

Abstract
Background
We present a case of fungal keratitis caused by Scedosporium apiospermum, which is a rare agent.
Case description
A 34-year-old Caucasian male patient was admitted to our clinic with complaints of pain and blurred vision in the left eye. The patient had a history of wearing contact lenses for 3 years. According to the Snellen chart, the patient’s visual acuity was 20/20 and counting fingers at 30 cm, for right and left eyes, respectively. A 3 × 3 mm corneal abscess at the center of the cornea with hypopyon in the patient’s left eye was observed. After the patient was hospitalized, fortified gentamicin and fortified cefazolin drops were started 24 times per day. Intravenous fluconazole 1 × 800 mg loading, 1 × 400 mg maintenance dose, intravenous vancomycin 4 × 500 mg and intravenous cefoperazone + sulbactam 2 × 2 g treatments were started. We observed S. apiospermum in the corneal scraping sample, which the identification was performed by combined phenotypic characteristics and matrix-assisted laser-desorption ionization time-of-flight mass spectrometry on the sixth day of treatment. The drops were revised as fortified vancomycin, ceftazidime, and voriconazole drops 24 times per day. Intravenous voriconazole 2 × 6 mg/kg loading and 2 × 4 mg/kg maintenance dose treatments were started. Three weeks later, left eye visual acuity increased to 20/40, and the corneal abscess regressed. On second-year follow-up, his visual acuity increased to 20/25 for the left eye and the cornea was transparent.
Conclusion
Scedosporium group is an opportunistic filamentous fungus that is very rarely seen and causes severe keratitis infections. In the literature, to the best of our knowledge, three cases of keratitis due to S. apiospermum after contact lenses were reported, and all were treated with penetrating keratoplasty. In this case, unlike the others, only medical treatment was applied. In cases with suspected fungal keratitis, medical treatment should be started without waiting for the culture result, the findings should be followed and penetrating keratoplasty should be performed in the case of no response to treatment.
Keywords: Anti-infective agents, Cornea, Diseases of the ocular surface, Fungal keratitis, Keratitis
Introduction
Fungal keratitis is an eye infection that is difficult to treat, with a poor prognosis. Fusarium and Aspergillus are the most common [1]. Scedosporium apiospermum is a filamentous fungus formerly known as Monosporium apiospermum. Scedosporium species are very rare among filamentous fungi causing keratitis. S. apiospermum is found on soil, fertilizer, polluted water, spoiled vegetables, and other natural areas. All over the world, it causes mycetoma, which is a chronic subcutaneous infection manifested by the formation of granules that causes severe local or widespread infections in patients with immunosuppression. The most common presentations in the eye are keratitis (84.6%) and sclerokeratitis (15.3%). Risk factors include ocular trauma, immunosuppressive drug use, long-term topical or systemic steroid use, preexisting corneal surface disease, underlying systemic diseases such as diabetes mellitus, and contact lens use [2].
In this study, we reported a case of keratitis due to Scedosporium apiospermum, which is seen rarely, after inappropriate contact lens wearing and treated only with medical treatment.
Case description
A 34-year-old Caucasian male patient was admitted to our clinic with complaints of pain in the left eye and blurred vision. He had no history of systemic disease, drug usage, or trauma. The patient had a history of wearing contact lenses for 3 years and continuously wearing them for 10–15 days. At the first examination, the patient’s visual acuity (VA) was 20/20 according to the Snellen chart and counting fingers at 30 cm, for the right and the left eyes, respectively, and intraocular pressure was 12 mmHg and 14 mmHg, respectively. On slit-lamp examination, the right eye was normal. There was a 3 × 3 mm corneal abscess at the center of the cornea with a 2 mm hypopyon on the left eye. Fundus examination was normal. Samples of conjunctival swab and corneal scrapings were taken on the same day of the patient’s admission to the hospital. Corneal scraping samples were plated onto Columbia agar with 5% sheep blood (Becton Dickinson, Germany) and Sabouraud dextrose agar (Becton Dickinson, Germany) and incubated at 30 °C under aerobic conditions. Two smears were made for a 10% KOH wet mount and Gram staining. Microscopic examination of the KOH wet mount and Gram staining showed fungal filaments. Empirically topical fortified (FF) cefazolin drops (Cefozin, Bilim İlaç) 24 times/day, FF Gentamycin Sulfate drops (gentamicin 0.3%, DEVA) 16 mg/ml 24 times per day, and fluconazole drops (Fluzamed/World Medicine) 2 mg/ml 24 times per day were started. Intravenous fluconazole (Candisept/VEM) 1 × 800 mg loading, 1 × 400 mg maintenance dose, intravenous vancomycin (Edicin/Sandoz) 4 × 500 mg, and intravenous cefoperazone + sulbactam (1107.4 mg + 1107.4 mg) (Sulzon/Tüm Ekip) 2 × 2 g treatment was started according to infectious disease consultation. The hypopyon regressed on the second day of treatment (Fig. 1A)
Fig. 1.
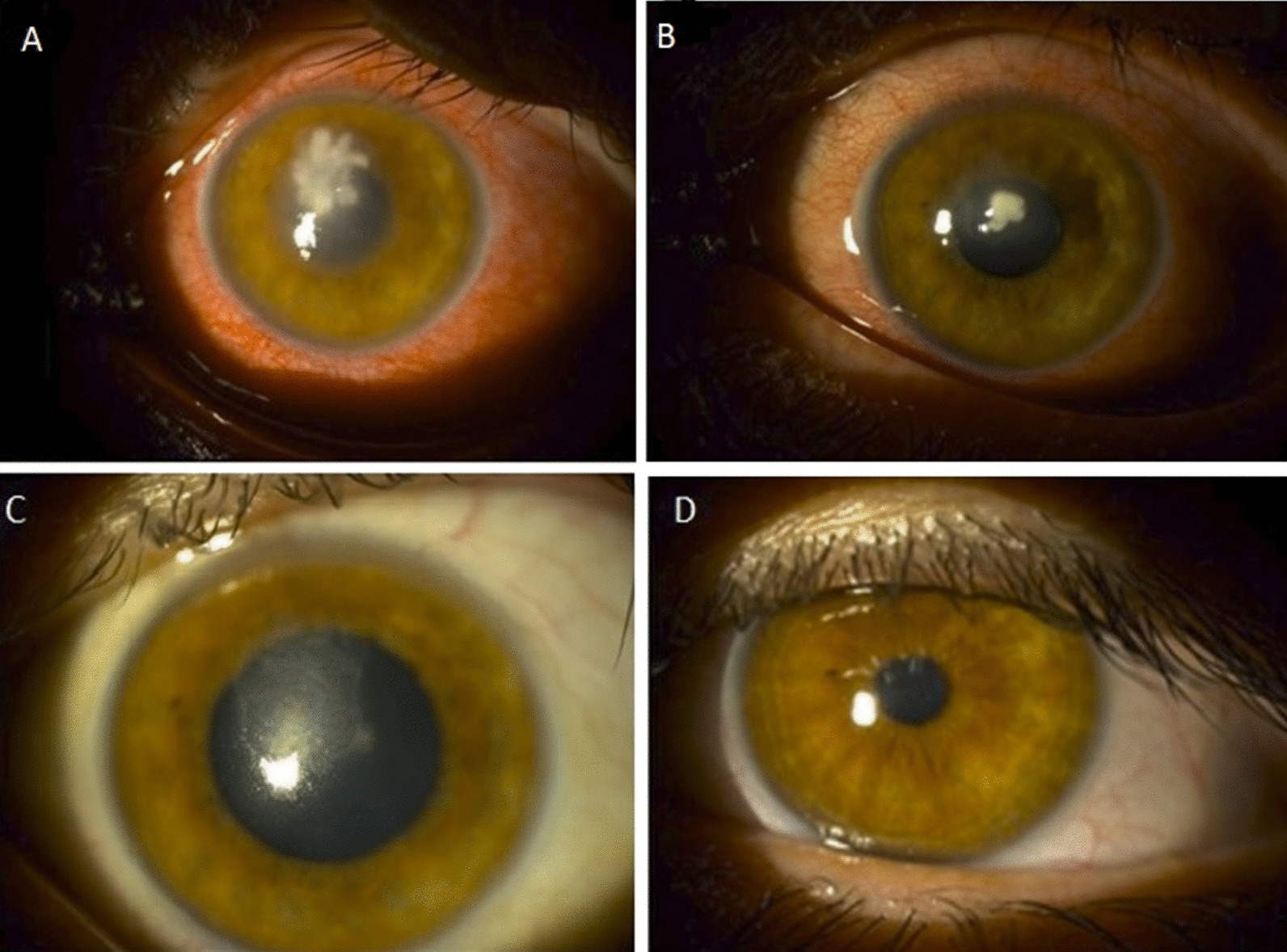
A The second day of patient’s treatment, 3 × 3 mm corneal abscess with conjunctival injection, hypopyon regressed. B The 22nd day of patient’s treatment, corneal abscess regressed. C Two months after treatment, the patient had a minimal corneal haze. D Two years after treatment, the patient had a clear cornea
When growth appeared (on the sixth day of treatment), it was examined both macroscopically and microscopically. Species identification was performed by combined phenotypic characteristics and matrix-assisted laser-desorption ionization time-of-flight mass spectrometry (MALDI-TOF–MS) (Bruker Daltonics, Germany). Scedosporium apiospermum colony was initially light-colored and later turned gray-brown (Fig. 2). The conidia were ovoid, unicellular, and subhyaline (Fig. 3). Antifungal susceptibility testing was performed by gradient diffusion test (E test, Biomerieux, Turkey) for amphotericin B, the azoles (fluconazole, itraconazole, posaconazole, and voriconazole), and the echinocandins (anidulafungin, caspofungin, micafungin) according to the manufacturer’s instructions. The minimum inhibitory concentrations for amphotericin B, itraconazole, posaconazole, voriconazole, anidulafungin, caspofungin, and micafungin were found to be 0.064, 0.25, 0.032, 0.064, 0.75, 0.125, and 0.032 μg/ml, respectively.
Fig. 2.
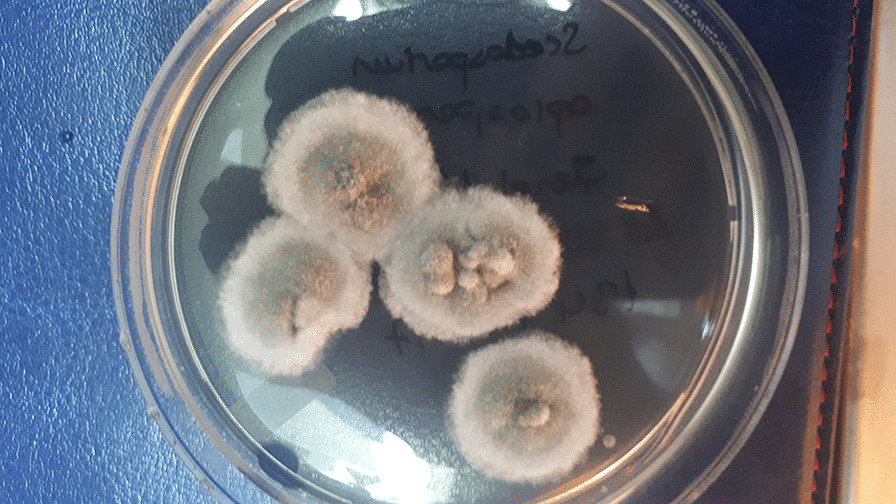
Scedosporium apiospermum. Sabouraud dextrose agar, 30 °C, 4 days. Surface of colony
Fig. 3.
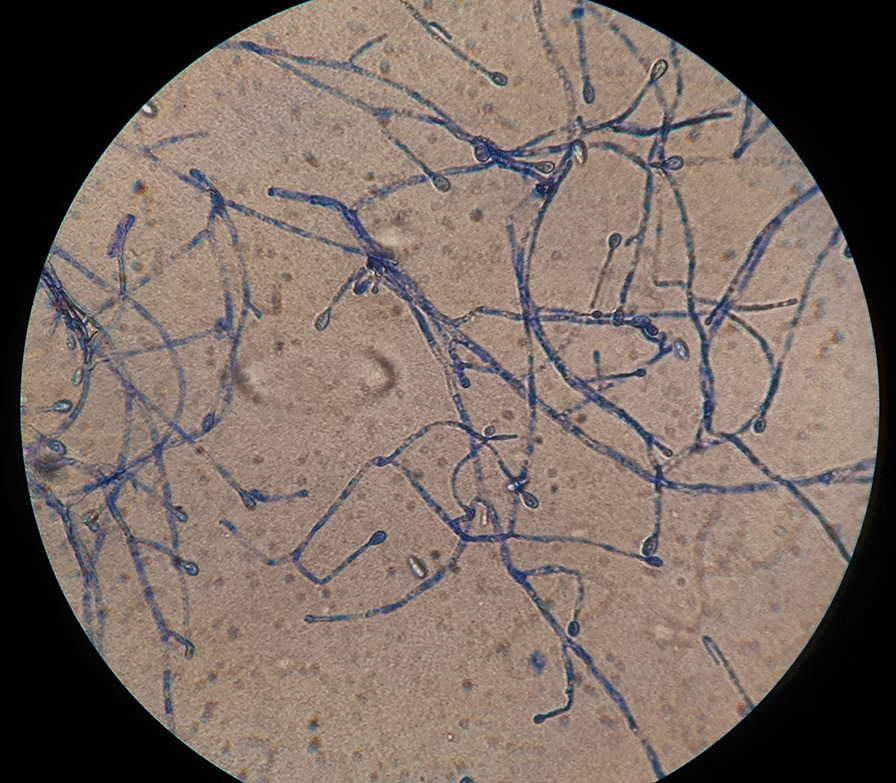
Scedosporium apiospermum. Lactophenol cotton blue (original magnification, ×400)
After culture results were obtained, the drops were revised as FF vancomycin (Edicin/ Sandoz İlaç) drops 24 times per day, FF ceftazidime drops (Zidim/Tüm Ekip) 24 times per day, and FF voriconazole drops (Vfend/Pfizer) 24 times per day. Intravenous fluconazole (Candisept/VEM) treatment was stopped, and intravenous voriconazole (Vfend/Pfizer) 2 × 6 mg/kg loading dose and 2 × 4 mg/kg maintenance dose treatments were started. On the 22nd day of hospitalization, the patient’s VA was 20/20 and 20/40 in the right and left eyes, respectively. On slit-lamp examination, we observed a 2 × 2 mm abscess in the left eye (Fig. 1B). After the patient was discharged from the hospital, oral voriconazole (Vfend/Pfizer) 2 mg/ml, 200 mg 2 × 1 treatment continued. Two months later, the corneal abscess regressed with minimal haze (Fig. 1C). On second-year follow-up, the patient’s visual acuity was 20/20 for the right and 20/25 for the left eye, and the cornea was transparent (Fig. 1D) (Table 1).
Table 1.
Timeline
| Time (days) | Day 0 | Day 6 | Day 22 | Day 60 | Day 730 |
|---|---|---|---|---|---|
| Visual acuity (Snellen chart) | Counting fingers at 30 cm | 20/400 | 20/40 | 20/25 | 20/25 |
| Findings | A 3 × 3 mm corneal abscess with hypopyon | The hypopyon regressed | A 2 × 2 mm corneal abscess | The corneal abscess regressed with minimal haze | The cornea was transparent |
| Treatment |
FF gentamicin and FF cefazolin drops 24 times per day Intravenous fluconazole 1 × 800 mg loading, 1 × 400 mg maintenance dose Intravenous vancomycin 4 × 500 mg Intravenous cefoperazone + sulbactam 2 × 2 g |
FF vancomycin, ceftazidime voriconazole drops 24 times per day Intravenous voriconazole 2 × 6 mg/kg loading and 2 × 4 mg/kg maintenance dose |
FF vancomycin, ceftazidime voriconazole drops 8 times per day Oral voriconazole 200 mg 2 × 1 |
Treatment stopped | No treatment |
FF fortified
Discussion
Fungal keratitis is one of the most important causes of ophthalmic mycosis. It is usually characterized by corneal epithelial defect and stromal infiltration. Corneal infection due to S. apiospermum was first described in 1955 [3]. While keratitis was detected in the majority of these patients, endophthalmitis, scleritis, corneal ulceration, conjunctival mycetoma, keratouveitis, retinitis, chorioretinitis, and orbital infection were also diagnosed [4].The use of steroids and the presence of immunosuppression from diseases such as diabetes may worsen the prognosis of fungal keratitis [5].
In previous case reports and literature review, a few cases of ocular infection due to Scedosporium were observed even in immunocompetent patients, resulting in vision loss or evisceration/enucleation despite medical and surgical treatment [6]. It is also suggested that early diagnosis, along with proper treatment, is the most important determinant of the prognosis. Soft contact lenses are one of the most important risk factors for fungal keratitis in temperate climates [7]. In this case, the main risk factor is improper use of the lens without removing the lens for a long time. Contamination of the cleaning solution may also have caused this condition. As of now, only three cases of keratitis due to S. apiospermum have been reported after wearing contact lenses [6, 8, 9]. The first case was treated with topical voriconazole and intravenous voriconazole [6], the second case (with endophthalmitis and had pars plana vitrectomy) was treated with intravenous voriconazole and intravitreal voriconazole [8], and the last case was treated with topical econazole (1%) and amphotericin B (0.15%) with oral itraconazole (200 mg daily) [9]. All three cases underwent penetrating keratoplasty. In this case, unlike other cases, keratitis regressed only with medical treatment.
In a study by Ramakrishnan et al. [10], Scedosporium was detected in 13 (0.8%) of 1621 patients with culture-positive fungal keratitis. The combination of natamycin and fluconazole was successful in seven out of ten patients. In total, 30.7% of these patients have trauma due to a nonspecific foreign body, 15.3% trauma with organic material, 7.6% have uncontrolled diabetes, and 7.6% have a recent history of cataract surgery. In five cases, no cause was found (38.46%). Nulens et al. [11] showed that, after 12 days of oral voriconazole treatment, the level of voriconazole in the aqueous humor reached 53% of the plasma. In that case, it was reported that, as there was no response from itraconazole and amphotericin B treatment, the patient was treated with penetrating keratoplasty and oral voriconazole treatment was initiated. In another study [12], 1% topical voriconazole monotherapy was found to be effective in Scedosporium keratitis accompanied by mild anterior chamber inflammation. Özkan et al. [13] report a case that was successfully treated with 1% voriconazole eye drops from the third day of prediagnosis.
Conclusion
We reported the case of a patient who developed fungal keratitis after wearing contact lenses, which is rarely seen. After S. apiospermum was detected in culture, the treatment of the patient, who responds to topical and intravenous voriconazole treatment, was continued. In patients with fungal keratitis or endophthalmitis, medical treatment should be started urgently, the findings should be followed daily, and if there is no response to treatment, keratoplasty should be performed without delay. The patient’s findings improved with medical treatment. In addition, fungal factors should be taken into consideration in cases followed up for keratitis (especially for contact lenses), and microbiological examinations should be performed accordingly.
Acknowledgements
Not applicable.
Author contributions
All authors contributed to the follow-up of the patient, as well as preparation and submission of the manuscript. The data used during the current study are available from the corresponding author on reasonable request. All authors read and approved the final manuscript.
Funding
There is no disclosure of any funding received for this work.
Availability of data and materials
Figures were added as supporting data.
Declarations
Ethics approval and consent to participate
This study was conducted in compliance with the ethical standards set out in the Declaration of Helsinki. Consent to participate was obtained.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.
Competing interests
The authors declare that they have no competing interests.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Çisil Erkan Pota, Email: cisilerkann@gmail.com.
Yusuf Ayaz, Email: yusufayaz120512@gmail.com.
Mustafa Ünal, Email: mustafaunalmd@gmail.com.
Özlem Koyuncu Özyurt, Email: ozlemozyurt@akdeniz.edu.tr.
References
- 1.Kwon Chung KJ, Bennett JE. Infections due to miscellaneous molds. In: Kwon Chung KJ, Bennett JE, editors. Medical mycology. Philadelphia: Lea & Febiger; 1992. pp. 733–767. [Google Scholar]
- 2.Al-Badriyeh D, Neoh CF, Stewart K, Kong DC. Clinical utility of voriconazole eye drops in ophthalmic fungal keratitis. Clin Ophthalmol. 2010;4:391–405. doi: 10.2147/opth.s6374. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wu Z, Ying H, Yiu S, Irvine J, Smith R. Fungal keratitis caused by Scedosporium apiospermum. Cornea. 2002;21(5):519–523. doi: 10.1097/00003226-200207000-00016. [DOI] [PubMed] [Google Scholar]
- 4.Manzouri B, Vafidis G, Wyse R. Pharmacotherapy of fungal eye infections. ExpertOpin Pharmacother. 2001;2(11):1849–1857. doi: 10.1517/14656566.2.11.1849. [DOI] [PubMed] [Google Scholar]
- 5.Devaraj NK, Aneesa AR, Abdul Hadi AM, Shaira N. Topical corticosteroids in clinical practice. Med J Malay. 2019;74(2):187–189. [PubMed] [Google Scholar]
- 6.Cassano F, Cardascia N, Tegola MGL, Boscia F, Alessio G. Scedosporium apiospermum contact lens-related keratitis: a case report and literature review. Med Hypothesis Discov Innov Ophthalmol. 2021;10(2):80–85. doi: 10.51329/mehdiophthal1425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Schmack I, Müller M, Kohnen T. Mikrobielle Keratitis—Teil 2: mykotische und Akanthamöbenkeratitiden [Microbial keratitis—part 2: specific aspects of mycotic and acanthamoeba keratitis] Klin Monbl Augenheilkd. 2018;235(4):511–530. doi: 10.1055/a-0483-4214. [DOI] [PubMed] [Google Scholar]
- 8.Lenk J, Raiskup F, Pillunat LE, Rossler S. Scedosporium apiospermum—a rare pathogen of keratomycosis. Ophthalmologe. 2020;117(12):1225–1228. doi: 10.1007/s00347-020-01073-x. [DOI] [PubMed] [Google Scholar]
- 9.Bui DK, Carvounis PE. Favorable outcomes of filamentous fungal endophthalmitis following aggressive management. J Ocul Pharmacol Ther. 2016;32(9):623–630. doi: 10.1089/jop.2016.0055. [DOI] [PubMed] [Google Scholar]
- 10.Ramakrishnan S, Mandlik K, Sathe TS, Gubert J, Krishnan T, Baskaran P. Ocular infections caused by Scedosporium apiospermum: a case series. Indian J Ophthalmol. 2018;66(1):137–140. doi: 10.4103/ijo.IJO_524_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Nulens E, Eggink C, Rijs AJ, Wesseling P, Verweij PE. Keratitis caused by Scedosporium apiospermum successfully treated with a cornea transplant and voriconazole. J Clin Microbiol. 2003;41(5):2261–2264. doi: 10.1128/JCM.41.5.2261-2264.2003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Al-Badriyeh D, Leung L, Davies GE, Stewart K, Kong D. Successful salvage treatment of Scedosporium apiospermum keratitis with topical voriconazole after the failure of natamycin. Ann Pharmacother. 2009;43(6):1139–1142. doi: 10.1345/aph.1M008. [DOI] [PubMed] [Google Scholar]
- 13.Özkan A, Susever S, Erturan Z, et al. A case of keratitis caused by Scedosporium apiospermum. J Microbiol Infect Dis. 2013;03(01):45–48. doi: 10.5799/ahinjs.02.2013.01.0079. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
Figures were added as supporting data.