

Abstract
Risankizumab is a humanized monoclonal antibody that binds the p19 subunit of interleukin-23. It is approved for treatment of moderate-severe chronic plaque psoriasis. This retrospective study included 66 consecutive adults with moderate-to-severe psoriasis vulgaris treated with risankizumab in monotherapy up to week 40 in a “real-life” setting. At week 40, 98.7%, 85.7% and 62.3% of patients achieved a Psoriasis Area and Severity Index (PASI) reduction ≥ 75% (PASI 75), PASI 90 and PASI 100, respectively. Patients who had not responded to 2 or more previous biologic treatments were significantly less likely to achieve PASI 75/90 at week 16 and PASI 90/100 at week 40 compared with those who had been previously treated with only 1 biologic, and compared with those treated with risankizumab as a first-line biologic. Increasing body mass index decreased the chances of reaching PASI 90 at week 40. No significant safety findings were recorded throughout the study, and none of the patients had to interrupt the treatment. These data suggest that the efficacy of risankizumab for plaque psoriasis in “real-life” clinical practice could differ from pivotal clinical trials data.
Key words: risankizumab, psoriasis, real-life
Psoriasis is a chronic, inflammatory disease with prominent skin manifestations, affecting 2–3% of the population worldwide (1). Biologic drugs have greatly improved psoriasis treatment outcomes, and enabled better understanding of its pathogenesis. Interleukin (IL)-23, a regulatory cytokine that is overexpressed in psoriatic skin, composed of the specific p19 subunit and the p40 subunit also shared by IL-12, is considered to be a key cytokine in the development and maintenance of chronic plaque psoriasis, as it induces the differentiation and amplification of T-helper-17 and innate immune cells, which are major sources of pro-inflammatory cytokines, such as IL-17 (2).
SIGNIFICANCE
New biologic drugs are rapidly improving outcomes of psoriasis treatment. Risankizumab (a new anti-interleukin-23 monoclonal antibody) has shown efficacy in 5 clinical trials. However, only limited evidence is available on the effectiveness and safety of risankizumab in real-life patients. The results of this study confirm that the efficacy of risankizumab is maintained over 40 weeks, while showing different therapeutic responses among different groups of patients. No safety issues were reported. These findings, which need to be confirmed by longer and larger studies, could be useful to clinicians in treating a broad cohort of patients with psoriasis.
Risankizumab, a humanized immunoglobulin G1 (IgG1) monoclonal antibody that selectively binds the p19 subunit of IL-23, was recently approved for moderate-severe chronic plaque psoriasis. Five phase 3 clinical trials (3–6) have shown superior efficacy of risankizumab to both placebo and active comparators, with the incidence of adverse events being similar across all treatment groups (2). However, real-life studies on patients treated with risankizumab are limited to case reports or studies with small numbers of participants, with the longest follow-up to date being up to 16 weeks of treatment (7). In order to establish the generalizability of clinical trials data for risankizumab, a real-life study of risankizumab efficacy and safety profiles up to week 40 was conducted.
MATERIALS AND METHODS
All selected patients received 2 subcutaneous injections of 75 mg risankizumab at weeks 0 and 4 and every 12 weeks after that, according to the summary of product characteristics (8). For each dose, the injections were performed at different anatomical sites (arms, thighs, or abdomen) and not into locations where the skin was tender, bruised, erythematous, indurated, or affected by psoriasis. Some patients self-injected the drug after receiving training in subcutaneous injection techniques.
Patients’ demographics, comorbidities, previous systemic treatments, and Psoriasis Area and Severity Index (PASI) (9) at each dermatological examination (at baseline, week 4, week 28 and week 40) were retrieved from electronic medical records. Finally, the percentages of patients achieving 75%, 90% and 100% (PASI 75, PASI 90 and PASI 100) improvement in PASI with respect to baseline PASI were registered, accounting for the PASI response percentage. Due to the study’s retrospective nature, missing data could not be retrieved. For patients who did not attend the scheduled dermatological visits and performed the injection at home or missed the injection, the PASI of the last observation carried forward (LOCF) was considered. If a dose was missed it was then administered as soon as possible. Thereafter, dosing started again at the regular scheduled time.
Safety was evaluated according to reported adverse events (AEs), including serious AEs, laboratory values (haematology, clinical chemistry, and urinalysis), physical examination, and local tolerability (swelling, induration, heat, redness, pain, or other findings at the injection site). The occurrence of AEs was collected at weeks 4, 16, 28 and 40. Routine blood chemistry tests were performed at the follow-up visits at the clinician’s discretion.
Baseline data included demographics (e.g. sex, age, body mass index (BMI)) and associated comorbidities, including psoriatic arthritis and cardiometabolic diseases (obesity, diabetes, and hypertension). The age of onset of psoriasis, disease duration, and number and type of previous systemic traditional and biologic treatments were also recorded at baseline.
Clinical assessment of the severity of psoriasis was performed at weeks 0 (baseline), 4, 16 and 28 and 40 using the PASI.
Ethical considerations
Institutional review board approval was exempted as the study protocol did not deviate from standard clinical practice. All included patients had provided written consent for retrospective study of data collected during routine clinical practice.
Statistical analysis
Data were presented as number and percentage, or mean ± standard deviation (SD) or median+interquartile range (IQR). PASIs were dichotomized with threshold 75, 90, or 100. The association of the dichotomized PASI with baseline patient’s characteristics was then explored with logistic regression analysis. Association of PASI with time, alone or corrected for baseline patient characteristics, was explored with mixed-effect regression. Pearson’s test or Spearman’s test were performed to analyse correlations. Confidence intervals (CI) were calculated. For all statistical analyses, a p-value inferior to 0.05 was considered significant. All analyses were performed with the Stata15 program.
RESULTS
Study population
A total of 77 patients were included in the study (Table I). The majority of patients were men (58 males and 18 females), and the mean (SD) age was 44 (15.6) years. Median (IQR) chronic plaque psoriasis duration was 14.5 years (7–26). Median (IQR) body mass index (BMI) at baseline was 27.8 kg/m2 (24.2–30.4). A total of 44 patients (57.1%) had at least one comorbidity. The most common comorbidities were arterial hypertension, obesity (BMI ≥ 30 kg/m2), and diabetes mellitus (27 (37.7%) patients, 14 (18.2%) patients, and 8 (10.4%) patients, respectively). Only one patient was affected by psoriatic arthritis.
Table I.
Clinical characteristics and baseline demographics of the study population
| Characteristics | Patients n = 77 |
|---|---|
| Male, n (%) | 58 (75) |
| Female, n (%) | 18 (25) |
| Age, years, mean ± SD | 44 ± 15.6 |
| Duration of psoriasis, years, median (IQR) | 14.5 (7–26) |
| BMI, kg/m2, median (IQR) | 27.8 (24.2–30.4) |
| Patients with comorbidities, n (%) | 44 (57.1) |
| Patients with CMC, n | 42 |
| Obesity, n (%) | 14 (18.2) |
| Diabetes, n (%) | 8 (10.4) |
| Arterial hypertension, n (%) | 29 (37.7) |
| Dyslipidaemia, n (%) | 4 (5.2) |
| Psoriatic arthritis, n (%) | 1 (1.3) |
| Bio-naïve, n (%) | 47 (61) |
| Exposure to previous biologics, n (%) | 30 (39) |
| 1 previous biologic | 15 (50.0) |
| 2 or more previous biologics | 15 (50.0) |
| Previous biologics, n (%) | |
| Anti-TNF | 20 (26) |
| Anti-IL 12/23 | 8 (10.4) |
| Anti-IL 17 | 18 (23.4) |
| Baseline PASI <20 | 59 (76.6) |
| Baseline PASI ≥20 | 18 (23.4) |
BMI: body mass index; TNF: tumour necrosis factor; IL: interleukin; PASI: Psoriasis Area and Severity Index; SD: standard deviation; IQR: interquartile range.
At baseline, the median (IQR) PASI was 16 (13–18), with a PASI of ≥ 20 in 18 patients (23.4%) and < 20 in 59 (76.6%) patients. A total of 47 patients (61%) were naïve to biologic therapies, and 30 (39%) had failed previous biologics therapies (bio-failure). Twenty (26%) patients had been previously administered TNF-α inhibitors, 8 (10.4%) ustekinumab, and 18 (23.4%) anti-IL17 antibodies; half of them (n = 15) had previously received 2 or more biologic agents (≥ 2 biologics). All of these 30 patients switched to risankizumab due to primary or secondary inefficacy of previous biologic drugs.
Effectiveness of risankizumab
Among the 77 enrolled patients, 2 did not attend the week 16 dermatological visit and performed the subcutaneous injection at home instead. As stated above, since no week 16 PASI was available for those 2 patients, the PASI of the LOCF was recorded. Moreover, one patient missed the week 16 visit and drug administration, although the PASI of the previous visit (LOCF) was considered.
Median (IQR) absolute PASI score decreased from 16 (13–18) at baseline to 1 (0–2) at week 16 and to 0 (0–1) at week 40, with a median PASI reduction of 93.8% at week 16 and of 100% at week 40 (p ≤ 0.001).
The results showed a significant association of PASI with time, both alone and corrected for baseline patient characteristics (sex, age, BMI, cardiometabolic comorbidities (CMC), bio-naïve, 1 biologic, ≥ 2 biologics, and baseline PASI) (p ≤ 0.001).
A significant reduction in mean PASI score was observed at both weeks 16 and 40, with an increasing proportion of patients achieving a PASI reduction of ≥ 75% (PASI 75) PASI 90 and PASI 100 throughout the 40-week study period. By week 16, 85.7% of the patients achieved PASI 75, 61% PASI 90, and 28.6% PASI 100 response, respectively. Patients reaching PASI 75, PASI 90, and PASI 100 at week 40 increased to 98.7%, 85.7% and 62.3% (Fig. 1).
Fig. 1.
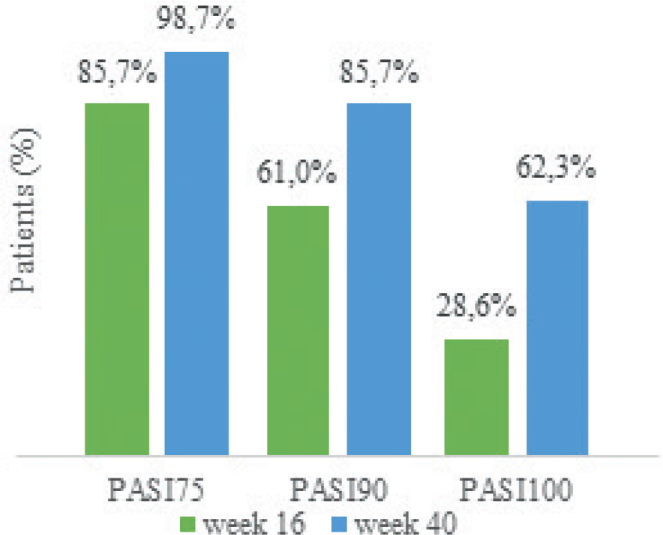
Percentages of patients treated with risankizumab achieving Psoriasis Area and Severity Index (PASI) 75, 90 and 100 responses at week 16 and week 40.
The graph in Fig. 2 shows that the percentages of patients achieving absolute PASI score ≤ 3 and ≤ 1 were approximately 84.4% and 58.4%, respectively, at week 16. Furthermore, a sustained improvement was found throughout week 40, as 96.1% of patients had a PASI score of ≤ 3 and 85.7% had an absolute PASI ≤ 1.
Fig. 2.
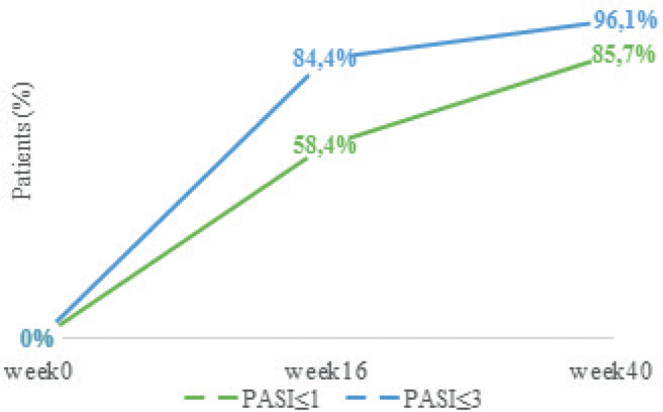
Percentages of patients achieving absolute Psoriasis Area and Severity Index (PASI) ≤3 and ≤1 at week 16 and week 28.
Logistic regression analysis
Risankizumab effectiveness in relation to sex, age, BMI, previous exposure to biologics, PASI at baseline, and cardiometabolic comorbidities is shown in Table II.
Table II.
Risankizumab effectiveness in relation to sex, age, body mass index (BMI), previous exposure to biologics, Psoriasis Area and Severity Index (PASI) at baseline, and cardiometabolic comorbidities
| Characteristics | OR (95% CI) | p-value | ||
|---|---|---|---|---|
| Week 16 | ΔPASI <75% | ΔPASI ≥75% | ||
| n = 77 | 11 | 66 | ||
| Sex, male, n (%) | 7 (63.6) | 51 (77.3) | 1.94 (0.50–7.54) | 0.337 |
| Age, years, mean ± SD | 55.1 ± 15.0 | 42.0 ± 14.9 | 0.94 (0.90–0.99) | 0.018 |
| BMI, kg/m2, median (IQR) | 30.4 (20.1–46.3) | 27.1 (19.8–39.2) | 0.87 (0.75–1.01) | 0.066 |
| Cardiometabolic comorbidities, n (%) | 7 (63.6%) | 35 (53.0%) | 0.65 (0.17–2.42) | 0.515 |
| Previous biological therapy, n (%) | ||||
| Bio-naïve | 5 (45.5) | 42 (63.6) | 1 | |
| 1 previous biologic | 1 (9.1) | 14 (21.2) | 1.66 (0.18–15.51) | 0.654 |
| ≥2 previous biologics | 5 (45.5) | 10 (15.2) | 0.24 (0.06–0.98) | 0.047* |
| Baseline PASI | 15 (8–16) | 16 (5–36) | 1.13 (0.98–1.31) | 0.093 |
| Baseline PASI (≥20) | 0 | 18 (27.3%) | – | |
| Week-16 | ΔPASI <90% | ΔPASI ≥90% | ||
| n = 77 | 30 | 47 | ||
| Sex, male, n (%) | 23 (76.7) | 35 (74.5) | 0.89 (0.30–2.59) | 0.827 |
| Age, years, mean ± SD | 46.2 ± 16.9 | 43.0 ± 14.7 | 0.99 (0.95–1.02) | 0.427 |
| BMI, kg/m2, median (IQR) | 28.1 (19.8–46.3) | 27.5 (20.0–39.2) | 0.97 (0.87–1.09) | 0.611 |
| Cardiometabolic comorbidities, n (%) | 20 (66.7) | 22 (46.8) | 0.44 (0.17–1.14) | 0.091 |
| Previous biological therapy, n (%) | ||||
| Bio-naïve | 14 (46.7) | 33 (79.2) | 1 | |
| 1 previous biologic | 7 (23.3) | 8 (17.0) | 0.48 (0.15–1.60) | 0.234 |
| ≥ 2 previous biologics | 9 (30.0) | 6 (12.8) | 0.28 (0.08–0.95) | 0.040* |
| Baseline PASI | 15 (8–27) | 16 (5–36) | 1.05 (0.97–1.14) | 0.211 |
| Baseline PASI (≥ 20) | 5 (16.7) | 13 (27.7) | 1.85 (0.62–5.54) | 0.271 |
| Week 16 | ΔPASI <100% | ΔPASI ≥100% | ||
| n = 77 | 55 | 22 | ||
| Sex, male, n (%) | 41 (74.6) | 17 (77.3) | 1.16 (0.36–3.73) | 0.802 |
| Age, years, mean ± SD | 45.2 ± 16.0 | 42.3 ± 15.0 | 0.99 (0.95–1.02) | 0.512 |
| BMI, kg/m2, median (IQR) | 28.4 (19.8–46.3) | 27.0 (20.0–36.0) | 0.95 (0.83–1.08) | 0.425 |
| Cardiometabolic comorbidities, n (%) | 33 (60.0) | 9 (40.9) | 0.46 (0.17–1.26) | 0.132 |
| Previous biological therapy, n (%) | ||||
| Bio-naïve | 33 (60.0) | 14 (63.6) | 1 | |
| 1 previous biologic | 10 (18.2) | 5 (22.7) | 1.18 (0.34–4.08) | 0.795 |
| ≥2 previous biologics | 12 (21.8) | 3 (13.6) | 0.59 (0.14–2.41) | 0.463 |
| Baseline PASI | 16 (5–36) | 15.5 (10–28) | 0.98 (0.91–1.06) | 0.669 |
| Baseline PASI (≥20) | 14 (25.5) | 4 (18.2) | 0.66 (0.20–2.16) | 0.498 |
| Week 40 | ΔPASI <75% | ΔPASI ≥75% | ||
| n = 77 | 1 | 76 | ||
| Week 40 | ΔPASI <90% | ΔPASI ≥90% | ||
| n = 77 | 11 | 66 | ||
| Sex, male, n (%) | 7 (63.4) | 51 (77.3) | 1.94 (0.50–7.54) | 0.337 |
| Age, years, mean ± SD | 53.9 ± 13.7 | 43.0 ± 15.5 | 0.96 (0.91–1.00) | 0.076 |
| BMI, kg/m2, median (IQR) | 32.0 (20.1–46.3) | 27.1 (19.8–36.8) | 0.82 (0.68–0.98) | 0.029* |
| Cardiometabolic comorbidities, n (%) | 8 (72.7) | 34 (51.5) | 0.40 (0.10–1.64) | 0.201 |
| Previous biological therapy, n (%) | ||||
| Bio-naïve | 3 (27.3) | 44 (66.7) | 1 | |
| 1 previous biologic | 1 (9.1) | 14 (21.2) | 0.95 (0.09–9.93) | 0.969 |
| ≥ 2 previous biologics | 7 (63.6) | 8 (12.1) | 0.08 (0.02–0.36) | 0.001* |
| Baseline PASI | 15 (12–36) | 16 (5–35) | 0.99 (0.90–1.09) | 0.824 |
| Baseline PASI (≥20) | 2 (18.2) | 16 (24.2) | 1.41 (0.30–6.67) | 0.662 |
| Week 40 | ΔPASI <100% | ΔPASI ≥100% | ||
| n=77 | 29 | 48 | ||
| Sex, male, n (%) | 23 (79.3) | 35 (72.9) | 0.70 (0.23–2.11) | 0.529 |
| Age, years, mean ± SD | 46.3 ± 15.6 | 43.2 ± 15.7 | 0.99 (0.95–1.02) | 0.455 |
| BMI, kg/m2, median (IQR) | 28.8 (19.8–46.3) | 27.0 (20.0–36.8) | 0.93 (0.82–1.05) | 0.228 |
| Cardiometabolic comorbidities, n (%) | 20 (69.0) | 22 (45.8) | 0.38 (0.14–1.00) | 0.051 |
| Previous biological therapy, n (%) | ||||
| Bio-naïve | 14 (48.3) | 33 (68.8) | 1 | |
| 1 previous biologic | 5 (17.2) | 10 (20.8) | 0.85 (0.24–2.94) | 0.795 |
| ≥2 previous biologics | 10 (34.5) | 5 (10.4) | 0.21 (0.06–0.73) | 0.014* |
| Baseline PASI | 16 (5–36) | 15 (6–35) | 0.96 (0.89–1.03) | 0.269 |
| Baseline PASI (≥20) | 8 (27.6%) | 10 (20.8%) | 1.81 (1.06–3.08) | 0.029* |
ΔPASI ≥75%: PASI 75; ΔPASI ≥90%: PASI 90; ΔPASI ≥100%: PASI 100; SD: standard deviation; IQR: interquartile range.
Lower percentages of patients achieving PASI 75/90/100 at weeks 16 and 40 were observed, among patients with cardiometabolic comorbidities (CMC) (i.e. hypertension, diabetes mellitus, obesity, dyslipidaemia, hyperglycaemia, hypercholesterolemia, and acute myocardial infarction) compared with patients with no CMC. The no CMC group had a higher percentage of patients who reached PASI 75/90/100 response at both weeks 16 (88.6%, 71.4% and 37.1% vs 83.3%, 52.4% and 21.4%, respectively) and 40 (100%, 91.4% and 74.3% vs 97.6%, 81% and 52.4%, respectively) compared with the CMC group. Nevertheless, from week 16 to 40, there is a consistent increase in response in both groups. Logistic regression showed, with a borderline significance, that patients with CMC had lower odds of reaching PASI 100 at week 40 compared with those without CMC (odds ratio (OR) 0.38, 95% CI 0.14–1.00, p = 0.051). Nevertheless, on bi-serial correlation the negative correlation between the presence of cardiometabolic comorbidities and the percentage PASI reduction at weeks 16 and 40 was not significant (week 16: Spearman’s rho –0.183, p = 0.111; week 40: Spearman’s rho –0.213, p = 0.063). Considering only the patients’ BMI, logistic regression showed a correlation between increased BMI and the achievement of PASI 90 at week 40. In fact, the higher the BMI, the lower were the chances that the patients would reach PASI 90 at week 40 (OR 0.82; 95% CI 0.68–0.98; p = 0.029).
With respect to PASI 75, 90 and 100 responses at both weeks 16 and 40, there was a difference in PASI percentage response rate between patients with baseline PASI < 20 and baseline PASI ≥ 20. Namely, at week 16, PASI 75 was achieved by 81.4% of the patients with baseline PASI < 20 compared with 100% of the patients with baseline PASI ≥ 20, PASI 90 was achieved by 57.6% (baseline PASI < 20) compared with 72.2% (baseline PASI ≥ 20) and PASI 100 was achieved by 30.5% (baseline PASI <20) compared with 22.2% (baseline PASI ≥ 20). At week 40 the difference in PASI percentage response between the categories decreased to 98.3% (baseline PASI < 20) vs 100% (baseline PASI ≥ 20) for PASI 75, 84.7% (baseline PASI < 20) vs 88.9% (baseline PASI ≥ 20) for PASI 90, and 64.4% (baseline PASI < 20) vs 55.6% (baseline PASI ≥ 20) for PASI 100.
Moreover, patients with baseline PASI ≥ 20 had higher odds of reaching PASI 100 at week 40 than patients with baseline PASI < 20 (OR 1.81; 95% CI 1.06–3.08; p = 0.029). Nevertheless, increased baseline PASI was not associated with higher odds of reaching PASI 75/90/100 at week 16 or 40.
Also at week 40, more patients with baseline PASI < 20 reached PASI 90 and 100, accounting for the decreased difference in PASI percentage responses between patients with baseline PASI < 20 and those with baseline PASI ≥ 20.
Patients who, before being treated with risankizumab, had been treated unsuccessfully with other biologic drugs had lower baseline PASI compared with patients that had not previously received treatment with biologics. Spearman’s analysis showed a weak negative correlation between the number of previous biologics (from 0 to 7) and the baseline PASI (Spearman’s rho –0.313 p = 0.006).
The current analysis compared patients who were naïve to biologic therapy with bio-failure patients who had failed 1, 2, or more than 2, previous biologic therapies (Fig. 3).
Fig. 3.

(A) Week 16 and (B) week 40 Psoriasis Area and Severity Index (PASI) response percentage for bio-naïve, >1 and ≥2 biologic failure patients. *p < 0.05.
Among the 30 bio-failure patients, 15 had failed just one previous biologic before starting (1 bio-failure) with risankizumab, while the other 15 patients had failed 2 or more previous biologics (≥ 2 bio-failure).
First, in all 3 groups (bio-naïve,1 bio failure, and ≥ 2 bio-failure), there is a consistent increase in PASI 90 and 100 response percentage between weeks 16 and 40. Comparing responses of patients who were bio-naïve with patients who had experienced just one previous biologic and who had experienced ≥ 2 previous biologics at both week 16 and 40, we can see that patients who had experienced ≥ 2 previous biologics had lower PASI 75, 90, and 100 response percentages (Fig. 3).
Interestingly the current analysis showed that, at almost every time-point, the ≥ 2 bio-failure status was associated with lower odds of reaching PASI 75, 90 and 100. More specifically, the negative association between the achievement of PASI 75 and the ≥ 2 bio-failure status remained statistically significant at week 16 (OR 0.24, 95% CI 0.06–0.98, p = 0.018), while the odds ratios at week 40 could not be calculated because there was only 1 patient out of 77 who had not reached PASI 75. The ≥ 2 bio-failure status was negatively associated with PASI 90 at both week 16 (OR 0.28, 95% CI 0.08–0.95; p = 0.04) and week 40 (OR 0.08, 95% CI 0.02–0.36; p = 0.001). Regarding PASI 100 at week 40, patients with ≥ 2 previous biologics status had lower odds of reaching PASI 100 (OR 0.96, 95% CI 0.06–0.73; p = 0.014).
Subgroup with week 52 follow-up
In addition, a small subgroup of patients (n = 29) reached a week 52 follow-up. Due to the small sample size, no statistical analysis of this group was performed. PASI 75, 90 and 100 responses at week 52 are shown in Fig. 4.
Fig. 4.
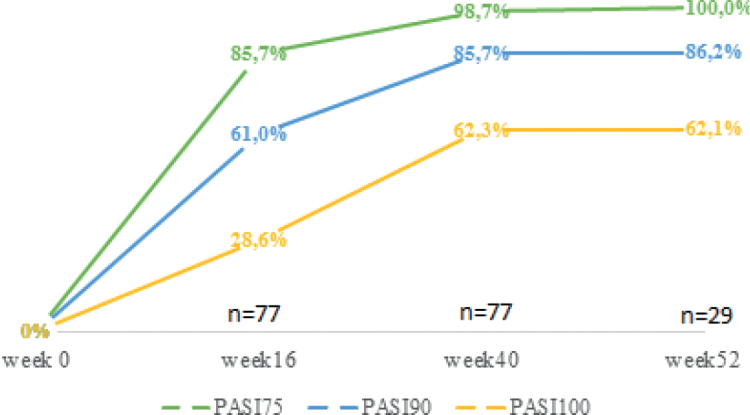
Psoriasis Area and Severity Index (PASI) responses percentages until week 52 (week 16 and 40 n = 77, week 52 n = 29).
Compared with week 40, at week 52, the patients’ PASI percentage response reached a plateau, with 100%, 86.2% and 62.1% of patients reaching PASI 75, PASI 90 and PASI 100, respectively.
Safety
Risankizumab showed no significant safety findings, and up to week 40, no side-effects were reported among all patients receiving risankizumab, and none of the 77 patients in the current study discontinued the treatment.
Although the patients received risankizumab treatment during the COVID-19 pandemic, no COVID-19-related symptoms, hospitalizations, or deaths were reported during the whole study period.
DISCUSSION
This study confirms the effectiveness of risankizumab in daily clinical practice in patients with moderate-to-severe plaque psoriasis, with the longest real-life follow-up to date. A significant reduction in median PASI was observed at both weeks 16 and 40, with an increasing proportion of patients achieving PASI 75/90/100 throughout the 40-week study period. By week 16, 85.7%, 61% and 28.6% of patients had achieved PASI 75, 90 and 100, respectively, increasing to 98.7%, 85.7% and 62.3% at week 40 (Fig. 1).
The effectiveness of risankizumab was also reflected by the percentage of patients achieving absolute PASI score ≤ 3 and ≤ 1 (84.4% and 58.4%, respectively) at week 16, with a sustained improvement throughout week 40, when 96.1% of patients had a PASI score of ≤ 3 and 85.7% had absolute PASI ≤ 1 (Fig. 2). Furthermore, the significant association of PASI with time, alone and corrected for baseline patient characteristics, might also be considered evidence of increasing effectiveness with continuous treatment with risankizumab (12).
A steady improvement in therapeutic responses was observed over the study period among all patients, with excellent rates of PASI 90 and PASI 100 responses at week 40 (85.7% and 62.3%, respectively, with a median PASI of 0 [IQR 0–1] at week 40, compared with 16 [IQR 13–18] at baseline). Moreover, in terms of absolute PASI, it is worth noting that at week 40, almost all patients (96.1%) had a PASI ≤ 3, with the majority (85.7%) reaching a PASI score of 1 or 0. This is particularly important because relative measures based on PASI reduction percentages, such as PASI 75 or PASI 90, might not always be suitable as the only parameter for therapeutic decisions or follow-up in clinical practice.
Interestingly, one patient missed the drug injection at week 16 because of the regional travel ban imposed during the COVID-19 pandemic. Although he missed one dose of risankizumab, he still achieved PASI 100 at week 40, supporting the efficacy of risankizumab. No significant safety signals were observed in the patients in the current study, as in phase 3 clinical trials, and none of the patients had to discontinue the treatment. Finally, the results of the current study on the effectiveness of risankizumab were similar to a 16-week real-life multicentre study from December 2019 to May 2020 in Central Italy (63.2% of patients reached PASI 90 and 49.1% PASI 100) (7).
Despite the negative association between cardiometabolic comorbidities, such as obesity, hypertension, diabetes, etc., and PASI 100 response of borderline significance (p = 0.051), no statistically significant association was found with the percentage of patients with or without CMC achieving PASI 75/90/100 at weeks 16 or 40. Therefore, based on the current data, we conclude that the patients’ CMC status does not significantly influence PASI response during the 40-week follow-up period.
Obesity can impair clinical response to any systemic treatments for psoriasis, including biologics. However, a broader series of studies in real clinical practice is needed to assess whether, and to what extent, BMI and obesity may influence the therapeutic response to risankizumab. Regarding this topic, a specific analysis has already been carried out for the variable weight, and the relationship with the improvement in PASI score using the data from ULTIMMA 1 and 2 trials (10–12). The results showed no significant difference in the percentage of improvement concerning the baseline value of PASI among 3 segments of BMI analysed, including BMI > 30, which is considered obesity. Another recently published 16-week real-life study reported higher PASI 75, 90, and 100 responses in patients with BMI < 25 kg/m2 (7). In the current study logistic regression showed that, at week 40, increasing BMI decreased the chances of achieving PASI 90, suggesting that, in contrast to previous studies, BMI may influence the patients’ response to risankizumab (Table II).
Previous biologic failure
An increasing number of biologics are becoming available, providing safe and effective treatment of psoriasis. Some individuals, however, remain refractory to the therapies or have a secondary loss of efficacy to the first biologic. In October 2020, a real-life retrospective study to evaluate the effectiveness, safety, and tolerability of risankizumab in patients who previously failed treatment with anti-IL-17, anti-IL12/23, or anti-IL-23 inhibitors was performed, and found risankizumab to be a promising treatment option in patients who failed various anti-IL classes, especially anti-IL-17, anti-IL-12/23 and even the other anti-IL-23 counterpart, guselkumab (13). Furthermore, another study reported a significant improvement in psoriasis in multi-failure psoriatic patients after switching from an anti-IL-17 to an anti-IL- 23 drug, suggesting that it would be reasonable to switch to an anti-IL-23 drug following the failure of an anti-IL-17 drug (14). In addition, a later real-life prospective study published in 2021, confirmed the promising results on the effectiveness and safety of risankizumab in a more challenging and real-world population composed of a high percentage of multi-bio-failure psoriatic patients (15).
It is notable that the current study found an association between patients who had failed more than 2 biologics (≥2 bio-failure) and lower probabilities of reaching PASI 75 and 90 at week 16 and PASI 90 and PASI 100 at week 40 compared with one bio-failure and bio-naïve patients. The fact that patients who had failed just one previous biologic did not have significantly decreased probabilities of reaching PASI 90 and 100 responses compared with bio-naïve patients may be linked to the fact that, as anticipated in 2009 by the British Association of Dermatologists’ guidelines, the loss of efficacy of a specific biologic may not necessarily equate to a loss of all biologics. Even though in the literature risankizumab is considered a valid treatment option for multi-bio-failure, and risankizumab showed an excellent clinical profile even in multi-failure psoriatic patients previously treated with different classes of agents (anti-TNFα, anti-IL-17, and anti-IL-12/23), we have to consider that, in patients who had failed more than 2 previous biologics, risankizumab may not be as effective as in bio-naïve and 1 bio-failure patients.
Comparing PASI responses with other randomized controlled trials
Randomized controlled trials (RCTs) are the gold standard for evaluating treatment outcomes and providing information on the “efficacy” of treatments. RCTs are conducted to assess a treatment under ideal settings without confounding factors. Therefore, they are known to have high internal validity (the extent to which a study establishes a trustworthy cause-and-effect relationship between a treatment and an outcome). The stringent and controlled settings under which RCTs are carried out result in limited generalizability, since they are performed in considerably different conditions from real-life routine care. In contrast to RCTs, real-life studies have high generalizability, but low internal validity (16).
Compared with data from phase 3 trials, the current real-life study showed slightly lower PASI 100, 90 and 75 response rates at week 16. In particular, PASI 100 was achieved by 29% (95% CI 20–40%) of patients in the current study, which is lower than that observed in UltIMMa-1 (36%), UltIMMa-2 (51%), IMMvent (40%) and IMMerge (44%). PASI 90 (61%; 95% CI 50–71%) was also lower than that observed in the phase 3 studies (ranging from 72% to 75%). Finally, PASI 75 was approximately 86% in the current study compared with 89% (95% CI 76–92%) (UltIMMa-1), 91% (UltIMMa-2), 91% (IMMvent), 89% (IMMhance) and 74% (IMMerge). Regarding the PASI 90 response at week 40, there are almost no differences between RCTs and the current study. Although the current study did not have a sufficient number of patients who reached the week 52 follow-up (n = 29), it is worth noting that the responses are similar to those seen in other RCTs. Like the RCTs (3–7), the current study had a challenging patient group; the percentage of patients who had previously failed systemic biological therapies was high (39%).
Compared with data from phase 3 trials, the current real-life study showed lower PASI 100 and PASI 90 response rates at week 16, while it had similar PASI 90 and 100 response rates at week 40. The potential difference in responses at week 16 could be due to multiple factors. First, the response to treatment is likely to differ between real-life conditions, as opposed to tightly controlled clinical trials, as also recently demonstrated by Yiu et al., who found a gap between the efficacy of ustekinumab and secukinumab in an idealized trial setting and in the real-world clinical setting in the treatment of psoriasis (10). Moreover, this difference in PASI percentage responses could also be because some patients were unable to strictly follow the schedule of the visits, as 3 patients missed their visit at week 16. Since the LOCF was considered for the missing week 16 PASI, this might account for the lower PASI 90 and PASI 100 response rates at week 16.
Despite the current data being collected during the first outbreak of the COVID-19 pandemic, in an area strongly affected by SARS-CoV-2, none of the patients experienced COVID-19-related symptoms, consistent with previously reported data on safety of biologics. Indeed, a recent study showed not significant number of hospitalizations or deaths from COVID-19 in patients affected by chronic plaque psoriasis and treated with immunosuppressive/immunomodulating biological agents (17).
Limitations and strengths
This study has some limitations, the main one being the retrospective design, which does not allow retrieval of missing data. The LOCF might have affected the variability of the results. Other significant limitations are the small size of the sample, the lack of a randomized controlled setting, the relatively short study period, and the heterogeneity of clinical assessment among clinicians from different centres.
Conclusion
The results at week 40 confirm that the efficacy of risankizumab is maintained over time, with higher therapeutic responses compared with week 16, and demonstrates the effectiveness of risankizumab in daily clinical practice in patients with moderate-to-severe plaque psoriasis, with the longest real-life follow up to-date. The failure of ≥ 2 previous biologics, BMI and baseline PASI ≥ 20, affected risankizumab effectiveness. Compared with RCTs, the current study found slightly lower PASI 75/90/100 responses at week 16, and similar PASI 90 responses at week 40, supporting risankizumab as an effective treatment in real-world conditions. Risankizumab was well tolerated, with no significant safety findings reported throughout the study. Larger and longer prospective studies and retrospective analyses of patient registries are needed to evaluate the safety and effectiveness of risankizumab further in a real-life setting.
ACKNOWLEDGEMENTS
Submission and publication fees will be covered by grants from “Fondazione Roma”, Italian Ministry of Health (Rome, Italy), ‘Ricerca Finalizzata’ project number CO-2013-02356463.
Footnotes
Conflicts of interest: RGB has been a consultant for Almirall and speaker for Abbvie. PM has been a speaker for AbbVie, Lilly, Novartis, Jannsen, Celgene, Leopharma, and Almirall. PD has been a speaker for Novartis, Abbvie, Sanofi, UCB, Janssen, Lilly, and Leopharma. AC has been a consultant and/or speaker for Abb-Vie, Almirall, Amgen, Janssen, Leo Pharma, Eli Lilly, Galderma, Boehringer, Novartis, Pfizer, Sandoz, and UCB.
REFERENCES
- 1.Gisondi P, Geat D, Pizzolato M, Girolomoni G. State of the art and pharmacological pipeline of biologics for chronic plaque psoriasis. Curr Opin Pharmacol 2019; 46: 90–99. [DOI] [PubMed] [Google Scholar]
- 2.Puig L. The role of IL 23 in the treatment of psoriasis. Expert Rev Clin Immunol 2017; 13: 525–534. [DOI] [PubMed] [Google Scholar]
- 3.Gordon KB, Strober B, Lebwohl M, Augustin M, Blauvelt A, Poulin Y, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet 2018; 392: 650–661. [DOI] [PubMed] [Google Scholar]
- 4.Reich K, Gooderham M, Thaçi D, Crowley JJ, Ryan C, Krueger JG, et al. Risankizumab compared with adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet 2019; 394: 576–586. [DOI] [PubMed] [Google Scholar]
- 5.Warren RB, Blauvelt A, Poulin Y, Beeck S, Kelly M, Wu, T, et al. Efficacy and safety of risankizumab vs. secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): results from a phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br J Dermatol 2021; 184: 50–59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Blauvelt A, Leonardi CL, Gooderham M, Papp KA, Philipp S, Wu JJ, et al. Efficacy and safety of continuous risankizumab therapy vs treatment withdrawal in patients with moderate to severe plaque psoriasis: a phase 3 randomized clinical trial. JAMA Dermatol 2020; 156: 649–658. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hansel K, Zangrilli A, Bianchi L, Peris K, Chiricozzi A, Offidani A, et al. A multicenter study on effectiveness and safety of risankizumab in psoriasis: an Italian 16-week real-life experience during the COVID-19 pandemic. J Eur Acad Dermatol Venereol 2021; 35: e169–e170. [DOI] [PubMed] [Google Scholar]
- 8.European Medicines Agency . Skyrizi (risankizumab): summary of product characteristics. 2019. [cited 2020 Nov 15]. Available from: http://www.ema.europa.eu/en/medicines/human/EPAR/skyrizi.
- 9.Fredriksson T, Pettersson U. Severe psoriasis-oral therapy with a new retinoid. Dermatologica 1978; 157: 238–244. [DOI] [PubMed] [Google Scholar]
- 10.Yiu ZZN, Mason KJ, Hampton PJ, Reynolds NJ, Smith CH, Lunt M, et al. Randomized trial replication using observational data for comparative effectiveness of secukinumab and ustekinumab in psoriasis: a study from the British Association of Dermatologists Biologics and Immunomodulators Register. JAMA Dermatol 2021; 157: 66–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Reddy V, Yang EJ, Myers B, Liao W. Clinical evaluation of risankizumab-rzaa in the treatment of plaque psoriasis. J Inflamm Res 2020; 13: 53–60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Norlin JM, Nilsson K, Persson U, Schmitt-Egenolf M. Complete skin clearance and Psoriasis Area and Severity Index response rates in clinical practice: predictors, health-related quality of life improvements and implications for treatment goals. Br J Dermatol 2020; 182: 965–973. [DOI] [PubMed] [Google Scholar]
- 13.Megna M, Fabbrocini G, Ruggiero A, Cinelli E. Efficacy and safety of risankizumab in psoriasis patients who failed anti-IL-17, anti-12/23 and/or anti IL-23: preliminary data of a real-life 16-week retrospective study. Dermatol Ther 2020; 33: e14144. [DOI] [PubMed] [Google Scholar]
- 14.Bonifati C, Morrone A, Cristaudo A, Graceffa D. Effectiveness of anti-interleukin 23 biologic drugs in psoriasis patients who failed anti-interleukin 17 regimens. A real-life experience. Dermatol Ther 2021; 34: 21–24. [DOI] [PubMed] [Google Scholar]
- 15.Megna M, Cinelli E, Gallo L, Camela E, Ruggiero A, Fabbrocini G. Risankizumab in real life: preliminary results of efficacy and safety in psoriasis during a 16-week period. Arch Dermatol Res 2021. Feb 20 [Epub ahead of print]. [DOI] [PubMed] [Google Scholar]
- 16.Crowley JJ, Warren RB, Cather JC. Safety of selective IL-23p19 inhibitors for the treatment of psoriasis. J Eur Acad Dermatol Venereol 2019; 33: 1676–1684. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gisondi P, Facheris P, Dapavo P, Conti A, Naldi L, Cazzaniga S, et al. The impact of the COVID-19 pandemic on patients with chronic plaque psoriasis being treated with biological therapy: the Northern Italy experience. Br J Dermatol 2020; 183: 373–374. [DOI] [PMC free article] [PubMed] [Google Scholar]