

Abstract
Background and Objectives:
Conventionally, stainless steel crown (SSC) is the preferred material for the restoration of pulpotomized primary molars. However, in situations where stainless steel cannot be used necessity for other restorative material arises.
Aim:
The aim of this study is to assess the microleakage of several coronal seal materials in pulpotomized primary molars– in vitro.
Methodology:
Seventy-five primary molars were prepared with proximo-occlusal cavities. Restoration was done with Zinc oxide eugenol cement, SSC, composite resin, resin-modified glass-ionomer cement (GIC), and amalgam. Microleakage was assessed using dye penetration technique with stereomicroscope and scanning electron microscope.
Statistical Analysis and Results:
The Kruskal–Wallis and Mann–Whitney tests were used to statistically analyze the results.
Conclusion:
With regard to this present study composite resin and resin-modified GIC offers a good alternative for SSC.
KEYWORDS: Microleakage, pulpotomy, sealing ability
INTRODUCTION
The treatment of choice for large caries with pulp involvement is pulpotomy which eliminates active disease and retains the tooth in a functional state.[1]
In general, SSC is the preferred material for the restorations of pulpotomized primary molars.[2] The parents express concerns about esthetics after SSC placement on children's teeth.[3]
With any restorative material treatment, success depends on the presence of leakage-free margins.[4]
Hence, this study was performed with the aim of assessing the microleakage among four groups of coronal seal material and also between each set of restorative material with the control group.
METHODOLOGY
Seventy-five human primary molars with at least three intact surfaces, exfoliated, or extracted were used for this study. Teeth were debrided and stored in distilled water for not more than 3 months.
Proximo-occlusal cavity preparations and access to pulp chamber were made under water coolant. Pulp chamber was deroofed and normal saline irrigation done [Figure 1].
Figure 1.

Pulpotomy procedure done
Teeth were randomly segregated into 5 sets. Before restoration:
Teeth were mounted on a 2 cm thickness wax and air-dried
A tofflemire matrix holder with a 0.5 mm thick metal matrix strip was adapted to the tooth. Teeth were restored as follows.
Group 1
Zinc oxide eugenol (ZOE) was filled till occlusal surface.
Group 2
ZOE lining and resin-modified glass-ionomer cement (GIC) was placed till occlusal surface.
Group 3
ZOE followed by 1 mm of type I GIC lining was placed which was etched and bonded. Composite was placed incrementally till occlusal surface.
Group 4
ZOE lining and silver amalgam were condensed till the occlusal surface.
Group 5
ZOE followed by type II GIC restoration over which SSC was cemented using type I GIC luting cement (control group) [Figure 2].
Figure 2.

Group 5 stainless steel crown placed
After preparation, samples were thermocycled at 5°C/55°C with 30 s dwell time for 200 cycles. The entire tooth excluding the restorations and 1 mm margin was covered with two layers of nail varnish. Afterward, specimens were immersed for 24 h in 0.5% basic fuchsine and washed under tap water. Using a diamond disc, each specimen was sectioned mesiodistally through the restoration.
Using a stereomicroscope of ×20 the specimens were examined for the signs of dye penetration [Figure 3]. The following criteria were used:[5]
Figure 3.
Group 5 showing no leakage (Steriomicroscope)
No leakage = 0
Leakage at the occlusal surface only = 1
Leakage at the cervical surface only = 2
Leakage at occlusal and cervical margins = 3
Continuous leakage at both cervical and occlusal aspects = 4.
Randomly selected three specimens from each group were gold sputter-coated and examined under a scanning electron microscope the highest leakage score for each tooth was recorded. The Kruskal–Wallis and Mann–Whitney tests had been used to analyze the results.
RESULTS
Remarkable differences between various sets (P < 0.0001) were demonstrated by the Kruskal–Wallis test. Of the various groups, SSC group demonstrated the least microleakage [Figure 4] followed by amalgam, resin-modified GIC, and composite. SSC, amalgam, composite resin, and resin-modified GIC groups showed a mean of 0.67, 0.87, 1.40, and 1.33, respectively [Table 1 and Graph 1].
Figure 4.
Group 5 showing no leakage scanning electron microscope
Table 1.
Leakage score of different groups using the Kruskal–Wallis test
| n | Mean | SD | Median | Percentiles | Kruskal–Wallis test | P | ||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| 25th | 75th | |||||||
| Group 1 | 15 | 3.47 | 0.640 | 4.00 | 3.00 | 4.00 | 36.659 | 0.000<0.0001, (HS) |
| Group 2 | 15 | 1.33 | 0.617 | 1.00 | 1.00 | 2.00 | ||
| Group 3 | 15 | 1.40 | 0.632 | 1.00 | 1.00 | 2.00 | ||
| Group 4 | 15 | 0.87 | 0.640 | 1.00 | 0.00 | 1.00 | ||
| Group 5 | 15 | 0.67 | 0.976 | 0.00 | 0.00 | 2.00 | ||
SD: Standard deviation, HS: High significant
Graph 1.
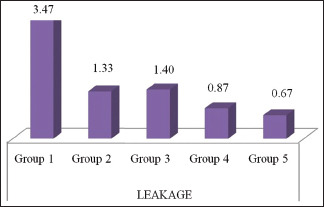
Microleakage of different groups
To compare the leakage between the groups Mann–Whitney test was used. ZOE group when compared to other groups showed more leakage which is highly significant. When resin-modified GIC and composite group were compared, it revealed both the groups demonstrated almost the same leakage. When resin-modified was compared with amalgam and stainless steel group, it showed more leakage than both groups which was significant. Composite group demonstrated more leakage than the amalgam and stainless steel group which was significant. Whereas the amalgam group demonstrated more leakage than the stainless steel group which was nonsignificant [Table 2].
Table 2.
Leakage score between various groups using the Mann–Whitney test
| Mean difference | Change (%) | Mann–Whitney test P | P | |
|---|---|---|---|---|
| Group 1 | ||||
| Group 2 | 2.133 | 61.54 | 0.000 | <0.001, (HS) |
| Group 3 | 2.067 | 59.62 | 0.000 | <0.001, (HS) |
| Group 4 | 2.600 | 75.00 | 0.000 | <0.001, (HS) |
| Group 5 | 2.800 | 80.77 | 0.000 | <0.001, (HS) |
| Group 2 | ||||
| Group 3 | −0.067 | −5.00 | 0.775 | NS |
| Group 4 | 0.467 | 35.00 | 0.042 | S |
| Group 5 | 0.667 | 50.00 | 0.036 | S |
| Group 3 | ||||
| Group 4 | 0.533 | 38.10 | 0.031 | S |
| Group 5 | 0.733 | 52.38 | 0.027 | S |
| Group 4 | ||||
| Group 5 | 0.200 | 23.08 | 0.314 | NS |
S: Significant, NS: Not significant, HS: High significant
DISCUSSION
A study among pediatric dentists (US) about parental attitude toward restorative materials for their children's teeth, revealed that 87% of the parents were dissatisfied with the usage of SSC.[6]
Due to its easy handling, low cost, and anti-inflammatory properties, ZOE cement is the stereotypical temporary restoration used to restore access preparation.[7] Breaking down of ZOE during moisture contact could be the cause of extensive leakage demonstrated by ZOE.[8] Since microleakage is more for ZOE its use as an alternative to SSC cannot be taken.
The possible reason for leakage of resin-modified GIC in this study might be polymerization shrinkage which causes marginal discrepancies leading to microleakage.[9] According to Attin et al., water expansion is also one factor that reduces microleakage.[10] While considering the above-mentioned factors resin-modified GIC can be a good substitute for stainless steel crown (SSC).
According to Andreina Castro et al.,(2002)[11] composite resin in primary teeth demonstrated more microleakage than permanent teeth. An increase in thickness of the hybrid layer in deciduous teeth causes decrease in penetration of adhesive resin into the dentin.[12] All these factors might have caused the microleakage.
Compared to other materials used in this study amalgam demonstrated the least microleakage. Amalgam is an exclusive restorative material which shows improved marginal seal over time due to corrosion.[13]
Even though amalgam has good biocompatibility and durability, esthetic value and contention on its safety remains.[14] The factors to be considered before selecting the restorative material in children are:
Caries risk assessment
Age and behavior of the patient
The remaining tooth structure
The time the tooth remains in the oral cavity
Conditions under which the treatment is being carried out.[15]
Pertaining to the abovementioned factors with regard to this present study composite resin and resin-modified GIC offers a good alternative for SSC in pulpotomized primary molars. However, their selection has to be judiciously carried out depending on the clinical situations.
CONCLUSION
From the results of the present study, we can conclude that:
The sealing ability can be summarized as: SSC <Amalgam <Resin-modified GIC <Composite resin <Zinc oxide eugenol cement
Composite resin and resin-modified glass ionomer offers good alternative to SSC after pulpotomized primary molars.
In the oral cavity, the eventual clinical effectiveness is determined by reciprocative numerous clinical variables.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Hill MW. The survival of vital and non-vital deciduous molar teeth following pulpotomy. Aust Dent J. 2007;52:181–6. doi: 10.1111/j.1834-7819.2007.tb00486.x. [DOI] [PubMed] [Google Scholar]
- 2.Seale NS. The use of stainless steel crowns. Pediatr Dent. 2002;24:501–5. [PubMed] [Google Scholar]
- 3.Croll TP, Riesenberger RE. Primary molar stainless steel crown restorations. Quintessence Int. 1986;17:221–6. [PubMed] [Google Scholar]
- 4.Barthel CR, Strobach A, Briedigkeit H, Göbel UB, Roulet JF. Leakage in roots coronally sealed with different temporary fillings. J Endod. 1999;25:731–4. doi: 10.1016/S0099-2399(99)80119-8. [DOI] [PubMed] [Google Scholar]
- 5.Bargrizan M, Mirkarimi M, Rezamand M, Eskandarion S. Microleakage and micrographic evaluation of composite restorations with various bases over ZOE layer in pulpotomized primary molars. J Dent (Tehran) 2011;8:178–85. [PMC free article] [PubMed] [Google Scholar]
- 6.Zimmerman JA, Feigal RJ, Till MJ, Hodges JS. Parental attitudes on restorative materials as factors influencing current use in pediatric dentistry. Pediatr Dent. 2009;31:63–70. [PubMed] [Google Scholar]
- 7.Tewari S, Tewari S. Assessment of coronal microleakage in intermediately restored endodontic access cavities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93:716–9. doi: 10.1067/moe.2002.122347. [DOI] [PubMed] [Google Scholar]
- 8.Hume WR. The pharmacologic and toxicological properties of zinc oxide-eugenol. J Am Dent Assoc. 1986;113:789–91. doi: 10.14219/jada.archive.1986.0256. [DOI] [PubMed] [Google Scholar]
- 9.Feilzer AJ, de Gee AJ, Davidson CL. Relaxation of polymerization contraction shear stress by hygroscopic expansion. J Dent Res. 1990;69:36–9. doi: 10.1177/00220345900690010501. [DOI] [PubMed] [Google Scholar]
- 10.Attin T, Buchalla W, Kielbassa AM, Helwig E. Curing shrinkage and volumetric changes of resin-modified glass ionomer restorative materials. Dent Mater. 1995;11:359–62. doi: 10.1016/0109-5641(95)80035-2. [DOI] [PubMed] [Google Scholar]
- 11.Castro A, Feigal RF. Microleakage of a new improved glass ionomerrestorative material in primary and permanent teeth. Pediatr Dent. 2002;24:23–8. [PubMed] [Google Scholar]
- 12.Nor J, Feigal R, Dennison J, Edwards C. Dentin bonding: SEM comparison of resindentin interface in primary and permanent teeth. J Dent Res. 1995;75:1396–403. doi: 10.1177/00220345960750061101. [DOI] [PubMed] [Google Scholar]
- 13.Fuks AB. The use of amalgam in pediatric dentistry. Pediatr Dent. 2002;24:448–55. [PubMed] [Google Scholar]
- 14.Osborne JW, Summitt JB, Roberts HW. The use of dental amalgam in pediatric dentistry: Review of the literature. Pediatr Dent. 2002;24:439–47. [PubMed] [Google Scholar]
- 15.Guelmann M, Major LA. Materials and techniques for restoration of primary molars by pediatric dentists in florida. Pediatr Dent. 2002;24:326–31. [PubMed] [Google Scholar]