

Abstract
BACKGROUND:
State-level laws governing recess policies vary widely across the United States. We characterize the presence of such laws and assess their associations with child-level outcomes.
METHODS:
Presence of a state recess law was determined using the Classification of Laws Associated with School Students (CLASS) database. Parents of 6–11 y old children reported physical activity, overall health, school absences, school-related problems, and ability to make/keep friends as part of the National Survey of Children’s Health (NSCH). Logistic regression was used to compare outcomes in states with and without recess laws cross-sectionally in 2018 and between 2003 and 2011/2012 using a difference-in-differences analysis.
RESULTS:
In 2018, 20 states had a law recommending or requiring recess. Cross-sectionally, the odds of being physically active every day (odds ratio, 95% confidence interval: 2.8, 1.2–6.5) and having no difficulty making or keeping friends (2.9, 1.2–7.2) were significantly higher for children residing in states with versus without a recess law. There were no significant associations in the difference-in-differences model.
CONCLUSIONS:
Significant cross-sectional associations in 2018 were not confirmed by a difference-in-differences analysis of two waves of the NSCH. Short follow-up time and apparent weakness of existing state laws warrants further assessment of state-level recess law.
Keywords: School, elementary, CLASS, youth
Recess, a scheduled period for unstructured physical activity (PA) and play,1 is one of the only opportunities for children to participate in free-play during the otherwise structured school day. While recess is an important opportunity for PA,2–6 it also improves classroom behaviors,7–9 offers a reprieve from classroom stressors,10, 11 and affords autonomy and social-emotional development12, 13 by allowing children to navigate situations like negotiation and following rules.14 Recess allows children to participate in a variety of activities, including muscle- and bone-strengthening activities which further benefit overall physical functioning and well-being.15
Daily recess has been endorsed by the Centers for Disease Control and Prevention, the Society of Health and Physical Educators (SHAPE),15 and other national organizations.16,17 However, while national survey data from 2014 indicate that 82.8% of schools in the United States reported providing daily recess,18 increasing academic pressures and time constraints can result in reductions in provided recess time since it is not mandated.19–21 Policy implementation at the school-, district-, or state-level can ensure recess time is protected and children are provided regular recess.
As state laws governing school policies can reach virtually all children in the United States, increasing the number of states requiring regularly scheduled recess was an objective of the Healthy People 2020 program which sets national health priorities. As of 2018, 20 states have laws in place governing elementary school recess22 but the content of these laws (e.g., whether recess is required or recommended) and their association with children’s physical or psychosocial outcomes on a national level has not been determined.23 Prior research on physical education policy has demonstrated that state laws are associated with increased PA participation in adolescents,24–26 but it is unknown if state laws governing recess have similar impacts on younger children. As recess has benefits beyond promotion of PA, it is also of interest to assess the relationship between state laws governing recess with other outcomes, like children’s overall health or ability to make/keep friends.
The overarching goal of this study is to characterize state laws governing school recess, hereafter referred to as state recess policies, and assess their association with child-level outcomes through cross-sectional and difference-in-differences analyses of parent-reported data from the National Survey of Children’s Health (NSCH). More specifically, we aim to 1) characterize state recess policies as of 2018, 2) cross-sectionally compare parent reports of their child’s PA, overall health, school absences, school-related problems, and ability to make/keep friends in states with or without a recess policy in 2018, and 3) use difference-in-differences analysis to longitudinally examine the association of state policies enacted between 2003 and 2011/2012 with children’s PA, overall health, school absence, and school-related problems.
This paper addresses five hypotheses. First, presence of a state recess policy will be associated with increased odds of being physically active every day as recess contributes to daily participation2–5 and enjoyment27, 28 of PA. Second, such policies will be associated with increased odds of having optimal overall health due to the positive effects of recess on physical, emotional, and social well-being.29 Third, school absence has been used as an indicator of overall child well-being,30 so recess policy will be associated with increased odds of having zero missed school days. Fourth, recess policy will be related to increased odds of reporting no school-related problems that required contacting the child’s parent as recess has been linked to reduced externalizing behaviors and improved classroom behaviors.7–9 Finally, recess policy will be related to increased odds of children having no difficulty making/keeping friends as recess offers an opportunity for social interaction and development, cooperation, negotiation, and conflict resolution.13, 14
METHODS
In this study, we linked state-level recess policy data from the Classification of Laws Associated with School Students (CLASS) enhanced files hosted by the National Cancer Institute22 and parent-reported outcomes regarding their children from the NSCH.31 In addition to characterizing state recess policies, two analytic approaches were undertaken to compare outcomes in states with and without recess policies- a cross-sectional comparison in 2018 and a difference-in-differences analysis from 2003 to 2011/2012.
Difference-in-differences analysis is used to estimate the causal impact of policy changes over time as a quasi-experimental alternative when randomized controlled trials are not feasible and works under the assumption that changes in an outcome would be identical between groups except for the impact of the policy implementation.32 This approach has been used to estimate the effect of marijuana laws,33, 34 texting-while-driving bans,35 and same-sex marriage laws.36 Due to changes in the NSCH sampling strategy, survey mode and other methodological changes, this analysis was limited to the 2003 to 2011/2012 period. The cross-sectional analysis allowed us to examine policies that had been in place for a longer time using more recent NSCH data from 2018.
Characterization of recess policies
We compared existing state recess policies to recess policy language that is recommended by SHAPE.37 Specifically, the CLASS enhanced citation file was used to identify statewide codified policies regarding school recess in 2018 for each state and the District of Columbia (DC; hereafter referred to as a state).22 We scored the presence or absence of each SHAPE policy item, resulting in a score from 0 to 7 (policy meets none to all components outlined by SHAPE). Items were double coded to ensure reliability and discrepancies were resolved through discussion. Briefly, the SHAPE components include: requirement of daily recess, specification of a time requirement, mandating recess before lunch, ensuring the use of age-appropriate equipment that meets safety standards, provision of professional development to recess supervisors, not allowing schools to assign/withhold PA as punishment, and prohibiting schools from using recess to fulfill physical education requirements.37
Instrumentation and procedure
Child-level data were collected from the NSCH which uses a probability random sample and is representative of non-institutionalized children (less than 18 years of age) in each state. The NSCH collects information in each state about children’s physical and mental health and related factors, like access to health care and neighborhood characteristics.31 In 2003, 2007, and 2011/2012, NSCH data collection was organized by the Centers for Disease Control and Prevention’s National Center for Health Statistics and sponsored by the Maternal and Child Health Bureau (MCHB) within the Health Resources and Services Administration. Since 2016, NSCH has been conducted annually by the Census Bureau, funded by the MCHB. The detailed methodology for each year has been reported previously 31, 38, 39 but is described briefly below.
In 2018, parents of one randomly selected child from each randomly sampled household were provided a web or paper survey to be completed between June 2018 and January 2019 (‘2018’). Household served as the primary sampling unit. Strata were state and an indication of the likelihood of a child living in a household as indicated by linking administrative records with household addresses. In 2003 and 2011/2012, the NSCH was conducted as a telephone survey (landlines only in 2003 and landlines and cellphones in 2011/2012) of randomly sampled households with children younger than 18 years of age within each state. Household served as the primary sampling unit and state served as the stratum. Parents of randomly selected children in randomly sampled households completed a survey between January 2003 and August 2004 (‘2003’) or February 2011 and June 2012 (‘2011/2012’). The percent of eligible households that completed the survey or interview was 68.6% in 2003, 41.2% (cellphone) to 54.1% (landline) in 2011/2012, and 78.7% in 2018; extensive information about overall response rates have been published previously.31, 38, 39
Survey questions and response options for each year are found in Supplementary Table 2. Outcomes were dichotomized as being physically active every day (active seven days in the past week vs. not), excellent or very good health (‘optimal health’ vs. poor-to-good health), no school absences (vs. ≥ one absence), no parent contacts due to school-related problems (vs. ≥ one contact), and no difficulty making or keeping friends (vs. a little or a lot of difficulty making/keeping friends). Dichotomizing PA reflects current US PA guidelines for children calling for 60 min of moderate-to-vigorous PA every day.40 Making/keeping friends was only available in 2018.
Data analysis
For the cross-sectional analysis of 2018 data, logistic regression was used to compare outcomes of interest (physically active every day, optimal health, no school absences, no school-related problems, no problem making/keeping friends), disaggregated by states with and without a recess policy according to the CLASS enhanced data file. We controlled for child’s age (in years) and race (Black, white, or other), whether the child received free or reduced lunch in the previous year, the strength of the state’s physical education policy, years since recess policy implementation, and a fixed effect for state to account for unmeasured state-level differences, similar to prior research.41–43 The strength of the state physical education policy was retrieved from the CLASS enhanced data file (TIMEES2 variable) and classified as no policy, weak policy (state only recommends a time requirement, requires <60 min/week or no specified time requirement), or strong policy (requires 60+ min/week of physical education).44 As NSCH data collection began in June 2018, recess policies had to be enacted by the end of 2017 according to CLASS to be in effect for the beginning of the 2018 school year and considered in the cross-sectional analysis (Figure 1).
Figure 1.
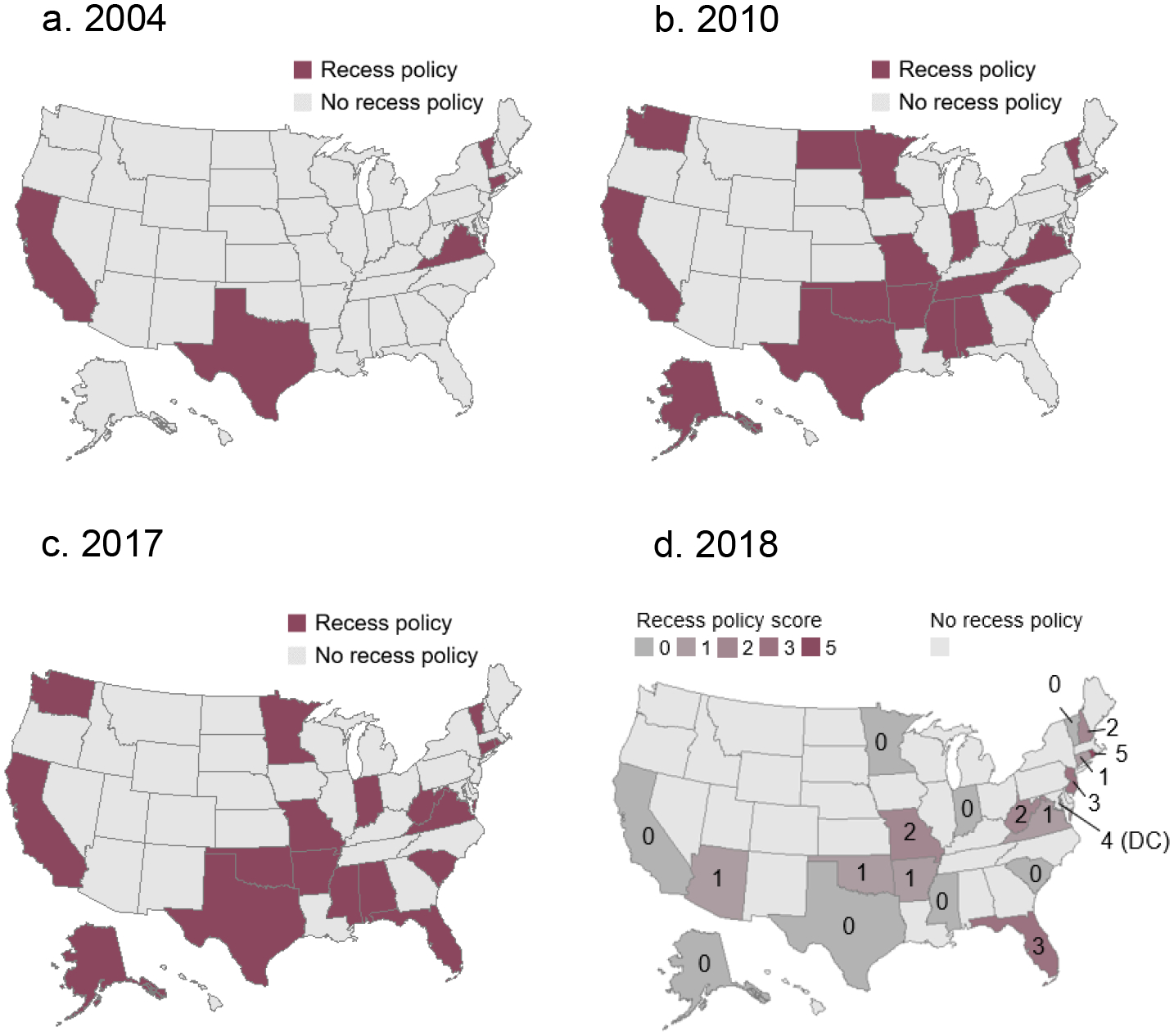
States with a Recess-Related Law Enacted by the End of 2004 (a), 2010 (b), and 2017 (c), and the Number of SHAPE Policy Items Present in States with a Policy in 2018 (d). Note that Different Classification of Laws Associated with School Students (CLASS) Data Resources Were Used for Figures a, b and c Versus d (as Discussed in Supplementary Table 1).
For the difference-in-differences analysis (2003 to 2011/2012), the five states with an existing recess policy in 2003 or 2004 (Figure 1) were excluded to allow the 2003 NSCH results to serve as baseline during which no states had an existing recess policy. Because 2011/2012 NSCH data collection started in February 2011, states implementing a policy by the end of 2010 were considered as having a policy at the 2011/2012 follow-up (Figure 1). A logistic regression model was fit for each of the outcomes of interest (physically active every day, optimal health, no school absences, no school-related problems) with the difference-in-differences estimator and fixed effects for year and state.34, 45 The parameter of interest is the difference-in-differences estimator,32 which is the interaction between a dummy variable indicating whether the state had a recess policy enacted by follow-up and a dummy variable indicating if the observation was from follow-up. The year fixed effect controls for any unmeasured trends in the outcomes over time while the state fixed effect controls for uncontrolled time-invariant differences between states. Additional covariates included child’s age, race, whether the child had free or reduced lunch in the previous year, strength of the state’s physical education policy, and years since recess policy implementation.
For both cross-sectional and difference-in-differences analyses, a sensitivity analysis was conducted with a different PA (majority of days), health (excellent), absence (missing ≥ four days), and school-related problems (>one contact) outcome to assess whether any associations were due to the definition of the outcome variable.
All analyses account for the complex survey design of the NSCH and use the provided weights. Taylor series linearization was used to estimate variance. Analyses were conducted in RStudio (Vienna Austria; version 1.3.1056) using the ‘survey’ package (version 4.0). Only 6-to-11-year-old children were included in the present analysis because recess is less commonly offered for older children.46 As the NSCH was designed to collect data on children 0–17 y of age, we used a subset function to ensure standard errors correctly accounted for the original design, as recommended in the NSCH methodology reports.39 We report Odds Ratios and 95% confidence intervals.
RESULTS
Included NSCH sample sizes were 31,117, 31,079, and 9,367 in 2003, 2011/2012, and 2018, respectively. State-specific sample sizes for each year are reported in Supplementary Table 3. Participant characteristics including age, sex, PA, overall health, school absences, school-related problems, and ability to make/keep friends for each year are shown in Table 1 for 2018 and Table 2 for 2003 and 2011/2012.
Table 1.
Participant Characteristics, Physical Activity, Overall Health, School Absences due to Illness or Injury, School-Related Problems (Number of Times Parents Contacted by School), and the Ability to Keep/Make Friends of Children in States with and Without a Recess Policy In 2018. Data are Shown as Mean or Percent ± Standard Error.
| No Policy | Policy | |
|---|---|---|
| Age (mean years) | 8.53 ± 0.04 | 8.58 ± 0.06 |
| Sex | ||
| Male (%) | 51.0 ± 1.1 | 50.9 ± 1.8 |
| Female (%) | 49.0 ± 1.1 | 49.1 ± 1.8 |
| Physical Activity | ||
| 0 days (%) | 5.3 ± 0.6 | 6.3 ± 1.0 |
| 1–3 days (%) | 37.0 ± 1.1 | 36.4 ± 1.8 |
| 4–6 days (%) | 27.7 ± 1.0 | 28.7 ± 1.6 |
| Every day (%) | 30.1 ± 1.0 | 28.7 ± 1.6 |
| Health | ||
| Excellent (%) | 66.1 ± 1.1 | 65.0 ± 1.8 |
| Very good (%) | 24.4 ± 1.0 | 25.3 ± 1.6 |
| Good (%) | 8.0 ± 0.6 | 8.3 ± 1.1 |
| Fair (%) | 1.2 ± 0.3 | 1.3 ± 0.3 |
| Poor (%) | 0.3 ± 0.2 | 0.0 ± 0.0 |
| Missed School Days | ||
| None (%) | 26.5 ± 1.1 | 29.8 ± 1.7 |
| 1–3 days (%) | 46.7 ± 1.1 | 44.4 ± 1.8 |
| 4–6 days (%) | 16.3 ± 0.8 | 16.7 ± 1.4 |
| 7–10 days (%) | 6.3 ± 0.5 | 6.0 ± 0.7 |
| 11+ days (%) | 3.7 ± 0.4 | 2.9 ± 0.5 |
| School-Related Problems | ||
| 0 contacts (%) | 69.7 ± 1.1 | 70.6 ± 1.6 |
| 1 contact (%) | 16.0 ± 0.9 | 15.7 ± 1.3 |
| 2+ contacts (%) | 14.3 ± 0.8 | 13.7 ± 1.1 |
| Keeping/Making Friends | ||
| No difficulty (%) | 77.3 ± 1.0 | 79.4 ± 1.4 |
| A little difficulty (%) | 19.2 ± 0.9 | 15.1 ± 1.2 |
| A lot of difficulty (%) | 3.6 ± 0.4 | 5.4 ± 0.8 |
Data are adjusted for the complex sampling design of the National Survey of Children’s Health
Table 2.
Participant Characteristics, Physical Activity, Overall Health, School Absences due to Illness or Injury, and School-Related Problems (Number of Times Parents Contacted by School) of Children in States with and Without a Recess Policy in 2011/2012. Data are Shown as Mean or Percent ± Standard Error.
| 2003 | 2011/2012 | |||
|---|---|---|---|---|
| No Policy | Policy* | No Policy | Policy | |
| Age (mean years) | 8.58 ± 0.02 | 8.51 ± 0.03 | 8.50 ± 0.02 | 8.51 ± 0.03 |
| Sex | ||||
| Male (%) | 51.3 ± 0.5 | 50.9 ± 0.8 | 51.1 ± 0.7 | 50.9 ± 0.9 |
| Female (%) | 48.7 ± 0.5 | 49.1 ± 0.8 | 48.9 ± 0.7 | 49.1 ± 0.9 |
| Physical Activity (mean days) | 5.37 ± 0.03 | 5.64 ± 0.03 | 5.74 ± 0.03 | 6.05 ± 0.04 |
| 0 days (%) | 6.9 ± 0.3 | 6.4 ± 0.4 | 5.5 ± 0.3 | 4.0 ± 0.4 |
| 1 days (%) | 4.5 ± 0.2 | 3.3 ± 0.3 | 3.1 ± 0.3 | 2.5 ± 0.3 |
| 2 days (%) | 11.4 ± 0.4 | 9.3 ± 0.4 | 8.1 ± 0.4 | 6.5 ± 0.5 |
| 3 days (%) | 15.1 ± 0.4 | 13.3 ± 0.5 | 12.5 ± 0.4 | 10.9 ± 0.6 |
| 4 days (%) | 12.1 ± 0.4 | 11.5 ± 0.5 | 12.6 ± 0.4 | 11.1 ± 0.6 |
| 5 days (%) | 14.6 ± 0.4 | 16.4 ± 0.5 | 17.1 ± 0.5 | 17.9 ± 0.7 |
| 6 days (%) | 4.7 ± 0.2 | 4.8 ± 0.3 | 6.5 ± 0.3 | 6.8 ± 0.5 |
| 7 days (%) | 30.6 ± 0.5 | 35.0 ± 0.7 | 34.6 ± 0.6 | 40.1 ± 0.9 |
| Health | ||||
| Excellent (%) | 62.1 ± 0.5 | 62.0 ± 0.7 | 60.3 ± 0.7 | 60.2 ± 0.9 |
| Very good (%) | 23.4 ± 0.5 | 24.3 ± 0.6 | 24.5 ± 0.6 | 24.3 ± 0.8 |
| Good (%) | 11.4 ± 0.4 | 11.3 ± 0.5 | 12.1 ± 0.5 | 12.5 ± 0.6 |
| Fair (%) | 2.7 ± 0.2 | 2.1 ± 0.2 | 2.6 ± 0.2 | 2.6 ± 0.3 |
| Poor (%) | 0.4 ± 0.1 | 0.3 ± 0.1 | 0.5 ± 0.1 | 0.4 ± 0.1 |
| Missed School Days (mean) | 4.59 ± 0.06 | 4.64 ± 0.7 | 4.72 ± 0.06 | 4.70 ± 0.09 |
| None (%) | 20.2 ± 0.5 | 20.7 ± 0.6 | 20.2 ± 0.5 | 19.8 ± 0.7 |
| School-Related Problems (mean) | 1.47 ± 0.01 | 1.46 ± 0.01 | 2.35 ± 0.05 | 2.51 ± 0.07 |
| 0 contacts (%) | 70.9 ± 0.5 | 71.3 ± 0.7 | 67.4 ± 0.6 | 66.6 ± 0.9 |
| 1 contact (%) | 11.5 ± 0.4 | 11.6 ± 0.5 | 11.1 ± 0.4 | 10.2 ± 0.6 |
| 2 contacts (%) | 17.6 ± 0.5 | 17.1 ± 0.6 | 8.5 ± 0.4 | 8.9 ± 0.5 |
Data are adjusted for the complex sampling design of the National Survey of Children’s Health.
We did not include states with a policy enacted in 2003; these are data from states that would go on to enact a policy before follow-up
Characterization of recess policies
Of the 51 states, 20 had a policy that referred to the provision of recess in 2018 (Figure 1) according to the CLASS citation file (note: different data sources were used for Figure 1a–1c so they should not be directly compared to Figure 1d). Presence of SHAPE-recommended policy components are reported in Table 3 while specific policy language can be found in Supplementary Table 4. Overall scores according to the SHAPE criteria ranged from zero (Alaska, California, Indiana, Minnesota, Mississippi, South Carolina, Texas, Vermont) to five (Rhode Island) out of a total possible seven points. Inclusion of specific SHAPE-recommended components was low as only eight states required daily recess and six specified an amount of time, ranging from 20 to 30 min a day. Three states specified that recess or PA should not be limited as punishment while one (New Jersey) specified when punishment could be used and one (DC) encouraged using PA as a reward. Six states specified that recess could not replace physical education time. Safety standards (n=1), professional development (n=2), and provision of recess before lunch (n=0) were rarely or never included in state policies.
Table 3.
Inclusion of Society of Health and Physical Educators (SHAPE) Recommended Recess Policy Components by State.
| State | Daily | Time | Lunch | Safety | Prof. Dev. | Punish. | PE | Score |
|---|---|---|---|---|---|---|---|---|
| Alaska | 0 | |||||||
| Arkansas | X | 1 | ||||||
| Arizona | X | 1 | ||||||
| California | Rec | 0 | ||||||
| Connecticut | X | 1 | ||||||
| DC | X | X | X | X | 4 | |||
| Florida | X | X | X | 3 | ||||
| Indiana | 0 | |||||||
| Minnesota | 0 | |||||||
| Missouri | X | X | 2 | |||||
| Mississippi | 0 | |||||||
| New Hampshire | Rec | X | X | 2 | ||||
| New Jersey | X | X | X | 3 | ||||
| Oklahoma | Rec | Rec | X | 1 | ||||
| Rhode Island | X | X | X | X | X | 5 | ||
| South Carolina | 0 | |||||||
| Texas | 0 | |||||||
| Virginia | X | 1 | ||||||
| Vermont | 0 | |||||||
| West Virginia | X | X | 2 | |||||
| Total | 8 | 6 | 0 | 1 | 2 | 3 | 6 |
Daily=daily recess required; Time=time requirement specified; Lunch=recess must be before lunch; Safety=requires safety standards be met; Prof. Dev.= requires annual professional development; Punish.=schools may not assign/withhold activity as punishment; PE=recess cannot fulfill physical education requirement; Rec=policy recommends instead of requires daily recess or recess of a certain duration (does not count towards score); Score= total score from 0–7.
Cross-sectional analysis in 2018
Odds ratios are reported in Table 4. The odds of being physically active every day were 2.82 times higher (95% confidence interval: 1.23–6.47) and the odds of having no difficulty making or keeping friends were 2.88 times higher (1.15–7.21) for children residing in states with a recess policy compared to those without a recess policy after controlling for covariates. The odds of having optimal health, not missing any school days, and having no school-related problems were not significantly different between states with and without a recess policy after controlling for covariates. Results of the sensitivity analysis are found in Supplementary Table 5. Of note, there was no difference in the odds of being active on the majority of days between states with and without a recess policy.
Table 4.
Adjusted Odds of Each Outcome for Children Residing in States with a Recess Law Compared to Those Living in a State Without a Recess Law (Referent Group) for the Cross-Sectional Analysis in 2018 and the Difference-in-differences Models from 2003 to 2011/2012.
| OR (95% Confidence Interval) | ||
|---|---|---|
| 2018 | 2003 to 2011/2012 | |
| Physically Active Every Day | 2.82 (1.23, 6.47) | 1.06 (0.90, 1.26) |
| Optimal Health | 1.38 (0.31, 6.23) | 0.90 (0.72, 1.12) |
| No School Absences | 1.61 (0.61, 4.26) | 0.90 (0.73, 1.11) |
| No Contacts due to School-Related Problems | 1.74 (0.72, 4.22) | 0.86 (0.72, 1.03) |
| No Difficulty Making or Keeping Friends | 2.88 (1.15, 7.21) | Not available |
OR: Odds Ratio; 2018 odds ratios are adjusted for state, length of recess policy, physical education policy, free and reduced lunch, race, and age; 2003 to 2011/2012 odds ratios are adjusted for year, state, length of recess policy, physical education policy, free and reduced lunch, race, and age
Difference-in-differences analysis from 2003 to 2011/2012
Odds ratios are reported in Table 4. The difference-in-differences parameter was not significant in any adjusted models. Thus, the odds of being physically active every day (Odds Ratio, 95% confidence interval: 1.06, 0.90–1.26), having optimal health (0.90, 0.72–1.12), having no school absences (0.90, 0.73–1.11), or having no school-related problems (0.86, 0.72–1.03) in 2003 versus 2011/2012 did not change significantly over survey iterations in the states that implemented a recess policy compared to states without a recess policy after controlling for covariates. Results of the sensitivity analysis are found in Supplementary Table 6. Of note, the odds of the school contacting the parent about an issue more than once were 33% higher in states with a recess policy compared to those without a recess policy (95% confidence interval: 1.09–1.61).
DISCUSSION
Implementation of state-level recess policy is recommended by SHAPE and was included as a Healthy People 2020 objective but less than half (n=20) of states implemented a recess policy by 2018.22 We characterize state recess policies and examine their association with children’s PA, overall health, school absence, school-related problems, and ability to make/keep friends at a population level. While we found cross-sectional associations between state recess policy and the odds of being physically active every day and having no problem making or keeping friends in 2018, we found no associations when using the more robust difference-in-differences approach on data from 2003 to 2011/2012. Overall, we found support for two of our five hypotheses.
Characterization of recess policies
State-level recess policies were generally weakly worded or non-specific47 and missing most components recommended by SHAPE.37 In 2018, only eight states required daily recess and six indicated a specific duration of recess. Some state policies simply encourage school boards or boards of education to require recess (California, Minnesota, New Hampshire, Oklahoma) or specify that PA is required and give recess as an example (Alaska, Arkansas, Indiana, Mississippi, Oklahoma, South Carolina, Texas, Vermont). Requiring PA is not the same as requiring recess as less than 70% of schools provide daily recess when PA, not recess, is required.48 Research on physical education policy supports that only strongly worded policies that specify a time requirement are effective in increasing physical education provision or participation.26, 49, 50 Lack of statistically significant associations between extant recess policies and our outcomes is consistent with the idea that weak policies have little effect.
A second issue is that existing policies do not use recess-centric language. For example, SHAPE recommends states mandate professional development of recess supervisors, but existing state policies refer to PA training generally. SHAPE’s recommended policy language also fails to be recess-centric sometimes, for example by recommending states not assign or withhold PA as punishment when a recess-centric recommendation would be to specify recess should not be withheld as punishment. Similarly, SHAPE recommends states mandate recess should not be used to meet physical education requirements. This physical education-centric language ignores the fact that physical education or PA cannot replace the purposes or benefits recess. In a recess-centric policy, the reciprocal should be mandated- physical education or PA should not be allowed to fulfill recess requirements. Overall, we find that existing state recess policies are lacking.
Cross-sectional and difference-in-differences analysis
While prior research on physical education policy has relied on cross-sectional designs,51 a strength of the present study was the inclusion of difference-in-differences analysis which incorporates information from before and after policy implementation. While the difference-in-differences analysis is generally more robust, we present the cross-sectional analysis for two reasons. First, the ability to make/keep friends was not captured in 2003 and 2011/2012, so we were unable to include this construct in the difference-in-differences analysis. Presence of cross-sectional associations between recess policy and this variable suggest that it would be of value to include this in future assessments of recess-related outcomes. Further, the policies in 2018 had been in place longer and it may be that policies, particularly weak policies, must be in place for many years before impacting child-level outcomes. The 2018 analysis also included five additional states that had to be removed from the difference-in-differences analysis to establish a no-policy baseline. As more states implement stronger recess policies, as existing policies are in place for longer, and as additional NSCH data are collected, similar follow-up research using a difference-in-differences or longitudinal approach could be conducted.
Habitual PA
Our cross-sectional analysis indicated 2.82 times higher odds of being physically active every day in children residing in states with a recess policy compared to those with no recess policy, supporting our first hypothesis. While there is no comparable research on the relationship of state recess policy with children’s PA, qualitative and cross-sectional evidence regarding state-level physical education24 or PA48 policy has also indicated positive relationships with PA participation. Implementation of school-level policies that include a recess component has also been positively associated with accelerometer-measured PA.52 Thus, state recess policy may have a positive impact on children’s PA participation, similar to other school- or state-level policies. However, these findings were not confirmed using the more robust difference-in-differences approach. Longer follow-up and assessment of the effects of policy strength are needed to resolve these contradictory results.
Ability to make/keep friends
The odds of having no difficulty making/keeping friends were 2.88 times higher in children residing in a state with a recess policy in 2018 compared to those without a policy, supporting our fifth hypothesis. Inclusion of this outcome is a strength of the present study as prior policy research, such as that on physical education, has only focused on health benefits and a need for research that considers motor skills, affective outcomes, or social outcomes has been suggested.53 While recess allows children to resolve conflicts54 and participate in social development and play with friends,13, 14 there have been no prior studies of the impact of state recess policies on this outcome. Unfortunately, this construct was not captured in the 2003 or 2011/2012 NSCH so we were unable to include it in the more robust difference-in-differences analysis. Thus, our findings must be interpreted cautiously as we cannot assess the causal effect of policy on children’s ability to make/keep friends.
Overall health, school absence, and school-related problems
There were no significant associations of state recess policy with overall health, school absences, or school-related problems in either the cross-sectional or difference-in-differences analyses. In addition to the non-specific or weak nature of state recess policy, there are other potential explanations for the lack of association. First, while the NSCH global health question is commonly used, interpretation of this question may change with age,55 making a parent’s rating of their child’s health different than a child’s actual or self-rated health. We included school absence as a less subjective indicator of child’s overall health30, 56–59 (although it was still parent-reported), but other factors, like parent support and family structure may have influenced school absence and be unaffected by recess policy.56 Alternatively, these outcomes may simply be affected to a greater extent by other policies or more proximal school variables. Future research could include more objective indicators or specific constructs that may be influenced by provision of recess, such as psychological (stress, mental restoration, externalizing disorders) or physical (weight status, metabolic health) health.
Recess policy was not associated with the odds of having no school-related problems warranting contact of the parent. However, the sensitivity analysis revealed increased odds of parents being contacted more than one time regarding school-related problems in states with a recess policy compared to those without a recess policy using the difference-in-differences analysis. This unintended consequence may be due to increased observation of bullying or other anti-social behaviors by teachers or staff on the schoolyard60 and is in line with an increase in disciplinary referrals when recess time was doubled.61 Training of recess supervisors is an important strategy for reducing bullying, facilitating positive experiences during recess,62 and promoting prosocial behaviors.63 As less than half of recess supervisors have received training,64 SHAPE recommends state policies require professional development of recess supervisors. We found that only two state recess policies mentioned this component, although these policies may be present elsewhere in state law(s). While outside the scope of the present analysis, inclusion of this component in future state recess policy may be a straightforward solution to preventing this negative consequence. Studies may also incorporate another measure, such as teacher-report, to better elucidate the impact of recess policy on classroom-specific behavioral problems.
Limitations
This paper has several limitations, notably the use of parent-reported data concerning PA, overall health, school absences, school-related problems, and ability to make/keep friends which may be subject to bias. Changes in NSCH methodology (e.g., inclusion of cellphones and landlines in 2011/2012 versus only landlines in 2003) and reduced response rates due to declining interest in completing phone interviews may have influenced our findings although NSCH has analyzed and accounted for potential nonresponse bias in their survey weighting scheme.31, 38, 39 We used both cross-sectional and difference-in-differences analysis to address limitations in the available NSCH data. We postulated that we found associations using the cross-sectional, but not the difference-in-differences analysis because recess policies in 2018 had been in place longer and/or may have been more strongly worded than earlier policies. However, we are unable to examine the actual impact of the strength of policy wording or the time since policy implementation due to lack of surveillance data and the small number of state policies. The current NSCH format has been used since 2016, so future research may use updated NSCH data as states implement new policies or strengthen existing policies. Additionally, we had no information about the school type (e.g., public vs. private) or grade level so were unable to limit our analysis to elementary school students, for example.
We focused on state policies, but there may be policies at other levels such as the school,64 school district65 or guidelines from the Board of Education that influence recess provision. Research on recess provision23 and withholding PA as punishment66 demonstrates that state policy has an independent effect from district policy but this has not been examined regarding the impact of recess policy on child-level outcomes. We also have no information about policy adherence/implementation. While prior research is limited, one study indicated that state policy increased the odds of provision of recess23 but there is varying degrees of policy adoption67 and may even be differences in policy adherence by region within a state.68
Conclusions
Our study adds to the limited literature on the impact of state recess policies on children’s PA, overall health, school absence, school-related problems, and the ability to make/keep friends. While we report positive cross-sectional associations between state policy and the odds of being active every day or having no difficulty making/keeping friends, these findings were not replicated in the more robust difference-in-differences analysis. Follow-up studies investigating the relationship of state recess policy with both PA and other outcomes, like social or mental health, should be conducted as states implement stronger recess policies.
IMPLICATIONS FOR SCHOOL HEALTH
The present study provides preliminary evidence that overall state recess policy can benefit children’s PA and ability to make/keep friends. Less than half of states had a school recess policy in 2018 and existing policies were weakly worded and did not adhere to the guidance set forth by SHAPE America. State policy makers should strive to implement and/or update existing state recess policies which better adhere to this guidance, for example, by requiring daily recess of a specific duration.
Supplementary Material
ACKNOWLEDGEMENTS
This work was supported through funding by the Cancer Prevention Fellowship Program, Division of Cancer Prevention, National Cancer Institute at the National Institutes of Health.
Footnotes
Human Subjects Approval Statement
The study involved secondary analyses of publicly available state law and deidentified data and therefore did not entail human subjects research.
Conflict of Interest Disclosure Statement
All authors of this article declare they have no conflicts of interest. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Cancer Institute or the National Institutes of Health.
Contributor Information
Kimberly A. Clevenger, Health Behaviors Research Branch, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, 9609 Medical Centre Dr, Rockville, MD 20850.
Frank M. Perna, Health Behaviors Research Branch, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, 9609 Medical Centre Dr, Rockville, MD 20850.
Richard P. Moser, Office of the Associate Director, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, 9609 Medical Centre Dr, Rockville, MD 20850.
David Berrigan, Health Behaviors Research Branch, Behavioral Research Program, Division of Cancer Control and Population Sciences, National Cancer Institute, 9609 Medical Centre Dr, Rockville, MD 20850.
REFERENCES
- 1.Institute of Medicine. Educating the Student Body: Taking Physical Activity and Physical Education to School. Washington DC: The National Academies Press; 2013. [PubMed] [Google Scholar]
- 2.Erwin H, Abel M, Beighle A, Noland MP, Worley B, Riggs R. The contribution of recess to children’s school-day physical activity. J Phys Act Health. 2012;9(3):442–448. [DOI] [PubMed] [Google Scholar]
- 3.Brusseau TA, Kulinna PH, Tudor-Locke C, Ferry M, Van Der Mars H, Darst PW. Pedometer-determined segmented physical activity patterns of fourth-and fifth-grade children. J Phys Act Health. 2011;8(2):279–286. [DOI] [PubMed] [Google Scholar]
- 4.Tudor-Locke C, Lee SM, Morgan CF, Beighle A, Pangrazi RP. Children’s pedometer-determined physical activity during the segmented school day. Med Sci Sports Exerc. 2006;38(10):1732–1738. [DOI] [PubMed] [Google Scholar]
- 5.Ridgers ND, Timperio A, Crawford D, Salmon J. Five-year changes in school recess and lunchtime and the contribution to children’s daily physical activity. Br J Sports Med. 2012;46(10):741–746. [DOI] [PubMed] [Google Scholar]
- 6.Guinhouya BC, Lemdani M, Apété GK, Durocher A, Vilhem C, Hubert H. How school time physical activity is the “big one” for daily activity among schoolchildren: a semi-experimental approach. J Phys Act Health. 2009;6(4):510–519. [DOI] [PubMed] [Google Scholar]
- 7.Barros RM, Silver EJ, Stein RE. School recess and group classroom behavior. Pediatrics. 2009;123(2):431–436. [DOI] [PubMed] [Google Scholar]
- 8.Ridgway A, Northup J, Pellegrini A, LaRue R, Hightsoe A. Effects of recess on the classroom behavior of children with and without attention-deficit hyperactivity disorder. Sch Psychol Q. 2003;18(3):253–268. [Google Scholar]
- 9.Stapp AC, Karr JK. Effect of recess on fifth grade students’ time on-task in an elementary classroom. Int Electron J Elementary Educ. 2018;10(4):449–456. [Google Scholar]
- 10.Ramstetter C, Murray R. Time to play: recognizing the benefits of recess. American Educator. 2017;41(1):17–23. [Google Scholar]
- 11.Woods AM, McLoughlin GM, Kern BD, Graber KC. What’s physical activity got to do with it? Social trends in less active students at recess. J Sch Health. 2018;88(7):500–507. [DOI] [PubMed] [Google Scholar]
- 12.Haapala HL, Hirvensalo MH, Laine K, Laakso L, Hakonen H, Kankaanpää, et al. Recess physical activity and school-related social factors in Finnish primary and lower secondary schools: cross-sectional associations. BMC Public Health. 2014;14(1):1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Prompona S, Papoudi D, Papadopoulou K. Play during recess: primary school children’s perspectives and agency. Education 3–13. 2020;48(7):765–778. [Google Scholar]
- 14.Stanley RM, Boshoff K, Dollman J. Voices in the playground: a qualitative exploration of the barriers and facilitators of lunchtime play. J Sci Med Sport. 2012;15(1):44–51. [DOI] [PubMed] [Google Scholar]
- 15.Centers for Disease Control and Prevention and SHAPE America. Strategies for Recess in Schools. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2017. [Google Scholar]
- 16.Murray R, Ramstetter C. The crucial role of recess in school. Pediatrics. 2013;131(1):183–188. [DOI] [PubMed] [Google Scholar]
- 17.National Association for Sport and Physical Education (NASPE). Recess for Elementary School Students. Reston, VA: NASPE; 2006. [Google Scholar]
- 18.Centers for Disease Control and Prevention. School Health Policies and Practices Study 2014 Overview. 2014. Available at: https://www.cdc.gov/healthyyouth/data/shpps/pdf/2014factsheets/2014_overview_fact_sheet.pdf. Accessed October 20, 2021.
- 19.McMurrer J. Choices, Changes, and Challenges: Curriculum and Instruction in the NCLB Era. Washington DC: Center on Education Policy Press; 2007. [Google Scholar]
- 20.Bohn-Gettler CM, Pellegrini AD. Chapter 12: Recess in primary school: the disjuncture between educational policy and scientific research. In: Bornstein B, Wiener R, eds. Justice, Conflict and Wellbeing. New York, NY: Springer; 2014:313–336. [Google Scholar]
- 21.Simon JB, Childers H. Principals’ perceptions of school recess: sources of information, benefits, and drawbacks. Research in the Schools. 2006;13(2):37–46. [Google Scholar]
- 22.National Cancer Institute. Classification of Laws Associated with School Students. 2008. Available at: https://class.cancer.gov/. Accessed October 20, 2021.
- 23.Slater SJ, Nicholson L, Chriqui J, Turner L, Chaloupka F. The impact of state laws and district policies on physical education and recess practices in a nationally representative sample of US public elementary schools. Arch Pediatr Adolesc Med. 2012;166(4):311–316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Lin W, Leider J, Shang C, Hennessy E, Perna FM, Chriqui JF. The association between state physical education laws and student physical activity. Am J Prev Med. 2020;58(3):436–445. [DOI] [PubMed] [Google Scholar]
- 25.Cawley J, Meyerhoefer C, Newhouse D. The impact of state physical education requirements on youth physical activity and overweight. Health Econ. 2007;16(12):1287–1301. [DOI] [PubMed] [Google Scholar]
- 26.Taber DR, Chriqui JF, Perna FM, Powell LM, Slater SJ, Chaloupka F. Association between state physical education (PE) requirements and PE participation, physical activity, and body mass index change. Prev Med. 2013;57(5):629–633. [DOI] [PubMed] [Google Scholar]
- 27.Eberline A, Judge LW, Walsh A, Hensley LD. Relationship of enjoyment, perceived competence, and cardiorespiratory fitness to physical activity levels of elementary school children. Physical Educator. 2018;75(3):394–413. [Google Scholar]
- 28.Massey WV, Szarabajko A, Thalken J, Perez D, Mullen SP. Memories of school recess predict physical activity enjoyment and social-emotional well-being in adults. Psychol Sport Exerc. 2021;55(101948):1–9. [Google Scholar]
- 29.Pellegrini AD, Holmes RM. Chapter 3: The role of recess in primary school. In: Singer DG, Golinkoff RM, Hirsh-Pasek K, eds. Play = Learning: How Play Motivates and Enhances Children’s Cognitive and Social-Emotional Growth. Oxford, UK: Oxford; 2006:36–53. [Google Scholar]
- 30.Chen L, Jennison BL, Yang W, Omaye ST. Elementary school absenteeism and air pollution. Inhal Toxicol. 2000;12(11):997–1016. [DOI] [PubMed] [Google Scholar]
- 31.US Census Bureau. 2018 National Survey of Children’s Health Methodology Report. 2019. Available at: https://www2.census.gov/programs-surveys/nsch/technical-documentation/methodology/2018-NSCH-Methodology-Report.pdf. Accessed October 20, 2021.
- 32.Wing C, Simon K, Bello-Gomez R. Designing difference in difference studies: best practices for public health policy research. Annu Rev Public Health. 2018;39:453–469. [DOI] [PubMed] [Google Scholar]
- 33.Harper S, Strumpf EC, Kaufman JS. Do medical marijuana laws increase marijuana use? Replication study and extension. Ann Epidemiol. 2012;22(3):207–212. [DOI] [PubMed] [Google Scholar]
- 34.Coley RL, Hawkins SS, Ghiani M, Kruzik C, Baum CF. A quasi-experimental evaluation of marijuana policies and youth marijuana use. Am J Drug Alcohol Abuse. 2019;45(3):292–303. [DOI] [PubMed] [Google Scholar]
- 35.Ferdinand AO, Menachemi N, Sen B, Blackburn JL, Morrisey M, Nelson L. Impact of texting laws on motor vehicular fatalities in the United States. Am J Public Health. 2014;104(8):1370–1377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Raifman J, Moscoe E, Austin SB, McConnell M. Difference-in-differences analysis of the association between state same-sex marriage policies and adolescent suicide attempts. JAMA Pediatr. 2017;171(4):350–356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.SHAPE America. Guide for Recess Policy. 2016. Available at: https://www.shapeamerica.org/advocacy/upload/Guide-for-Recess-Policy.pdf. Accessed October 20, 2021.
- 38.Blumberg SJ. Design and operation of the National Survey of Children’s Health, 2003. Vital Health Stat. 2005;1(43):1–131. [PubMed] [Google Scholar]
- 39.Bramlett MD, Blumberg SJ, Zablotsky B, George JM, Ormson AE, Frasier AM, et al. Design and operation of the National Survey of Children’s Health, 2011–2012. Vital Health Stat. 2017;1(59):1–256. [PubMed] [Google Scholar]
- 40.Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Cawley J, Meyerhoefer C, Newhouse D. The correlation of youth physical activity with state policies. Contemp Econ Policy. 2007;25(4):506–517. [Google Scholar]
- 42.An R, Ji M, Clarke C, Guan C. Impact of state laws governing physical education on attendance among US high school students, 2003 to 2017. Am J Health Promot. 2019;33(8):1144–1151. [DOI] [PubMed] [Google Scholar]
- 43.Dills AK, Morgan HN, Rotthoff KW. Recess, physical education, and elementary school student outcomes. Econ Educ Rev. 2011;30(5):889–900. [Google Scholar]
- 44.Mâsse LC, Chriqui JF, Igoe JF, Atienza AA, Kruger J, Kohl HW, et al. Development of a physical education–related state policy classification system (PERSPCS). Am J Prev Med. 2007;33(4):S264–S276. [DOI] [PubMed] [Google Scholar]
- 45.Puhani PA. The treatment effect, the cross difference, and the interaction term in nonlinear “difference-in-differences” models. Econ Lett. 2012;115(1):85–87. [Google Scholar]
- 46.Centers for Disease Control and Prevention. Results from the School Health Policies and Practices Study 2014. 2014. Available at: https://www.cdc.gov/healthyyouth/data/shpps/pdf/SHPPS-508-final_101315.pdf. Accessed October 20, 2021.
- 47.Carlson JA, Sallis JF, Chriqui JF, Schneider L, McDermid LC, Agron P. State policies about physical activity minutes in physical education or during school. J Sch Health. 2013;83(3):150–156. [DOI] [PubMed] [Google Scholar]
- 48.Evenson KR, Ballard K, Lee G, Ammerman A. Implementation of a school‐based state policy to increase physical activity. J Sch Health. 2009;79(5):231–238. [DOI] [PubMed] [Google Scholar]
- 49.Perna FM, Oh A, Chriqui JF, Mâsse LC, Atienza AA, Nebeling L, et al. The association of state law to physical education time allocation in US public schools. Am J Public Health. 2012;102(8):1594–1599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Cawley J, Frisvold D, Meyerhoefer C. The impact of physical education on obesity among elementary school children. J Health Econ. 2013;32(4):743–755. [DOI] [PubMed] [Google Scholar]
- 51.Kim J Are physical education‐related state policies and schools’ physical education requirement related to children’s physical activity and obesity? J Sch Health. 2012;82(6):268–276. [DOI] [PubMed] [Google Scholar]
- 52.Cradock AL, Barrett JL, Carter J, McHugh A, Sproul J, Russo ET, et al. Impact of the Boston active school day policy to promote physical activity among children. Am J Health Promot. 2014;28(suppl 3):S54–S64. [DOI] [PubMed] [Google Scholar]
- 53.Landi D, Walton-Fisette JL, Sutherland S. Physical education policy research in the united states: setting a new orientation. Quest. 2021;73(1):45–62. [Google Scholar]
- 54.Powell M The hidden curriculum of recess. Child Youth Environ. 2007;17(4):86–106. [Google Scholar]
- 55.Jylhä M What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc Sci Med. 2009;69(3):307–316. [DOI] [PubMed] [Google Scholar]
- 56.Gubbels J, van der Put CE, Assink M. Risk factors for school absenteeism and dropout: a meta-analytic review. J Youth Adolesc. 2019;48(9):1637–1667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Vish NL, Stolfi A. Relationship of children’s emotional and behavioral disorders with health care utilization and missed school. Acad Pediatr. 2020;20(5):687–695. [DOI] [PubMed] [Google Scholar]
- 58.Taras H, Potts‐Datema W. Obesity and student performance at school. J Sch Hlth. 2005;75(8):291–295. [DOI] [PubMed] [Google Scholar]
- 59.Centeio EE, Cance JD, Barcelona JM, Castelli DM. Relationship between health risk and school attendance among adolescents. Am J Health Educ. 2018;49(1):28–32. [Google Scholar]
- 60.Glew GM, Fan M-Y, Katon W, Rivara FP, Kernic MA. Bullying, psychosocial adjustment, and academic performance in elementary school. Arch Pediatr Adolesc Med. 2005;159(11):1026–1031. [DOI] [PubMed] [Google Scholar]
- 61.Erwin H, Fedewa A, Wilson J, Ahn S. The effect of doubling the amount of recess on elementary student disciplinary referrals and achievement over time. J Res Child Educ. 2019;33(4):592–609. [Google Scholar]
- 62.Pellegrini AD. The recess debate: a disjuncture between educational policy and scientific research. Am J Play. 2008;1(2):181–191. [Google Scholar]
- 63.Mayfield CA, Child S, Weaver RG, Zarrett N, Beets MW, Moore JB. Effectiveness of a playground intervention for antisocial, prosocial, and physical activity behaviors. J Sch Health. 2017;87(5):338–345. [DOI] [PubMed] [Google Scholar]
- 64.Thalken J, Massey WV, Szarabajko A, Ozenbaugh I, Neilson L. From policy to practice: examining the role of recess in elementary school. Public Health in Pract. 2021;100091:1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Chierici M, Powell E, Manes R. Time To Play. 2013. Available at: https://www.jumpinforhealthykids.org/userfiles/file/news/DASH-NY_Mandatory_Daily_Active_Recess_Guide.pdf. Accessed October 20, 2021.
- 66.Turner L, Chriqui JF, Chaloupka FJ. Withholding recess from elementary school students: policies matter. J Sch Health. 2013;83(8):533–541. [DOI] [PubMed] [Google Scholar]
- 67.Lounsbery MA, McKenzie TL, Morrow JR Jr, Monnat SM, Holt KA. District and school physical education policies: implications for physical education and recess time. Ann Behav Med. 2013;45(suppl 1):S131–S141. [DOI] [PubMed] [Google Scholar]
- 68.Kelder SH, Springer AE, Barroso CS, Smith CL, Sanchez E, Ranjit N, et al. Implementation of Texas Senate Bill 19 to increase physical activity in elementary schools. J Public Health Pol. 2009;30(1):S221–S247. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.