

Abstract
Objective
To assess the effects of eLongTermCare (eLTC), a telehealth program implemented by an integrated health system in 45 nursing homes across the Midwest, on the use of acute hospital services and total expenditures for Medicare residents.
Data Sources
Minimum Data Set, Medicare fee‐for‐service claims, and enrollment data from 2013 to 2018.
Study Design
We used a longitudinal difference‐in‐differences design to estimate the changes in outcomes for treatment beneficiaries before and after participating in the eLTC program, relative to changes for the matched comparison beneficiaries over the same period. We measured outcomes over a 24‐month follow‐up period, including total Medicare spending, emergency department (ED) visits, hospitalizations, and the likelihood of readmission.
Data Collection/Extraction Methods
Using administrative data, we identified treatment beneficiaries who stayed at participating nursing facilities during the program period and matched comparison beneficiaries with similar baseline characteristics from non‐participating facilities in the same geographic locations.
Principal Findings
For long‐term care residents, the eLTC program led to an estimated reduction of 73 ED visits per 1000 beneficiaries (p < 0.01, 8.6% effect) over the two‐year follow‐up period. The estimated effects for this group were concentrated among beneficiaries who entered the nursing home after program startup, with sizable reductions in hospitalizations, ED visits, and spending. For skilled care residents, the program was associated with an estimated reduction of 85 ED visits per 1000 beneficiaries (p = 0.03, 9.7% effect), but had no discernible effect on their hospitalizations or total Medicare spending.
Conclusions
Telehealth can be a valuable tool for nursing homes to enhance care coordination and provide timely access to care, leading to lower spending for nursing home residents. Future research needs to explore payment methods that encourage telehealth expansion in nursing homes.
Keywords: health care costs, Medicare, nursing homes, program evaluation, technology adoption/diffusion/use, telehealth, utilization of services
What is known on this topic
Telehealth technologies can help improve access to care while delivering comparable health outcomes. But most nursing homes in the United States have low use of telehealth.
Previous studies have focused on the use of telehealth in homes, hospitals, and physicians' offices. However, relatively few studies have examined the effects of telehealth services on medical costs in nursing home settings.
What this study adds
Using telehealth for transitional care planning and round‐the‐clock access to clinicians can reduce unnecessary use of emergency and inpatient services, which lowers spending for nursing home residents.
Investment in high‐quality, continuous support for frontline staff may contribute to the successful implementation of telehealth programs in nursing homes.
Payers and policy makers interested in expanding telehealth services in nursing homes should explore payment models that align the costs of telehealth programs with potential savings from reduced hospital use.
1. INTRODUCTION
Telehealth technologies have long held promise for transforming the health care industry by improving access to care and lowering costs. During the COVID‐19 pandemic, telehealth experienced explosive growth in all regions of the country because of its potential to lower disease exposure, preserve supplies of personal protective equipment, and reduce patient demand on health care facilities. 1 Given this experience, Medicare, Medicaid, and commercial payers are beginning to establish policies to sustain and advance the adoption and use of telehealth technologies in the post‐pandemic era.
The literature has demonstrated telehealth technologies' potential to improve patient satisfaction and reduce health disparities by increasing access to care and empowering patients' self‐management of their conditions. 2 Several studies suggested that integrating telehealth in care management for patients with chronic diseases can be effective in reducing hospitalizations and emergency department (ED) visits. 3 , 4 , 5 , 6 , 7 Other studies showed that, for elderly adults with multiple comorbidities, the use of ambulatory telehealth interventions (e.g., telemonitoring, video consults, and tele‐exercise programs) can help improve access to specialists while achieving comparable health outcomes. 8 , 9
The nursing home is an area where telehealth technologies may help provide timely services to residents who lack access to onsite physicians, thus reducing costly and inconvenient transfers to EDs and hospitals. 10 A few studies found preliminary evidence that implementing telehealth consultations in nursing homes led to reduced hospital admissions and ED visits among residents, but the generalizability of existing studies is low due to small sample sizes or incomplete study designs. 11 In practice, most nursing facilities in the United States do not provide remote consultations with specialists via telehealth. 12 This study expands to the literature by assessing the effect of telehealth services in nursing homes on medical costs and providing evidence on whether such services can generate savings to payers, such as Medicare.
In this study, we examine the effect of a telehealth program implemented in 45 nursing homes that partnered with Avera Health, a nonprofit integrated health system that operates a large network of providers across the Upper Midwest region. To help nursing home residents gain access to timely, resident‐centered care, Avera Health implemented the eLongTermCare (eLTC) program that provided transitional care coordination and instant, round‐the‐clock access to clinicians for all residents in participating facilities. Avera Health provided these eLTC services at a centrally staffed telehealth hub in Sioux Falls, South Dakota. The eLTC staff at the hub site included clinicians (such as nurses and physicians) and administrative staff. Avera Health operated the eLTC program from November 2014 through August 2018. The program was funded by the Centers for Medicare & Medicaid Service (CMS) as part of the second round of Health Care Innovation Awards.
The eLTC program included three components:
Telehealth consults for urgent and specialty care. The eLTC team provided 24/7 access to telehealth consults for all nursing home residents. Nursing home staff were encouraged to call the eLTC team at the hub site whenever a resident needed urgent medical care; the hub team member evaluated the resident via synchronous two‐way audio and video, if necessary, and instructed staff on the next steps for care. For nonurgent specialty care, the hub team offered to schedule a telehealth appointment with other Avera Health specialists.
Telehealth transitional care coordination. For newly admitted residents, the eLTC team at the telehealth hub reviewed their medical records and assessed their health status to identify those at high risk for ED and hospital transfers. For high‐risk residents, the eLTC team conducted a full geriatric evaluation and developed a tailored electronic care plan, which included a chronic disease management plan, a schedule for telephone and video consults, and a task list for nursing home staff to follow as appropriate. For low‐risk residents, the eLTC team reviewed medication lists and provided medication recommendations to the primary care provider and nursing home staff.
Staff training and empowerment. Upon launching the eLTC program, Avera Health provided formal training to nursing home staff in participating facilities to ensure that they know when and how to initiate telehealth consults. Avera Health subsequently provided monthly training to nursing home staff on how to identify early changes in residents' conditions to avoid unnecessary ED or hospital transfers. Avera Health held regular meetings with staff to review unplanned transfers to an ED or hospital that nursing homes made without first consulting the eLTC team.
We conducted an independent evaluation on the effect of Avera Health's eLTC program on service use and costs for Medicare fee‐for‐service (FFS) beneficiaries. 13 We also examined the differential effects of the intervention on long‐term care residents and skilled care residents. We hypothesized that by training nursing home staff to use telehealth consults and providing remote clinical consults (or referrals to specialists) to their residents, the eLTC program would reduce unnecessary transfers to EDs and hospitals among residents, both of which would reduce the total cost of care. Further, we hypothesized that the overall effects of the program would be more pronounced among long‐term care residents than among skilled care residents who had less exposure to program services due to their shorter length of stay.
2. METHODS
2.1. Study design
Avera Health implemented the eLTC program at participating nursing homes in Iowa, South Dakota, North Dakota, and Minnesota on a rolling basis. All residents in participating nursing homes were eligible to receive eLTC services. To capture potential positive spillover effects from staff training and eliminate selection bias at the beneficiary level, we included all residents in participating nursing homes in the treatment group, regardless of whether they received telehealth services during their stay. We defined residents' eLTC enrollment date based on whether they were residing in the facility when the program was launched or were admitted to the facility after the program began. For beneficiaries who were in the nursing home before the facility launched the program, the launch date serves as the beneficiary's enrollment date. For beneficiaries entering the nursing home on or after the program launch date, their enrollment date is the day they were admitted to the facility.
The study period covers a 12‐month period before a beneficiary enrolled in the intervention (baseline) and a 24‐month period after they enrolled (follow‐up), conditional on being alive and enrolled in Medicare FFS. To avoid bias due to the potentially endogenous effect of the intervention on nursing home length of stay (which also affects outcomes), we followed all beneficiaries for 24 months after enrollment, including those who were discharged from the nursing facility during the follow‐up period.
2.2. Data and study population
Using the Minimum Data Set and Medicare enrollment data from November 2014 through February 2018, we identified all Medicare FFS beneficiaries who were residing in a participating facility when the eLTC program was launched or who were admitted to a participating facility after the start of the program. To ensure we had complete data over a sufficient period to measure the outcomes, we limited the treatment group to the 9608 Medicare FFS beneficiaries who were enrolled in both Medicare Parts A and B and had Medicare as the primary payer on their eLTC program enrollment date, were enrolled in Medicare for at least 90 days during the 12 months immediately before their program enrollment date, and were alive for a period of at least 30 days after their enrollment date.
We drew a comparison group from beneficiaries who stayed in a nursing home located in the same four states as the program during the same calendar period (to minimize cross‐state variation in health care practice patterns and outcomes), but were not affiliated with Avera Health and thus ineligible to participate in the eLTC program. We used the same rules for assigning enrollment dates for potential comparison beneficiaries as for the treatment group, using November 1, 2014 as a pseudo program launch date (the earliest launch date among the 45 participating nursing homes). Using propensity score matching techniques, we selected 24,620 comparison beneficiaries whose demographic, health status, service use, and spending characteristics were similar to treatment group members at baseline (defined as the 12‐month period before enrollment). Our propensity score matching model also controlled for facility characteristics, including rural location, bed size, nonprofit status, and a five‐star rating from the CMS Nursing Home Compare. We required an exact match on the state in which the facility was located, rural facility status, and length of nursing home residency before the enrollment date (0 days, 1–180 days, and more than 180 days).
Because of differences in health care needs between long‐term care nursing home residents and those receiving short‐term, rehabilitative skilled nursing care only, we drew a comparison group and modeled program effects for each group separately. We defined skilled care beneficiaries as those who had a Medicare skilled nursing facility (SNF) claim spanning the date they were enrolled in the eLTC program. We classified beneficiaries without an SNF claim at enrollment as long‐term care residents.
2.3. Outcomes
Using Medicare Part A and Part B claims, we constructed four outcomes: total Medicare FFS expenditures per beneficiary per month (PBPM), number of hospitalizations, number of outpatient ED visits (including outpatient observation stays), and the likelihood of hospital readmission within 30 days of discharge from an initial hospitalization. We constructed the first three outcomes for each beneficiary over every 6‐month segment covering the study period. In other words, each beneficiary had two observations in the baseline period and up to four observations in the follow‐up period (observations were truncated accordingly if the beneficiary died or left Medicare FFS during the follow‐up period). We annualized all three outcomes and measured them per 1000 beneficiaries. To account for extreme outliers in expenditures and number of visits or stays, we trimmed the outcome values for both groups at the 98th percentile of the treatment group distribution; that is, all values above the 98th percentile were replaced with the value of the outcome variable at the 98th percentile.
The last outcome, hospital readmission within 30 days of discharge, is a binary variable defined at the discharge level. The variable takes the value 1 if a hospital discharge was associated with at least one subsequent readmission within 30 days and 0 if not. A beneficiary with multiple discharges during the study period would have each discharge included as a separate observation.
2.4. Statistical analysis
To study the effect of the eLTC program, we employed a longitudinal difference‐in‐differences design. Our regression model measures program effects as the change in outcomes among treatment beneficiaries after versus before enrollment relative to the change in outcomes over the same period among matched comparison group beneficiaries with similar baseline characteristics.
For each continuous outcome (total Medicare expenditures, hospitalizations, and outpatient ED visits), we estimated a regression model that included observations for all baseline and follow‐up time periods that were available for each beneficiary in the sample. Our regression model included beneficiary‐level fixed effects and a follow‐up time indicator that took the value of 1 during a specific follow‐up period (months 1–12 and months 13–24). The beneficiary‐level fixed effects help isolate the treatment effect by removing any bias from unmeasured confounders at the individual level. In other words, the baseline observation serves as each individual's own control. We identified the effect of the program by the interaction between the time indicator and a binary treatment indicator. Due to the fixed‐effect specification, the treatment indicator and baseline characteristics of beneficiaries and facilities were not included as stand‐alone variables because the coefficients would not be identified. To control for the differential outcome trends among beneficiaries with different baseline health statuses, we included an interaction between the time indicator and the beneficiary's hierarchical condition category (HCC) score measured at baseline. The HCC score reflects the predicted cost of a beneficiary's care based on their Medicare claims history and demographic information. Beneficiaries with higher HCC scores at baseline have higher expected expenditures in the follow‐up period.
We used a different regression model for the 30‐day readmission outcome. Because the outcome was defined at the discharge level and the event did not typically repeat on the same beneficiaries over time, we estimated a point‐in‐time cross‐sectional model instead of the difference‐in‐difference model. We used a binary treatment indicator, time indicators for follow‐up period, and their interactions to identify the effect of the program, controlling for beneficiaries' and nursing facilities' characteristics at baseline, and discharge‐level risk factors for readmission (See Appendix S1 for modeling details.).
We used ordinary least squares to estimate all models. To account for the correlation in outcomes among multiple observations for the same beneficiary in our longitudinal dataset, we adjusted the standard errors for clustering at the beneficiary level.
3. RESULTS
3.1. Baseline characteristics
The treatment group represented a population of high‐need, high‐cost beneficiaries, as typically seen in nursing homes. The average age of treatment group beneficiaries at enrollment was 80 years (Table 1). Nearly two‐thirds of them were female, and 30% were dually eligible for Medicare and Medicaid. Measured over the 12 months before enrollment, the average HCC risk score for treatment group beneficiaries was 2.3, indicating their health care expenditures in the next year were expected to be nearly two‐and‐a‐half times the national Medicare FFS average. Congestive heart failure and vascular disease were the most common chronic conditions among them. Treatment group beneficiaries were in relatively high resource use groups (RUGs) upon nursing home admission, with an average RUG‐IV case‐mix index of 42 (out of a maximum of 66). They also had high rates of service use and Medicare expenditures during the baseline year. For example, the rate of hospitalization was 1002 per 1000 beneficiaries for the treatment group, 3.5 times higher than the U.S. average of 274 per 1000 beneficiaries. 14 About two‐thirds of the treatment group beneficiaries resided in rural facilities with an average of 93 certified beds. The average star rating for the participating nursing homes was 3.1 out of 5.
TABLE 1.
Characteristics of treatment and matched comparison groups at baseline
| Full study population | Treatment group only, by type of stay | ||||
|---|---|---|---|---|---|
| Treatment | Comparison | Long‐term care residents | Skilled care residents | ||
| Measure | (N = 9608) | (N = 24,620) | Standardized difference | (N = 7194) | (N = 2414) |
| Patient characteristics | |||||
| Age at enrollment | 80 | 80 | 0.05 | 81 | 79 |
| Female, % | 65 | 65 | 0.01 | 66 | 62 |
| White, % | 94 | 93 | 0.05 | 95 | 93 |
| Medicare/Medicaid dual status a , % | 30 | 30 | −0.02 | 33 | 18 |
| Days between admission and enrollment: 0, % | 39 | 39 | 0 | 22 | 92 |
| Days between admission and enrollment: 1–180, % | 10 | 10 | 0 | 11 | 7 |
| Days between admission and enrollment: 181+, % | 51 | 51 | 0 | 68 | 2 |
| HCC score b | 2.3 | 2.4 | −0.05 | 2.2 | 2.7 |
| COPD, % | 26 | 27 | −0.02 | 25 | 27 |
| CHF, % | 34 | 35 | −0.02 | 33 | 37 |
| Morbid obesity, % | 8 | 8 | −0.02 | 7 | 9.2 |
| Vascular disease, % | 31 | 29 | 0.03 | 33 | 25 |
| Major depressive disorder, % | 11 | 11 | 0 | 12 | 9.1 |
| RUG‐IV case‐mix index at admission c | 42 | 42 | −0.01 | 40 | 49 |
| RUG‐IV group: rehabilitation, % | 78 | 79 | −0.01 | 73 | 95 |
| RUG‐IV group: reduced physical function, % | 10 | 10 | 0.02 | 13 | 2 |
| RUG‐IV group: clinically complex, % | 4 | 4 | −0.01 | 5 | 2 |
| Service use and expenditures | |||||
| Number of hospital admissions (per 1000) | 1002 | 1058 | −0.04 | 824 | 1533 |
| Number of outpatient ED visits (per 1000) | 919 | 892 | 0.02 | 871 | 1064 |
| Total Medicare expenditures ($ PBPM) | 2274 | 2423 | −0.05 | 2060 | 2912 |
| Facility characteristics | |||||
| Facility state: Iowa, % | 23 | 23 | 0 | 26 | 13 |
| Facility state: Minnesota, % | 10 | 10 | 0 | 9 | 14 |
| Facility state: Nebraska or South Dakota, % | 68 | 68 | 0 | 66 | 73 |
| Rural facility, % | 64 | 64 | 0 | 65 | 59 |
| Nonprofit facility, % | 37 | 43 | −0.13 | 38 | 34 |
| Number of federally certified beds | 93 | 94 | −0.03 | 93 | 94 |
| Nursing home compare 5‐star rating | 3.1 | 3.1 | −0.04 | 3.1 | 3.1 |
Note: All beneficiary characteristics were measured during or as of the end of the baseline year, which is defined as the 365 days before each beneficiary's enrollment date. The statistics are weighted means, with beneficiary weights proportional to the number of months during the 12‐month baseline period that the beneficiary was enrolled in both Medicare Parts A and B. In addition, statistics for comparison beneficiaries are weighted to reflect the size of its match set (i.e., the number of comparison beneficiary matched to a treatment beneficiary). Facility characteristics are summarized from the beneficiary‐level data. The reference group for nonprofit facilities are for‐profit facilities. Public facilities are excluded from the study. Standardized differences are calculated as the ratio of the difference in means and standard deviation of the variable estimated on the treatment group.
Abbreviations: CHF, congestive heart failure; CMS, Centers for Medicare & Medicaid Services; COPD, chronic obstructive pulmonary disorder; ED, emergency department; ESRD, end‐stage renal disease; HCC, hierarchical condition category; PBPM, per beneficiary per month; RUG, resource utilization group.
Includes residents with both a disability and ESRD.
The HCC score incorporates diagnosis history and demographics to estimate a score representing the expected costs of a Medicare beneficiary in the upcoming year. A score of one represents average expected expenditures. HCC scores were calculated by using the most recently available HCC algorithms.
Case‐mix index is an integer ranking of the RUG Codes based on the total Medicare rate, and reflects the relative resources predicted to provide care to a resident. A case‐mix index is designated to each RUG under the CMS RUG‐IV system. The higher the case‐mix index, the greater the resource requirements for the resident.
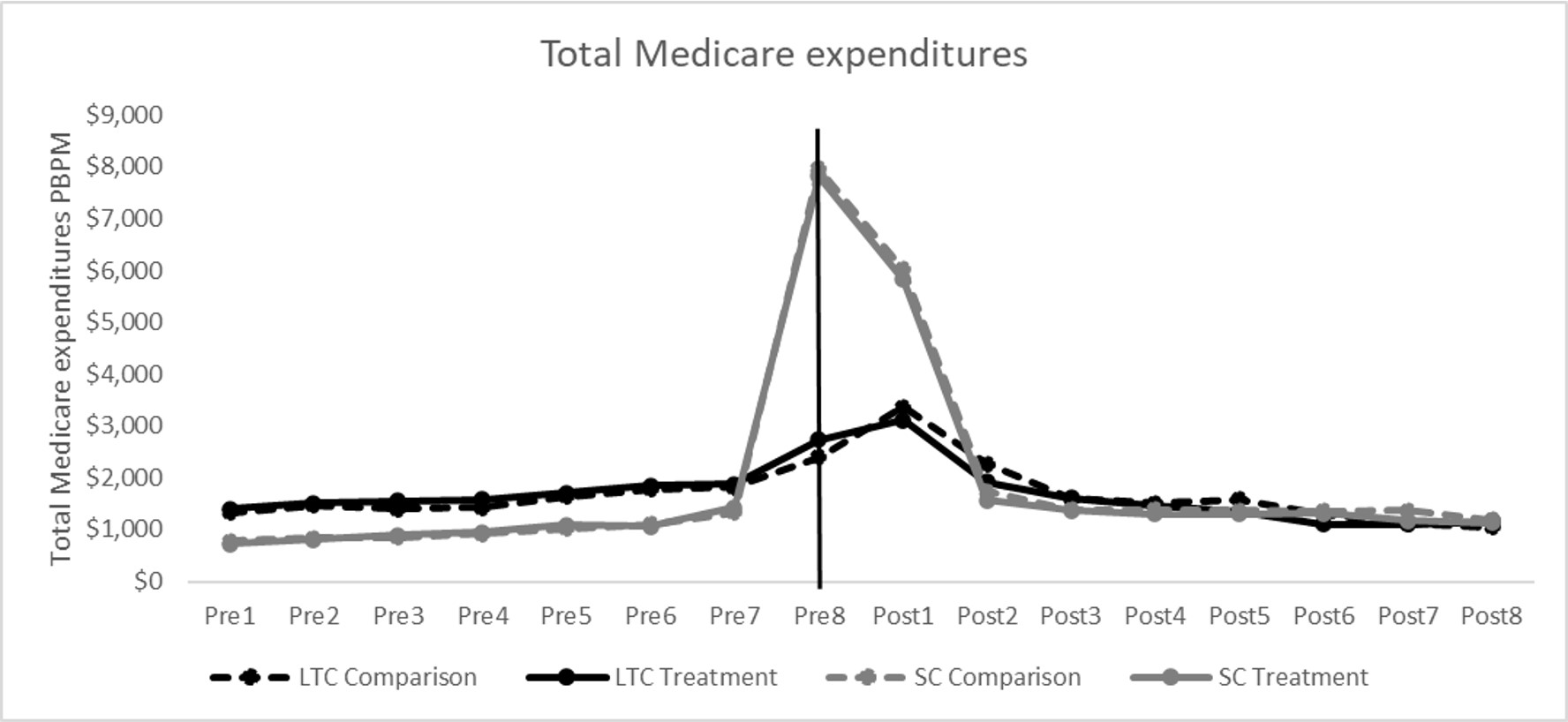
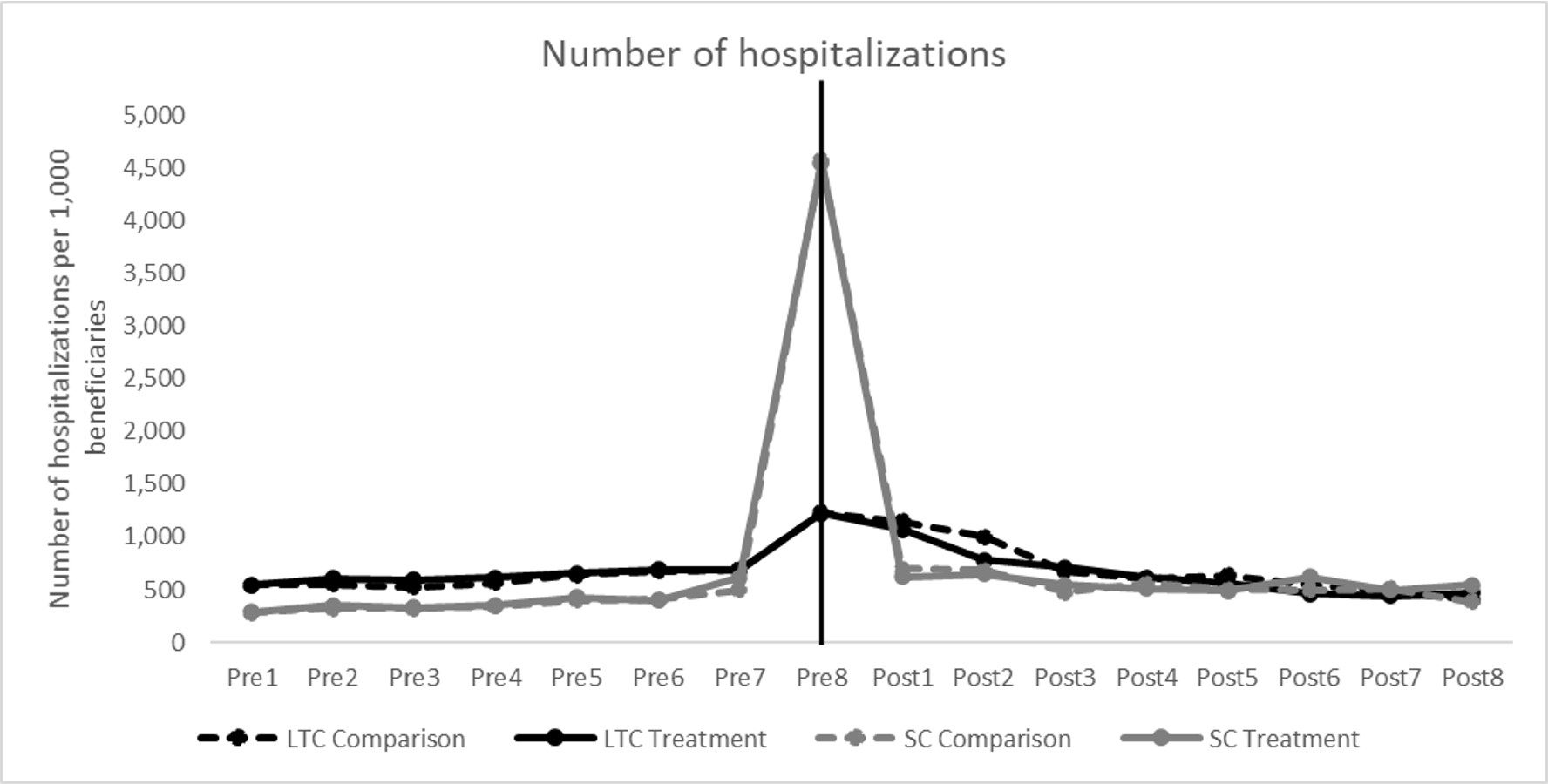
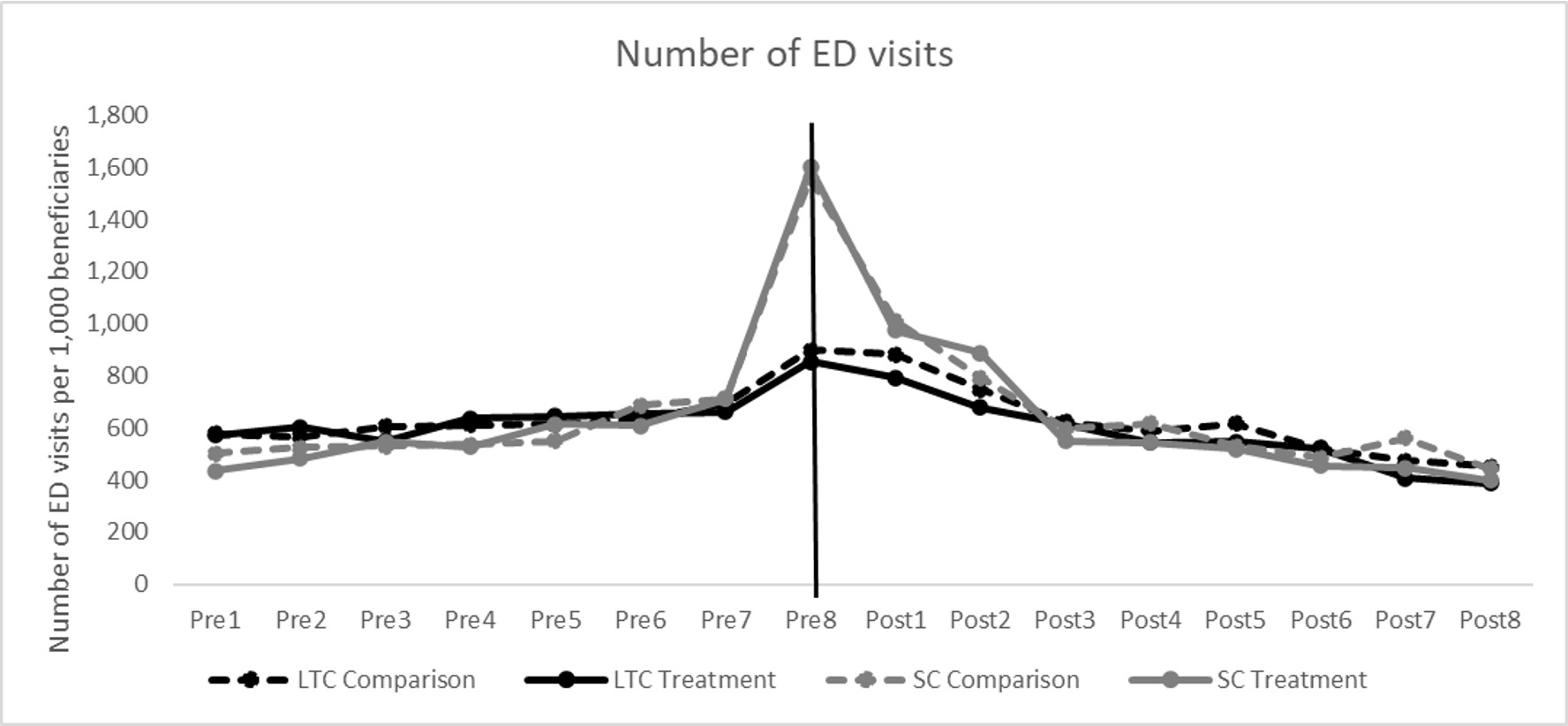
The matched comparison group beneficiaries were very similar to the treatment group on baseline measures (means for the two groups were within 0.05 standard deviations of each other for all but one baseline variable). They also showed similar trends for hospital admissions, ED visits, and total Medicare expenditures during the 24‐month period before enrollment (Figures [Link], [Link]).
Table 1 also shows that short‐term skilled care residents had higher health risks on average than long‐term care residents. Skilled care residents had higher HCC risk scores at baseline (2.7 vs. 2.2) and were expected to have a higher need for care, indicated by the RUG‐IV case‐mix index (49 vs. 40), than long‐term care residents. Skilled care residents also had higher Medicare expenditures and rates of inpatient service use during the baseline year than long‐term care residents. Medicare coverage for nursing facility costs explains part of the difference in baseline expenditures and service use between the two groups of nursing home residents. Long‐term nursing home care is not covered under Medicare, and thus the cost of long‐term care is not captured in our total expenditures measure.
3.2. Effect of eLTC program on service use and expenditures
3.2.1. Long‐term care nursing home residents
For long‐term care nursing home residents, the regression‐adjusted total Medicare expenditures for treatment group beneficiaries decreased by roughly 1% (from $1987 PBPM in the baseline year to $1970 PBPM) over the 24‐month follow‐up period (Table 2). During the same period, the Medicare expenditures for the comparison group beneficiaries increased from $2148 to $2204 PBPM. The differential change between the two groups suggests that the eLTC program was associated with a marginally significant reduction of Medicare expenditures by $73 PBPM (p = 0.08) over 2 years, which represents a 3.6% reduction from what the treatment group mean would have been absent in the program (the treatment group's predicted mean in the follow‐up period minus the estimated effect). The estimated relative reduction in Medicare expenditures was similar in the first and second follow‐up years: $81 PBPM (p = 0.07) in Year 1 and $89 PBPM (p = 0.08) in Year 2.
TABLE 2.
Estimated effect of the eLTC program on service use and spending outcomes among long‐term care beneficiaries
| Treatment group mean (N = 7194) | Comparison group mean (N = 19,713) | Estimated effect (SE) | Percent effect | p‐value | |
|---|---|---|---|---|---|
| Total Medicare expenditures ($ PBPM) | |||||
| Baseline year | 1987 | 2148 | |||
| Follow‐up year 1 | 2109 | 2351 | −81* (44) | −3.7% | 0.07 |
| Follow‐up year 2 | 1855 | 2105 | −89* (53) | −4.6% | 0.09 |
| Cumulative | 1970 | 2204 | −73* (42) | −3.6% | 0.08 |
| Hospital stays (per 1000 beneficiaries) | |||||
| Baseline year | 805 | 888 | |||
| Follow‐up year 1 | 793 | 880 | −4.1 (20) | −0.5% | 0.84 |
| Follow‐up year 2 | 738 | 855 | −35 (25) | −4.5% | 0.17 |
| Cumulative | 753 | 845 | −9.9 (19) | −1.3% | 0.60 |
| ED and observation visits (per 1000 beneficiaries) | |||||
| Baseline year | 814 | 831 | |||
| Follow‐up year 1 | 779 | 871 | −75*** (22) | −8.8% | <0.01 |
| Follow‐up year 2 | 757 | 841 | −66** (28) | −8.0% | 0.02 |
| Cumulative | 772 | 863 | −73*** (21) | −8.6% | <0.01 |
| Likelihood of readmission within 30 days of hospital discharge (percentage) | |||||
| Baseline year | 18 | 18 | |||
| Follow‐up year 1 | 22 | 22 | −1.0 (1.0) | −4.3% | 0.30 |
| Follow‐up year 2 | 18 | 18 | −0.89 (1.4) | −4.7% | 0.52 |
| Cumulative | 21 | 21 | −0.98 (0.94) | −4.5% | 0.30 |
Note: Estimated effects for expenditures and number of visits or stays are based on a difference‐in‐differences approach and show the regression‐adjusted change for the treatment group relative to that for the comparison group between the baseline and follow‐up periods. The estimated effect for the binary outcome of any readmission within 30 days of hospital discharge is a regression‐adjusted treatment–comparison difference based on a cross‐sectional regression that controls for a beneficiary's baseline characteristics and discharge‐level risk factors for having a readmission. The follow‐up years are beneficiary‐specific and defined relative to each beneficiary's date of enrollment. Percentage effect is relative to a counterfactual value defined as the regression‐adjusted treatment group mean minus the estimated effect.
Abbreviations: ED, emergency department; eLTC, eLongTermCare; PBPM, per beneficiary per month.
Significantly different from zero at the 0.10 level, two‐tailed test.
Significantly different from zero at the 0.05 level, two‐tailed test.
Significantly different from zero at the 0.01 level, two‐tailed test.
Consistent with the estimated reduction in total expenditures, the eLTC program was associated with a statistically significant estimated reduction of 73 ED visits per 1000 beneficiaries (p < 0.01), or 8.6% over the two‐year follow‐up period. The number of hospitalizations declined by 52 per 1000 beneficiaries during the two‐year period in the treatment group, compared with a decline of 43 per 1000 beneficiaries in the comparison group. However, the estimated number of hospitalizations and the likelihood of 30‐day readmission were not statistically significant, suggesting that any effects the eLTC program had on hospitalizations or readmission among long‐term care residents were small or nonexistent.
Because the eLTC program provided risk‐stratified transitional care coordination services to newly admitted residents only (and not existing residents), the program effects might concentrate more on the newly admitted beneficiaries. To test this hypothesis, we re‐estimated the regression model by including only residents who enrolled after the start of the eLTC program (accounting for about 22% of the treatment group of long‐term care residents). As expected, the estimated program effects are larger for the group of newly admitted long‐term care residents than for the full group (Table 3). For this group of beneficiaries over the two‐year follow‐up period, the eLTC program was associated with estimated reductions in total Medicare expenditures by $467 PBPM (p < 0.01, 11.3% effect), 237 per 1000 beneficiaries fewer ED visits (p < 0.01, 18.5% effect), and 84 fewer hospitalizations (p < 0.01, 6.1% effect) relative to the comparison group.
TABLE 3.
Estimated effect of the eLTC program on service use and spending outcomes among newly admitted long‐term care beneficiaries
| Treatment group mean (N = 1558) | Comparison group mean (N = 5082) | Estimated effect (SE) | Percent effect | p‐value | |
|---|---|---|---|---|---|
| Total Medicare expenditures ($ PBPM) | |||||
| Baseline year | 2444 | 2665 | |||
| Follow‐up year 1 | 4230 | 4975 | −524*** (115) | −11.0% | <0.01 |
| Follow‐up year 2 | 2526 | 2976 | −229 (146) | −8.3% | 0.12 |
| Cumulative | 3671 | 4359 | −467*** (111) | −11.3% | <0.01 |
| Hospital stays per 1000 beneficiaries | |||||
| Baseline year | 1177 | 1325 | |||
| Follow‐up year 1 | 1445 | 1693 | −100** (50) | −6.5% | 0.05 |
| Follow‐up year 2 | 1015 | 1209 | −47 (70) | −4.4% | 0.51 |
| Cumulative | 1290 | 1521 | −84* (47) | −6.1% | 0.07 |
| ED & observation visits per 1000 beneficiaries | |||||
| Baseline year | 1255 | 1207 | |||
| Follow‐up year 1 | 1128 | 1316 | −236*** (59) | −17.3% | <0.01 |
| Follow‐up year 2 | 827 | 1008 | −229*** (77) | −21.7% | <0.01 |
| Cumulative | 1044 | 1233 | −237*** (57) | −18.5% | <0.01 |
| Percentage likelihood of hospital discharges with a 30‐day readmission | |||||
| Baseline year | 21 | 21 | |||
| Follow‐up year 1 | 27 | 28 | −1.4 (2.0) | −4.9% | 0.50 |
| Follow‐up year 2 | 22 | 17 | 4.1 (3.0) | 22.9% | 0.18 |
| Cumulative | 27 | 26 | −0.64 (1.9) | −2.3% | 0.74 |
Note: Estimated effects for expenditures and number of visits or stays are based on a difference‐in‐differences approach and show the regression‐adjusted change for the treatment group relative to that for the comparison group between the baseline and follow‐up periods. The estimated effect for the binary outcome of any readmission within 30 days of hospital discharge is a regression‐adjusted treatment–comparison difference based on a cross‐sectional regression that controls for a beneficiary's baseline characteristics and discharge‐level risk factors for having a readmission. The follow‐up years are beneficiary‐specific and defined relative to each beneficiary's date of enrollment. Percentage effect is relative to a counterfactual value defined as the regression‐adjusted treatment group mean minus the estimated effect.
Abbreviations: ED, emergency department; eLTC, eLongTermCare; PBPM, per beneficiary per month.
Significantly different from zero at the 0.10 level, two‐tailed test.
Significantly different from zero at the 0.05 level, two‐tailed test.
Significantly different from zero at the 0.01 level, two‐tailed test.
3.3. Skilled care nursing home residents
For short‐term skilled care beneficiaries, the eLTC program was associated with an estimated reduction of 85 ED visits per 1000 beneficiaries (p = 0.03), or 9.7% over the two‐year period (Table 4). However, the estimated reduction in ED visits was not large enough to result in a statistically significant reduction in total Medicare expenditures. Neither was there a discernable change in the number of hospitalizations and likelihood of 30‐day readmission. We did not repeat the analysis on newly admitted short‐term skilled care beneficiaries, because virtually all beneficiaries in this group were newly admitted.
TABLE 4.
Estimated effect of the eLTC program on service use and spending outcomes among skilled care beneficiaries
| Treatment group mean (N = 2414) | Comparison group mean (N = 4907) | Estimated effect (SE) | Percent effect | p‐value | |
|---|---|---|---|---|---|
| Total Medicare expenditures ($ PBPM) | |||||
| Baseline year | 2810 | 2975 | |||
| Follow‐up year 1 | 2823 | 2906 | 83 (75) | 3.0% | 0.27 |
| Follow‐up year 2 | 1932 | 2126 | −29 (102) | −1.5% | 0.78 |
| Cumulative | 2493 | 2602 | 57 (74) | 2.3% | 0.44 |
| Hospital stays per 1000 beneficiaries | |||||
| Baseline year | 1472 | 1507 | |||
| Follow‐up year 1 | 567 | 617 | −15 (32) | −2.6% | 0.63 |
| Follow‐up year 2 | 705 | 738 | 2.2 (47) | 0.3% | 0.96 |
| Cumulative | 592 | 636 | −8.8 (30) | −1.5% | 0.77 |
| ED & Observation visits per 1000 beneficiaries | |||||
| Baseline year | 977 | 977 | |||
| Follow‐up year 1 | 815 | 896 | −81* (43) | −9.0% | 0.06 |
| Follow‐up year 2 | 729 | 837 | −108** (55) | −12.9% | 0.05 |
| Cumulative | 793 | 878 | −85** (40) | −9.7% | 0.03 |
| Percentage likelihood of hospital discharges with a 30‐day readmission | |||||
| Baseline year | 21 | 19 | |||
| Follow‐up year 1 | 13 | 13 | −0.52 (1.5) | −3.8% | 0.73 |
| Follow‐up year 2 | 17 | 12 | 4.7** (2.3) | 38.2% | 0.05 |
| Cumulative | 13 | 13 | 0.26 (1.5) | 2.0% | 0.86 |
Note: Estimated effect for expenditures and number of visits or stays are based on a difference‐in‐differences approach and show the regression‐adjusted change for the treatment group relative to that for the comparison group between the baseline and follow‐up periods. The estimated effect for the binary outcome of any readmission within 30 days of hospital discharge is a regression‐adjusted treatment–comparison difference based on a cross‐sectional regression that controls for a beneficiary's baseline characteristics and discharge‐level risk factors for having a readmission. The follow‐up years are beneficiary‐specific and defined relative to each beneficiary's date of enrollment. Percentage effect is relative to a counterfactual value defined as the regression‐adjusted treatment group mean minus the estimated effect.
Abbreviations: ED, emergency department; eLTC, eLongTermCare; PBPM, per beneficiary per month.
Significantly different from zero at the 0.10 level, two‐tailed test.
Significantly different from zero at the 0.05 level, two‐tailed test.
3.4. Robustness test
To test the robustness of our results, we re‐estimated the regression models for expenditures, hospitalizations, and outpatient ED visits, using a baseline period covering 2 years before the enrollment date—as opposed to 1 year only as in the main analysis. This test helps assess the parallel trends assumption for the difference‐in‐differences model. If trends in outcomes for the treatment and comparison groups are not parallel during the baseline period, the estimated effects are likely to change substantially as the baseline period extends back an additional year. Results from this analysis are qualitatively similar to the main results (see Table S2).
4. DISCUSSION
This study assessed the effects of a telehealth program for nursing home residents. The results suggest that the eLTC program reduced the number of ED and observation visits among long‐term care Medicare residents. The reduced hospital service use might have also reduced total Medicare expenditures, but the estimated effect was small and imprecise. However, the program had larger estimated effects and led to a greater reduction in the number of hospitalizations and Medicare expenditures among newly admitted long‐term care residents, who received telehealth transitional care coordination in addition to having access to telehealth consults with specialists. For beneficiaries in short‐term skilled nursing care, the program led to fewer ED and observation visits but had no discernable effect on total Medicare expenditures. The lack of program effects on Medicare expenditures among skilled care beneficiaries could be due to less exposure to the intervention, given that skilled care beneficiaries in the study spent fewer than 60 days in nursing homes on average.
Avera Health's comprehensive, continuous support for frontline staff may have contributed to the favorable estimated effect of the eLTC program in participating nursing homes. Qualitative information collected in the study suggested that Avera Health provided frequent, intense training to frontline staff who were responsible for initiating telehealth consults. The training aimed at helping staff identify early changes in residents' conditions that could be medically addressed through a telehealth consult, thereby avoiding unnecessary ED or hospital transfers. According to Avera Health, these training efforts yielded high levels of engagement and satisfaction by the nursing staff, which is a possible driver of the favorable program effects. 13
Although the estimated reduction in Medicare expenditures for long‐term care beneficiaries is small and lacks statistical significance, its consistency with results for service use outcomes suggests that if CMS were to implement a program such as eLTC in nursing homes nationwide, it might generate modest savings for Medicare through the reduced hospital and ED use among Medicare beneficiaries residing in nursing facilities. At the time of the intervention, Avera Health reported that it would take a one‐time fee of $250 plus a monthly fee of $55 per resident to cover the cost of the eLTC program (regardless of the frequency of telehealth consults provided). Using the average length of stay of 19 months for long‐term care residents in our treatment group, we estimated that eLTC would have an incremental cost of about $68 PBPM ([$250/19 months] + $55), compared with the usual care a resident would receive in a nursing home such program. Considering the estimated reduction of $73 PBPM in Medicare expenditures due to eLTC (i.e., the difference‐in‐differences savings estimate for Medicare long‐term care residents), the program would generate a net saving of $5 PBPM, amounting to a total saving of $95 per long‐term care resident over the average stay.
There are several caveats to our savings estimate of $95 per long‐term care resident. First, the 95% confidence interval for our point estimate of $73 PBPM was large, ranging from a cost reduction of $155 PBPM to a cost increase of $8 PBPM. Second, our study was based on a group of nursing homes that chose to participate in Avera Health's eLTC program, which may differ from other nursing homes in ways that limit the generalizability to the potential effect of the program. For example, the nursing homes participating in the intervention might have been more invested in other quality improvement strategies than non‐participating nursing homes, making the eLTC program more likely to yield a favorable effect on their residents. For these reasons, the actual total cost savings to Medicare can be much higher or lower than $95 per long‐term care resident if a program like eLTC was implemented nationally.
4.1. Limitations
This study has several limitations. First, the study was based on a matched group design rather than a randomized control trial. The treatment and comparison beneficiaries might have had different trajectories of outcomes over time, even in the absence of the intervention, which could lead to a biased estimate of the program effect. The close match of the two groups on the baseline characteristics of residents and facilities, along with a fixed‐effects specification to net out any time‐invariant differences on unobservables and the parallel trends in outcomes observed in the baseline period, lessen our concern about remaining biases. Second, we were not able to obtain cost and other outcome data for nursing home residents who had only Medicaid coverage. Thus, we cannot assess whether the program would generate savings for Medicaid for those residents, since they may have quite different needs and risks for hospitalization than less economically disadvantaged patients. Furthermore, we were unable to assess whether the program might have reduced Medicaid costs for dual‐eligible beneficiaries by limiting the need for transferring patients to infirmaries and other more intensive care sections of the nursing home. Third, sample sizes for minority populations were insufficient to assess whether the program was able to reduce any racial disparities in outcomes. Finally, as noted above, the facility‐level differences between Avera Health's nursing homes and other nursing homes across the nation may limit the generalizability of this study. Nonetheless, the results suggest that expanding the use of telehealth in nursing homes could benefit residents through reduced hospital service use and potentially lower spending.
4.2. Implications
Findings from this study provide three important implications for nursing homes, payers, plans, and policy makers. First, when implemented effectively, telehealth can be a useful tool to enhance care coordination and provide timely access to care for nursing home residents. Our findings are consistent with existing evidence that telehealth interventions can reduce hospitalizations and ED visits in nursing homes. 6 , 7 , 11
Second, although our study did not test the effect of training frontline staff on job satisfaction, Avera Health's emphasis on high‐quality staff training as part of the eLTC intervention is consistent with the literature that suggested a positive correlation between training support and staff satisfaction and quality of care in nursing home facilities. 15 As COVID‐19 accelerated the diffusion of digital technologies in the health care system, more research is needed to understand the effective strategies that help engage frontline nursing home staff with new technologies while maintaining staff morale and satisfaction.
Third, despite the advantages of the program for patients and potential cost savings to payers, nursing homes may have limited financial incentives to adopt similar telehealth interventions. In the current payment model, nursing homes have to cover the full cost of telehealth programs—which is not a trivial amount in the case of eLTC. The Medicare SNF Patient‐Driven Payment Model and SNF Value‐Based Purchasing program both provide incentives for nursing homes to reduce hospital readmissions among SNF patients. But, given that Medicaid is the largest payer for long‐term care, it is unclear whether the Medicare incentives alone will lead nursing homes to widely adopt telehealth programs. Medicare Advantage plans might have an incentive to encourage telehealth visits for their enrollees who are in long‐term care facilities, but relatively few nursing home residents are enrolled in Medicare Advantage. 16 Emerging capitated payment initiatives may provide incentives for a broader range of health care organizations to invest in nursing home telehealth. For example, the CMS Direct Contracting Model offers ACO‐like organizations and Medicaid Managed Care Organizations the opportunity to take on the financial risk for managing patients' total cost of care. These organizations may be more willing to pay for a telehealth program in affiliated nursing homes if they provide long‐term and post‐acute care to many attributed beneficiaries. As value‐based purchasing continues to evolve, more research is needed to examine the value to payers for improved nursing home outcomes, as well as to explore payment models that encourage the expansion of telehealth services in nursing homes.
Supporting information
Appendix S1. Supplementary information.
Figure S1. Unadjusted mean total Medicare expenditures by quarter and treatment group
{kind=link}
Figure S2. Unadjusted mean number of hospitalizations by quarter and treatment group
{kind=link}
Figure S3. Unadjusted mean number of emergency department visits by quarter and treatment group
{kind=link}
ACKNOWLEDGMENTS
Many individuals contributed to this study. We acknowledge the important contribution made by Mark Flick, Xiao Barry, and Lauryn Ringwood, who skillfully processed and helped analyze data used for this study. We also thank Avera Health for providing us with information about its program. The evaluation of the eLTC program was funded by the Centers for Medicare & Medicaid Services, Center for Medicare & Medicaid Innovation, contract number: HHSM‐500‐2014‐00034I/HHSM‐500‐T0001. The views expressed herein are those of the authors and do not necessarily reflect those of the Centers for Medicare & Medicaid Services or the US Department of Health and Human Services.
Li Suhui ( Evelyn), Hossain M, Gilman B, Forrow LV, Lee KM, Brown R. Effects of a nursing home telehealth program on spending and utilization for Medicare residents. Health Serv Res. 2022;57(5):1191‐1200. doi: 10.1111/1475-6773.13936
Funding information Centers for Medicare and Medicaid Services, Grant/Award Number: HHSM‐500‐2014‐00034I/HHSM‐500‐T0001
REFERENCES
- 1. Koonin LM, Hoots B, Tsang CA, et al. Trends in the use of telehealth during the emergence of the COVID‐19 pandemic ‐ United States, January‐march 2020. Morb Mortal Wkly Rep. 2020;69(43):1595‐1599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Totten AM, Hansen RN, Wagner J, et al. Telehealth for acute and chronic care consultations. Comparative Effectiveness Review. 2019. No. 216(AHRQ Publication No. 19‐EHC012‐EF). [PubMed]
- 3. Baker LC, Johnson SJ, Macaulay D, Birnbaum H. Integrated telehealth and care management program for Medicare beneficiaries with chronic disease linked to savings. Health Aff. 2011;30(9):1689‐1697. [DOI] [PubMed] [Google Scholar]
- 4. Dinesen B, Haesum LK, Soerensen N, et al. Using preventive home monitoring to reduce hospital admission rates and reduce costs: a case study of telehealth among chronic obstructive pulmonary disease patients. J Telemed Telecare. 2012;18(4):221‐225. [DOI] [PubMed] [Google Scholar]
- 5. Cryer L, Shannon SB, Van Amsterdam M, Leff B. Costs for ‘hospital at home’ patients were 19 percent lower, with equal or better outcomes compared to similar inpatients. Health Aff. 2012;31(6):1237‐1243. [DOI] [PubMed] [Google Scholar]
- 6. Grabowski DC, O'Malley AJ. Use of telemedicine can reduce hospitalizations of nursing home residents and generate savings for Medicare. Health Aff. 2014;33(2):244‐250. [DOI] [PubMed] [Google Scholar]
- 7. Joseph JW, Kennedy M, Nathanson LA, Wardlow L, Crowley C, Stuck A. Reducing emergency department transfers from skilled nursing facilities through an emergency physician telemedicine service. West J Emerg Med. 2020;21(6):205‐209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Batsis JA, DiMilia PR, Seo LM, et al. Effectiveness of ambulatory telemedicine care in older adults: a systematic review. J Am Geriatr Soc. 2019;67(8):1737‐1749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Shigekawa E, Fix M, Corbett G, Roby DH, Coffman J. The current state of telehealth evidence: a rapid review. Health Aff. 2018;37(12):1975‐1982. [DOI] [PubMed] [Google Scholar]
- 10. Morley JE. Telemedicine: coming to nursing homes in the near future. J Am Med Dir Assoc. 2016;17(1):1‐3. [DOI] [PubMed] [Google Scholar]
- 11. Groom LL, McCarthy MM, Stimpfel AW, Brody AA. Telemedicine and telehealth in nursing homes: an integrative review. J Am Med Dir Assoc. 2021;22:1784‐1801.e7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Alexander GL, Powell KR, Deroche CB. An evaluation of telehealth expansion in US nursing homes. J Am Med Inform Assoc. 2021;28(2):342‐348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Gilman B, Whicher D, Brown R, et al. Evaluation of the health care innovation awards, round 2: final report. Evaluation of the Health Care Innovation Awards, Round 2. 2020. https://innovation.cms.gov/data-and-reports/2020/hcia2-round-2-final-eval-report-sept-2020-0.
- 14. Centers for Medicare and Medicaid Services. CMS program statistics‐ 2019 Medicare Sections. 2021.
- 15. Rajamohan S, Porock D, Chang Y. Understanding the relationship between staff and job satisfaction, stress, turnover, and staff outcomes in the person‐centered care nursing home arena. J Nurs Scholarsh. 2019;51(5):560‐568. [DOI] [PubMed] [Google Scholar]
- 16. Jung HY, Li Q, Rahman M, Mor V. Medicare advantage enrollees' use of nursing homes: trends and nursing home characteristics. Am J Manag Care. 2018;24(8):e249–e256. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1. Supplementary information.
Figure S1. Unadjusted mean total Medicare expenditures by quarter and treatment group
Figure S2. Unadjusted mean number of hospitalizations by quarter and treatment group
Figure S3. Unadjusted mean number of emergency department visits by quarter and treatment group