

Sir,
Nutritional supplements have the potential to induce adverse cutaneous drug eruptions (ADRs), including generalized bullous fixed drug eruption (GBFDE), maculopapular eruptions, drug rash with eosinophilia and systemic symptoms (DRESS) syndrome, bullous erythema multiforme (BEM), and Stevens–Johnson syndrome (SJS)/toxic epidermal necrolysis (TEN). Here, we share an interesting case of severe cutaneous ADRs induced by the consumption of collagen supplements in a previously healthy patient.
A 30-year-old woman presented with a 1-week history of extensive painful violaceous skin rash with blisters over the face, trunk, extremities, and mucosal surfaces. She denied intake of any medications prior to rash onset except collagen supplements, which were consumed for 1 month until 1 week before the eruption. There was no history of allergy to food or medications. On examination, she had flat targetoid lesions on the face and palms, flaccid blisters, and dusky violaceous detachable skin on the trunk [Figure 1] and extremities [Figure 2] involving approximately 25% of body surface area with positive Nikolsky sign. Oral cavity, conjunctiva long with vaginal mucosa were affected. The patient refused skin biopsy and was hospitalized with a working diagnosis of SJS/TEN overlap. SCORTEN, an illness-severity score, was 0–1. Intravenous hydrocortisone, 50 mg oral cyclosporine twice per day, and wound care management were initiated with complete resolution of lesions in 2 weeks [Figure 3].
Figure 1.
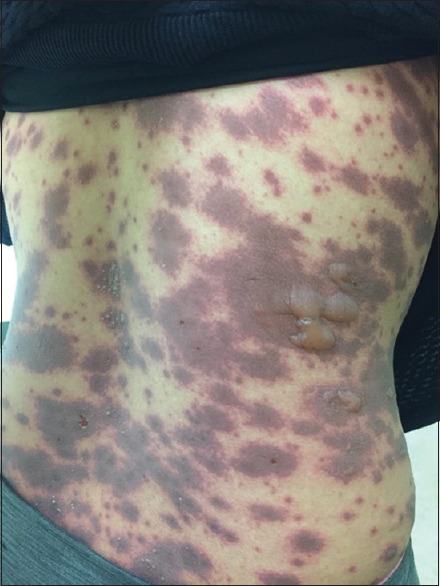
Flaccid blisters on top of dusky violaceous patches over the trunk
Figure 2.

Flaccid blisters on top of dusky violaceous patches over the upper limb
Figure 3.

Resolution of most of the skin lesions without serious consequences
SJS/TEN, GBFDE, and BEM were the initial working diagnosis in this case. The lack of biopsy posed a challenge in confirming the absolute diagnosis. Clinical judgment using diagnostic criteria made SJS/TEN superior in the list. Usually, patients with GBFDE have similar earlier reactions, absence of classical targetoid lesions, and less mucous membrane involvement (<2). On the contrary, BEM lesions are usually raised and lack prodromal symptoms. The patient presented with constitutional symptoms of fever and malaise a few days prior to cutaneous eruption. Presenting targetoid lesions were flat. Three mucous membrane surfaces were involved and the onset was new. Despite the presentation being more consistent with SJS/TEN clinically, other differentials cannot be ruled out completely without a histopathological examination. Therefore, cyclosporine was the appropriate choice for managing the three entities.[1]
Collagen supplements have not yet been reported to cause delayed drug reactions. It has been proven that fish-derived collagen can result in immediate hypersensitivity reactions.[2] However; there are no data available so far reporting delayed adverse skin reactions. Collagen refers to a family of proteins that are the primary components of connective tissue in tendons, cartilage, and skin in the human body. Due to its unique nutritional and functional properties, collagen and collagen-derived products are now widely used in the pharmaceutical, food, and cosmetic industries.[3] The main sources of commercial collagen are marine, porcine, and bovine. Marine collagen offers greater advantages compared to the land animal sources, including low immunogenicity, nonsignificant presence of biological contaminants, and higher absorption due to low molecular weight.[3]
In our patient, the source of the collagen was of marine origin. Other ingredients included zinc, acerola cherry, grape seed, red-orange complex, alpha-lipoic acid, pomegranate, and vitamin C; none of them were reported to cause delayed skin reactions. Although they presented in trace concentration, they cannot be excluded as a possible trigger of a delayed skin reaction.[4]
We encourage physicians to be observant and report any suspected reactions to collagen supplements. This will help build more evidence and knowledge about potential delayed skin reactions to collagen supplements. This will reflect in early diagnosis and timely initiation of appropriate treatment and increase awareness about the possibility of delayed skin reactions to collagen.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Ng QX, De Deyn ML, Venkatanarayanan N, Ho CY, Yeo WS. A meta-analysis of cyclosporine treatment for Stevens–Johnson syndrome/toxic epidermal necrolysis. J Inflamm Res. 2018;11:135–42. doi: 10.2147/JIR.S160964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kobayashi Y, Kuriyama T, Nakagawara R, Aihara M, Hamada-Sato N. Allergy to fish collagen: Thermostability of collagen and IgE reactivity of patients’ sera with extracts of 11 species of bony and cartilaginous fish. Allergol Int. 2016;65:450–8. doi: 10.1016/j.alit.2016.04.012. [DOI] [PubMed] [Google Scholar]
- 3.Avila Rodríguez MI, Rodriguez Barroso LG, Sánchez ML. Collagen: A review on its sources and potential cosmetic applications. J Cosmet Dermatol. 2018;17:20–6. doi: 10.1111/jocd.12450. [DOI] [PubMed] [Google Scholar]
- 4.Kirchhof MG, Miliszewski MA, Sikora S, Papp A, Dutz JP. Retrospective review of Stevens-Johnson syndrome/toxic epidermal necrolysis treatment comparing intravenous immunoglobulin with cyclosporine. J Am Acad Dermatol. 2014;71:941–7. doi: 10.1016/j.jaad.2014.07.016. [DOI] [PubMed] [Google Scholar]