

Abstract
Non-invasive pressure and flow data from Venturi-based sensors can be used with validated models to identify patient-specific lung mechanics. To validate applied respiratory models a secondary measurement is required. Rotary encoder-based tape measures were designed to capture change in circumference of a subject’s thorax and diaphragm. Circumferential changes can be correlated to measured or modelled change in lung volume and associated muscular recruitment measures (patient work of breathing). Hence, these simple measurement devices can expedite respiratory research, by adding low-cost, accessible, and clinically useful measurements.
Keywords: CPAP, Respiration, Pressure, Flow, Venturi, Thoracic, Abdominal
Specifications table
| Hardware name | Respiratory bi-directional pressure and flow data collection device with auxiliary thoracic and abdominal circumferential monitoring. |
| Subject area |
|
| Hardware type |
|
| Closest commercial analog | Flow sensor units are commercially available but are expensive. The circumferential monitoring has been done using motion capture in research, but no commercial analog exists. |
| Open source license | Creative Commons Attribution-ShareAlike license |
| Cost of hardware | ∼ $550 NZD |
| Source file repository | https://doi.org/10.17632/wfw7nyctcy.1 |
| OSHWA certification UID (OPTIONAL) | NZ000002 |
Hardware in context
This work presents two devices, comprising: 1) a respiratory pressure and flow sensing system; and 2) a dynamic chest circumference measurement system, both of which are designed for research studies and settings. They are designed for joint use, but can be deployed separately for their individual capabilities. The primary intended use of these devices is 1) to provide pressure and flow data which respiratory mechanics models can be applied to and tested; and 2) to validate and assess patient effort and tidal volume in measuring using dynamic chest and abdominal circumferences.
The respiratory pressure and flow sensing system is designed to provide data for respiratory modelling, typically based on airway flow and pressure measurements. Commercial flow meters with corresponding software are expensive (∼USD$1300 [1]). Simple, low-cost, 3D printed Venturi sensors have been previously designed for determining one directional flow in respiratory research [2]. Both inspiratory and expiratory data is useful in modelling lung mechanics. In particular, in passive breathing, expiration is a predominantly passive process and can be used to identify or calculate passive lung mechanics parameters before considering active patient-driven inspiratory mechanics. Hence, in this study, the 3D printed Venturi design of [2] is extended to measure bidirectional flow, where the original application in mechanical ventilation required only unidirectional flow measurement.
Validation of respiratory models is challenging and often requires invasive measurements or maneuvers [3], [4], [5]. Thus, validation of respiratory models of healthy or partially assisted (non-invasive MV) poses particular difficulty, as these measurements are not ethically or clinically feasible for conscious subjects. However, motion capture, inductance plethysmography, and strain gauge belts/ garments have been used to non-invasively measure changes in thoracic and abdominal volumes, but they require careful calibration, specific location conditions such as unobstructed view, and/or purchase of specialty equipment [6], [7], [8], [9]. In this study, a basic tape measure is modified using a rotary encoder and spring to output dynamic change in unspooled length, which generates similar data to commercial analogs, at a much lower cost and higher degree of customization. Further, calibration can simply be made against visual tape markers.
While the quoted cost is approximately NZ$550 (NZ$280 for two tape measures without Venturi), the devices are designed for utility to researchers who likely have access to stocked bulk components. Thus, standard materials (microcontrollers and fasteners) were used, reducing the primary cost of the device to the researcher to the sensors (∼$400 NZD). The differential pressure sensors are more expensive than in previous designs [2] ($73 NZD), as they were chosen for higher accuracy at low-flow levels common in healthy passive breathing where the system in [2] was used for mechanical ventilation research with higher flows and pressures. Limited access to electrical components in the wake of the COVID-19 pandemic and war in Ukraine, also restricted choices for sensors and increased cost. The design is customisable for lower cost sensors. However, the desired flow range and required accuracy should be considered.
Hardware description
The Venturi flow meter is adapted from a basic 3D printed design [2], to monitor differential pressure in both directions and at lower flow rates, which can be combined to generate complete breath profiles. The Venturi is designed to be integrated in series with respiratory circuitry, combined 22 m cone and 15 mm socket (22 M/15F) connections. In its current application, one end is connected to a CPAP device using its accompanying circuitry, and the other end is connected to Heat and Moisture Exchanger Pleated Mechanical (HEPA) Filter (002874, Smiths Medical, MN, USA), subsequently leading to a Bi-level CPAP System Hospital Mask (RT041S, Fisher and Paykel Healthcare, Auckland, New Zealand).
Auxiliary measurements of thoracic and abdominal circumferences provide external non-invasive data, which can be correlated to change in lung volume. Thus, measurement of change in circumference can be used to validate models of patient-specific lung mechanics applied to the Venturi pressure and flow dataset. Circumference is measured by a flexible fiberglass dressmakers tape spooled onto spring loaded barrel connected to a rotary encoder. Rotary encoder counts are subsequently translated into change in unspooled tape length via calibration.
Ultimately, the devices are designed for respiratory research, specifically the application and validation of computational models designed to ascertain patient-specific respiratory condition using simple non-invasive measurements and parameter identification. The outlined devices provides researchers:
-
-
A low-cost alternative to commercial sensor systems for measuring bi-directional flow and pressure.
-
-
Non-invasive data collection.
-
-
Dynamic chest circumference measurements for validation.
-
-
High level of customization.
Design files
The included device design files are outlined in Table 1 and the type of files are indicated.
Table 1.
Design files summary.
| Design file name | File type | Open source license | Location of the file |
|---|---|---|---|
| BidirectionalVenturi | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Venturi Flow Meter |
| BarbEnds | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Venturi Flow Meter |
| BarbMiddle | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Venturi Flow Meter |
| VenturiStand | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Stand |
| TapeCaseCoupler | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Rotary Encoder Tape Measure |
| TapeCaseHousingBase | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Rotary Encoder Tape Measure |
| TapeCaseHousingLid | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Rotary Encoder Tape Measure |
| TapeCasePin | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Rotary Encoder Tape Measure |
| TapeCasePinCap | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Rotary Encoder Tape Measure |
| TestStand | CAD (SLDPRT) and STL files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 3D Printed Hardware/Stand |
| Control Board | KiCAD files and PDF schematic | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 PCBs/Control Board |
| Pressure Sensor Breakout Board | KiCAD files and PDF schematic | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 PCBs/Flow Meter Breakout Board |
| Rotary Encoder Breakout Board | KiCAD files and PDF schematic | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 PCBs/Tape Measure Breakout Board |
| Arduino Code | Arduino files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 Code/Arduino Code |
| Teensy Code | Teensyduino files | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 Code/TeensyCode |
| Data Collection Code | Matlab file | CC BY 4.0 |
https://doi.org/10.17632/wfw7nyctcy.1 Code/Data Collection Code |
As indicated (Table 1), design files are organized in subfolders: 3D Printed Hardware; PCBs; and Code. Both CAD and STL files are provided for the 3D printed components to allow for modifications to suit different applications. Similarly, KiCAD files and PDF schematics are provided for PCBs and full code files are provided for each of the microcontrollers. The MATLAB data collection code is also included.
Bill of materials
The bill of materials is attached as an excel file (https://doi.org/10.17632/wfw7nyctcy.1).
Build instructions
-
1.
The PCBs (Pressure Sensor Breakout Board, Rotary Encoder Breakout Board, and Control Board) were ordered from LCSC. The device is designed for research use and so several test points are implemented for troubleshooting and a high number of redundant components (primarily for extra connectors and communication lines) are utilised for and extension of the device for future research and in case of damage.
-
2.
PCBs were populated in the SMT lab at the University of Canterbury. Resistors (R), capacitors (C), LEDs (D and WS2812B), connector headers (5055680471), mosfets (BSS138-G), test points (RCTCTE), and the bus splitter (PCA9548APW) were placed onto footprints (to which solder paste had been hand-applied) using a pick and place machine (ProtoPlace S, LPKF Laser and Electronics, Naklo, Slovenia) and reflow soldered in a reflow oven (LPKF ProtoFlow, LPKF Laser and Electronics, Naklo, Slovenia).
-
3.
Pin headers (Headers Male and Female), pressure sensors (P1J-10-AX16PA), and rotary encoder leads (HEDS-8903) were hand-soldered on the PCBs (Fig. 1). Arduino (Arduino Nano v3) and Teensy (Teensy 4.0) microcontrollers were subsequently connected, and code (Arduino Code, and Teensy Code respectively) was uploaded to these boards. The code is written using Arduino IDE (Arduino IDE 1.8.16, Arduino, Somerville, MA, USA), with the Teensyduino software add-on (Teensyduino v1.56, PJRC, Portland, Oregon, USA), and utilizing a downloaded existing library (teensy4_i2c, Richard Gemmell).
-
4.
The Venturi tube (BidirectionalVenturi), middle barb (BarbMiddle), and two end barbs (BarbEnds) were 3D printed using a Prusa Mini (Prusa Mini+, Prusa Research, Prague, Czech Republic). Some filament fibers remained in interior of the barbs and Venturi during some of the prints. These were removed from the Venturi tube using a pipe cleaner and from the barbs using a needle (∼24 gauge). The barbs were then inserted into the Venturi tube and superglued in place. The middle barb (indicated by a notch printed on the outer surface) fits into the barb hole at the Venturi constriction and the two end barbs insert into the holes either side (Fig. 2).
-
5.
The tape measure housing (TapeCaseHousingBase and TapeCaseHousingLid) and coupler (TapeCaseCoupler) were also 3D printed (Fig. 3). The housing and coupler design is specific to the tape measure barrel taken from an inexpensive metal tape measure (5660482) and will need adjustment to fit alternative barrel designs.
-
6.
A basic metal tape measure (5660482) was disassembled to retrieve the barrel with inbuilt torsional spring (Fig. 4a). Making a custom barrel would require winding a torsional spring, which is very expensive in low quantities, but is a basic mechanism which can be removed from most inexpensive tape measures. The tape coupler was press fit into top of the torsional spring barrel (Fig. 4b). The metal tape measure was removed and replaced by a dress-makers fiberglass tape measure (9313792113157). The end of the fiberglass tape measure was adhered to the barrel using epoxy (Fig. 4c). After the glue was cured the tape was wound around the barrel and the barrel was inserted into the base of the tape measure housing (Fig. 4d) using the central ratcheting mechanism.
-
7.
The Pin Cap and Pin (TapeCasePinCap and TapeCasePin) are 3D printed. The tape measure is wrapped and glued around the pin (Fig. 5a) which was then inserted into the cap (Fig. 5b). The length wrapped around is set to ensure the tape reads the 108 mm offset circumference when fully spooled (Fig. 5c), generated due to the width of the tape device.
-
8.
The rotary encoders (HEDM-5500#J12) were attached to the lids of the tape measure housings using M2 8 mm Button Socket Screws and nylock nuts (Fig. 6). The coupler was fit onto the top of the barrel, the lid was attached (Fig. 6a). Finally, the grub screw was tightened to fix the shaft to the rotary encoder Fig. 6b. Attachment of the rotary encoder to the shaft is shown in Fig. 7.
-
9.
The Venturi stand (VenturiStand) was 3D printed. The three pressure breakout boards and the control board were attached to the stand using M3 10, 12, and 16 mm Socket Cap Screws, plastic spacers, and nylock nuts as illustrated in Fig. 8.
-
10.
Pressure tubing (B08JRPLJXK) and tees (T0-1-200NN) were connected between barbs and sensors (Fig. 9), to achieve differential pressure between the intake and constriction in both directions, as well as gauge pressure at the constriction.
-
11.
A basic test frame was laser cut (TestStand) from Perspex. However, a custom stand based on the setting of the trial would be most efficient. The attached frame design indicates the required mounting hole configuration for the device and can be easily adapted to suit varied trial settings. The Venturi stand was attached to the frame by M4 10 mm Socket Cap Screws and nylock nuts and the rotary encoder breakout board was attached by M3 10 mm Socket Cap Screws and nylock nuts (Fig. 10). It is important to note, any test frame meeting the basic mounting requirements and accommodating the PCBs could be used depending on the specific application.
-
12.
The rotary encoder breakout board is connected to the control board by a 300 mm connector lead (451110403) (Fig. 10), and a jumper added (Fig. 10) to allow the nano to power the breakout board. Pressure sensor breakout boards are attached to the control board using 100 and 150 mm connector leads (451110401 and 451110402) (Fig. 10). Rotary encoder breakout board leads are fed through the hole in the frame and attached to the rotary encoder tape devices (Fig. 10). The rotary encoder subsystem can be used separately or in conjunction with the control board, increasing the devices customisability. Using the rotary encoder sub-system separately would require a separate data collection code.
-
13.
Similarly, the Venturi system flow sensor can be used separately to tape measures using a variation of the data collection code. A trial specific test frame is recommended based on the position of the subject being tests (e.g., reclined) to reduce potential sources of user error. The Venturi stand can be attached to any such frame by M4 fasteners.
-
14.
Data collection code (Data Collection Code) for the collective device outlined was written in MATLAB (Matlab 2021b, The Mathworks Inc, Natick, MA, USA). The collection code records the 3 differential pressures, and 2 rotary encoder counts at a frequency of 100 Hz for a designated time period. The code processes the differential pressures (which can later be processed to ascertain bi-directional flow) are converted to cmH2O and rotary encoder counts to circumferences (which can be correlated to change in volume). Rotary encoder counts are also scaled to account for change in spool diameter due to unspooled length. Thus, the thickness of the tape and original barrel diameter should be checked for each device as these may differ due to differences in thickness of fiberglass tape or barrel dimensions. These device-specific values should be input to the data collection code. Raw and processed data files are saved as CSV files.
Fig. 1.

Hand-soldered PCB components.
Fig. 2.

Assembled Venturi with barbs.
Fig. 3.

Tape measure housing components.
Fig. 4.

(a) Disassembly of tape measure, (b) insertion of coupler, (c) attachment of fiberglass tape, and (d) insertion of barrel into base of tape measure housing.
Fig. 5.

Attachment of Tape Pin and Pin Cap.
Fig. 6.

Attachment of rotary encoder to tape housing lid.
Fig. 7.

Attachment of rotary encoder to shaft of coupler by (a) assembly of the tape measure using screws salvaged from dissembled tape measure, (b) tightening of rotary encoder grub screw onto the shaft of the coupler, and (c) careful removal of the grub screw Allen key.
Fig. 8.

Control and Pressure Sensor Breakout Board attachment to Venturi Stand.
Fig. 9.

Differential pressure sensor tubing.
Fig. 10.

Test Frame Assembly.
Operation instructions
-
1.
The computer collecting data is first connected to the Arduino nano. The computer must be connected to the nano prior to any extension of the tape measures (prior to their attachment to a subject). The computer should be connected while the tape measures are fully wound up with the end slotted into the housing (Fig. 11), as they are calibrated to the 108 mm initial circumference in this position.
-
2.
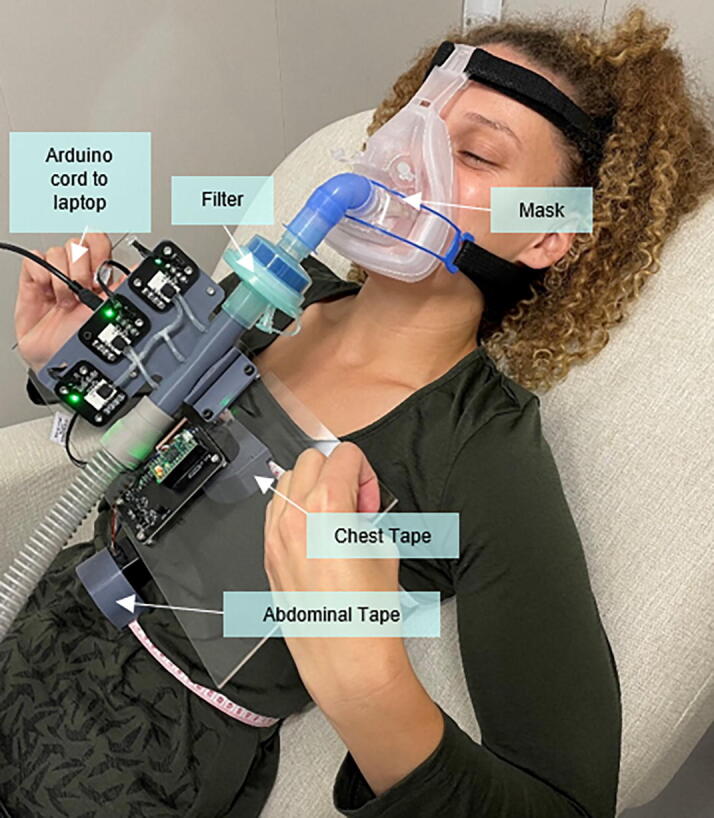
After the computer is connected the boards will be powered, and the tape measures can be fit to the chest and abdomen of the subject (Fig. 12), use physical landmarks specific to the trial requirements (ie armpit height, just below pectoral muscles/bottom of bra, waist, etc.). The Venturi can then be added in series with breathing circuitry, below mask and filter (Fig. 12). The mask should be fit tightly to the subject’s face using the head straps to ensure no expiratory leaks from the mask/face seal. If capturing data with ventilatory support (ie CPAP) an expiration hole is required between the Venturi and the ventilator. If the tape measure falls horizontal rather than sitting vertical (chest tape in Fig. 12) a wedge may be placed below it to ensure it sits vertically. Tape measures sit correctly on reclined subjects. However, wedges are required when the patients are sitting/standing up. For patients of different body sizes, the leads to the rotary encoders could be extended and a longer fiberglass tape wound onto the barrel (with the housing size adjusted accordingly).
-
3.
The sample time length and trial information are input to the MATLAB script prior to data collection (Fig. 13).
-
4.
The script is run and saves both raw and processed data as CSV files. The data is plotted so it can be inspected during the trial (Fig. 14). The smaller nosier peaks from the differential pressure sensors are generated from the respective backflow (throat to outlet), which accounts for their turbulent readings. These peaks are not used in modelling of this dataset as inspiration and expiration are combined in post-processing using data from the appropriate sensor based on flow direction.
-
5.
Basic Data Processing/Analysis would begin with separation of data into breaths, allowing the inspiration and expiration differential pressure to be combined. Flow can then be calculated based on conservation of flow and Bernoulli's Principle:
where, a discharge coefficient () of 0.97, air density () of 1.225 kg/m3, differential pressure () measured over the constriction, and cross-sectional areas (A1 and A2) at the inlet and restriction respectively). Subsequently, flow be integrated to ascertain tidal volume. From there pressure, flow and volume can be input to relevant respiratory models.
Fig. 11.

Device prior to use (tapes spooled prior to system being powered).
Fig. 12.
Trial setup example.
Fig. 13.

Trial information inputs in MATLAB data collection script.
Fig. 14.

MATLAB generated graph of collected data.
Validation and characterization
Venturi flow calibration was conducted using flow generated by a standard CPAP device’s range of PEEP settings (4 – 20 cmH2O in 0.5 cmH2O increments). The measured flow was compared with a TSI 4000 Series externally calibrated flow sensor connected in series with the breathing circuitry and Venturi device (Fig. 15). This calibration illustrated a consistent offset (Fig. 16), likely due to losses through the Venturi. Venturi flow was subsequently scaled by the average percentage offset to achieve an average error in delivered flow of 0.0075 % (Fig. 16). This calibration scaling can be implemented based on data usage in the processing of the flow (not included in the attached code).
Fig. 15.

Flow calibration schematic.
Fig. 16.
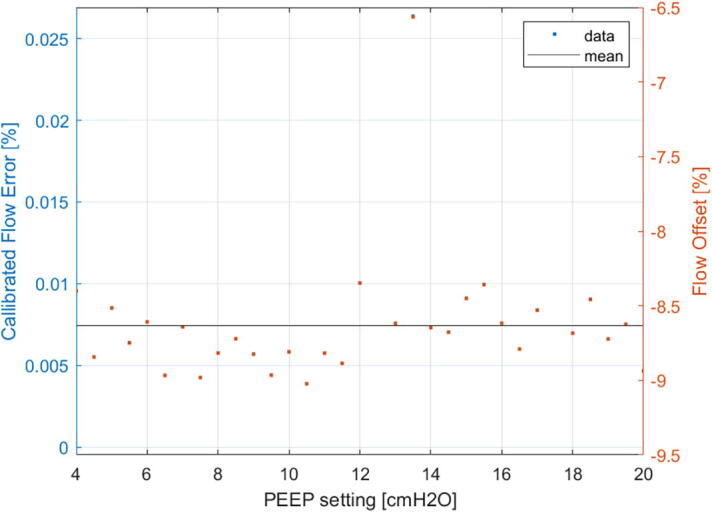
Calibration of Venturi Flow Sensors (Mean offset = -8.6382 %) and Error in Calibrated Flow (Mean Error = 0.0075 %).
To ensure the tape measures are correctly calibrated they should be plugged in while fully wound (108.0 mm), extended to the maximum 1500.0 mm length, and retracted back to fully wound (108.0 mm). If the recorded circumference does not return to 108.0 mm the encoder should be checked for damage. If the recorded peak is not 1500.0 mm, but returns to the 108 mm reading the barrel diameter and tape thickness for the specific device should be checked and altered in the code before further troubleshooting.
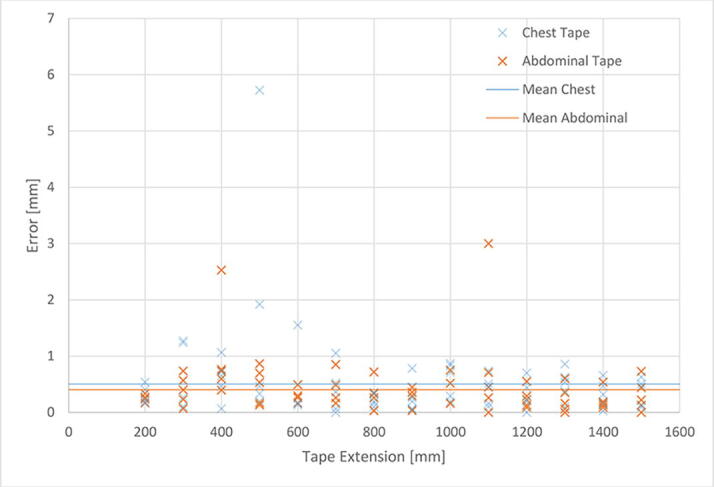
Tapes were validated using the tape measure increments (1 mm). Each tape measure was extended to read 200.0 mm, extended to read 300.0 mm, subsequently retracted by 100.0 mm then increased by 200 mm until the maximum 1500.0 mm extension, retracted to 1400.0 mm, and finally increased to 1500 mm again. These points were determined using the markings on the fiberglass tape. The resultant two measurements of each increment of 100.0 mm were compared and the absolute error calculated. The validation test was repeated five times for each tape to generate error distributions (Fig. 17).
Fig. 17.
Validation of the tape measures.
The average error was 0.5 and 0.4 mm for the chest and abdominal tape measure devices, respectively. The rotary encoder tape gives a higher degree of accuracy than manually reading the printed tape measure increments (1.0 mm) and so would require further validation tests to assess any higher degree of accuracy. However, this level of accuracy was not required for its current use in this respiratory research where errors up to 1.0 mm are more than tolerable. The errors outside the 1.0 mm accuracy was likely due to error in judgment of the markers on the tape measure, for example the over 5.0 mm error outlier is likely due to extension to the line next 5.0 mm line from the desired marker.
Characterization of hardware performance:
-
-
Maximum circumference is 1500.0 mm using existing tape measure device.
-
-
Minimum circumference of 200.0 mm as at smaller circumferences (down to physical 108.0 mm minimum) the torsional spring does not provide sufficient force to consistently retract the tape.
-
-
The 54.0 mm flat section of tape measure creates an error in measuring when placed on a curved surface. However, this error is minimal on most body types as the tape is placed on the sternum or center of abdominal muscles, respectively, which provides a relatively flat surface.
Human and animal rights
Subjects were given a written and verbal explanation of the test protocol before signing a consent form. Subjects were made aware they could inform a researcher they wished to withdraw from the testing point at any point and testing would be terminated immediately and their data would be deleted.
Ethical consent was granted by the Human Ethics Committee at the University of Canterbury (Ref: HEC 2020/14/LR) with amendments to add thoracic and abdominal circumference measurements granted 22 NOV 2021.
Declaration of Competing Interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgments
Funding: University of Canterbury Doctoral Scholarship Programme.
Biography

Ella F. S. Guy PhD Candidate at the University of Canterbury, Mechanical Engineering Department, Centre for Bioengineering.
References:
- 1.TSI. (2022). 4000 Series Analog and Digital Flow Meters. Available: https://tsi.com/products/flow-meters,-flow-sensors,-and-flow-analyzers/4000-series-analog-and-digital-flow-meters/.
- 2.Holder-Pearson L., Lerios T., Chase J.G. Physiologic-range three/two-way valve for respiratory circuits. HardwareX. 2021;10:e00234. doi: 10.1016/j.ohx.2021.e00234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.J. G. Chase, K. Moeller, G. M. Shaw, C. Schranz, Y. S. Chiew, and T. J. B. r. n. Desaive, “When the value of gold is zero,” vol. 7, no. 1, pp. 1-3, 2014. [DOI] [PMC free article] [PubMed]
- 4.Hutten G., Van Thuijl H., Van Bellegem A., Van Eykern L., Van Aalderen W. A literature review of the methodology of EMG recordings of the diaphragm. J. Electromyogr. Kinesiol. 2010;20(2):185–190. doi: 10.1016/j.jelekin.2009.02.008. [DOI] [PubMed] [Google Scholar]
- 5.Maisch S., et al. Determination of functional residual capacity by oxygen washin-washout: a validation study. Intensive Care Med. 2007;33(5):912–916. doi: 10.1007/s00134-007-0578-2. [DOI] [PubMed] [Google Scholar]
- 6.Laufer B., Krueger-Ziolek S., Docherty P.D., Hoeflinger F., Reindl L., Moeller K. 2019 41st Annual International Conference of the IEEE EngIneerIng In MedicIne and Biology Society (EMBC) 2019. Tidal volume via circumferences of the upper body: a pilot study; pp. 3559–3562. [DOI] [PubMed] [Google Scholar]
- 7.Laufer B., et al. A Minimal Set of Sensors in a Smart-Shirt to Obtain Respiratory Parameters. IFAC-PapersOnLine. 2020;53(2):16293–16298. [Google Scholar]
- 8.Boudewyns A., Willemen M., Wagemans M., De Cock W., Van de Heyning P., De Backer W.J.S. Assessment of respiratory effort by means of strain gauges and esophageal pressure swings: a comparative study. Sleep. 1997;20(2):168–170. doi: 10.1093/sleep/20.2.168. [DOI] [PubMed] [Google Scholar]
- 9.Shafiq G., Veluvolu K.C. Multimodal chest surface motion data for respiratory and cardiovascular monitoring applications. Sci. Data. 2017;4(1):1–12. doi: 10.1038/sdata.2017.52. [DOI] [PMC free article] [PubMed] [Google Scholar]