

Abstract
Background:
This article reports on a test of a youth substance use prevention program conducted in Nogales-Sonora, a Mexican city on the US border.
Objective:
The study tested the efficacy of a version of the keepin’ it REAL curriculum for middle school students that was culturally adapted for Mexico and renamed Mantente REAL.
Methods:
Students in 7th grade classrooms in four public schools participated in the study (N = 1,418, 49% female, mean age = 11.9). Using a clustered randomized design, two schools received the intervention and two served as a treatment-as-usual control group. Regular classroom teachers were trained to deliver the twelve-lesson Mantente REAL manualized curriculum. Parents provided active consent and students gave written assent to collect pretest and posttest questionnaire data, 7 months apart, at the beginning and end of the 2017-2018 academic year. We assessed the Mantente REAL intervention with general linear models adjusted for baseline, attrition, non-linear distributions, and school-level clustering.
Results:
Students who participated in Mantente REAL reported relatively less frequent use of alcohol and illicit drugs other than marijuana, compared to students in control schools. Males alone reported desirable intervention effects for marijuana use. These desirable effects were especially strong among students who reported higher initial levels of involvement in risky behaviors. Among students more at risk, both females and males receiving the program reported relative reductions in the frequency of use of alcohol and illicit drugs.
Conclusions:
These promising results within the Mexico-US border context support a further dissemination of the intervention and additional youth prevention research in the region.
Keywords: Substance use, prevention, youth, Mexico, Border, cultural adaptation
Alcohol use, binge drinking, and illegal drug use are increasing among Mexican adolescents of both sexes, and the gender gap in use is narrowing or disappearing (ENCODAT, 2017a, 2017b). Male and female Mexican students in 5th to 12th grade report converging rates of lifetime alcohol use (males 54%, females 52.5%), excessive alcohol use (males 15.7%, females 13.3%), and no significant gender differences in the average age for initiating alcohol (12.6 years) or illicit drug (13.0 years) use (Villatoro Velázquez et al., 2016). Marijuana (10.6%) is the most widely used illicit drug in both sexes, followed by inhalants (5.8%) and cocaine (3.3%).
Substance use, violence and prevention in border communities
Sonora, the current study site, and other northern Mexican border states are areas of heightened vulnerability for substance use and antisocial behaviors, witnessing sharply increasing use of illegal drugs, mainly marijuana, cocaine, and amphetamines (INPRFM, 2017a). Alcohol use and binge drinking among adolescents (12–17 years) are more prevalent and growing faster in Sonora’s region than nation-wide (ENCODAT, 2017a, 2017b). Sonora’s residents report high rates of antisocial and criminal activities around their homes: alcohol use in the street (70.3%), illegal drug use (66.3%), robberies and assaults (51.6%), and drug selling (47.7%) (INEGI, 2018). Their region receives national and international attention due to violence linked to organized crime and drug trafficking (Buchanan, 2011; UNODC, 2010). Sonora ranks third among Mexican states in drug trafficking offenses and second in trafficking convictions (Piña Osuna & Poom Medina, 2019). Youth on the US-Mexico border are targeted increasingly by drug traffickers, as potential consumers and for drug smuggling (DEA, 2017; Puyana et al., 2017; United Nations, 2018). Mexican youth play a significant role in drug trafficking: 3.5% of high school students report dealing hard drugs other than marijuana (Vilalta & Martinez, 2012).
Nogales, on Sonora’s border with the US, is one of 14 identified Mexican cities in urgent need of drug prevention and treatment services due to macro-social risk factors like poverty and drug trafficking that contribute to substance use (García Aurrecoechea et al., 2016). Mexican educational authorities recommend the implementation of evidence-based prevention programs to reduce risks facing students due to violence, threats, extortion, guns, and substance use around schools (SEP, 2012a). However, most students in Mexico do not have access to these programs (Castro et al., 2015; CONADIC, 2008; Secretaría de Salud, n.d.; Vargas Contreras et al., 2016), particularly in northern Mexico (CONADIC, 2003; Villatoro Velázquez et al., 2016). Moreover, to date the substance use prevention programs for youth that have sometimes been implemented in northern Mexico, such as Chimalli-Integral Family Development, Centers of Youth Integration (CIJ), and Ambar Interactive Centers, lack evidence of efficacy (Castro et al., 2015; CIJ, 2019; CONADIC, 2003; CONEVAL, 2013, 2015; SEP, 2012b). Efforts to culturally adapt, implement, and evaluate evidence-based prevention programs in Mexico, employing efficacious programs from elsewhere, are one way to address this unmet need. The culturally adapted version of the keepin’ it REAL curriculum for Mexico is a program proven effective in many settings that has now been adapted to the contexts surrounding substance use among Mexican youth (Marsiglia et al., 2019).
Keepin’ it REAL/Mantente REAL
Mantente REAL is the Spanish language version of keepin’ it REAL (kiREAL), a manualized universal prevention intervention that was originally developed and tested in the US with a predominantly Latino youth sample (Marsiglia & Hecht, 2005). The curriculum integrates ecological risk and resiliency theory, communication competence theory, and narrative theory to teach skills for resisting risky behaviors (Gosin et al., 2003). The program aims to delay or reduce substance use among early adolescents by increasing their use of culturally congruent drug resistance skills and by promoting non-permissive substance use norms and attitudes. The REAL acronym—Refuse, Explain, Avoid, Leave—represents the drug resistance strategies most often used by youth who do not use substances: refuse substance offers with a direct no, explain why you decline, avoid substance offer situations, or leave them.
Randomized controlled trials demonstrate that kiREAL delays adolescent substance use initiation (Hecht et al., 2003) and reduces substance use among those who have initiated it (Kulis et al., 2007). Evidence of the effectiveness of kiREAL with Latino heritage youth is considerable, including Mexican American youth in the US (Kulis et al., 2005) and in Guatemala (Kulis et al., 2019), Uruguay (Marsiglia et al., 2018), and Guadalajara, Mexico (Marsiglia et al., 2014, 2015). The current study tests a culturally adapted version of kiREAL for Mexico that recognizes violence, intimidation and gender differences in how these youth contend with substance use offers. The adaptation process included a feasibility trial of the original kiREAL, translated into Mexican Spanish, in Mexico’s three largest cities, a concurrent process evaluation, a year-long curriculum adaptation effort integrally involving Mexican research partners, a pilot test of the initial adaptation with subsequent refinements, and new curriculum videos produced in Mexican cities (see Marsiglia et al., 2019 for details). This adapted version for Mexico, renamed Mantente REAL (MREAL), has 12 weekly lessons that middle school teachers deliver in regular classes.
This study reports on the efficacy of MREAL in a northern Mexican border city, one experiencing growing levels of drug-related violence and substance use. The study aims were to implement the MREAL curriculum in middle schools and assess its efficacy in a field trial with a cluster randomized design. The study hypothesized that the early adolescents exposed to MREAL would report relatively less alcohol, tobacco, and other drug use compared to a treatment-as-usual control group. A second aim was to test the risk moderation hypothesis that the efficacy of MREAL would be greatest for students with more prior engagement in risk behaviors like substance use, violence, and other anti-social behaviors. Third, the study tested whether there were gender differences in efficacy.
Methods
The study was conducted in 2017–2018 in Nogales, Sonora through collaboration by researchers from El Colegio de la Frontera Norte (COLEF) and Arizona State University (ASU), and with the cooperation and support of system administrators, principals, and teachers.
Sample and participants
Figure 1 provides a CONSORT diagram describing the selection of schools and flow of participants. Nogales public middle schools have three classifications: technical (n = 5), state (n = 2), and national/general (n = 4). All four national/general middle schools (secundarias generales) were invited, and agreed, to participate in the study. The rationale for selection was that these schools broadly represented the socioeconomic profile of Nogales neighborhoods (low income), covered different geographical areas of the city, and operated under the same administrative system. Using random numbers, two schools were randomly assigned to receive MREAL and the other two served as a treatment-as-usual control group. The student participants were in the first year of middle school (secundaria), the equivalent of 7th grade in the US.
Figure 1.
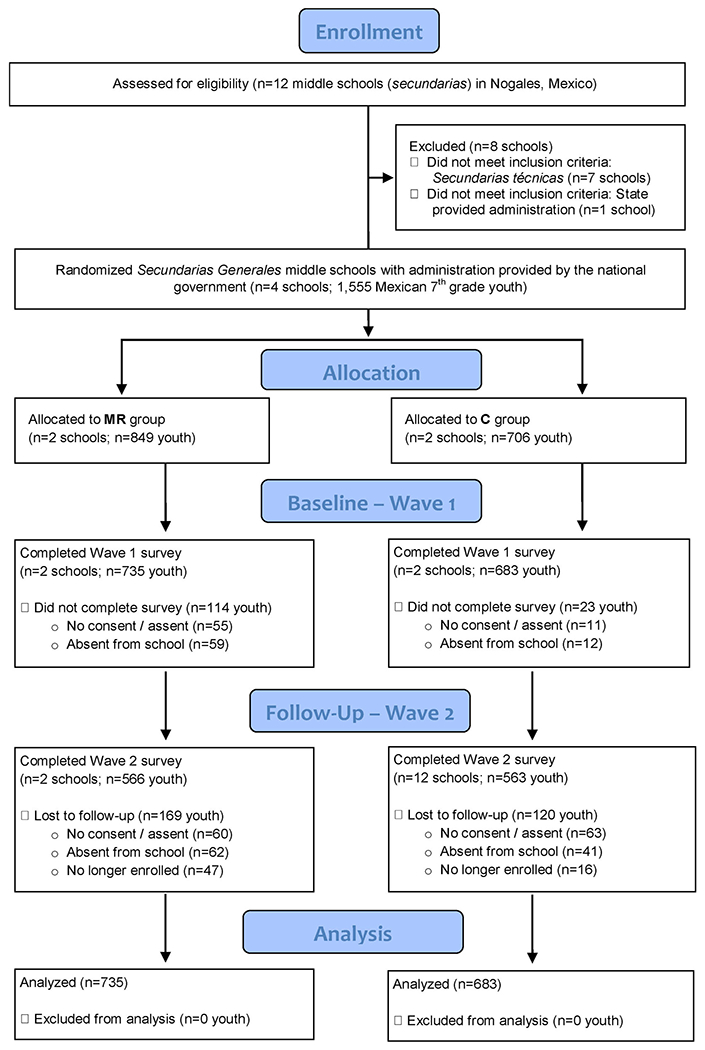
Participants in the Mantente REAL efficacy trial in Nogales, Mexico.
Curriculum training and delivery
Forty-seven classrooms participated in the study (26 MREAL and 21 controls). All 7th grade classrooms in intervention schools received the MREAL curriculum. Classroom sizes ranged from 20 to over 40 students. Assisted by COLEF researchers, a bilingual team from ASU trained 17 teachers to deliver the MREAL curriculum with fidelity. The two-day training allowed teachers to become familiar with the curriculum, understand the underlying pedagogy, and practice each lesson interactively. Teachers began delivering the curriculum in November 2017 and aimed to complete one lesson per week. Some lessons required multiple days to give extra time for students in large classes to participate in the interactive activities. With breaks for holidays, teachers completed delivery of MREAL by April 2018. Observers from the research team rated each teacher’s degree of fidelity to two core lessons that taught the REAL strategies, noting adherence to the curriculum (e.g. “How closely did the teacher follow the instructions?”) and competence (e.g. “Was the teacher prepared?”). Teachers in control schools continued with any regular instruction on alcohol and drug use that was a normal part of the curriculum in health, civics or ethics classes.
Consents, survey administration, and data entry
School authorities informed parents in writing about the study goals and parents signed an informed consent giving permission for their children to participate in data collection. Students with parental consent in all four schools completed a pretest questionnaire in October 2017 and a posttest seven months later, after intervention schools finished delivery of the program. The Mexican research team administered the questionnaires without teachers being present. Proctors informed students that their answers would remain confidential, and students provided written assent to participate. The ethical research review committees of both COLEF and ASU approved the data collection procedures.
The Mexican research team entered all questionnaire data and shared an individually de-identified dataset with the ASU research team for analysis. Surveys were collected from 1,418 participants at pretest and 1,129 at posttest. After sorting on school and classroom identifiers, we linked 80% of individual pretests to a corresponding posttest using a combination of characteristics: gender, birthdate, birth order, and number of brothers and of sisters.
Measurements
Recent substance use
Students responded to identically phrased questions at pretest and posttest about their substance use in the last 30 days. They reported how many times they had “drunk more than a sip of alcohol,” “smoked cigarettes or tobacco,” “smoked marijuana,” “used other drugs like cocaine, heroin, methamphetamines, and piedra [crack],” and “used inhalants” (Graham et al., 1984). Responses on a Likert scale were: never (0), once (1), 2–3 times (2), 4–9 times (3), 10–19 times (4), 20–39 times (5), and 40 or more times (6). Three additional items assessed the amounts of last 30-day use: number of alcohol drinks, of tobacco cigarettes, and of marijuana “joints” (churros). Likert responses, scored from 0 to 6, were: none, part of one, one whole, 2–3, 4–9, 10–19, and 20 or more.
Intervention condition
Students in schools that implemented MREAL were coded 1; those in non-implementing schools were coded 0.
Risk behavior profile
To test the risk moderation hypothesis that students at higher initial risk of substance use would show stronger desired intervention effects than those at lower risk, we created a composite risk behavior profile by calculating the mean of 16 items (see the Appendix). They included a range of behaviors, such as lifetime substance use (separate items for alcohol, cigarettes, marijuana, inhalants, other illicit drugs) (Graham et al., 1984), engaging in criminal violence and bullying (Nadel et al., 1996), and other risk behaviors like cheating on exams, doing dangerous things on a dare, and school suspension (Achenbach, 2009). The composite risk profile also included multi-item scales: exposure to substance offers and access to licit and illicit substances (Hecht et al., 2003); associations with substance-using friends and peers (Hansen & Graham, 1991); antisocial peer influences (Luengo et al., 1999); and permissive norms and attitudes toward substance use, such as viewing it as harmless or beneficial (Hansen & Graham, 1991). Because the items had different response categories and ranges, we standardized them with z-score transformations before combining into a mean score.
Covariates
All analyses of intervention effects controlled for a set of demographic and educational variables, measured at pretest. These included the student’s gender (dichotomous, female = 0, male = 1), age (in years), household size (number of people now at home), and whether the student lived with both parents (no = 0, yes = 1). Students reported length of residence in Nogales, from less than a year (1) to all their life (6). Parental education was the highest level attained by the student’s mother and/or father, from no education (1), to education beyond high school (8). The student’s educational aspirations (expected terminal degree) were measured on a Likert scale, from not completing middle school (1), to competing a master’s degree or higher (6).
Plan of analyses
We first assessed the psychometric properties of the substance use outcomes, and tested for baseline (pretest) differences between the intervention and control groups. To assess the intervention effects, we tested a series of baseline adjusted linear regression models in Mplus 7.0 (Muthén & Muthén, 2012), controlling for the outcome as measured at pretest, and including controls for baseline differences and the overall risk profile score. Additional models tested the risk moderation hypothesis by adding the interaction between the risk profile score and intervention condition. All models adjusted for the nesting of data at the school level, specifying a unique school identifier in the Mplus “cluster” command to provide unbiased individual level estimates. Because the distributions of the substance use outcomes all had positive values for skewness (> 3.0), the models also employed a maximum likelihood estimator (MLR) that is robust to non-normal distributions. Models utilized full-information maximum likelihood (FIML) estimation to account for attrition to the posttest (20%), which ensured that all cases with pretests contributed to the estimates of intervention effects. We estimated models for the sample as a whole, for males and females separately, and in a model testing whether the differences in intervention effects by gender were statistically significant using gender moderation interactions.
Results
Participant characteristics
Table 1 presents a demographic profile of the respondents, for the whole sample and separately by intervention condition. To aid in interpreting some means in the table, we describe key features of the distributions (data not presented in tables). The gender composition was nearly balanced. Students were age typical for the start of 7th grade, with 93% aged 11 or 12. Most students (73%) lived with both parents, in households that averaged about four people. Most students resided in Nogales all their life (62%). The educational level of the students’ parents varied, with almost a third (32%) having only a middle school education or less, over a third (38%) starting or completing high school, and 30% attaining education beyond high school. The students’ educational aspirations were high: 45% expected to earn a technical or bachelor’s degree, and 43% expected a masters’ degree or beyond. Low means for all substance use outcomes, close to the minimum (0) indicating no use, reflect the low prevalence of last 30-day use of alcohol (14.6%), cigarettes (4.8%), marijuana (1.9%), other illicit drugs (0.6%), and inhalants (11.5%).
Table 1.
Demographic characteristics of participants, and outcomes at pretest, by intervention condition.
| Mantente REAL (n = 737) | Control group (n = 680) | Total (N = 1418) | Difference test: Mantente REAL versus control | |
|---|---|---|---|---|
| Gender | ||||
| Female | 48.7% | 49.7% | 49.2% | X2 = 0.1, 1 df, p = 0.710 |
| Male | 51.3% | 50.3% | 50.8% | |
| Living arrangement | ||||
| Both Parents | 68.6% | 78.0% | 73.1% | X2 = 22.2, 2 df, p = 0.001 |
| Single Parent | 28.4% | 21.4% | 25.0% | |
| Other Relative | 3.0% | 0.6% | 1.9% | |
| Age (Mean) | (11.96) | (11.89) | (11.93) | t = 2.60, p = 0.009 |
| Household size (Mean) | (3.86) | (4.01) | (3.95) | t = 2.99, p = 0.003 |
| Years of residence in Nogales (Mean) | (5.01) | (5.17) | (5.08) | t = 2.16, p = 0.036a |
| Parental education (Mean) | (6.15) | (6.43) | (6.28) | t = 2.16, p = 0.005a |
| Educational aspirations (Mean) | (4.74) | (5.00) | (4.87) | t = 3.67, p = 0.001a |
| Risk behavior profile (Mean) | (0.05) | (−0.06) | (0.00) | t = 4.48, p = 0.001 |
| Alcohol frequency (Mean) | (0.22) | (0.17) | (0.19) | t = 1.52, p = 0.129 |
| Alcohol amount (Mean) | (0.25) | (0.17) | (0.21) | t = 2.26, p = 0.024a |
| Cigarette frequency (Mean) | (0.18) | (0.07) | (0.09) | t = 3.46, p = 0.001a |
| Cigarette amount (Mean) | (0.14) | (0.04) | (0.04) | t = 3.62, p = 0.001a |
| Marijuana frequency (Mean) | (0.05) | (0.02) | (0.04) | t = 1.50, p = 0.134 |
| Marijuana amount (Mean) | (0.06) | (0.01) | (0.00) | t = 2.16, p = 0.015a |
| Other illicit drug freq. (Mean) | (0.02) | (0.00) | (0.01) | t = 1.58, p = 0.113 |
| Inhalants frequency (Mean) | (0.23) | (0.23) | (0.23) | t = 0.09, p = 0.925 |
Note: t-tests assume non-equal variance across intervention and control groups.
Non-parametric (Mann-Whitney) tests showed significant differences between intervention and control groups when treating these variables as ordinal rather than interval measures, as the t-tests assumed.
Baseline differences and adjustments
Tests of baseline differences between the MREAL and control groups appear in the last column of Table 1. It reports Chi-square tests for nominal variables and t-tests of mean differences for remaining variables. For variables measured on ordinal scales we also conducted non-parametric tests (Mann-Whitney) to verify t-test results. Although there were no significant differences by gender, the MREAL group was less likely than the control group to live with both parents, lived in smaller households, had parents with less education, and had lived for less of their lives in Nogales. MREAL students were also slightly older than controls, had lower educational aspirations, and higher risk behavior profile scores. Together these covariates suggested there were common underlying differences between the MREAL and control groups at pretest, with MREAL students more “at risk” for substance use on multiple indicators. Accordingly, these covariates were included as controls in tests of intervention effects. The MREAL group reported small but significantly higher means on pretest measures of amounts of recent alcohol, cigarette and marijuana use, and higher frequency of cigarette use, but there were no significant differences in the frequency of use of alcohol, marijuana, other illicit drugs, or inhalants.
Tests of intervention effects
Tables 2 and 3 report the intervention effects on recent substance use, as reported at posttest. Four models are tested for each outcome: total sample, females only, males only, and a test of significant gender differences. The first predictor (DV at T1) serves as a control for use of the same substance at pretest, making the model a prediction of change from pretest to posttest. The next predictors are demographic controls for baseline differences, the risk behavior profile score, the intervention condition dummy variable, and the interaction term for intervention condition by risk behavior profile. The fourth model adds two interaction terms to test whether there are significant gender differences in the overall intervention effect or in the risk moderated intervention effect.
Table 2.
Short-term effects of MREAL on recent alcohol and cigarette use, for total sample and by gender (N = 1,418, 692 female, 719 male).
| Alcohol frequency |
Alcohol amount |
Cigarette frequency |
Cigarette amount |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Female | Male | Total | Total | Female | Male | Total | Total | Female | Male | Total | Total | Female | Male | Total | |
| Intercept | 0.883* | 0.969 | 0.813 | 0.889* | 0.190 | −0.253 | 0.778 | 0.196 | −0.602 | 0.102 | −1.588 | −0.589 | −0.500 | 0.472 | −1.933 | −0.496 |
| 0.438 | 0.667 | 0.937 | 0.444 | 0.397 | 0.586 | 0.917 | 0.377 | 0.966 | 0.624 | 2.360 | 0.953 | 0.416 | 0.768 | 1.906 | 0.436 | |
| DV at T1 | 0.279** | 0.374*** | 0.213 | 0.281** | 0.32* | 0.39*** | 0.268 | 0.319* | 0.477*** | 0.606*** | 0.384*** | 0.478*** | 0.528*** | 0.327* | 0.733*** | 0.528*** |
| 0.100 | 0.091 | 0.169 | 0.099 | 0.145 | 0.071 | 0.234 | 0.147 | 0.024 | 0.058 | 0.063 | 0.017 | 0.091 | 0.141 | 0.113 | 0.093 | |
| Age | −0.038 | −0.086 | −0.009 | −0.039 | 0.008 | −0.005 | 0.000 | 0.005 | 0.097 | 0.019 | 0.185 | 0.096 | 0.069* | −0.012 | 0.184 | 0.068* |
| 0.030 | 0.055 | 0.058 | 0.030 | 0.041 | 0.057 | 0.074 | 0.037 | 0.084 | 0.055 | 0.198 | 0.084 | 0.032 | 0.071 | 0.158 | 0.032 | |
| Years in Nogales | −0.006 | 0.010 | −0.018 | −0.004 | −0.003 | 0.029 | −0.04* | −0.001 | −0.016 | −0.024† | 0.003 | −0.014 | 0.003 | 0.000 | 0.007 | 0.003 |
| 0.009 | 0.020 | 0.020 | 0.009 | 0.021 | 0.033 | 0.018 | 0.021 | 0.016 | 0.013 | 0.016 | 0.014 | 0.012 | 0.011 | 0.020 | 0.012 | |
| Two parents | −0.010 | −0.082 | 0.056† | −0.006 | 0.112** | 0.084† | 0.097 | 0.112** | −0.049 | −0.097 | 0.017 | −0.043 | −0.019 | −0.022 | −0.041 | −0.022 |
| 0.034 | 0.053 | 0.032 | 0.035 | 0.039 | 0.045 | 0.112 | 0.036 | 0.093 | 0.081 | 0.101 | 0.094 | 0.081 | 0.071 | 0.104 | 0.083 | |
| Household size | −0.030 | −0.002 | −0.044 | −0.031 | −0.013 | 0.025 | −0.028 | −0.014 | 0.010 | 0.023 | −0.005 | 0.009 | −0.001 | −0.025 | 0.032 | 0.000 |
| 0.033 | 0.021 | 0.040 | 0.033 | 0.019 | 0.020 | 0.021 | 0.019 | 0.017 | 0.025 | 0.033 | 0.016 | 0.028 | 0.026 | 0.031 | 0.028 | |
| Parental education | 0.008 | 0.027*** | −0.003 | 0.008 | 0.005 | 0.009 | 0.003 | 0.005 | −0.020*** | −0.020 | −0.016 | −0.020*** | −0.022* | −0.019* | −0.021 | −0.023* |
| 0.008 | 0.005 | 0.009 | 0.008 | 0.009 | 0.009 | 0.020 | 0.010 | 0.005 | 0.017 | 0.018 | 0.004 | 0.011 | 0.006 | 0.014 | 0.011 | |
| Educational aspirations | 0.006 | 0.044*** | −0.032* | 0.005 | 0.008 | 0.055* | −0.032 | 0.007 | −0.011 | 0.035* | −0.054 | −0.013 | 0.001 | 0.021 | −0.017 | 0.002 |
| 0.007 | 0.005 | 0.015 | 0.006 | 0.020 | 0.022 | 0.027 | 0.020 | 0.014 | 0.017 | 0.035 | 0.015 | 0.016 | 0.024 | 0.035 | 0.016 | |
| Risk profile | 0.648*** | 0.658*** | 0.631* | 0.646*** | 0.914** | 1.001* | 0.796*** | 0.906*** | 0.551** | 0.516 | 0.587*** | 0.552** | 0.324 | 0.587 | 0.200* | 0.320 |
| 0.144 | 0.109 | 0.283 | 0.145 | 0.133 | 0.504 | 0.224 | 0.135 | 0.162 | 0.436 | 0.078 | 0.165 | 0.225 | 0.501 | 0.082 | 0.229 | |
| Gender: F = 0, M = 1 | −0.060 | −0.052 | −0.024 | 0.039* | −0.033 | −0.046 | −0.018 | 0.010 | ||||||||
| 0.061 | 0.062 | 0.071 | 0.015 | 0.047 | 0.072 | 0.030 | 0.024 | |||||||||
| MREAL v. control | −0.037* | −0.002 | −0.048 | −0.027 | 0.002 | 0.086 | −0.077 | 0.071 | 0.034 | 0.032 | 0.046 | 0.023 | 0.016 | 0.043 | −0.027 | 0.044 |
| 0.017 | 0.032 | 0.070 | 0.049 | 0.070 | 0.091 | 0.115 | 0.057 | 0.054 | 0.089 | 0.066 | 0.076 | 0.072 | 0.092 | 0.078 | 0.076 | |
| MREAL v. control X risk profile | −0.383*** | −0.326*** | −0.437* | −0.269** | −0.467** | −0.473 | −0.414*** | −0.347† | −0.028 | 0.043 | −0.150 | 0.111 | −0.142 | −0.272 | −0.167 | −0.183 |
| 0.605 | 0.062 | 0.174 | 0.092 | 0.674 | 0.471 | 0.070 | 0.182 | 0.649 | 0.426 | 0.238 | 0.155 | 0.521 | 0.579 | 0.124 | 0.318 | |
| MREAL v. Control X gender | −0.015 | −0.134 | 0.028 | −0.060 | ||||||||||||
| 0.130 | 0.131 | 0.102 | 0.041 | |||||||||||||
| MREAL v. Control X risk profile X gender | −0.215*** | −0.203** | −0.271 | 0.086 | ||||||||||||
| 0.034 | 0.064 | 0.220 | 0.097 | |||||||||||||
| R square | 0.131 | 0.183 | 0.099 | 0.131 | 0.209 | 0.327 | 0.136 | 0.208 | 0.275 | 0.327 | 0.237 | 0.273 | 0.204 | 0.160 | 0.302 | 0.206 |
| Cohen’s d | 0.064 | 0.119 | 0.152 | 0.072 | ||||||||||||
Notes: Unstandardized estimates with standard errors in italics. Cohen’s d effect sizes are for the main intervention effect.
p < 0.10;
p < 0.05;
p < 0.01;
p < 0.001.
Table 3.
Short-term effects of MREAL on Marijuana, other illicit drugs and inhalants, for total sample and by gender (N = 1,418, 692 female, 719 male).
| Marijuana frequency |
Marijuana amount |
Other illicit drug frequency |
Inhalants frequency |
|||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | Female | Male | Total | Total | Female | Male | Total | Total | Female | Male | Total | Total | Female | Male | Total | |
| Intercept | −0.144 | −0.643* | 0.497 | −0.136 | −0.428 | −0.392 | −0.502 | −0.427 | 0.104 | 0.080 | 0.172 | 0.104 | 0.446 | 0.521 | 0.477 | 0.449 |
| 0.333 | 0.314 | 0.809 | 0.343 | 0.344 | 0.284 | 0.815 | 0.338 | 0.083 | 0.104 | 0.141 | 0.086 | 0.795 | 0.649 | 1.591 | 0.789 | |
| DV at T1 | 0.410 | 1.211*** | 0.086 | 0.439 | 0.398*** | 0.441*** | 0.345** | 0.389*** | 0.282 | −0.183*** | 0.313** | 0.271 | 0.286*** | 0.308*** | 0.278*** | 0.291*** |
| 0.331 | 0.332 | 0.094 | 0.275 | 0.034 | 0.082 | 0.102 | 0.033 | 0.173 | 0.051 | 0.105 | 0.184 | 0.029 | 0.066 | 0.076 | 0.034 | |
| Age | 0.030 | 0.057† | −0.013 | 0.027 | 0.039 | 0.027† | 0.051 | 0.038 | −0.002 | −0.006 | −0.001 | −0.003 | −0.003 | −0.048 | 0.029 | −0.006 |
| 0.031 | 0.032 | 0.050 | 0.031 | 0.027 | 0.015 | 0.063 | 0.026 | 0.004 | 0.009 | 0.007 | 0.004 | 0.061 | 0.052 | 0.118 | 0.060 | |
| Years in Nogales | −0.004 | −0.007 | −0.002 | −0.001 | 0.010*** | 0.005 | 0.018*** | 0.012*** | 0.001 | 0.005* | −0.002 | 0.002 | −0.025 | −0.008 | −0.039 | −0.022 |
| 0.008 | 0.010 | 0.009 | 0.007 | 0.002 | 0.004 | 0.004 | 0.002 | 0.002 | 0.002 | 0.002 | 0.002 | 0.029 | 0.010 | 0.068 | 0.030 | |
| Two parents | −0.045*** | −0.039 | −0.024 | −0.042*** | −0.048* | −0.050* | −0.049 | −0.048* | −0.009 | −0.018 | −0.002 | −0.009 | −0.004 | 0.048 | −0.071 | −0.003 |
| 0.006 | 0.028 | 0.025 | 0.008 | 0.019 | 0.022 | 0.033 | 0.020 | 0.007 | 0.012 | 0.017 | 0.007 | 0.104 | 0.174 | 0.113 | 0.102 | |
| Household size | 0.040 | 0.070** | 0.009 | 0.038* | 0.030 | 0.031 | 0.026 | 0.030 | −0.001 | −0.002 | 0.000 | −0.001 | 0.002 | −0.038 | 0.031† | 0.001 |
| 0.018 | 0.025 | 0.015 | 0.017 | 0.024 | 0.026 | 0.039 | 0.024 | 0.004 | 0.002 | 0.006 | 0.004 | 0.025 | 0.041 | 0.018 | 0.024 | |
| Parental education | −0.030*** | −0.019* | −0.035 | −0.030*** | −0.010 | 0.005 | −0.021 | −0.009 | −0.007* | −0.005* | −0.008* | −0.007* | 0.013 | 0.021 | 0.007 | 0.013 |
| 0.008 | 0.008 | 0.022 | 0.007 | 0.009 | 0.004 | 0.015 | 0.009 | 0.003 | 0.002 | 0.003 | 0.003 | 0.012 | 0.018 | 0.012 | 0.012 | |
| Educational aspirations | 0.003 | −0.002 | 0.004 | 0.001 | −0.008 | −0.004 | −0.012 | −0.009 | −0.001 | 0.006† | −0.011 | −0.002 | −0.019 | 0.057*** | −0.095 | −0.021 |
| 0.020 | 0.021 | 0.022 | 0.020 | 0.017 | 0.012 | 0.026 | 0.017 | 0.006 | 0.003 | 0.012 | 0.006 | 0.034 | 0.012 | 0.065 | 0.034 | |
| Risk profile | 0.476* | 0.474 | 0.471*** | 0.465* | 0.223* | 0.222 | 0.213*** | 0.219* | 0.047*** | −0.014 | 0.088 | 0.045*** | 0.388** | 0.328*** | 0.379 | 0.373** |
| 0.200 | 0.470 | 0.076 | 0.201 | 0.105 | 0.251 | 0.014 | 0.107 | 0.009 | 0.014 | 0.012 | 0.008 | 0.129 | 0.021 | 0.229 | 0.131 | |
| Gender: F = 0, M = 1 | −0.024 | 0.018 | −0.014 | 0.019 | 0.007 | 0.021 | −0.043 | 0.024 | ||||||||
| 0.036 | 0.039 | 0.026 | 0.017 | 0.009 | 0.015 | 0.068 | 0.040 | |||||||||
| MREAL v. control | −0.023 | 0.005 | −0.061† | 0.024 | −0.022 | 0.018 | −0.059*** | 0.014 | −0.024** | 0.001 | −0.041* | −0.009*** | −0.030 | 0.069 | −0.127† | 0.043 |
| 0.041 | 0.083 | 0.035 | 0.057 | 0.030 | 0.051 | 0.017 | 0.044 | 0.008 | 0.003 | 0.018 | 0.002 | 0.060 | 0.066 | 0.071 | 0.094 | |
| MREAL v. control X risk profile | −0.177 | −0.242 | −0.356 | −0.007 | −0.152 | −0.090 | −0.196*** | −0.072 | −0.022*** | 0.089** | −0.088*** | 0.006 | −0.262 | −0.009 | −0.425† | −0.097 |
| 0.203 | 0.503 | 0.210 | 0.208 | 0.130 | 0.275 | 0.055 | 0.147 | 0.024 | 0.029 | 0.019 | 0.014 | 0.796 | 0.125 | 0.220 | 0.192 | |
| MREAL v. control X gender | −0.089* | −0.070** | −0.029* | −0.141 | ||||||||||||
| 0.039 | 0.026 | 0.015 | 0.107 | |||||||||||||
| MREAL v. control X risk profile X gender | −0.320*** | −0.135 | −0.048 | −0.287*** | ||||||||||||
| 0.029 | 0.132 | 0.030 | 0.056 | |||||||||||||
| R square | 0.278 | 0.569 | 0.168 | 0.285 | 0.219 | 0.303 | 0.155 | 0.216 | 0.142 | 0.067 | 0.193 | 0.131 | 0.096 | 0.126 | 0.101 | 0.100 |
| 0.026 | 0.032 | 0.058 | 0.036 | |||||||||||||
Notes: Unstandardized estimates with standard errors in italics. Cohen’s d effect sizes are for the main intervention effect.
p < 0.10;
p < 0.05;
p < 0.01;
p < 0.001.
There were significant overall intervention effects in the total sample (MREAL v. control) for the frequency of alcohol (b = −0.037, p = 0.031) and other illicit drug use (b = −0.024, p = 0.002), indicating that MREAL students had smaller increases from pretest to posttest than control students; these effects were largely attributable to males. Among males alone there was a significant desired overall intervention effect on use of marijuana (both measures), illicit drugs, and inhalants. Assessing the risk moderation hypothesis, results for the next predictor indicate that desirable MREAL effects were stronger among students with higher risk behavior scores at pretest for alcohol frequency (b = −0.383, p = 0.001), alcohol amounts (b = −0.467, p = 0.006), and other illicit drug use (b = −0.022, p = 0.001). The added gender interaction terms in the fourth model test for significant gender differences in intervention effects overall, and in intervention effects moderated by the level of the risk behavior profile score. Where there were significant gender differences, they pointed consistently to stronger desired intervention effects among males. Overall effects of MREAL were stronger for males than females on measures of marijuana frequency (b = −0.089, p = 0.023) and amounts (b = −0.070, p = 0.008), and other illicit drug use (b = −0.029, p = 0.049). The risk moderated intervention effect was significantly stronger for males than for females for alcohol frequency (b = −0.215, p = 0.001) and amounts (b = −0.203, p = 0.001), marijuana frequency (b = −0.320, p = 0.001) and use of inhalants (b = −0.037, p = 0.031). In a single instance, illicit drug use, the risk moderated intervention effect was significant for both males and females in separate models, and not statistically distinguishable in the gender interaction test (b = −0.048, p = 0.109).
Figure 2 depicts the nature of the risk moderated intervention effects, separately by gender, for alcohol frequency. Among students with a low risk behavior score at pretest, their predicted alcohol frequency at post-test did not differ notably for MREAL and control students, both female and male. But among students at moderate and high levels of risk (separated at one standard deviation intervals on the risk behavior profile measure), sharper differences emerged between the MREAL and control groups. Predicted growth in alcohol use increased at successively higher levels of the risk behavior score, but less steeply for MREAL than for control students, and with a wider gap for males than for females.
Figure 2.
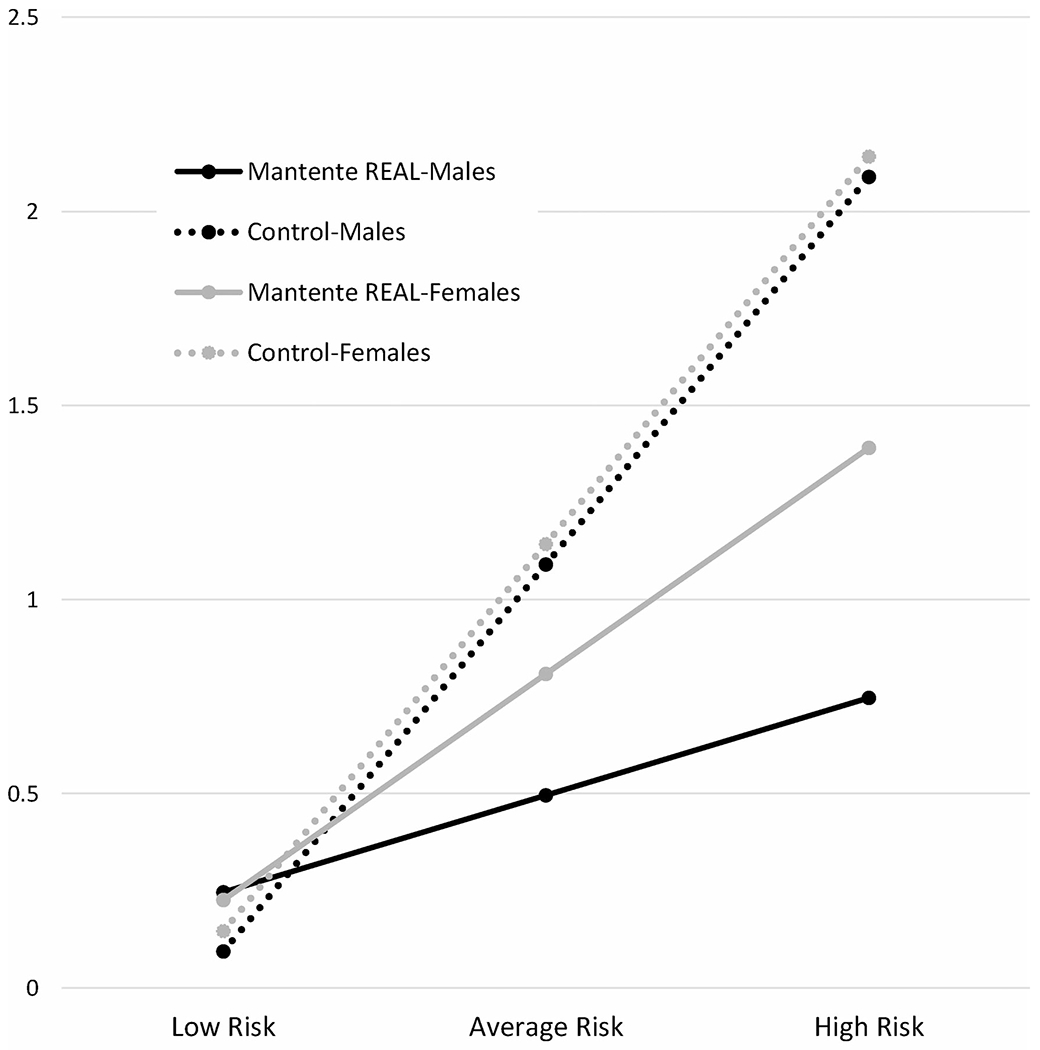
Posttest alcohol frequency by risk behavior score at pretest, intervention condition, and gender*.
*Predicted last 30 day alcohol frequency at post-test; risk level at pretest provided at 1 SD intervals.
The demographic predictors showed isolated effects for age: older students reported more growth in cigarette amounts (an effect driven by males), and older female students reported more growth in marijuana use. Students residing longer in Nogales reported less growth in alcohol amounts (males only) and cigarette frequency (females only), while also reporting more growth in marijuana use amounts (mostly males) and other illicit drug use (females only). Students in two-parent families reported larger increases in alcohol amounts but less growth in marijuana use (both measures). Household size was a significant predictor in two instances: those from larger households reported more marijuana use frequency (females only) and inhalant use (males only). Students with more extensively educated parents reported more growth in alcohol frequency (females only), but less growth in cigarette use frequency and amounts, and increasing frequency of marijuana and other illicit drug use. Among females, higher educational aspirations predicted greater use of alcohol (both measures), and frequency of cigarette, illicit drug, and inhalants use. Among males, higher educational aspirations predicted less frequent alcohol use. The overall risk behavior profile score generally predicted more growth in all types of substance use.
In considering the efficacy results, it is important to note that, although effects sizes (Cohen’s d) for the main effects of the intervention were small, less than 0.20, most were in the typical range for school-based substance use prevention programs (Tanner-Smith et al., 2018). Tables 2 and 3 involve multiple tests that are not adjusted for the possibility of familywise error or a false discovery rate (FDR). Applying the Benjamini and Hochberg (1995) adjustment for FDR, all of the estimates flagged at p < 0.05 would remain significant, with one exception: the main intervention effect for alcohol frequency in the total sample would miss the adjusted threshold for p by 0.019. There are substantive reasons and strong rationales for examining all of the substance use outcomes (Gottfredson et al., 2015): the intervention is designed specifically to prevent substance use, the most common types of substance use for this age group were included, and the outcomes were modestly inter-correlated. Most FDR corrections assume that the multiple tests are independent, and recommended alternatives like composite measures (Schochet, 2009) pose other drawbacks, such as ignoring differences across substances in the etiology of adolescent substance use and in the effectiveness of universal prevention approaches.
Discussion
This article tested the efficacy of MREAL, a culturally adapted version of keepin’ it REAL created for Mexico, among middle school students in Nogales, Mexico, and whether program efficacy differed by individual risk level and gender. MREAL showed several favorable signs of effectiveness in drug prevention. Students who participated in MREAL reported relatively less frequent use of alcohol and illicit drugs other than marijuana, compared to students in schools serving as a control group. These desirable effects were especially strong among students who reported higher initial levels of involvement in risky behaviors. There were both gender similarities and gender differences in the desirable prevention program effects. Among students more at risk, both females and males receiving the program reported relative reductions in the frequency of use of alcohol and illicit drugs. However, for alcohol frequency the program effects were significant and in the same direction for both genders but stronger for males than for females. Males alone reported desirable effects on marijuana and inhalants use, both overall and even more strongly when they were initially more extensively engaged in risk behaviors.
The findings are consistent with evidence that youth are increasingly vulnerable to marijuana and other illicit drug use in Mexican border states, including Sonora (INPRFM, 2017a). In this study, length of residence in Nogales was associated with increased risk of marijuana use. The concentration of many of the prevention effects of MREAL among middle school students already involved in risk behaviors, among those living longer in Nogales, and among males especially, can be interpreted within the current social, political, and economic context of Nogales. The city straddles a major international trucking route and border crossing and is a transit area for illegal drug trafficking and associated violence. It attracts migrants from throughout Mexico to work in low wage maquiladora jobs and has significant daily bi-directional flows of migrants across the US border, documented and undocumented. These macro-level factors exacerbate the substance use risks facing youth in Nogales and highlight the need for efficacious prevention programs. Effective prevention for youth already at relatively higher risk for substance use is important in slowing the progression to more problematic substance use, during later adolescence and early adulthood, which has lifelong and cumulative negative health effects.
The gendered patterns in the effectiveness of MREAL deserve further investigation. They may reflect gender differences at an early developmental period in ready access to licit versus illegal substances, with early and preadolescent males more exposed to the latter, as well as different sources of substance offers for females and males, such as family versus peers.
Another notable result was a non-finding: no significant effects of MREAL on tobacco use. This might reflect overall declining tobacco use rates in Mexico nationally, and in Sonora (INPRFM, 2017b). Results from the current study, however, confirmed that older adolescents and those from lower socio-economic status families (as measured by parental education), were more at risk of using tobacco.
The current study shines some light on other family factors. Students in two-parent families reported larger increases in alcohol amounts but less growth in marijuana use. While Mexican culture can be relatively permissive toward alcohol use by youth in family settings, family tolerance of illegal drug use is low (INPRFM, 2017a). Students with more educated parents reported significantly less of an increase in cigarette use, as well as in marijuana and other illicit drug use frequency, which is consistent with prior research (Andrabi et al., 2017).
Nonequivalence issues and adjustments
This small intervention trial encountered several unanticipated challenges in school selection that might influence the tests of program efficacy, such as variations in risk behavior profiles among the schools. We found that neighborhoods surrounding the selected schools included a mix of residents that was more variable in socioeconomic status than expected. This may be due to factors such as the lack of residential zoning regulations and urban planning, and the hilly topography of the city. In our study, parental education was lower overall among the students in the intervention schools compared to the control schools. Although we selected schools that operated under the same administrative system and with similar aggregate family income profiles in the education system’s reports, students reported unexpected differences in health risk behaviors across schools. Despite school-level randomization, these differences were not distributed equally across the intervention and control schools. Students in intervention schools had higher scores on our risk behavior profile measure. Although the models testing efficacy made statistical adjustments for individual risk behaviors, these may not have accounted for risk processes at the neighborhood and community levels.
A key decision in the study was how to adjust for differences among students in prior risk behaviors and associated vulnerability to substance use. This measure was crucial for conducting the tests of the risk moderation hypothesis. We explored various composite measures, such as counts of the number of past risk behaviors, dichotomous variables such as any risk behavior, and measures restricted to past substance use alone. In the end, we employed a multi-item measure that reflected a very broad range of risk behaviors, not just substance use, and one that preserved variations in degree of involvement in the risk behaviors. The prevalence of substance use was low, limiting the utility of a measure confined to experiences with substances. Relatively few of the youth in this sample had engaged in prior risk behaviors, and had done so usually in an infrequent manner. Our chosen measure enhanced the chance of registering some type of risk behavior, while also highlighting differences between the relatively few at high risk and those at very low or no risk. Thus, the results of the tests of risk moderation effects tend to emphasize the desirable program effects of MREAL on the minority of youth who, at this developmental stage, are beginning to engage in risky behaviors. Although there was some substantive overlap between the risk profile and post-test outcome measures (past versus recent substance use), the association was modest (r = 0.08 to r = 0.24).
Study limitations
There are limitations to consider in this study. First, the results cannot be generalized to the city of Nogales, to the state of Sonora, or other areas of Mexico. With only two schools in each condition, randomization alone did not prevent a lack of baseline equivalence between intervention and control group schools. The findings apply only to students attending school. As the differences in the number of students completing pretests and posttests suggest, some students left school during the trial. Schools face several issues associated with high residential mobility in the area (returnees, internal and international migrants) that affect school attendance, with variations across schools. For instance, approximately 18% of students were born outside of Nogales, 10% were American citizens and 2% were citizens of another country. Future studies need to follow-up with students who drop out of school or move away. Although our statistical models included adjustments for attrition, there could be unmeasured differences between those who stayed in their school and those who did not. Because the intervention showed the strongest effects with students at higher risk, attrition through the departure of at-risk students may actually have underestimated the program effects. The concentration of many desirable intervention effects on students already at relatively high risk of substance use might raise concerns that the results reflect regression to the mean, but any that might occur should apply equally to the MREAL and control groups. There is also a dosage concern connected to high levels of absenteeism common in border towns. We were unable to measure or control for individual student dosage to account for student absences from particular MREAL lessons. Future studies in northern Mexico border towns could benefit from a systematic integration of dosage into their models. Finally, as part of the randomized controlled design, MREAL teachers received special attention from the researchers through separate training and periodic contact with the research team to help them with any implementation challenges. These somewhat intensive interactions may have influenced their motivation and teaching effectiveness in ways that would not apply in a less controlled setting.
The distinctive contextual characteristics of Nogales as a border town may have played an important role in the results. The study lacked the contextual and migration-related measures that might document distinctive characteristics of the students, their families, schools, and neighborhoods that may shape responsiveness to the prevention program. Future studies on the border may benefit from a more detailed sociodemographic analysis of the school population and communities selected for sampling before conducting a stratified randomization.
Finally, there were important gender differences in the degree of efficacy of the intervention and its effects on different types of substance use. To ensure that both females and males benefit equally from the prevention program, an extensive gendered exploration of measures of substance use access, offers, and settings might be needed to understand the gender differences in program effects.
Conclusion
The promising study results justify further research on MREAL for Mexico. Although a larger scale trial is needed to verify findings, they suggest that students at highest risk benefit the most from the MREAL intervention. For youth on the Mexico’s northern border, the risks of using addictive substances can be reduced through participation in a culturally adapted prevention intervention for middle schools. This study shows that children, parents, teachers, and leaders of Mexican border cities need, respond to, and can successfully implement evidence-based substance use prevention programs.
Funding
National Institute on Drug Abuse.
Appendix: Variables included in the risk profile measure (pretest, before standardization)
| M | SD | Range, coding | Scale Items | Scale α | |
|---|---|---|---|---|---|
| Lifetime substance use frequency | |||||
| Alcohol | 0.58 | 1.03 | 0–6a | ||
| Cigarettes | 0.17 | 0.68 | 0–6a | ||
| Marijuana | 0.05 | 0.41 | 0–6a | ||
| Other hard drugs | 0.02 | 0.25 | 0–6a | ||
| Inhalants | 0.12 | 0.62 | 0–6a | ||
| Violence and risk behaviors | |||||
| Perpetrate criminal violence: attack another with knife, attack with pistol, threaten with knife, threaten with pistol, commit robbery | 0.09 | 0.41 | 0–4b | 5 | 0.89 |
| Perpetrate bullying: hit, beat, push, hurt, or verbally abuse another | 0.62 | 0.90 | 0–4b | 5 | 0.88 |
| Cheat on school exams | 0.20 | 0.62 | 0–4c | ||
| Do something dangerous on a dare | 0.47 | 0.92 | 0–4c | ||
| Suspended from school | 0.14 | 0.56 | 0–4c | ||
| Substance use exposure | |||||
| Access to substances: How easy to get alcohol, cigarettes, & marijuana | 1.72 | 0.86 | 1–4d | 3 | 0.87 |
| Substance offers: Frequency offered alcohol, cigarettes, marijuana, and other drugs in the past year Peer influence | 0.15 | 0.45 | 0–4e | 4 | 0.83 |
| Peer substance use: Proportion of school peers using alcohol, cigarettes, and marijuana | 1.37 | 1.15 | 0–5f | 3 | 0.91 |
| Friends’ substance use: Proportion of “best friends” using alcohol, cigarettes, and marijuana | 0.46 | 0.78 | 0–5f | 3 | 0.85 |
| Negative peer influence: would give in to peer pressure to smoke cigarettes, skip class, go out with friends instead of studying for exams, drink alcohol at a party, vandalize a library book, hang out with others who get in trouble (Yes/No) | 0.38 | 0.89 | 0–6g | 6 | NA |
| Pro-drug attitudes | |||||
| Positive substance use expectancies: substance use helps you deal with problems, relax, be happy, be creative, be part of a group, be less nervous, have fun at parties, know its effects | 1.72 | 0.81 | 1–4h | 8 | 0.93 |
Response categories:
Never/Once/2–3 times/4–9/10–19/20–39/40+ times.
Never/Once/Twice/3 times/4+ times.
Never/Once/2–3 times/4–9 times/10+ times.
Very difficult/Somewhat difficult/Somewhat easy/Very easy.
Never/Once/2–3 times/4–9 times/10+ times.
None/Almost none/Some/Half/Almost all/All.
Count of number of items responding yes.
Strongly disagree/Disagree/Agree/Strongly agree.
Footnotes
Declaration of interest
The authors declare that they have no conflict of interest. The authors alone are responsible for the content and writing of the article.
References
- Achenbach TM (2009). The Achenbach system of empirically based assessment (ASEBA): Development, findings, theory, and applications. University of Vermont Research Center for Children, Youth, & Families. [Google Scholar]
- Andrabi N, Khoddam R, & Leventhal AM (2017). Socioeconomic disparities in adolescent substance use: Role of enjoyable alternative substance-free activities. Social Science & Medicine (1982), 176, 175–182. 10.1016/j.socscimed.2016.12.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Benjamini Y, & Hochberg Y (1995). Controlling the false discovery rate: A practical and powerful approach to multiple testing. Journal of the Royal Statistical Society: series B (Methodological), 57(1), 289–300. [Google Scholar]
- Buchanan H (2011). Fleeing the drug war next door: Drug-related violence as a basis for refugee protection for Mexican asylum-seekers. Merkourios-Utrecht Journal of International & European Law, 27, 28. [Google Scholar]
- Castro ME, Llanes J, Amador Buenabad NG, Villatoro J, & Medina-Mora ME (2015). La preventión del consumo de drogas en México. In Pérez Gómez A, Mejía Trujillo J, & Becoña Iglesias E (Eds.), De la prevención y otras historias. Historia y evolución de la prevención del consumo del alcohol y drogas en América Latina y Europa (pp. 114–131). California-Edit. [Google Scholar]
- Centros de Integratión Juvenil A.C. (CIJ). (2019). Red de atención. Mexico City: CIJ. http://www.cij.org.mx/Contenidos/Red_Atencion/red_atencion.html [Google Scholar]
- Consejo Nacional Contra las Adicciones (CONADIC). (2003). Modelos preventivos. Mexico City: CONADIC. http://www.conadic.salud.gob.mx/pdfs/publicaciones/modprev.pdf [Google Scholar]
- Consejo Nacional Contra las Adicciones (CONADIC). (2008). Modelo de Atención UNEME–CAPA, Centros de Atención Primaria en Adicciones “Nueva Vida”. Mexico City: CONEVAL. http://www.conadic.salud.gob.mx/pdfs/publicaciones/UNEME_CAPA.pdf [Google Scholar]
- Consejo Nacional de Evaluación de la Política de Desarrollo (CONEVAL). (2013). Programa de Escuela Segura. Mexico City: CONEVAL. https://www.coneval.org.mx/Informes/Evaluacion/Ficha_Monitoreo_Evaluacion_2013/SEP/11_S222.pdf [Google Scholar]
- Consejo Nacional de Evaluación de la Politíca de Desarrollo (CONEVAL). (2015). Programa de Escuela Segura. Informe de la evaluación específica de desempeño 2014–2015. Mexico City: CONEVAL. https://www.coneval.org.mx/Evaluacion/Documents/EVALUACIONES/EED_2014_2015/SEP/S222_PES/S222_PES_IE.pdf [Google Scholar]
- Drug Enforcement Administration (DEA). (2017). 2017 National Drug Threat Assessment (D. S. I. Section, Trans.). Washington, DC: Drug Enforcement Administration. [Google Scholar]
- Encuesta Nacional del Consumo de Drogas, Alcohol y Tabaco (ENCODAT), 2016. (2017a). Consumo de alcohol: prevalencias globales, patrones de consumo y variaciones estatales. Mexico City. https://www.gob.mx/cms/uploads/attachment/file/246052/hojasresumen_Alcohol-V3.pdf [Google Scholar]
- Encuesta Nacional de Consumo de Drogas, Alcohol y Tabaco (ENCODAT), 2016. (2017b). Consumo de drogas: prevalencias globales, tendencias y variaciones estatales. Mexico City. https://www.gob.mx/cms/uploads/attachment/file/234856/CONSUMO_DE_DROGAS.pdf [Google Scholar]
- García Aurrecoechea VR, Rodríguez Kuri SE, Córdova Alcaráz AJ, & Fernández Cáceres M. d. C. (2016). Diagnóstico macrosocial de riesgo del consumo de drogas en Máxico. Acta de Investigación Psicológica, 6(3), 2516–2526. 10.1016/j.aipprr.2016.11.005 [DOI] [Google Scholar]
- Gosin M, Marsiglia FF, & Hecht ML (2003). Keepin’ it R.E.A.L.: A drug resistance curriculum tailored to the strengths and needs of pre-adolescents of the southwest. Journal of Drug Education, 33(2), 119–142. 10.2190/DXB9-1V2P-C27J-V69V [DOI] [PubMed] [Google Scholar]
- Gottfredson DC, Cook TD, Gardner FE, Gorman-Smith D, Howe GW, Sandler IN, & Zafft KM (2015). Standards of evidence for efficacy, effectiveness, and scale-up research in prevention science: Next generation. Prevention Science: The Official Journal of the Society for Prevention Research, 16(7), 893–926. 10.1007/s11121-015-0555-x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Graham JW, Flay BR, Johnson CA, Hansen WB, Grossman LM, & Sobel JL (1984). Reliability of self-report measures of drug use in prevention research: Evaluation of the Project SMART questionnaire via the test-retest reliability matrix. Journal of Drug Education, 14(2), 175–193. 10.2190/CYV0-7DPB-DJFA-EJ5U [DOI] [PubMed] [Google Scholar]
- Hansen WB, & Graham JW (1991). Preventing alcohol, marijuana, and cigarette use among adolescents: Peer pressure resistance training versus establishing conservative norms. Preventive Medicine, 20(3), 414–430. [DOI] [PubMed] [Google Scholar]
- Hecht ML, Marsiglia FF, Elek E, Wagstaff DA, Kulis S, Dustman P, & Miller-Day M (2003). Culturally grounded substance use prevention: An evaluation of the keepin’ it REAL curriculum. Prevention Science, 4(4), 233–248. 10.1023/A:1026016131401 [DOI] [PubMed] [Google Scholar]
- Instituto Nacional de Estadística e Informática (INEGI). (2018). Encuesta nacional de victimización y percepción sobre seguridad pública 2018. Principales resultados Sonora. https://www.inegi.org.mx/programas/envipe/2018/ [Google Scholar]
- Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz (INPRFM). (2017a). Encuesta nacional de consumo de drogas, alcohol y tabaco 2016–2017: Reporte de drogas. Mexico City: INPRFM. [Google Scholar]
- Instituto Nacional de Psiquiatría Ramón de la Fuente Muñiz (INPRFM). (2017b). Encuesta nacional de consumo de drogas, alcohol y tabaco 2016–2017: Reporte de tabaco. Mexico City: INPRFM. [Google Scholar]
- Kulis S, Marsiglia FF, Elek E, Dustman P, Wagstaff DA, & Hecht ML (2005). Mexican/Mexican American adolescents and keepin’ it REAL: An evidence-based substance use prevention program. Children & Schools, 27(3), 133–145. 10.1093/cs/27.3.133 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kulis SS, Marsiglia FF, Nuño-Gutiérrez BL, Corona-Lozano MD, Mendoza-Meléndez MA, Kiehne E, Jager J, Ayers SL, & Han S (2019). Reciprocal effects of alcohol use and violence perpetration among early adolescents in Mexico: A gendered analysis. Journal of Youth and Adolescence, 48(8), 1519–1531. 10.1007/s10964-019-01014-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kulis SS, Marsiglia FF, Porta M, Arévalo Avalos MR, & Ayers SL (2019). Testing the keepin’ it REAL substance use prevention curriculum among early adolescents in Guatemala City. Prevention Science: The Official Journal of the Society for Prevention Research, 20(4), 532–543. 10.1007/s11121-018-0956-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kulis S, Nieri T, Yabiku S, Stromwall LK, & Marsiglia FF (2007). Promoting reduced and discontinued substance use among adolescent substance users: Effectiveness of a universal prevention program. Prevention Science: The Official Journal of the Society for Prevention Research, 8(1), 35–49. 10.1007/s11121-006-0052-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luengo MA, Romero E, Gómez-Fraguela JA, Guerra Lopez A, & Lence M (1999). La prevención del consumo de drogas y la conducta antisocial en la escuela: Analisis y evaluacion de un programa. Plan Nacional sobre Drogas. [Google Scholar]
- Marsiglia F, & Hecht M (2005). Keepin’ it REAL. Drug resistance strategies: Teacher guide. ETR Associates. [Google Scholar]
- Marsiglia FF, Booth JM, Ayers SL, Nuño-Gutierrez BL, Kulis S, & Hoffman S (2014). Short-term effects on substance use of the keepin’ it real pilot prevention program: Linguistically adapted for youth in Jalisco, Mexico. Prevention Science: The Official Journal of the Society for Prevention Research, 15(5), 694–704. 10.1007/s11121-013-0421-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsiglia FF, Kulis SS, Booth JM, Nuño-Gutierrez B, & Robbins DE (2015). Long-term effects of the keepin’ it REAL model program in Mexico: Substance use trajectories of Guadalajara middle school students. The Journal of Primary Prevention, 36(2), 93–104. 10.1007/s10935-014-0380-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marsiglia FF, Kulis S, Kiehne E, Ayers E, Libisch Recalde C, & Barros Sulca L (2018). Adolescent substance use prevention and legalization of Marijuana in Uruguay: A feasibility trial of the keepin’ it REAL prevention program. Journal of Substance Use, 23(5), 457–465. 10.1080/14659891.2017.1358308 [DOI] [Google Scholar]
- Marsiglia FF, Medina-Mora ME, Gonzalvez A, Alderson G, Harthun M, Ayers S, Gutiérrez BN, Corona MD, Melendez MAM, & Kulis S (2019). Binational cultural adaptation of the keepin’ it REAL substance use prevention program for adolescents in Mexico. Prevention Science: The Official Journal of the Society for Prevention Research, 20(7), 1125–1135. 10.1007/s11121-019-01034-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2012). Mplus user’s guide (7th ed.). Muthén & Muthén. [Google Scholar]
- Nadel H, Spellmann M, Alvarez-Canino T, Lausell-Bryant L, & Landsberg G (1996). The cycle of violence and victimization: A study of the school-based intervention of a multidisciplinary youth violence-prevention program. American Journal of Preventive Medicine, 12(5 Suppl), 109–119. 10.1016/S0749-3797(18)30243-5 [DOI] [PubMed] [Google Scholar]
- Piña Osuna FM, & Poom Medina J (2019). Deterioro social y participación en el tráfico de drogas en el estado de Sonora. Frontera Norte, 31, 1–20. https://doi.org/10.17428/rfn.v31i61.1754 https://doi.org/10.33679/rfn.v1i1.1976 [Google Scholar]
- Puyana JC, Puyana JCJ, Rubiano AM, Montenegro JH, Estebanez GO, Sanchez AI, & Vega-Rivera F (2017). Drugs, violence, and trauma in Mexico and the USA. Medical Principles and Practice: International Journal of the Kuwait University, Health Science Centre, 26(4), 309–315. 10.1159/000471853 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Secretaría de Salud. (n.d.). El consumo de drogas en México: Diagnóstico, tendencias y acciones. http://www.salud.gob.mx/unidades/cdi/documentos/CDM2-3.htm
- Secretaría de Educación Pública (SEP). (2012a). Manual de seguridad escolar. Recomendaciones para protegernos de la inseguridad y la violencia. https://educacionbasica.sep.gob.mx/multimedia/RSC/BASICA/Documento/201611/201611-3-RSC-DSat1SAXsU-manualseguridadsep12.pdf
- Secretaría de Educación Pública (SEP). (2012b). Programa Escuela Segura. Manual para fortalecer la prevención de adicciones desde la educación secundaria. https://hivhealthclearinghouse.unesco.org/sites/default/files/resources/21432_mpfpaes.pdf
- Schochet PZ (2009). An Approach for Addressing the Multiple Testing Problem in Social Policy Impact Evaluations. Evaluation Review, 33(6), 539–567. 10.1177/0193841X09350590 [DOI] [PubMed] [Google Scholar]
- Secretaría de Educación Pública (SEP). (2013). Evolución del presupuesto PES. https://educacionbasica.sep.gob.mx/multimedia/RSC/BASICA/Documento/201611/201611-3-RSC-787XzBdi17-evoluci_n_presupuesto_pes_2008-2013.pdf
- Tanner-Smith EE, Durlak JA, & Marx RA (2018). Empirically based mean effect size distributions for universal prevention programs targeting school-aged youth: A review of meta-analyses. Prevention Science: The Official Journal of the Society for Prevention Research, 19(8), 1091–1101. 10.1007/s11121-018-0942-1 [DOI] [PubMed] [Google Scholar]
- United Nations. (2018). Drugs and age. Drugs and associated issues among young people and older people. United Nations publication, Sales No. E.18.XI.9. https://www.unodc.org/wdr2018/prelaunch/WDR18_Booklet_4_YOUTH.pdf [Google Scholar]
- United Nations Office on Drugs and Crime (UNODC). (2010). The globalization of crime: A transnational organized crime threat assessment. United Nations. [Google Scholar]
- United Nations Office on Drugs and Crime (UNODC). (2018). World drug report 2018. Pre-briefing to the member states. New York: United Nations. www.unodc.org/wdr2018/prelaunch/Pre-briefingAM-fixed.pdf. [Google Scholar]
- Vargas Contreras E, Mendoza Galindo A, Martínez KIM, Lira Mandujano J, Oropeza Tena R, & Tiburcio Sainz MA (2016). Transferencia tecnológica en Psicología: El caso de los Centros de Atención Primaria de Adicciones del Estado de Baja California. Uaricha Revista de Psicología, 13, 124–148. [Google Scholar]
- Vilalta CJ, & Martinez JM (2012). The making of Narco bosses: Hard drug dealing crimes among Mexican students. Trends in Organized Crime, 15(1), 47–63. 10.1007/s12117-011-9144-y [DOI] [Google Scholar]
- Villatoro Velázquez JA, Medina-Mora ME, Martín del Campo Sánchez R, Fregoso Ito DA, Bustos Gamino MN, Resendiz E, Mujica R, Bretón M, Soto IS, & Cañas V (2016). El consumo de drogas en estudiantes de México: Tendencias y magnitud del problema. Salud Mental, 39(4), 193–203. 10.17711/SM.0185-3325.2016.023 [DOI] [Google Scholar]