

INTRODUCTION
Leiomyomas are benign tumors that originate on the smooth muscle, usually found in the uterus, gastrointestinal tract and skin. This type of tumor rarely occurs in the oral cavity, specially because of the lack of smooth muscle in this area1. Its most frequent location in this region, by decreasing order of appearance is: lips, palate, tongue and oral mucosa2. It is usually asymptomatic; however it may be painful in some cases.
Our goal with this paper is to report on a case of a patient with a painful tongue leiomyoma.
CASE REPORT
A 34 year old man, with the Acquired Immunedeficiency Syndrome (AIDS), visited the physician, complaining of a spontaneous stinging pain in the oral cavity for 2 years. During exam we saw a reddish mass, of regular contours, measuring about one centimeter in diameter, located on the tongue base. Tecnecium-99 scintigraphy used to assess the presence of ectopic thyroid tissue was negative.
The tumor was biopsied and the pathology (Figure 1) showed a solid type of leiomyoma with positive immunohistochemistry for desmine and actine. The lesion was removed through the mouth. The pain improved in the post-operative and the one year follow up did not show recurrence.
Figure 1.
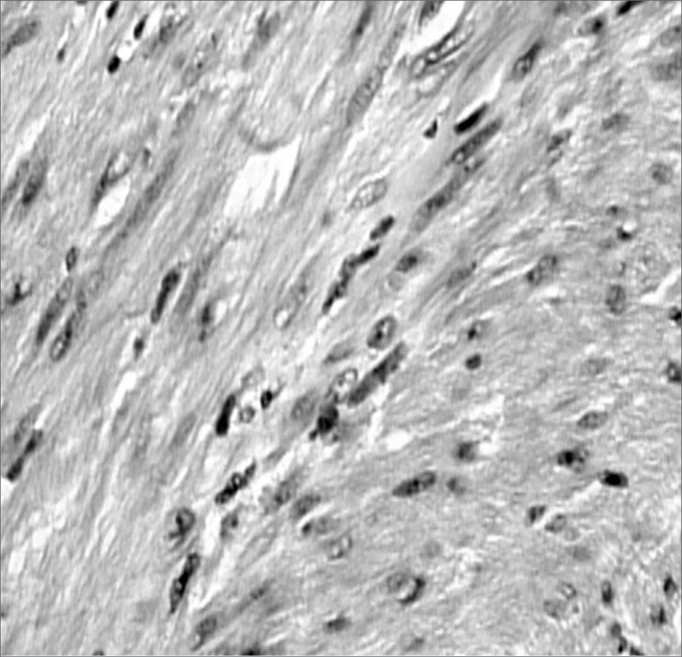
Histopathology confirming it to be a leiomyoma with prolipheration of elongated cells with fasciculated and other times stirred arrangement (100X magnification- Dyed by Hematoxylin & eosin).
DISCUSSION
Leiomyomas may be divided according to the World Health Organization in three types: angioleiomyomas, solid leiomyomas and leiomyoblastomas. The most common type in the oral cavity is the angioleiomyoma, with 74% prevalence rate, followed by the solid leiomyoma, the most common in the tongue, with 25%3 prevalence. The smooth muscle tumor origin in the oral cavity could be in the middle layer of the arteries, ectopic smooth muscle tissues or the tongue taste buds2.
Its occurrence on the tongue was reported in only 23 cases in the English literature2. Its color varies from reddish to bluish, depending on its vascularization. Its painful tongue location is rare, with only one case reported in the literature4. The pain mechanism is not clear; it is believed to be caused by muscle contractions over the tumor vascularization, causing ischemia4. As clinical and histopathology differential diagnosis we have: leiomyosarcoma, fibroma, neurofibroma and lipoma.
We did not find other cases of painful leiomyomas in AIDS patients.
FINAL COMMENTS
Tongue base leiomyoma differential diagnosis must be carried out bearing in mind the other tumors that may affect this region, and be specially based on histopathology. Pain, although rare, may be its major manifestation, such as the one reported here. This is its first publication of an occurrence in an AIDS patient.
Footnotes
Paper submitted to the ABORL-CCF SGP (Management Publications System) on March 11th, 2005 and accepted for publication on May 1st, 2006. Cod. 103.
REFERENCES
- 1.Lloria Benet M, Bagan J, Miguel E Morant A, Alonso S. Leiomioma oral: a propósito de un caso clínico. Med Oral. 2003;8:215–219. [PubMed] [Google Scholar]
- 2.Kotler H, Gould N, Gruber B. Leiomyoma of the tongue presenting as congenital airway obstruction. Int J Pediatr Otorhinolaryngol. 1994;29:139–145. doi: 10.1016/0165-5876(94)90093-0. [DOI] [PubMed] [Google Scholar]
- 3.Brooks JK, Nikitakis NG, Goodman NJ. Clinicopathologic characterization of oral angioleiomyomas. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;94:221–227. doi: 10.1067/moe.2002.125276. [DOI] [PubMed] [Google Scholar]
- 4.Toida M, Koizumi H, Shimokawa K. Painful Angiomyoma of the Oral Cavity:report of a case and review of the literature. J Oral Maxillofac Surg. 2000;58:450–453. doi: 10.1016/s0278-2391(00)90935-2. [DOI] [PubMed] [Google Scholar]