoretical models (e.g., leading operationalizations of depressive rumination and post-event processing specify self-evaluative content; Nolen-Hoeksema et al., 2008; Rachman et al., 2000). It might be interesting for future studies to examine the extent to which content that is commonly associated with, but not part of the definition of, a given “class” of perseverative thought (e.g., contamination-related thought content and obsessions) covaries with other characteristics attributed to that a priori class (e.g., intrusiveness).
Finally, the clinical implications of the present approach require rigorous examination in future research. Does a dimensional framework improve on a categorical approach for guiding treatment decisions? Does the severity of a thought’s dyscontrol or negative valence provide useful information for decision-making around cognitive restructuring, behavioral activation, or emotion regulation skills? Which dimensions, if any, predict differential responsivity to exposure-based versus mindfulness-based interventions? These are all empirical questions that will need exploration before the model is ready for large-scale adoption in clinical practice. Proof-of-concept experimental work, clinical trials (e.g., stratification to intervention based on dimension scores), and quantitative modeling (e.g., application of a “feature ablation” technique in machine learning models; Coutanche & Hallion, 2020) will each be valuable and necessary to advance this goal of a consensus-based, clinically useful, and empirically-robust model that offers the possibility of a non-incremental step forward in cognitive-behavioral treatment of perseverative thought.
Conclusions and Future Directions
The present study was novel in several respects. From a theoretical perspective, the data-driven conceptual framework and analytic approach allowed us to identify, critique, and test traditional assumptions about the latent structure of PT. From a methodological perspective, we also leveraged statistical approaches that are traditionally used to study individual differences (traits) to instead classify and make predictions at the level of individual thoughts, controlling for person-level characteristics. With the caveat that the present findings await conceptual replication across samples and methods, the present findings provide some of the strongest early evidence that perseverative thought is organized along underlying dimensions rather than subtypes. Specifically, we found consistent support for a five-factor dimensional model of perseverative thought that reliably outperformed a categorical (subtype) model. These findings should not be interpreted as authoritative, but instead should be considered an early step toward a larger aspirational goal of establishing a comprehensive, empirically grounded, and clinically useful taxonomy of perseverative thought that is informed by both data-driven and theoretical approaches. Several important questions remain to be addressed in future research. For example, does a dimensional approach offer incremental utility beyond the categorical approach, e.g., for predicting treatment response? In what ways do these dimensions overlap with – or serve as mechanisms of – other major dimensions of psychopathology? Which of these dimensions, if any, would be most fruitful to target in treatment, and for whom? This challenge is particularly salient in the broad area of emotional disorders, where the taxonomies that are used to classify thoughts have essential implications for theory, diagnosis, and treatment.
Supplementary Material
Acknowledgments
L.S.H.’s efforts on this project were supported by a grant from the National Institutes of Health (K01 MH116328). Portions of this research were presented at the Annual Meetings of the Association for Behavioral and Cognitive Therapies (November, 2018 and 2019) and the Anxiety and Depression Association of America (March, 2019). We thank Drs. Thomas Ehring, Joel Minden, and Suzanne Segerstrom for helpful comments on an earlier draft of this manuscript.
Footnotes
A preprint is available on PsyArXiv (https://psyarxiv.com/gu7xp/). All procedures were approved by the University of Pittsburgh Institutional Review Board #PRO18010220.
This criterion was implemented after data collection for Study 1 but prior to data collection for Study 2. Although this criterion was not specified in our initial protocol, the change was necessary and justified as it was theoretically-rather than statistically-motivated, finalized without knowledge of any impact on the results (i.e., prior to running the analyses), and in-effect prior to data collection for Study 2.
References
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). American Psychiatric Association. [Google Scholar]
- Andrews-Hanna JR, Kaiser RH, Turner AE, Reineberg AE, Godinez D, Dimidjan S, & Banich MT (2013). A penny for your thoughts: Dimensions of self-generated thought content and relationships with individual differences in emotional wellbeing. Frontiers in Psychology, 4, 1–13. 10.3389/fpsyg.2013.00900 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Antony MM, Bieling PJ, Cox BJ, Enns MW, & Swinson RP (1998). Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychological Assessment, 10(2), 176–181. 10.1037/1040-3590.10.2.176 [DOI] [Google Scholar]
- Arditte KA, Shaw AM, & Timpano KR (2016). Repetitive negative thinking: A transdiagnostic correlate of affective disorders. Journal of Social and Clinical Psychology, 35(3), 181–201. 10.1521/jscp.2016.35.3.181 [DOI] [Google Scholar]
- Baer L, Brown-Beasley MW, Sorce J, & Henriques AI (1993). Computer-assisted telephone administration of a structured interview for obsessive-compulsive disorder. American Journal of Psychiatry, 150(11), 1737–1738. 10.1176/ajp.150.11.1737 [DOI] [PubMed] [Google Scholar]
- Borkovec TD, Alcaine OM, & Behar E (2004). Avoidance theory of worry and generalized anxiety disorder. In Heimberg RG, Turk CL, & Mennin DS (Eds.), Generalized anxiety disorder: Advances in research and practice (pp. 77–108). The Guilford Press. [Google Scholar]
- Borkovec TD, & Inz J (1990). The nature of worry in generalized anxiety disorder: A predominance of thought activity. Behaviour Research and Therapy, 28(2), 153–158. 10.1016/0005-7967(90)90027-G [DOI] [PubMed] [Google Scholar]
- Borkovec TD, Robinson E, Pruzinsky T, & DePree JA (1983). Preliminary exploration of worry: Some characteristics and processes. Behaviour Research and Therapy, 21(1), 9–16. 10.1016/0005-7967(83)90121-3 [DOI] [PubMed] [Google Scholar]
- Brosschot JF, Gerin W, & Thayer JF (2006). The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research, 60(2), 113–124. [DOI] [PubMed] [Google Scholar]
- Chandler J, & Shapiro D (2016). Conducting clinical research using crowdsourced convenience samples. Annual Review of Clinical Psychology, 12, 53–81. 10.1146/annurev-clinpsy-0218515-093623 [DOI] [PubMed] [Google Scholar]
- Chandler J, Sisso I, & Shapiro D (2020). Participant carelessness and fraud: Consequences for clinical research and potential solutions. Journal of Abnormal Psychology, 129(1), 49–55. [DOI] [PubMed] [Google Scholar]
- Chmielewski M, & Kucker SC (2019). An MTurk Crisis? Shifts in Data Quality and the Impact on Study Results. Social Psychological and Personality Science, 1–10. 10.1177/1948550619875149 [DOI] [Google Scholar]
- Cooney RE, Joormann J, Eugène F, Dennis EL, & Gotlib IH (2010). Neural correlates of rumination in depression. Cognitive, Affective, and Behavioral Neuroscience, 10(4), 470–478. 10.3758/CABN.10.4.470 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Countanche MN, & Hallion LS (2020). Machine learning for clinical psychology and clinical neuroscience. In Wright AGC Hallquist MN(Eds.), The Cambridge Handbook of Research Methods in Clinical Psychology. Cambridge University Press. https://psyarxiv.com/7zswh/ [Google Scholar]
- Digman JM (1990). Personality structure: Emergence of the five-factor model. Annual Review of Psychology, 41(1), 417–440. [Google Scholar]
- Ehlers C, Hackmann A, & Michael T (2004). Intrusive re-experiencing in post-traumatic stress disorder: Phenomenology, theory, and therapy. Memory, 12(4), 403–415. 10.1080/09658210444000025 [DOI] [PubMed] [Google Scholar]
- Ehring T, & Watkins ER (2008). Repetitive negative thinking as a transdiagnostic process. International Journal of Cognitive Therapy, 1(3), 192–205. 10.1521/ijct.2008.1.3.192 [DOI] [Google Scholar]
- Ehring T, Zetsche U, Weidacker K, Wahl K, Schönfeld S, & Ehlers A (2011). The Perseverative Thinking Questionnaire (PTQ): Validation of a content-independent measure of repetitive negative thinking. Journal of Behavior Therapy and Experimental Psychiatry, 42, 225–232. 10.1016/j.jbtep.2010.12.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feldman GC, Joormann J, & Johnson SL (2008). Responses to positive affect: A self-report measure of rumination and dampening. Cognitive Therapy Research, 32, 507–525. 10.1007/s10608-006-9083-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fresco DM, Coles ME, Heimberg RG, Liebowitz MR, Hami S, Stein MB, & Goetz D (2001). The Liebowitz Social Anxiety Scale: A comparison of the psychometric properties of self-report and clinician-administered formats. Psychological Medicine, 31, 1025–1035. 10.1017/S0033291701004056 [DOI] [PubMed] [Google Scholar]
- Fresco DM, Mennin DS, Heimberg RG, & Turk CL (2003). Using the Penn State Worry Questionnaire to identify individuals with generalized anxiety disorder: A receiver operating characteristics analysis. Journal of Behavior Therapy and Experimental Psychiatry, 34, 283–291. 10.1016/j.jbtep.2003.09.001 [DOI] [PubMed] [Google Scholar]
- Goodman WK, Price LH Rasmussen SA, Mazure C, Fleischmann RL, Hill CL, Heninger GR, & Charney DS (1989). The Yale-Brown Obsessive Compulsive Scale 1: Development, use, and reliability. Archives of General Psychiatry, 46, 1006–1011. [DOI] [PubMed] [Google Scholar]
- Harvey AG, Watkins E, Mansell W, & Shafran R (2004). Cognitive behavioral processes across psychological disorders: A transdiagnostic approach to research and treatment. Oxford University Press Inc. [Google Scholar]
- Henry JD, & Crawford JR (2005). The short-form version of the Depression Anxiety Stress Scales (DASS-21): Construct validity and normative data in a large non-clinical sample. British Journal of Clinical Psychology, 44, 227–239. 10.1348/014466505X29657 [DOI] [PubMed] [Google Scholar]
- Henry KL, & Muthén B (2010). Multilevel latent class analysis: An application of adolescent smoking typologies with individual and contextual predictors. Structural Equation Modeling, 17(2), 193–215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hopwood CJ, Malone JC, Ansell EB, Sanislow CA, Grilo CM, McGlashan TH, Pinto A, Markowitz JC, Shea MT, Skodol AE, Gunderson JG, Zanarini MC, & Morey LC (2011). Personality assessment in DSM-5: Empirical support for rating severity, style, and traits. Journal of Personality Disorders, 25(3), 305–320. 10.1521/pedi.2011.25.3.305 [DOI] [PubMed] [Google Scholar]
- IBM Corp. (2017). IBM SPSS Statistic for Windows (Version 25.0) [Computer software] IBM Corp. https://www.ibm.com/analytics/spss-statistics-software [Google Scholar]
- John OP, Naumann LP, & Soto CJ (2008). Paradigm shift to the integrative Big Five trait taxonomy: History, measurement, and conceptual issues. In John OP, Robins RW, & Pervin LA (Eds.), Handbook of personality: Theory and research (3rd ed., pp. 114–158). Guilford Press. [Google Scholar]
- Kim H, & Newman MG (2019). The paradox of relaxation training: Relation induced anxiety and mediation effects of negative contrast sensitivity in generalized anxiety disorder and major depressive disorder. Journal of Affective Disorders, 259, 271–278. 10.1016/j.jad.2019.08.045 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kircanski K, Thompson RJ, Sorenson JE, Sherdell L, & Gotlib IH (2015). Rumination and worry in daily life: Examining the naturalistic validity of theoretical constructs. Clinical Psychological Science, 3(6), 926–939. 10.1177/2167702614566603 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotov R, Krueger RF, Watson D, Achenbach TM, Althoff RR, Bagby RM, Brown TA, Carpenter WT, Caspi A, Clark LA, Eaton NR, Forbes MK, Forbush KT, Goldberg D, Hasin D, Hyman SE, Ivanova MY, Lynam DR, Markon K, … Zimmerman M (2017). The Hierarchical Taxonomy of Psychopathology (HiTOP): A dimensional alternative to traditional nosologies. Journal of Abnormal Psychology, 126(4), 454–477. 10.1037/abn0000258 [DOI] [PubMed] [Google Scholar]
- Langlois F, Freeston MH, & Ladouceur R (2000). Differences and similarities between obsessive intrusive thoughts and worry in a non-clinical population: Study 1. Behaviour Research and Therapy, 38, 157–173. 10.1016/S0005-7967(99)00027-3 [DOI] [PubMed] [Google Scholar]
- Leigh E, & Hirsch CR (2011). Worry in imagery and verbal form: Effect on residual working memory capacity. Behaviour Research and Therapy, 49(2), 99–105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lewis EJ, Blanco I, Raila H, & Joormann J (2019). Does repetitive negative thinking affect attention? Differential effects of worry and rumination on attention to emotional stimuli. Emotion, 19(8), 1450. [DOI] [PubMed] [Google Scholar]
- Liebowitz MR (1987). Social phobia. Modern Problems in Psychopharmacopsychiatry, 22, 141–173. 10.1159/000414022 [DOI] [PubMed] [Google Scholar]
- Lorenzo-Seva U, & ten Berge JMF (2006). Tucker’s congruence coefficient as a meaningful index of factor similarity. Methodology, 2(2), 57–64. 10.1027/1614-2241.2.2.57 [DOI] [Google Scholar]
- Martin LL, & Tesser A (1996). Some ruminative thoughts. In Wyer RS (Ed.), Advances in Social Cognition, Volume IX: Ruminative Thoughts (pp. 1–48). Lawrence Erlbaum. [Google Scholar]
- Mathworks. (2017). Matlab (Version R2017a) [Computer software]. The Mathworks, Inc. https://www.mathworks.com/products/matlab.html [Google Scholar]
- McEvoy PM, & Kingsep P (2006). The post-event processing questionnaire in a clinical sample with social phobia. Behaviour Research and Therapy, 44, 1689–1697. 10.1016/j.brat.2005.12.005 [DOI] [PubMed] [Google Scholar]
- McEvoy PM, Watson H, Watkins ER, & Nathan P (2013). The relationship between worry, rumination, and comorbidity: Evidence for repetitive negative thinking as a transdiagnostic construct. Journal of Affective Disorders, 151(1), 313–320. 10.1016/j.jad.2013.06.014 [DOI] [PubMed] [Google Scholar]
- McLaughlin KA, Borkovec TD, & Sibrava NJ (2007). The effects of worry and rumination on affect states and cognitive activity. Behavior Therapy, 38, 23–38. 10.1016/j.beth.2006.03.003 [DOI] [PubMed] [Google Scholar]
- Mennin DS, Fresco DM, Heimberg RG, Schneier FR, Davies SO, & Liebowitz MR (2002). Screening for social anxiety disorder in the clinical setting: using the Liebowitz Social Anxiety Scale. Anxiety Disorder, 16, 661–673. 10.1016/S0887-6185(02)00134-2 [DOI] [PubMed] [Google Scholar]
- Meyer TJ, Miller ML, Metzger RL, & Borkovec TD (1990). Development and validation of the Penn State Worry Questionnaire. Behaviour Research and Therapy, 28(6), 487–495. 10.1016/0005-7967(90)90135-6 [DOI] [PubMed] [Google Scholar]
- Moore MT, Anderson NL, Barnes JM, Haigh EAP, Fresco DM (2014). Using the GAD-Q-IV to identify generalized anxiety disorder in psychiatric treatment seeking and primary care medical samples. Journal of Anxiety Disorders, 28, 25–30. 10.1016/j.janxdis.2013.10.009 [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2017). Mplus User’s Guide (8th ed). Muthén & Muthén. [Google Scholar]
- Newman MG, Zuellig AR, Kachin KE, Constantino MJ, Przeworski A, Erickson T, & Cashman-McGrath L(2002). Preliminary reliability and validity of the Generalized Anxiety Disorder Questionnaire-IV: A revised self-report diagnostic measure of generalized anxiety disorder. Behavior Therapy, 33, 215–233. 10.1016/S0005-7894(02)80026-0 [DOI] [Google Scholar]
- Nolen-Hoeksema S (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100(4), 569–582. 10.1037/0021-843X.100.4.569 [DOI] [PubMed] [Google Scholar]
- Nolen-Hoeksema S, Wisco BE, & Lyubomirsky S (2008). Rethinking rumination. Perspectives on Psychological Science, 3(5), 400–424. 10.1111/j.1745-6924.2008.00088.x [DOI] [PubMed] [Google Scholar]
- Olatunji BO, Williams BJ, Haslam N, Abramowitz JS, & Tolin DF (2008). The latent structure of obsessive-compulsive symptoms: A taxometric study. Depression and Anxiety, 25, 956–968. 10.1002/da.20387 [DOI] [PubMed] [Google Scholar]
- Rachman S, Grüter-Andrew J, & Shafran R (2000). Post-event processing in social anxiety. Behaviour Research and Therapy, 38, 611–617. 10.1016/S0005-7967(99)00089-3 [DOI] [PubMed] [Google Scholar]
- Ruggiero KJ, Del Ben K, Scotti JR, & Rabalaid AE (2003). Psychometric properties of the PTSD Checklist-Civilian Version. Journal of Traumatic Stress, 16(5), 495–502. 10.1023/A:1025714729117 [DOI] [PubMed] [Google Scholar]
- Ruscio A, Borkovec TD, & Ruscio J (2001). A taxometric investigation of the latent structure of worry. Journal of Abnormal Psychology, 110(3), 413–422. 10.1037/0021-843X.110.3.413 [DOI] [PubMed] [Google Scholar]
- Ryu E, & West SG (2009). Level-specific evaluation of model fit in multilevel structural equation modeling. Structural Equation Modeling, 16(4), 583–601. [Google Scholar]
- Schönbrodt FD, & Perugini M (2013). At what sample size do correlations stabilize?. Journal of Research in Personality, 47(5), 609–612. [Google Scholar]
- Segerstrom SC, Hardy JK, Evans DR, Boggero IA, Alden LE & Stanton AL (2016). Briefly assessing repetitive thought dimensions: Valence, purpose, and total. Assessment, 23(5), 614–623. 10.1177/1073191115586458 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Segerstrom SC, Stanton AL, Alden LE, & Shortridge BE (2003). A multidimensional structure for repetitive thought: What’s on your mind, and how, and how much? Journal of Personality and Social Psychology, 85(5), 909–921. 10.1037/0022-3514.85.5.909 [DOI] [PubMed] [Google Scholar]
- Spinhoven P, Drost J, van Hemert B, & Penninx BW (2015). Common rather than unique aspects of repetitive negative thinking are related to depressive and anxiety disorders and symptoms. Journal of Anxiety Disorders, 33, 45–52. [DOI] [PubMed] [Google Scholar]
- Spitzer RL (1976). More on pseudoscience in science and the case for psychiatric diagnosis: A critique of DL Rosenhan’s “On Being Sane in Insane Places” and “The Contextual Nature of Psychiatric Diagnosis”. Archives of General Psychiatry, 33(4), 459–470. https://doi/10.1001/archpsyc.1976.01770040029007 [DOI] [PubMed] [Google Scholar]
- Steketee G, Frost R, & Bogart K (1996). The Yale-Brown Obsessive Compulsive Scale: Interview versus self-report. Behaviour Research and Therapy, 34(8), 675–684. 10.1016/0005-7967(96)00036-8 [DOI] [PubMed] [Google Scholar]
- Szkodny LE, & Newman MG (2017). Delineating characteristics of maladaptive repetitive thought: Development and preliminary validation of the Perseverative Cognitions Questionnaire. Assessment, 1–21. 10.1177/1073191117698753 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tackett JL, & Miller JD (2019). Introduction to the special section on increasing replicability, transparency, and openness in clinical psychology. Journal of Abnormal Psychology, 128(6), 487–492. 10.1037/abn0000455 [DOI] [PubMed] [Google Scholar]
- Thompson JS, Jamal-Orozco N, & Hallion LS (2019). Differential relationships of the five facets of mindfulness to worry, rumination, and transdiagnostic perseverative thought. 10.31234/osf.io/kxy67 [DOI]
- Topper M, Emmelkamp PMG, Watkins E, & Ehring T (2017). Prevention of anxiety disorders and depression by targeting excessive worry and rumination in adolescents and young adults: A randomized controlled trial. Behaviour Research and Therapy, 90, 123–136. 10.1016/j.brat.2016.12.015 [DOI] [PubMed] [Google Scholar]
- Topper M, Molenaar D, Emmelkamp P, & Ehring T (2014). Are rumination and worry two sides of the same coin? A structural equation modeling approach. Journal of Experimental Psychology, 5(3), 363–381. 10.5127/jep.038813 [DOI] [Google Scholar]
- Trapnell PD, & Campbell JD (1999). Private self-consciousness and the five-factor model of personality: Distinguishing rumination from reflection. Journal of Personality and Social Psychology, 76(2), 284–304. 10.1037/0022-3514.76.2.284 [DOI] [PubMed] [Google Scholar]
- Treynor W, Gonzalez R, & Nolen-Hoeksema S (2003). Rumination reconsidered: A psychometric analysis. Cognitive Therapy and Research, 27(3), 247–259. 10.1023/A:1023910315561 [DOI] [Google Scholar]
- Tucker LR (1951). A method for synthesis of factor analysis studies (Personnel Research Section Report No. 984). Department of the Army. [Google Scholar]
- Turner SM, Beidel DC, & Stanley MA (1992). Are obsessional thoughts and worry different cognitive phenomena? Clinical Psychology Review, 12, 257–270. 10.1016/0272-7358(92)90117-Q [DOI] [Google Scholar]
- Vermunt JK (2003). Multilevel latent class models. In Stolsenberg RM(Ed.) Sociological Methodology, vol. 33, (pp. 213–293). Boston, MA: Blackwell Publishing. [Google Scholar]
- Wang HT, Poerio G, Murphy C, Bzdok D, Jefferies E, & Smallwood J (2018). Dimensions of experience: Exploring the heterogeneity of the wandering mind. Psychological Science, 29(1), 56–71. 10.1177/0956797617728727 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watkins E, Moulds M, & Mackintosh B (2005). Comparisons between rumination and worry in a non-clinical population. Behaviour Research and Therapy, 43, 1577–1585. 10.1016/j.brat.2004.11.008 [DOI] [PubMed] [Google Scholar]
- Watkins ER (2008). Constructive and unconstructive repetitive thought. Psychological Bulletin, 134(2), 163–206. https://doi/10.1037/0033-2909.134.2.163 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Watson D, & Clark LA (1994). The PANAS-X: Manual for the positive and Negative affect schedule – Expanded form. Unpublished manuscript. The University of Iowa. [Google Scholar]
- Weathers FW, Litz BT, Herman DS, Huska JA, & Keane TM (1993, October). The PTSD Checklist (PCL): Reliability, validity, and diagnostic utility. Paper presented at the 9th Annual Meeting of the International Society for Traumatic Stress Studies, San Antonio, Texas. [Google Scholar]
- Weiss RB, Aderka IM, Lee J, Beard C, & Björgvinsson T (2015). A comparison of three brief depression measures in an acute psychiatric population: CES-D-10, QIDS-SR, and DASS-21-DEP. Journal of Psychopathological Behavior Assessment, 37, 217–230. 10.1007/s10862-014-9461-y [DOI] [Google Scholar]
- Wells A & Morrison AP (1994). Qualitative dimensions of normal worry and normal obsessions: A comparative study. Behaviour Research and Therapy, 32(8), 867–870. 10.1016/0005-7967(94)90167-8 [DOI] [PubMed] [Google Scholar]
- Wright AGC, Krueger RF, Hobbs MJ, Markon KE, Eaton NR, & Slade T (2013). The structure of psychopathology: Toward an expanded quantitative empirical model. Journal of Abnormal Psychology, 122(1), 281–294. 10.1037/a0030133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wright AGC, Beltz AM, Gates KM, Molenaar PCM, & Simms LJ (2015). Examining the dynamic structure of daily internalizing and externalizing behavior at multiple levels of analysis. Frontiers in Psychology, 6, 1914. 10.3389/fpsyg.2015.01914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yuan KH, & Bentler PM (2007). 3. Multilevel Covariance Structure Analysis by Fitting Multiple Single-Level Models. Sociological methodology, 37(1), 53–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zainal NH, Newman MG, & Hong RY (in press). Cross-cultural and gender invariance of transdiagnostic processes in the United States and Singapore. Assessment, 1–18. 10.1177/1073191119869832. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.