

Abstract
Objective:
This study aimed to compare the effects of human umbilical cord mesenchymal stem cells (hUCMSCs), amniotic fluid (AF), and a combination of both on the uterus and ovaries in a rat model of abdominal adhesions.
Material and Methods:
This study was designed as a controlled study. Four groups, each consisting of six rats, were randomly formed. One group was designated as the control (CNT). hUCMSCs - applied (hUCSC), AF-applied (AMN), and a combination of both (hUCSC + AMN) were the experimental groups. All rats were given intraperitoneal talc powder to create adhesions. After 21 days, animals in experimental groups were further treated with hUCMSC, AF or a combination of these.
Results:
There was a statistically significant difference in primordial follicle count, endometrial gland number, and endometrial blood vessel count (p<0.05). AMN provided the best results in the endometrial vessel and primordial follicle count. The average endometrial gland count in AMN and hUCSC + AMN was similarly higher than CNT and hUCSC alone.
Conclusion:
There were significantly higher for counts for endometrial glands, endometrial blood vessels, and primordial follicles in the hUCSC, AMN and hUCSC + AMN groups compared to controls. Animals in the AMN group had the best result for endometrial vessel and highest primordial follicle count.
Keywords: Amniotic fluid, case-control studies, infertility, ovaries, rats, stem cells, surgical adhesions, uterus
Introduction
Adhesion is one of the most common reactions observed between two tissues after abdominal surgery. It is reported as a common cause of morbidities, such as second surgery, infertility, ileus, pain, and intraoperative complications in further surgeries (1). It is reported that of the patients who undergo open abdominal or pelvic surgery, 79-90% develop adhesions (2,3,4). The ratio of relaparotomy due to adhesions varies between 5-20% (2). Laparoscopic surgery decreases the extent and severity of the formation of adhesions by approximately 50%, mainly at the incision line (3,5). However, even with the more widespread use of laparoscopic surgery, its overall surgical burden remains high (1).
There is no quantitative marker for the diagnosis of adhesions. As a result, the best evaluation is made via inspection. However, some objective techniques may be used to study the severity of adhesions, such as ultrasonography, computed tomography, and magnetic resonance imaging (6,7). Non-invasive techniques are better for aiding diagnosis, as laparoscopy may be a cause of adhesions (8).
Limiting and preventing adhesions would dramatically decrease potential complications, such as infertility, ileus, and pain (9). Many studies have investigated adhesion prophylaxis but the problem remains unsolved (10,11,12,13,14,15). According to Liakakos et al. (16), the primary aim should be minimalizing mechanical and energy-related trauma, such as avoiding powdered gloves in open surgical interventions, as minimal trauma allows for better vascularization in the postoperative period. Risberg (17) suggested that cleaning the necrotic debris with crystalloid solutions in the surgical site and using barrier gel for damaged and unprotected surfaces would decrease postoperative adhesions by decreasing the fibrosis and extracellular matrix accumulation. In a study by Canbaz et al. (18) in a rat model, gonadotropin-releasing hormone agonist therapy successfully reduced postoperative adhesion formation but was not superior to intraperitoneal Ringer’s lactate solution. An increasing number of studies (19) have researched the adhesion prevention capability of various barrier agents (20,21,22,23), various combination gels (24,25,26,27,28,29), biomaterials (30), growth factor inhibitors (31,32), and stem cells (33,34,35), which is evidence of the importance of adhesion-related problems.
It is essential to understand the pathophysiological process of adhesion formation in order to find effective solutions, especially when using stem cells in regenerative treatments. After a surgery, inflammatory cells recruited for the healing process collect at the surgical site and the surrounding tissues via the vascular supply. Macrophages are dominant in the first 24 hours, followed by neutrophils. Peritoneal healing occurs in seven to ten days. Tissue surfaces are filled with highly regenerative promesothelial and mesothelial cells (36). When these cells arrive at the damaged tissue, they collect in the extracellular matrix. The extracellular matrix, formed by fibronectin, hyaluronic acid, and proteoglycans, gets replaced with permanent collagen and widespread fibrosis occurs (16). Therefore, primary repair through the mesothelial cells completes with scarring. Regenerative treatments mainly focus on cell therapies and biomaterials, such as umbilical cord and amniotic fluid stem cells (AFSCs) that are multipotent cells, and thus can differentiate into the tissue they are integrated into. This quality renders stem cells a candidate treatment to improve post-surgical tissue healing.
Many studies have demonstrated that the mesenchymal stromal cells of amniotic fluid (AF) have cytoprotective and regenerative effects (37,38,39,40). It has been demonstrated that AF mesenchymal stromal cells significantly reduced postsurgical intra-abdominal adhesions in a rat model (41). The epithelial cells of human AF are proposed as a novel stem cell candidate in the treatment of severe intra-abdominal adhesions in a second rat model study (42). Additionally, human umbilical cord mesenchymal stem cells (hUCMSCs) are also a significant source of regenerative potential, and have been described in many kinds of tissue, such as bone, wound, nerves and vessels (43,44,45,46,47,48,49). However, the effect of hUCMSCs on intra-abdominal adhesions is unknown. One of the important complications of intra-abdominal adhesions is infertility, and the effect of intra-abdominal adhesions on infertility needs further researching.
The primary aim of this study was to evaluate and compare the effects of hUCMSCs, AF, and a combination of both on the uterus and ovaries in a rat model with abdominal adhesions with a control group. The secondary aim of the study was to determine the penetration of hUCMSCs into the uterus and ovaries and the effects of the treatments on adhesion healing.
Material and Methods
The ethical approval of this study was authorized by Acıbadem Mehmet Ali Aydınlar University Faculty of Medicine Animal Experiments Local Ethics Committee (approval number: 2017/37, date: 07.09.2017).
Selection and description of rats
Twenty-four 6-8 week-old, female Wistar-Albino rats, with an average weight of 350-400 g, were purchased from Acıbadem University ACU-DEHAM, following the Federation of European Laboratory Animal Science Associations guidelines and accredited by the Association for Assessment and Accreditation of Laboratory Animal Care. The inclusion criterion was being healthy, and the exclusion criteria were being pregnant and having previous surgery. The rats were housed with a 24 °C room temperature, 12:12 hour day/night cycle, with adequate water and food supply.
Technical information
A hypothesis with its research questions was developed and are presented below:
Hypothesis: hUCMSCs, AF, and a combination of these are associated with a high number of follicles, endometrial glands, and endometrial blood vessels of the uterus and ovaries in a rat model with abdominal adhesions.
1. Is there a significant difference between the treatments in terms of the uterus (number of endometrial glands and endometrial blood vessels, macroscopic morphology)?
2. Is there a significant difference between the treatments in terms of the ovaries (primordial and preantral follicle counts)?
Therefore, the primary outcomes were the number of endometrial glands and endometrial blood vessels, macroscopic uterus morphology, primordial and preantral follicle counts. The secondary outcomes were the penetration of the hUCMSCs into the uterus and ovaries and adhesion healing.
Study design
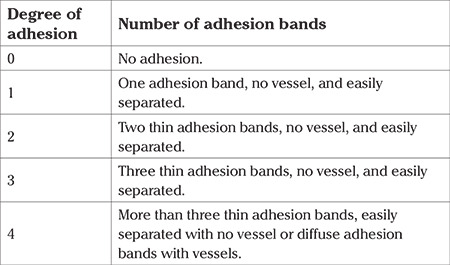
This study was designed as a controlled study. Four groups, each consisting of six rats, were randomly formed. One group was designated as the control (CNT). hUCMSCs - applied (hUCSC), AF-applied (AMN), and a combination of both (hUCSC + AMN) were designated as the experimental groups. All rats were given intraperitoneal talc powder to create adhesions. After 21 days, animals in experimental groups were further treated with hUCMSC, AF or a combination of these. Two rats in the hUCSC group were given green fluorescent protein (GFP)-marked stem cells, and another two in the same group were treated with quantum dot (QD)-marked stem cells to evaluate deep penetration into gynaecologic tissues. The sample size and experimental interventions are shown in Table 1. After one week, the rats were sacrificed, and the abdominal walls were incised to evaluate the abdomen. Macroscopic evaluation of any adhesions (secondary outcome) was conducted according to the modified adhesion scoring scale defined by Canbaz et al. (18) (Table 2). Afterwards, the uterus, ovaries, and fallopian tubes were removed and then macroscopically and microscopically evaluated (primary and secondary outcomes). The researchers were not blinded to any data.
Table 1. Description of the sample size.
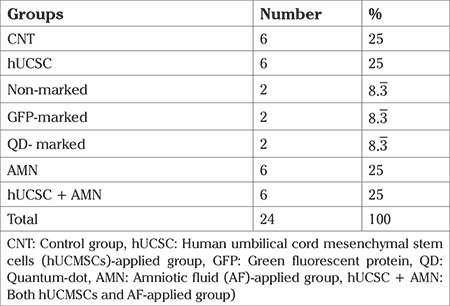
Table 2. Modified adhesion scoring scale (18).
Human umbilical cord mesenchymal stem cell preparation
The cells were obtained from the umbilical cord blood of an informed, healthy woman who underwent caesarean delivery. All steps were carried out with sterilised equipment. First, the umbilical cord was washed with normal saline [0.9% sodium chloride (NaCl)]. Afterwards, it was dissected, and the vasculature was removed using a scalpel to obtain Wharton’s jelly. The Wharton’s jelly was cut into pieces 5 mm in length, 5 mm in width, 3 mm in height and washed with 0.9% NaCl solution. The pieces were put on the base of T75 flasks so that each would contain 7-8 pieces. The flasks were gently turned upside down and put in incubators at 37 oC, 5% CO2, and 7% O2 for 45 minutes for the pieces to stick to the flasks. Afterwards, Dulbecco’s modified eagle medium-low glucose (DMEM-LG) (Sigma-Aldrich, St. Louis, Missouri, USA) including 1% penicillin/streptomycin and 10% human serum was poured into the flasks. The flasks were put in incubators at 37 oC, 5% CO2, and 7% O2 for six days and the medium was changed on the sixth day. The cells were passaged after the confluency exceeded 70%. Then the cells were put in a solution containing Ringer’s lactate and 1% human serum albumin. A total of 3.5 mL hUCMSCs divided into 500 µL (1x107 hUCMSCs) per animal was used.
Green fluorescent protein marking
The envelope pCMV-VSV-G [a gift from Bob Weinberg (Addgene, Watertown, Massachusetts, USA #8454. http://n2t.net/addgene:8454; RRID: Addgene_8454)] plasmid, the packaging psPAX2 [a gift from Didier Trono (Addgene #12260; http://n2t.net/addgene:12260; RRID: Addgene 12260)] plasmid, and the GFP-encoding pCDH-EF1-copGFP-T2A-Puro plasmid DNA was transformed into competent E. coli DH5a bacteria [NEB® 5-alpha competent E. coli (high efficiency)]. The endotoxin-free plasmids were amplified using the QIAfilter Plasmid Giga Kit (QIAGEN, Hilden, Germany), and quality control tests of the produced plasmid were performed in (blinded for review) with accredited protocols. HEK293T cells as host cells were cultured in 5-layer cell culture flasks in an incubator at 37 °C, 5% CO2 (NEST) for 70% confluence the day before transfection under an inverted microscope. The isolated envelope, packaging, and pCDH-EF1-copGFP-T2A-Puro plasmids (1:1:2 ratio) were mixed with FuGENE HD (Promega, Madison, Wisconsin, USA) transfection reagent for lentivirus (LV) production in opti-MEM reduced serum media (Thermo Fisher Scientific, Waltham, Massachusetts, USA), including 1% penicillin/streptomycin. The packaged recombinant GFP-LV was harvested from the supernatant of the cell cultures 48 hours after transfection. The supernatant, including GFP-LV was filtered (0.45 µm) and concentrated 100x with the Lenti-X concentrator (Takara Bio, Kusatsu, Shiga, Japan). Jurkat cell line (ATCC, Manassas, Virginia, Product Code: TIB-152TM) was suspended as 10,000 cells in 100 µL of RPMI medium with glutamine HEPES with 10% foetal bovine serum (FBS), 1% penicillin/streptomycin, 1% non-essential amino acids, 1% sodium pyruvate, and 1% vitamins. The Jurkat cells in 100 µL of the medium were plated in 96-well plates from A to I. The wells were adjusted to have 10 µL, 3 µL, 1 µL, 0.3 µL, 0.1 µL, and 0.03 µL of the 100x-concentrated GFP-LV solutions in each 50 µL of the medium, respectively, and then 50 µL of virus dilution from each concentration was transferred to Jurkat cultured wells, the total volume was adjusted to 150 µL, and cells were incubated for 3-4 days. Flow cytometry was performed using MACSQuant flow cytometry (Miltenyi Biotec, Bergisch Gladbach, North Rhine-Westphalia, Germany) for GFP expression. Following the GFP-LV titer assay and other quality control tests, including sterility and purity analyses, the GFP-coding viruses were stored at -80 °C. Mesenchymal stem cells were infected with the GFP-coding LV (1-5 multiplicity of infection) expressing pCDH-EF1-copGFP-T2A-Puro. A flow cytometer confirmed stem cells synthesizing GFP at the end of the 4th day. Greater than 95% GFP positive stem cells were replicated in an incubator at 37 °C, 5% CO2 up to 1x107 cells by the antibiotic selected result, only GFP-labelled mesenchymal stem cells were obtained. A total of 1 mL GFP-marked UCSC, divided into 500 µL (1x107 umbilical cord stem cells) per animal were used.
Quantum dot marking
QD marking was utilised to be able to observe the depth of penetration of the hUCMSCs into gynaecologic tissues. A sample was taken from an unmarked cell (to use as control inflow). QtrackerTM 655 Cell Labelling Kit (Thermo Fisher Scientific, Waltham, Massachusetts, USA) A and B components were gently mixed. For every 1x107 cells, 10 µL A and B components were added into the tube. The mixture was incubated at 37 °C, 5% CO2 for 5 minutes. Immediately after the incubation, 0.2 mL freshly prepared solution containing DMEM-LG, 10% FBS, and 1% penicillin was added and vortex mixed for 30 seconds. Cells were incubated at 37 °C, 5% CO2 for 45-60 minutes in a tube. After the incubation, the cells were centrifuged for 10 minutes at 400 G and bathed in DMEM-LG, 10% FBS, and 1% penicillin medium. The batheing was repeated. A sample was taken from the medium to quantify the marked cells using flow cytometry. The marked and control cells were sent for quality control in terms of viability, sterility, and differentiability. A total of 1 mL QD-marked hUCMSCs divided into 500 µL (1x107 umbilical cord stem cells) per animal were used.
Amniotic fluid preparation
For the AF, the samples were derived from the amniotic sac of the same informed, healthy woman who underwent caesarean delivery. AF was put through 0.22 µm filters to decontaminate upon arrival. Afterwards, it was kept at -80 oC before gamma irradiation for decontamination. Lastly, the samples were liquefied for study use. A total of 24 mL of AF, 1 mL per animal, was used.
Intraperitoneal talc and treatment injection
The rats were anesthetized with xylazine (0.6 mg/kg/intraperitoneal) and ketamine (0.9 mg/kg/intraperitoneal) and fixed in a dorsosupine position. The abdominal walls were shaved and disinfected with povidone-iodine. The abdominal wall was incised with a vertical incision (Figure 1A), and sterile cannulas were placed into the abdominal cavities (Figure 1B). 1 cc talc powder was given intra-abdominally per rat to create adhesions. Afterwards, the cannulas were removed, and the peritoneum and the abdominal wall were closed with 2/0 rapid vicryl. The rats were given daily amoxicillin/clavulanic acid in the postoperative three days.
Figure 1.
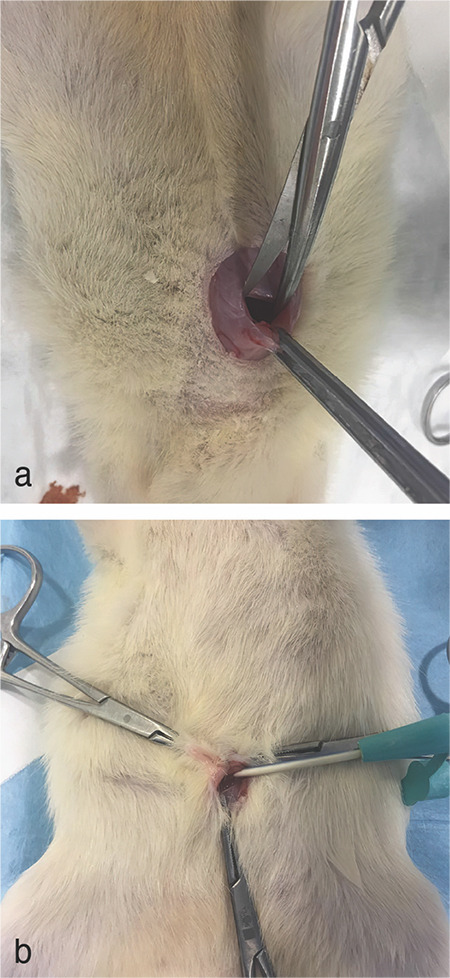
Images of the surgical procedure used. a) Vertical incision in the abdominal wall. b) Placement of a sterile cannula into the abdominal cavity for the application of talc powder
On the twenty first day of the study, the rats were injected with hUCMSCs or AF or both. After one week, on the twenty-eighth day, the rats were sacrificed and disected. The uterus, ovaries, fallopian tubes, and peritoneum were removed through an approximately 4 cm incision and placed in 10% formaldehyde solutions for histopathologic evaluations.
Statistical analysis
Normality of data was tested with the Shapiro-Wilk test. Non-parametric statistical methods were used for values with skewed distribution (non-normally distributed, Shapiro-Wilk p>0.05). Descriptive statistics are presented using mean and standard deviation for normally distributed variables and median (and minimum-maximum) for the non-normally distributed variables. For comparison of two normally distributed independent groups, the Student’s t-test was used. Non-parametric statistical methods were used for values with skewed distribution. For comparison of two non-normally distributed independent groups, the Mann-Whitney U test was used. Statistical analysis was performed using IBM SPSS Statistics, version 24 (IBM, Armonk, New York, USA).
Results
The sample size for experimental groups is shown in Table 1. There was no incidence of intra-abdominal ascites, surgical site infection, nor animal death following the application of talc powder.
Microscopic evaluations of the gynaecological system
Uterus and ovaries (primary outcomes)
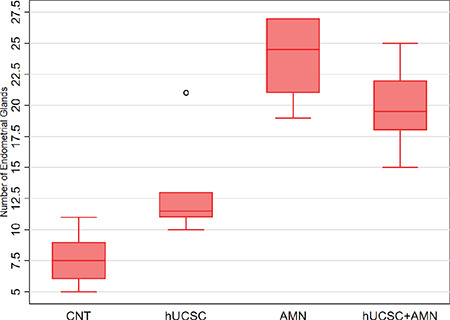
There was a statistically significant difference in terms of endometrial gland number, endometrial blood vessel count, and primordial follicle count distributions according to the groups (Kruskal-Wallis test, p<0.05) (Table 3).
Table 3. Comparison of the groups in terms of uterus and ovarian histology.
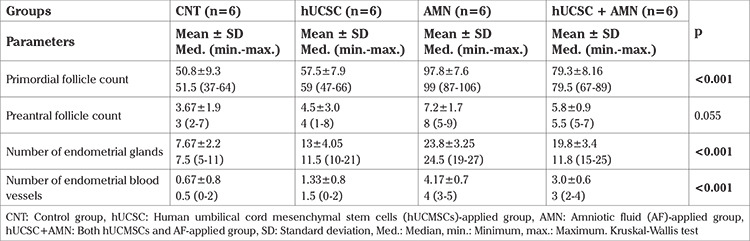
According to the post-hoc pairwise comparison (Table 4), in terms of endometrial gland count, there was a significant difference between pairwise groups except for CNT versus hUCSC and AMN versus hUCSC + AMN (Table 4) (Mann-Whitney U test, p<0.008, Bonferroni correction). The average number of endometrial glands in AMN was higher than CNT and hUCSC and similar to hUCSC + AMN (Figure 2).
Table 4. Post-hoc pairwise comparisons of the groups by Mann-Whitney U test.

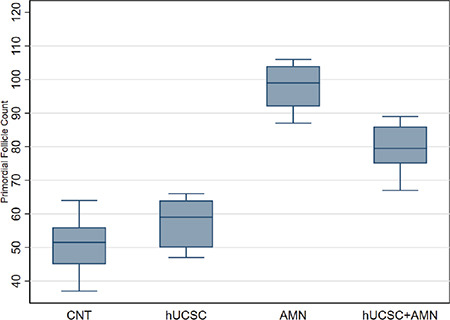
Figure 2.
Box plot of the primordial follicle counts of the groups
CNT: Control group, hUCSC: Human umbilical cord mesenchymal stem cells (hUCMSCs)-applied group, AMN: Amniotic fluid (AF)-applied group, hUCSC + AMN: Both hUCMSCs and AF-applied group
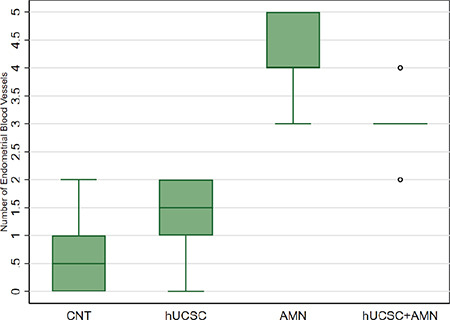
In terms of endometrial blood vessel count, there was a significant difference between pairwise groups except for CNT versus hUCSC, AMN versus hUCSC + AMN, and hUCSC versus hUCSC + AMN (Table 4) (Mann-Whitney U test, p<0.008, Bonferroni correction). The average blood vessel count in the AMN group was significantly higher than the others (Figure 3).
Figure 3.
Box plot of the number of endometrial glands of the groups
CNT: Control group, hUCSC: Human umbilical cord mesenchymal stem cells (hUCMSCs)-applied group, AMN: Amniotic fluid (AF)-applied group, hUCSC + AMN: Both hUCMSCs and AF-applied group
In terms of distribution of primordial follicle count, there was a significant difference between the pairwise groups, except for CNT versus hUCSC (Mann-Whitney U test p<0.008, Bonferroni correction). In addition, the average number of primordial follicles in AMN was found to be significantly higher than the other groups (Figure 4).
Figure 4.
Box plot of the number of blood vessels of the groups
CNT: Control group, hUCSC: Human umbilical cord mesenchymal stem cells (hUCMSCs)-applied group, AMN: Amniotic fluid (AF)-applied group, hUCSC + AMN: Both hUCMSCs and AF-applied group
On histopathological semi-quantitative evaluation, in CNT the ovary germinal epithelium was observed as single-layered and cubical. Small-sized primordial follicles were lost in the oocytes. Additionally, atretic follicles (Figure 5A) and areas of vacuolation (Figure 5B) were present. The integrity of the uterine tissue was not preserved (Figure 6A) and the tunica albuginea layer was enlarged.
Figure 5.
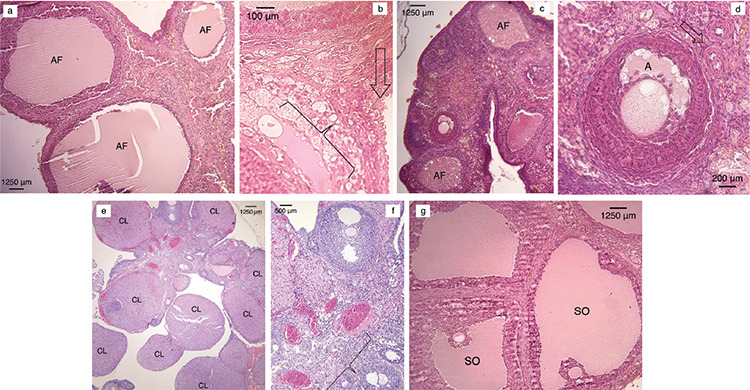
Photomicrographs of the ovaries of the groups. (haematoxylin & eosin). a) Different stages of degenerated atretic follicles (AF) are evident in the CNT group animal samples (x40 magnification). b) Vacuolation in the interfollicular area (parenthesis) is evident in the CNT group samples in the interstitial area (arrow) (x400 magnification). c) The human umbilical mesenchymal cord stem cells (hUCMSCs)-applied group shows healthy antral follicles (AF) surrounded by a preantral follicle (x40 magnification). d) The hUCMSCs-applied group demonstrating intact zona pellucida and antrum a) and oocytes and primordial follicles (arrow) (x200 magnification). e) The amniotic fluid (AF)-applied group exhibited superovulation and multiple corpus luteum (CL) (x40 magnification). f) The AF-applied group displayed multiple endometrial blood vessels (parenthesis) (x100 magnification). g) Both hUCMSCs and AF-applied groups showed superovulated follicles (SO) (x40 magnification)
Figure 6.
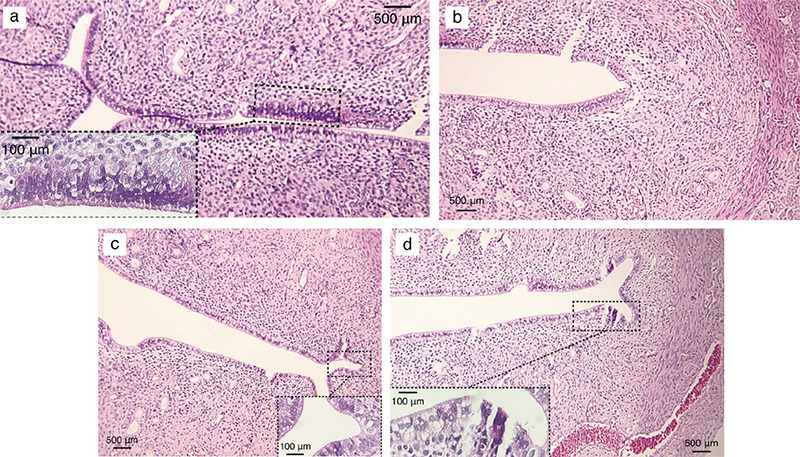
Photomicrographs of uterine tissue and endometrium of the groups (haematoxylin & eosin). a) The control group exhibited hyperplasia, metaplasia, and vacuolation of the epithelial lining of the endometrium, shedding of the epithelium and perimetrium, narrow uterine lumen, and decrease in myometrial smooth muscle cells (main image, x100 magnification), and connective tissue loss in the endometrium (lower-left corner image, x400 magnification). b) The human umbilical cord mesenchymal stem cells (hUCMSCs)-applied group displayed endometrial proliferation, extensive myometrium, and blood vessel increase in the stratum vasculare (x100 magnification). c) The amniotic fluid (AF)-applied group showed narrow uterine lumen (main image, x100 magnification) due to increase and enlargement of the uterine glands, and their movement towards the surface of the endometrium (lower-right corner image, x400 magnification). d) Both hUCMSCs and AF-applied groups demonstrated connective tissue proliferation in the uterine wall with the formation of newly formed blood capillaries, growth in myometrium and increased collagen (main image, x100 magnification), and irregularity in glandular structures (lower-left corner image, x400 magnification)
In hUCSC, the ovary germinal epithelium was observed as mildly proliferated. Dominant follicles were high in number. Antral follicles were surrounded with normal-sized preantral follicles (Figure 5C, D). Stromal vascularity and the number of endometrial glands were high. A high number of cells in the connective tissue and the superficial endometrium was present. Epithelial gland cells were proportionate to the surface epithelium, and the glandular lumen was filled with secretion. The integrity of the uterine tissue was preserved (Figure 6B).
In AMN, the ovary germinal epithelium was observed as proliferated. A high number of primordial follicles was present. A high number of corpus luteum was also present, suggesting ovulation (Figure 5E). Multiple endometrial glands and increased endometrial vascularity were present (Figure 5F). The endometrium showed general proliferation (Figure 6C).
In hUCSC + AMN, the ovary germinal epithelium was also observed as cubical-columnar cells, and the basal membrane was regular. Primordial and preantral follicles were present and intact. Additionally, several superovulated follicles were present (Figure 5G). Glandular, vascular, and connective tissue were proliferated (Figure 6D).
Penetration of human umbilical cord stem cells into uterus and ovaries (secondary outcome)
GFP and QD-marked areas were examined under a fluorescent microscope. None of the uteri gave signalling in both marked-hUCMSCs subgroups. However, the GFP-marked hUCMSCs were observed in the intrafollicular area and around oocytes (Figure 7A). In addition, a remarkable signal of QD-marked hUCMSCs in the interfollicular area and around oocytes was detected in terms of ovary penetration (Figure 7B).
Figure 7.
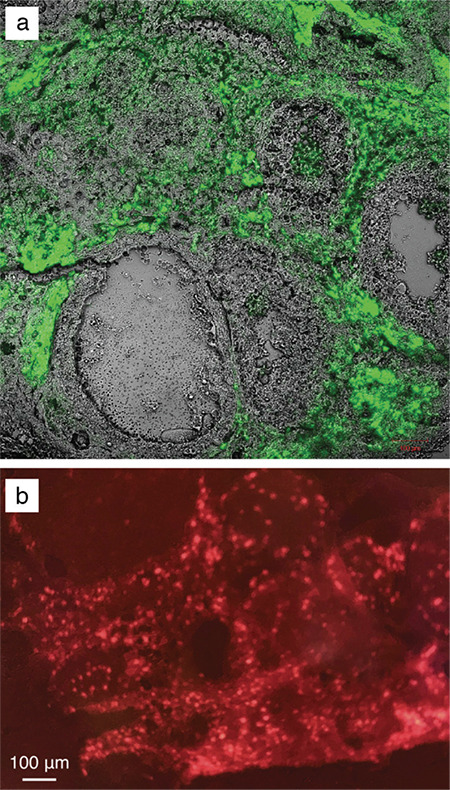
Fluorescent microscopy images of the marked-human umbilical cord stem cell applied subgroups. a) Increased signalling of green fluorescent proteins. b) Increased signalling of the quantum dot.
Macroscopic evaluations
Uterus (primary outcome)
hUCSC, AMN, and hUCSC + AMN increased the ovarian volume, fallopian tubes, uterus serosa, and peripheral vascularity, with the AMN having the greatest increase when all experimental groups were compared with CNT.
Abdominal adhesions (secondary outcome)
Macroscopic examination revealed that the talc powder caused a high degree of intra-abdominal adhesions. However, all groups were internally uniform in abdominal adhesions (Table 5) and defined according to the modified adhesion scoring scale (Table 2).
Table 5. Macroscopic adhesion scoring of the groups.

In CNT, dense adhesions between bowels, uterus, peritoneum, ovaries and residual foci of talc powder collections and the highest number of adhesions were present (Figures 8A). The least number of adhesions was observed in hUCSC (Figures 8B). AMN (Figure 8C) and hUCSC + AMN had a moderate and similar number of adhesions (Figures 8D).
Figure 8.
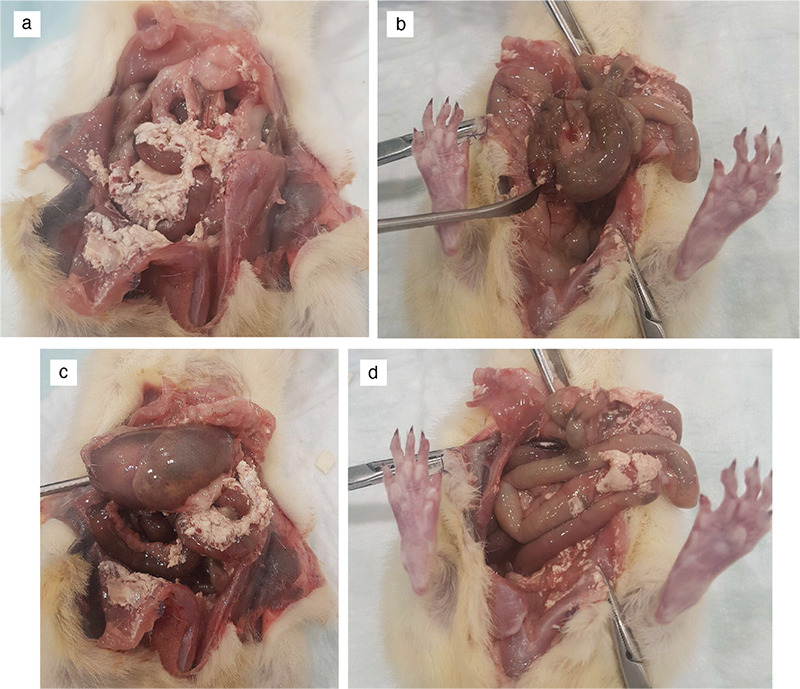
Exposed abdomens of the groups. a) The control group exhibited the highest number of intra-abdominal adhesions. b) The human umbilical cord mesenchymal stem cell (hUCMSCs)-applied group displayed the lowest number of intra-abdominal adhesions. c) The amniotic fluid (AF)-applied group showed a moderate number of intra-abdominal adhesions. d) Combined hUCMSCs and AF-applied group also demonstrated a moderate number of intra-abdominal adhesions.
Discussion
The current study evaluated the effect of hUCMSCs, AF, and a combination of both on uterus and ovaries in a rat model of abdominal adhesions. In terms of the primary outcome results regarding endometrial gland number, AMN was better than CNT and hUCSC and similar to hUCSC + AMN. In addition, AMN was better than all groups in terms of endometrial blood vessel count, primordial follicle count, and macroscopic uterus morphology (Table 3, 4). In terms of secondary outcomes, the hUCSCs penetrated the ovaries, but not the uterus. Furthermore, in terms of adhesion healing, hUCSC produced better results than groups without hUCSCs and even out-performed the combined group of hUCSC + AMN (Table 5).
Studies to prevent intra-abdominal adhesions after surgery have been ongoing since the beginning of the last century (10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35). Considering the significant postoperative complications caused by adhesions, such as second surgery, ileus, pain, intraoperative complications in further surgeries, and infertility, initiating an effective treatment is clinically available (1). Surgical techniques and principles of surgery are the initial strategies in the prevention of adhesions. Laparoscopic surgery was significantly more successful in preventing adhesions when compared to open surgery (3,5). However, the overall surgical load of adhesions is still high (1). In addition, infertility is a significant and costly complication of intra-abdominal adhesions (50,51,52,53). Therefore, prevention and successful treatment of intra-abdominal adhesions could conceivably decrease infertility.
In the current century regenerative therapy has become one of the most important emerging treatment methods for adhesions. The regenerative characteristics of hUCMSCs and AF play a significant role in treating and preventing adhesions. Additionally, several animal studies utilising AFSCs have been published (33,34,35,41). However, adult stem cells have a limited capacity for regeneration, and foetal stem cells may be ethically unacceptable. However, umbilical cord, placenta, and AF are biological waste that may have a great regenerative and cytoprotective potential with minimum ethical issues (54). Additionally, in the current study, hUCMSCs were also used for intraperitoneal application, and no adverse effects on the experimental rat gynaecological system were observed.
Bollini et al. (38) described the positive in vivo effects of cells in various organs by paracrine effect, and they claimed that these effects were performed by secretomes possessed by these cells’ membranes. The regenerative potential of the secretomes produced by the stem cells is vital in maintaining microvascular structure healing and increasing glandular structures (55). In the current study, hUCMSCs were observed to positively affect both the uterus and the ovaries histologically and morphologically. Similar to the current study’s results regarding positive regenerative effects of hUCMSCs on the uterus, Kuramoto et al. (56) found out that hUCMSCs also improve uterine incision repair in rats. hUCMSCs sheets were used and showed significantly smaller fibrotic-to-normal myometrium ratios.
Additionally, Tang et al. (57), in their rat model with intrauterine adhesions, reported that hUCMSCs transplantation significantly increased the number of endometrial glands, decreased fibrosis, and improved the proliferation of endometrial cells. The low immunogenic properties of hUCMSCs make them suitable options for repairing endometrial damage (58). Moreover, similar to the current study’s results regarding the effect of hUCMSCs on ovaries, Zhu et al. (59) showed regenerative effects of hUCMSCs on ovaries with an ovarian injury model in rats with an intraperitoneal injection of cyclophosphamide. The levels of sex hormones, oestrous cycle, and reproductive potential of the treated rats were recovered to some extent, and some transplanted rats even recovered fertility. Other studies also showed the positive effects of hUCMSCs on premature ovarian failure and ovarian dysfunction in a rat model (60,61,62,63,64). In the current study, hUCSC was better than all groups in terms of intra-abdominal adhesions. It could be because increased angiogenesis enables the delivery of more anti-inflammatory mediators (36,55).
AF contains many types of cells, including mesenchymal stem cells. Therefore, it is used as a proven resource for regenerative treatments (65,66,67,68,69,70,71). The stem cells in the AF do not possess oncogenic properties, and they could be used even in immunosuppressed rats (72).
Regenerative effects of the AF on the uterus and ovaries were observed in the current study. The current study showed that AMN was better than all groups in terms of endometrial blood vessels and primordial follicle counts. In terms of endometrial glands, it was better than CNT and hUCSC and similar to hUCSC + AMN. Positive effects of the AF on the uterus could be explained by its promotion of oestrogen receptor expression in the endometrium and uterine microenvironment regulation. Bai et al. (42) highlighted this in their study and also mentioned inhibition of fibrosis progression, promotion of proliferation, and angiogenesis in a rat model. A similar study showed that human amniotic mesenchymal cells facilitated endometrial regeneration after injury (73). Additionally, AF was observed to restore chemotherapy-induced damage to ovarian morphology (64). In the current study, AMN and hUCSC + AMN were equally effective and better than the other groups for healing of adhesions. This could be attributed to the high angiogenetic potential of AF. Hypothetically, the combination of two highly regenerative biomaterials could synergistically increase their effects. hUCSC + AMN provided positive results on the uterus and ovaries. However, it was not better than hUCSC alone nor AMN alone in all parameters. Lastly, it had an equal effect on endometrial glands and adhesion healing compared to AMN alone.
This study evaluated and compared the different effects of highly potent biomaterials such as hUCMSCs and AF on the uterus and ovaries of rats in a model of talc-induced abdominal adhesion. The increase in uterus connective tissue, endometrial glands, and improved vasculature; and increase in the number of primordial and preantral follicles in ovaries support the regenerative effects of hUCMSCs and AF on the gynaecological system. However, further studies with infertile or ovarian dysfunctional rats must be conducted to investigate the effect of biomaterials on infertility more fully.
Study Limitations
The limitations of this study are, first, the limited number of rats. Secondly, only one single adhesion agent was used. Studies with larger sample sizes with control groups researching the effects of various surgical traumas induced by suturing, electrosurgery, and abrasion on the uterus and ovaries must be conducted to further explore the regenerative effects of biomaterials.
Conclusion
The results suggest that AF, hUCMSCs, and a combination of both have a significant positive effect on the gynaecological system of experimental animals in a model of abdominal adhesion. Compared to control animals, all groups except showed significantly better results regarding the number of endometrial glands, endometrial blood vessels, and primordial follicles. AMN had the best results in the endometrial vessel and primordial follicle count and equal results with hUCSC + AMN in the endometrial glands. None of the experimental groups had any significant effect on the number of preantral follicles compared to controls.
Footnotes
Ethical Committee Approval: The ethical approval of this study was authorized by Acıbadem Mehmet Ali Aydınlar University Faculty of Medicine Animal Experiments Local Ethics Committee (approval number: 2017/37, date: 07.09.2017).
Informed Consent: Patient approval has not been obtained as it is performed on animals.
Peer-review: Externally peer-reviewed.
Author Contributions: Surgical and Medical Practices: E.G.A., G.T.; Concept: E.G.A., G.T.; Design: E.G.A., G.T.; Data Collection or Processing: E.G.A., G.T.; Analysis or Interpretation: E.G.A., G.T.; Literature Search: E.G.A., G.T.; Writing: E.G.A., G.T.
Conflict of Interest: No conflict of interest is declared by the authors.
Financial Disclosure: The authors declared that this study received no financial support.
References
- 1.Krielen P, Stommel MWJ, Pargmae P, Bouvy ND, Bakkum EA, Ellis H, et al. Adhesion-related readmissions after open and laparoscopic surgery: a retrospective cohort study (SCAR update) Lancet. 2020;395:33–41. Erratum in: Lancet 2020; 395: 272. doi: 10.1016/S0140-6736(19)32636-4. [DOI] [PubMed] [Google Scholar]
- 2.Menzies D, Ellis H. Intestinal obstruction from adhesions-How big is the problem? Ann R Coll Surg Engl. 1990;72:60–3. [PMC free article] [PubMed] [Google Scholar]
- 3.Stommel MWJ, Ten Broek RPG, Strik C, Slooter GD, Verhoef C, Grünhagen DJ, et al. Multicenter observational study of adhesion formation after open-and laparoscopic surgery for colorectal cancer. Ann Surg. 2018;267:743–8. doi: 10.1097/SLA.0000000000002175. [DOI] [PubMed] [Google Scholar]
- 4.Diamond MP, Freeman ML. Clinical implications of postsurgical adhesions. Hum Reprod Update. 2001;7:567–76. doi: 10.1093/humupd/7.6.567. [DOI] [PubMed] [Google Scholar]
- 5.Ten Broek RP, Kok-Krant N, Bakkum EA, Bleichrodt RP, van Goor H. Different surgical techniques to reduce post-operative adhesion formation: a systematic review and meta-analysis. Hum Reprod Update. 2013;19:12–25. doi: 10.1093/humupd/dms032. [DOI] [PubMed] [Google Scholar]
- 6.Yasemin A, Mehmet B, Omer A. Assessment of the diagnostic efficacy of abdominal ultrasonography and cine magnetic resonance imaging in detecting abdominal adhesions: A double-blind research study. Eur J Radiol. 2020;126:108922. doi: 10.1016/j.ejrad.2020.108922. [DOI] [PubMed] [Google Scholar]
- 7.Gopireddy DR, Soule E, Arif-Tiwari H, Sharma S, Kanmaniraja D, Jain K, et al. Spectrum of CT findings related to bowel adhesions without bowel obstruction: a comprehensive imaging review. J Clin Imaging Sci. 2020;10:80. doi: 10.25259/JCIS_126_2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Levrant SG, Bieber EJ, Barnes RB. Anterior abdominal wall adhesions after laparotomy or laparoscopy. J Am Assoc Gynecol Laparosc. 1997;4:353–6. doi: 10.1016/s1074-3804(05)80227-0. [DOI] [PubMed] [Google Scholar]
- 9.Ellis H, Moran BJ, Thompson JN, Parker MC, Wilson MS, Menzies D, et al. Adhesion-related hospital readmissions after abdominal and pelvic surgery: A retrospective cohort study. Lancet. 1999;353:1476–80. doi: 10.1016/S0140-6736(98)09337-4. [DOI] [PubMed] [Google Scholar]
- 10.Greene AK, Alwayn IP, Nose V, Flynn E, Sampson D, Zurakowski D, et al. Prevention of intra-abdominal adhesions using the antiangiogenic COX-2 inhibitor celecoxib. Ann Surg. 2005;242:140–6. doi: 10.1097/01.sla.0000167847.53159.c1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Özçelik B, Serin IS, Basburg M, Uludag S, Narin F, Tayyar M. Effect of melatonin in the prevention of post-operative adhesion formation in a rat uterine horn adhesion model. Hum Reprod. 2003;18:1703–6. doi: 10.1093/humrep/deg337. [DOI] [PubMed] [Google Scholar]
- 12.Weibel MA, Majno G. Peritoneal adhesions and their relation to abdominal surgery. A postmortem study. Am J Surg. 1973;126:345–53. doi: 10.1016/s0002-9610(73)80123-0. [DOI] [PubMed] [Google Scholar]
- 13.Parker MC, Wilson MS, Menzies D, Sunderland G, Clark DN, Knight AD, et al. The SCAR-3 study: 5-year adhesion-related readmission risk following lower abdominal surgical procedures. Color Dis. 2005;7:551–8. doi: 10.1111/j.1463-1318.2005.00857.x. [DOI] [PubMed] [Google Scholar]
- 14.Ellis H. Intraabdominal and postoperative peritoneal adhesions. J Am Coll Surg. 2005;200:643–4. doi: 10.1016/j.jamcollsurg.2004.10.023. [DOI] [PubMed] [Google Scholar]
- 15.Rodgers KE, diZerega GS. Modulation of peritoneal re-epithelialization by postsurgical macrophages. J Surg Res. 1992;53:542–8. doi: 10.1016/0022-4804(92)90104-8. [DOI] [PubMed] [Google Scholar]
- 16.Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL. Peritoneal adhesions: Etiology, pathophysiology, and clinical significance - Recent advances in prevention and management. Dig Surg. 2001;18:260–73. doi: 10.1159/000050149. [DOI] [PubMed] [Google Scholar]
- 17.Risberg B. Adhesions: preventive strategies. Eur J Surg Suppl. 1997;577:32–9. [PubMed] [Google Scholar]
- 18.Canbaz MA, Ustün C, Koçak I, Yanik FF. The comparison of gonadotropin-releasing hormone agonist therapy and intraperitoneal Ringer’s lactate solution in prevention of postoperative adhesion formation in rat models. Eur J Obstet Gynecol Reprod Bio. 1999;82:219–22. doi: 10.1016/s0301-2115(98)00230-9. [DOI] [PubMed] [Google Scholar]
- 19.Hindocha A, Beere L, Dias S, Watson A, Ahmad G. Adhesion prevention agents for gynaecological surgery: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;1:CD011254. doi: 10.1002/14651858.CD011254.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ahmad G, Kim K, Thompson M, Agarwal P, O’Flynn H, Hindocha A, et al. Barrier agents for adhesion prevention after gynaecological surgery. Cochrane Database Syst Rev. 2020;3:CD000475. doi: 10.1002/14651858.CD000475.pub4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Wei G, Wu Y, Gao Q, Zhou C, Wang K, Shen C, et al. Effect of emodin on preventing postoperative intra-abdominal adhesion formation. Oxid Med Cell Longev. 2017;2017:1740317. doi: 10.1155/2017/1740317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Cheng F, Wu Y, Li H, Yan T, Wei X, Wu G, et al. Biodegradable N, O-carboxymethyl chitosan/oxidized regenerated cellulose composite gauze as a barrier for preventing postoperative adhesion. Carbohydr Polym. 2019;207:180–90. doi: 10.1016/j.carbpol.2018.10.077. [DOI] [PubMed] [Google Scholar]
- 23.Lalountas M, Ballas KD, Michalakis A, Psarras K, Asteriou C, Giakoustidis DE, et al. Postoperative adhesion prevention using a statin-containing cellulose film in an experimental model. Br J Surg. 2012;99:423–9. doi: 10.1002/bjs.7817. [DOI] [PubMed] [Google Scholar]
- 24.Chen PC, Chen YP, Wu CC, Tseng CC, Yang CY, Hung YW, et al. A resorbable hyaluronic acid hydrogel to prevent adhesion in porcine model under laparotomy pelvic surgery. J Appl Biomater Funct Mater. 2021;19:2280800020983233. doi: 10.1177/2280800020983233. [DOI] [PubMed] [Google Scholar]
- 25.Vediappan RS, Bennett C, Cooksley C, Finnie J, Trochsler M, Quarrington RD, et al. Prevention of adhesions post-abdominal surgery: Assessing the safety and efficacy of Chitogel with Deferiprone in a rat model. PLoS One. 2021;16:e0244503. doi: 10.1371/journal.pone.0244503. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hol JC, Strik C, Chaturvedi AA, Lomme RMLM, van Goor H, Stommel MWJ, et al. The efficacy of an ultrapure alginate gel in reducing adhesion formation in a rat model of blood contamination. J Surg Res. 2019;241:271–6. doi: 10.1016/j.jss.2019.03.035. [DOI] [PubMed] [Google Scholar]
- 27.Zhang E, Guo Q, Ji F, Tian X, Cui J, Song Y, et al. Thermoresponsive polysaccharide-based composite hydrogel with antibacterial and healing-promoting activities for preventing recurrent adhesion after adhesiolysis. Acta Biomater. 2018;74:439–53. doi: 10.1016/j.actbio.2018.05.037. [DOI] [PubMed] [Google Scholar]
- 28.Almamar A, Schlachta CM, Alkhamesi NA. The systemic effect and the absorption rate of aerosolized intra-peritoneal heparin with or without hyaluronic acid in the prevention of postoperative abdominal adhesions. Surg Endosc. 2019;33:2517–20. doi: 10.1007/s00464-018-6540-2. [DOI] [PubMed] [Google Scholar]
- 29.Ha US, Koh JS, Cho KJ, Yoon BI, Lee KW, Hong SH, et al. Hyaluronic acid-carboxymethylcellulose reduced postoperative bowel adhesions following laparoscopic urologic pelvic surgery: a prospective, randomized, controlled, single-blind study. BMC Urol. 2016;16:28. doi: 10.1186/s12894-016-0149-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Zhang E, Song B, Shi Y, Zhu H, Han X, Du H, et al. Fouling-resistant zwitterionic polymers for complete prevention of postoperative adhesion. Proc Natl Acad Sci U S A. 2020;117:32046–55. doi: 10.1073/pnas.2012491117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Lai HS, Chen Y, Chang KJ, Chen WJ. Effects of octreotide on epidermal growth factor receptor, tissue plasminogen activator, and plasminogen activator inhibitor during intraperitoneal adhesion formation. J Gastroenterol. 2003;38:555–60. doi: 10.1007/s00535-002-1103-6. [DOI] [PubMed] [Google Scholar]
- 32.Soleimani A, Asgharzadeh F, Rahmani F, Avan A, Mehraban S, Fakhraei M, et al. Novel oral transforming growth factor-β signaling inhibitor potently inhibits postsurgical adhesion band formation. J Cell Physiol. 2020;235:1349–57. doi: 10.1002/jcp.29053. [DOI] [PubMed] [Google Scholar]
- 33.Nassif J, Abbasi SA, Kechli MK, Boutary SS, Ghulmiyyah L, Khalifeh I, et al. Effect of the mode of application of cryopreserved human amniotic membrane on adhesion formation after abdomino-pelvic surgery in a mouse model. Front Med (Lausanne) 2016;3:10. doi: 10.3389/fmed.2016.00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kuckelman JP, Kononchik J, Smith J, Kniery KR, Kay JT, Hoffer ZS, et al. Human-derived amniotic membrane is associated with decreased postoperative intraperitoneal adhesions in a rat model. Dis Colon Rectum. 2018;61:484–90. doi: 10.1097/DCR.0000000000001037. [DOI] [PubMed] [Google Scholar]
- 35.Nemec HM, Atalah H, Kling M, Nichols L, Powers B, Montgomery A, et al. Does human amnion membrane prevent postoperative abdominal adhesions? Am Surg. 2020;86:1038–42. doi: 10.1177/0003134820939939. [DOI] [PubMed] [Google Scholar]
- 36.Foley-Comer AJ, Herrick SE, Al-Mishlab T, Prêle CM, Laurent GJ, Mutsaers SE. Evidence for incorporation of free-floating mesothelial cells as a mechanism of serosal healing. J Cell Sci. 2002;115:1383–9. doi: 10.1242/jcs.115.7.1383. [DOI] [PubMed] [Google Scholar]
- 37.Gnecchi M, Zhang Z, Ni A, Dzau VJ. Paracrine mechanisms in adult stem cell signaling and therapy. Circ Res. 2008;103:1204–19. doi: 10.1161/CIRCRESAHA.108.176826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Bollini S, Gentili C, Tasso R, Cancedda R. The regenerative role of the fetal and adult stem cell secretome. J Clin Med. 2013;2:302–27. doi: 10.3390/jcm2040302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Mirotsou M, Jayawardena TM, Schmeckpeper J, Gnecchi M, Dzau VJ. Paracrine mechanisms of stem cell reparative and regenerative actions in the heart. J Mol Cell Cardiol. 2011;50:280–9. doi: 10.1016/j.yjmcc.2010.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Maraldi T, Bertoni L, Riccio M, Zavatti M, Carnevale G, Resca E, et al. Human amniotic fluid stem cells: neural differentiation in vitro and in vivo. Cell Tissue Res. 2014;357:1–13. doi: 10.1007/s00441-014-1840-x. [DOI] [PubMed] [Google Scholar]
- 41.Iwasaki K, Ahmadi AR, Qi L, Chen M, Wang W, Katsumata K, et al. Pharmacological mobilization and recruitment of stem cells in rats stops abdominal adhesions after laparotomy. Sci Rep. 2019;9:7149. doi: 10.1038/s41598-019-43734-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Bai X, Liu J, Yuan W, Liu Y, Li W, Cao S, et al. Therapeutic Effect of human amniotic epithelial cells in rat models of intrauterine adhesions. Cell Transplant. 2020;29:963689720908495. doi: 10.1177/0963689720908495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Zhao ZH, Ma XL, Zhao B, Tian P, Ma JX, Kang JY, et al. Naringin-inlaid silk fibroin/hydroxyapatite scaffold enhances human umbilical cord-derived mesenchymal stem cell-based bone regeneration. Cell Prolif. 2021;19:e13043. doi: 10.1111/cpr.13043. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Yang J, Chen Z, Pan D, Li H, Shen J. Umbilical cord-derived mesenchymal stem cell-derived exosomes combined pluronic F127 hydrogel promote chronic diabetic wound healing and complete skin regeneration. Int J Nanomedicine. 2020;15:5911–26. doi: 10.2147/IJN.S249129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Zhang Y, Wang WT, Gong CR, Li C, Shi M. Combination of olfactory ensheathing cells and human umbilical cord mesenchymal stem cell-derived exosomes promotes sciatic nerve regeneration. Neural Regen Res. 2020;15:1903–11. doi: 10.4103/1673-5374.280330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Chen W, Liu X, Chen Q, Bao C, Zhao L, Zhu Z, et al. Angiogenic and osteogenic regeneration in rats via calcium phosphate scaffold and endothelial cell co-culture with human bone marrow mesenchymal stem cells (MSCs), human umbilical cord MSCs, human induced pluripotent stem cell-derived MSCs and human embryonic stem cell-derived MSCs. J Tissue Eng Regen Med. 2018;12:191–203. doi: 10.1002/term.2395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chen W, Liu J, Manuchehrabadi N, Weir MD, Zhu Z, Xu HH. Umbilical cord and bone marrow mesenchymal stem cell seeding on macroporous calcium phosphate for bone regeneration in rat cranial defects. Biomaterials. 2013;34:9917–25. doi: 10.1016/j.biomaterials.2013.09.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Kouroupis D, Churchman SM, English A, Emery P, Giannoudis PV, McGonagle D, et al. Assessment of umbilical cord tissue as a source of mesenchymal stem cell/endothelial cell mixtures for bone regeneration. Regen Med. 2013;8:569–81. doi: 10.2217/rme.13.47. [DOI] [PubMed] [Google Scholar]
- 49.Ye B, Luo X, Li Z, Zhuang C, Li L, Lu L, et al. Rapid biomimetic mineralization of collagen fibrils and combining with human umbilical cord mesenchymal stem cells for bone defects healing. Mater Sci Eng C Mater Biol Appl. 2016;68:43–51. doi: 10.1016/j.msec.2016.05.104. [DOI] [PubMed] [Google Scholar]
- 50.Benyamini Y, Gozlan M, Kokia E. Variability in the difficulties experienced by women undergoing infertility treatments. Fertil Steril. 2005;83:275–83. doi: 10.1016/j.fertnstert.2004.10.014. [DOI] [PubMed] [Google Scholar]
- 51.Ranjbar F, Behboodi-Moghadam Z, Borimnejad L, Ghaffari SR, Akhondi MM. Experiences of infertile women seeking assisted pregnancy in iran: a qualitative study. J Reprod Infertil. 2015;16:221–8. [PMC free article] [PubMed] [Google Scholar]
- 52.Macaluso M, Wright-Schnapp TJ, Chandra A, Johnson R, Satterwhite CL, Pulver A, et al. A public health focus on infertility prevention, detection, and management. Fertil Steril. 2010;93:16.e1–10. doi: 10.1016/j.fertnstert.2008.09.046. [DOI] [PubMed] [Google Scholar]
- 53.Fidler AT, Bernstein J. Infertility: from a personal to a public health problem. Public Health Rep. 1999;114:494–511. doi: 10.1093/phr/114.6.494. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Loukogeorgakis SP, De Coppi P. Stem cells from amniotic fluid--potential for regenerative medicine. Best Pract Res Clin Obstet Gynaecol. 2016;31:45–57. doi: 10.1016/j.bpobgyn.2015.08.009. [DOI] [PubMed] [Google Scholar]
- 55.Song T, Zhao X, Sun H, Li X, Lin N, Ding L, et al. Regeneration of uterine horns in rats using collagen scaffolds loaded with human embryonic stem cell-derived endometrium-like cells. Tissue Eng Part A. 2015;21:353–61. doi: 10.1089/ten.tea.2014.0052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Kuramoto G, Hammad IA, Einerson BD, Allshouse AA, Debbink M, Grainger DW, et al. Human mesenchymal stem cell sheets improve uterine incision repair in a rodent hysterotomy model. Am J Perinatol. 2020. doi: 10.1055/s-0040-1721718. [DOI] [PubMed] [Google Scholar]
- 57.Tang YQ, Gan L, Xu Q, Wang S, Li JJ, Duan H. Effects of human umbilical cord mesenchymal stem cells on intrauterine adhesions in a rat model. Int J Clin Exp Pathol. 2016;9:12119–29. [Google Scholar]
- 58.Wang D, Chen K, Du WT, Han ZB, Ren H, Chi Y, et al. CD14+ monocytes promote the immunosuppressive effect of human umbilical cord matrix stem cells. Exp Cell Res. 2010;316:2414–23. doi: 10.1016/j.yexcr.2010.04.018. [DOI] [PubMed] [Google Scholar]
- 59.Zhu SF, Hu HB, Xu HY, Fu XF, Peng DX, Su WY, et al. Human umbilical cord mesenchymal stem cell transplantation restores damaged ovaries. J Cell Mol Med. 2015;19:2108–17. doi: 10.1111/jcmm.12571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Song D, Zhong Y, Qian C, Zou Q, Ou J, Shi Y, et al. Human umbilical cord mesenchymal stem cells therapy in cyclophosphamide-induced premature ovarian failure rat model. Biomed Res Int. 2016;2016:2517514. doi: 10.1155/2016/2517514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Zhang X, Zhang L, Li Y, Yin Z, Feng Y, Ji Y. Human umbilical cord mesenchymal stem cells (hUCMSCs) promotes the recovery of ovarian function in a rat model of premature ovarian failure (POF) Gynecol Endocrinol. 2021;37:353–7. doi: 10.1080/09513590.2021.1878133. [DOI] [PubMed] [Google Scholar]
- 62.Wang Z, Wei Q, Wang H, Han L, Dai H, Qian X, et al. Mesenchymal stem cell therapy using human umbilical cord in a rat model of autoimmune-induced premature ovarian failure. Stem Cells Int. 2020;2020:3249495. doi: 10.1155/2020/3249495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Elfayomy AK, Almasry SM, El-Tarhouny SA, Eldomiaty MA. Human umbilical cord blood-mesenchymal stem cells transplantation renovates the ovarian surface epithelium in a rat model of premature ovarian failure: Possible direct and indirect effects. Tissue Cell. 2016;48:370–82. doi: 10.1016/j.tice.2016.05.001. [DOI] [PubMed] [Google Scholar]
- 64.Pan Y, Zhang L, Zhang X, Hu C, Liu R. Biological and biomechanical analysis of two types of mesenchymal stem cells for intervention in chemotherapy-induced ovarian dysfunction. Arch Gynecol Obstet. 2017;295:247–52. doi: 10.1007/s00404-016-4224-5. [DOI] [PubMed] [Google Scholar]
- 65.Fuchs JR, Kaviani A, Oh JT, LaVan D, Udagawa T, Jennings RW, et al. Diaphragmatic reconstruction with autologous tendon engineered from mesenchymal amniocytes. J Pediatr Surg. 2004;39:834–8. doi: 10.1016/j.jpedsurg.2004.02.014. [DOI] [PubMed] [Google Scholar]
- 66.Kunisaki SM, Freedman DA, Fauza DO. Fetal tracheal reconstruction with cartilaginous grafts engineered from mesenchymal amniocytes. J Pediatr Surg. 2006;41:675–82. doi: 10.1016/j.jpedsurg.2005.12.008. [DOI] [PubMed] [Google Scholar]
- 67.Sun Q, Li F, Li H, Chen RH, Gu YZ, Chen Y, et al. Amniotic fluid stem cells provide considerable advantages in epidermal regeneration: B7H4 creates a moderate inflammation microenvironment to promote wound repair. Sci Rep. 2015;5:11560. doi: 10.1038/srep11560. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Sedrakyan S, Da Sacco S, Milanesi A, Shiri L, Petrosyan A, Varimezova R, et al. Injection of amniotic fluid stem cells delays progression of renal fibrosis. J Am Soc Nephrol. 2012;23:661–73. doi: 10.1681/ASN.2011030243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Rota C, Imberti B, Pozzobon M, Piccoli M, De Coppi P, Atala A, et al. Human amniotic fluid stem cell preconditioning improves their regenerative potential. Stem Cells Dev. 2012;21:1911–23. doi: 10.1089/scd.2011.0333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Prasongchean W, Bagni M, Calzarossa C, De Coppi P, Ferretti P. Amniotic fluid stem cells increase embryo survival following injury. Stem Cells Dev. 2012;21:675–88. doi: 10.1089/scd.2011.0281. [DOI] [PubMed] [Google Scholar]
- 71.Chiavegato A, Bollini S, Pozzobon M, Callegari A, Gasparotto L, Taiani J, et al. Human amniotic fluid-derived stem cells are rejected after transplantation in the myocardium of normal, ischemic, immuno-suppressed or immuno-deficient rat. J Mol Cell Cardiol. 2007;42:746–59. doi: 10.1016/j.yjmcc.2006.12.008. [DOI] [PubMed] [Google Scholar]
- 72.De Coppi P, Bartsch G Jr, Siddiqui MM, Xu T, Santos CC, Perin L, et al. Isolation of amniotic stem cell lines with potential for therapy. Nat Biotechnol. 2007;25:100–6. doi: 10.1038/nbt1274. [DOI] [PubMed] [Google Scholar]
- 73.Gan L, Duan H, Xu Q, Tang YQ, Li JJ, Sun FQ, et al. Human amniotic mesenchymal stromal cell transplantation improves endometrial regeneration in rodent models of intrauterine adhesions. Cytotherapy. 2017;19:603–16. doi: 10.1016/j.jcyt.2017.02.003. [DOI] [PubMed] [Google Scholar]