

Abstract
Introduction:
The emergence of coronavirus disease-2019 (COVID-19) pandemic poses an immense global health challenge. It also had a profound impact on dentistry with all elective treatment grinding to half initially and a slow phased return to normal services. The aim of the article is to provide an insight into the effect of COVID-19 on endodontic treatment.
Materials and Methods:
A cross-sectional study among endodontists of various southern states of India was conducted from January 1, 2021 to March 31, 2021, using an online questionnaire. A total of 300 dentists who perform endodontic treatment in daily clinical practice were chosen for the survey. The information was coded, entered, and analyzed utilizing SPSS 20.0 version.
Results:
A total of 263 questionnaires were answered by the selected group. About 92.01% of endodontists have made changes in infection control including modification in their personal protective equipment and duration of the interval between their appointments. A whopping 74.14% of endodontists faced the economic loss of varying degrees due to the pandemic. In general tremendous changes have been occurred in their daily practice following the pandemic.
Conclusion:
The pandemic's current and enduring consequences on every part of our lives have been a cause of pain and frustration, but it has also highlighted the human spirit's resilience. Ideally, endodontists must be able to select the best arrangements for safely performing their procedures.
KEYWORDS: Economics, endodontic practice, endodontists
INTRODUCTION
A developing sickness called as coronavirus disease (COVID-19) was spreading from Wuhan City, China in late December 2019.[1] Due to the severity of the disease and its global spread, the World Health Organization (WHO) labeled the COVID-19 outbreak a pandemic in March 2020.[2] The first laboratory-confirmed case of COVID-19 in India was reported on January 30 in Kerala, with a history of travel from Wuhan, China. Severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) spreads from person to person through droplets or direct contact of infectious material on the oral, nasal, or ocular mucous membranes.[3] Health-care workers are most susceptible to contracting the virus after coming into contact with infected body fluids.[4] The employment of aerosol-producing devices in oral health care, as well as their proximity to the mouth mucosa and secretions, puts dental practitioners in the greatest risk category for COVID-19 exposure.[5,6] There is a significant risk of cross-infection between dental practitioners and COVID-19 patients. As a result, most of the dental practitioners were stressed, anxious, and depressed as a result of the looming uncertainty.[7] Our country's health authorities instructed dental facilities to stop offering nonemergency dental care and exclusively provide emergency dental care.[8] The Centers for Disease Control and Prevention (CDC), the American Dental Association (ADA), and the WHO have all released guidelines to assist reduce the spread of COVID-19. They emphasize the use of personal protective equipment, as well as complete patient and personnel screening, clinic facility disinfection, rubber dam isolation, and other measures.[9] These are recommendations for treating people who are in pain and require endodontic treatments.
Using aseptic techniques and producing as little aerosol as possible should be the goal. Another goal is to provide the best possible endodontic access and instruments. The increased usage of cell phones and related software programs has facilitated clinical data transmission between patients and doctors, which has been nicknamed “teledentistry.”[10] Given the volatile nature of dentistry today, it is critical to check for mental health issues, such as depression, among the Indian dental community. Dental clinics must also deal with the business and economic effects of the pandemic. Over the course of a year, the COVID-19 shutdowns resulted in a 29% loss for dental clinics, according to economic analysis.[11]
The aim of the study is to assess the challenges faced by endodontists in South India during the pandemic and also to understand the changes adopted in their daily practice in terms of infection control and patient management by application of questionnaire survey.
MATERIALS AND METHODS
Study design and participants
A cross-sectional study was conducted among the dentist practicing across various states in south India. It was conducted from January 2021 to March 30, 2021.
Eligibility criteria
The respondent must be a dentist who regularly performs endodontic procedures in clinical practice although he or she does not need to be an endodontic specialist.
The self-supporting form in English was created using simple Google forms and the link was spread among the doctors via numerous closed social media sites along with a consent form.
Ethical consideration
The study participation was entirely voluntary. Anonymity was ensured and no personal identification such as IP address, E-mail ID name, etc., was collected.
Data collection
A randomized selection of the sample was chosen for the survey dental group present on social media. A total of 300 dentists were chosen for the survey. The questionnaire was divided mainly into two sections. The first section of the survey focused on personal data information (demographic variables) such as sex, location, and years of experience.
The second part included question about dentist perception and behavior regarding endodontic treatment during the COVID-19 pandemic. They were also asked about the financial impact due to lockdown, anxiety and stress as well. The recent changes they have introduced in their endodontic practice due to COVID-19 were also included in the questionnaire.
When a multiple-choice selection was requested, some of the responses were coded as dichotomous variables, such as Yes/No responses, or as categorical variables in general. Because of the nature of the survey, we used descriptive statistics for the majority of the questions.
Data analysis
The information was coded, entered, and analyzed utilizing SPSS 20.0 version (IBM Corp., Armonk, NY, USA). Descriptive statistics, frequencies, and percentages were utilized to sum up information.
RESULTS
A total of 300 endodontists were included in the study, 37 endodontists did not respond. In all, 263 questionnaires were answered by endodontists from various states of South India. The final sample size was 263 endodontists assuming an 8.1% nonresponse rate. Female respondents accounted for, 137 (52.09%) and male 126 (47.9%) of the total. Regarding year of practice, about 68 (25.8%) had a clinical experience of <10 years, 152 (57.7%) had about 11–20 years of experience, and 43 (16.3%) with >20 years of experience. The majority of endodontists belonged to Kerala 116 (44.1%) followed by Karanataka 53 (20.15%) and Tamil Nadu 51 (19.3%). Regarding marital status of participants, 193 (73.3%) were married. Greater part of the participants held an MDS degree (64.2%) [Table 1].
Table 1.
Participant demographic characteristics
| Characteristics | Variables (%) |
|---|---|
| 1. Sex | |
| Male | 126 (47.9) |
| Female | 137 (52.09) |
| 2. Professional experience (years) | |
| Up to 10 | 68 (25.8) |
| 11-20 | 152 (57.7) |
| >20 | 43 (16.3) |
| 3. Marital status | |
| Single or never married | 70 (26.6) |
| Married | 193 (73.3) |
| 4. Location | |
| Kerala | 116 (44.1) |
| Tamil nadu | 51 (19.3) |
| Karnataka | 53 (20.1) |
| Telangana | 12 (4.56) |
| Andhra pradesh | 31 (11.78) |
| 5. Educational qualification | |
| BDS | 94 (35.7) |
| MDS | 169 (64.2) |
Table 2 shows the participants who were under stress during this pandemic was about 79.8%. Endodontists who have made changes in infection control protocol gave a good score of 92.01% which included patient screening (79.08%), no contact thermal scanners in the clinic (93.9%), changes in personal protective equipment used (94.67%), and increased duration of the interval between appointments (64.6%).
Table 2.
Dentist’s responses to pandemic preparedness and perceptions of infection control measures
| Changes during the pandemic period | Yes, n (%) | No, n (%) |
|---|---|---|
| Has your stress level increased during COVID 19 pandemic? | 210 (79.8) | 53 (20.1) |
| Did the pandemic change the infection control routine in your clinic? | 242 (92.01) | 21 (7.9) |
| Do you think patient screening and usage of PPE has reduced the risk of cross infection? | 208 (79.08) | 55 (20.9) |
| Have you introduced any changes in protective equipment used during endodontic procedures? | 249 (94.67) | 14 (5.3) |
| Did you install a no contact thermal scanner for screening the patients? | 247 (93.9) | 16 (6.08) |
| Have you increased duration of interval between appointments? | 170 (64.6) | 93 (35.3) |
| Do you consider tele dentistry effective for patient management during COVID-19 pandemic? | 213 (80.8) | 50 (19.01) |
| Is symptomatic irreversible pulpitis the most commonly encountered endodontic emergency? | 203 (77.1) | 60 (22.8) |
| Is it necessary to change some clinical procedures in endodontic treatment due to pandemic? | 151 (57.4) | R112 (42.5) |
| Do you find pulpotomy with/without canal instrumentation acceptable in managing endodontic emergency? | 195 (74.1) | 65 (24.7) |
| Is the usage of electronic apex locator proven useful during COVID 19 outbreak? | 82 (31.1) | 181 (68.8) |
| Do you prefer to use rubber dam isolation during endodontic access cavity preparation? | 181 (68.8) | 82 (31.1) |
| Have you shifted from reusable endodontic instruments to disposable? | 121 (46) | 142 (53.9) |
| Have you shifted to the usage of tungsten carbide burs to reduce debris generation? | 63 (23.9) | 200 (76.04) |
| Do you prefer slow-speed micromotor without water spray for cavity preparation during COVID 19 outbreak? | 129 (49.04.) | 134 (50.9) |
| Are you comfortable in using airotor with water spray during access cavity preparation in the COVID-19 era? | 126 (47.9) | 137 (52.09) |
| Has the need for usage of magnification techniques such as full-face visor led to technostress in endodontists? | 22 (8.3) | 241 (91.6) |
| Do you find your patients cooperating with the delay in dental treatment during lockdown? | 128 (48.6) | 135 (51.3) |
| Are the patients willing to adhere to guidelines set out by dentists to minimize the risk of virus transmission? | 134 (50.9) | 129 (49.04) |
| Has a fear raised regarding the impact of the COVID - 19 crisis on dentists livelihood? | 244 (92.7) | 19 (7.2) |
| Do you think there is the necessity of endodontists in public health systems? | 210 (79.8) | 53 (20.1) |
| Has practicing four-handed dentistry increased the expenditure in terms of providing PPE? | 163 (61.9) | 100 (38.02) |
| Are the measures adopted for infection control difficult to practice? | 163 (61.9) | 100 (38.02) |
| Do you have a telescreening facility in your clinic before giving patient appointments? | 135 (51.33) | 128 (48.6) |
| Do you adhere to regular treatment line of pulpotomy/pulpectomy for managing symptomatic irreversible pulpitus during COVID-19 outbreak? | 99 (37.6) | 164 (62.3) |
COVID-19: Corona virus disease-2019, PPE: Personal protective equipment
More than two-thirds of participants find teledentistry effective in management during pandemics (80.8%). About 77.1% find symptomatic irreversible pulpitis, the most commonly encountered emergency. About 57.4% find it necessary to change the clinical procedures in endodontic treatment due to pandemic. About 74.1% accept pulpotomy with or without canal instrumentation in managing emergencies. Electronic apex locator was found useful by 31.1% of the respondents. 68.8% of respondents prefer rubber dam isolation before cavity preparation. Less than 50% of respondents have shifted to disposable instruments and slow speed airotors and only a quarter to tungsten carbide burs. 47.9% feel uncomfortable in using airotor with water spray. Few believe the usage of magnification techniques leads to technostress. Almost half of the participants find that patients are not cooperating with the delay in treatment and do not adhere to guidelines. 92.7% fear about the impact of the pandemic on their livelihood. A necessity of endodontists in the Public health system was found right by 79.8%. 61.9% find that four-handed dentistry has increased expenditure in terms of providing personal protective equipment. About 61.9% of participants have difficulty in practicing the measures adopted for infection control. About half of the respondents had telescreening facilities in the clinic before giving patient appointments. Only 37.6% of endodontists adhere to a regular treatment line for managing symptomatic irreversible pulpitis during the COVID-19 outbreak.
Table 3 shows that most of the participants agree that there is change in the total cost of endodontic treatment (85.9%) during pandemic. Personal Protective equipment provide a sense of security in 76.4% of the participants. Amoxicillin-Clavulanic acid was the first choice of treatment in 62.3% of endodontists and 58.17% agree ibuprofen as the first choice for acute dental pain treatment. 78.32% endodontists chose pulpectomy with endodontic instruments for interim relief of vital teeth. 71.4% agree that high volume suction reduces exposure to aerosols. Survey results indicate that the pandemic has a negative impact on 75% of respondents with 1.14% reporting loss of >75% [Figure 1].
Table 3.
Dentist’s responses to changes in endodontic practice during pandemic
| Changes in endodontic practice during pandemic | Agree, n (%) | Disagree, n (%) |
|---|---|---|
| 1. Total cost of endodontic treatment has changed due to pandemic | 226 (85.9) | 37 (14.06) |
| 2. PPE usage ensured sense of security | 201 (76.4) | 62 (23.5) |
| 3. Amoxicillin-clavulanic acid is considered the first choice of treatment for symptomatic irreversible pulpitis during the COVID-19 outbreak | 164 (62.3) | 99 (37.64) |
| 4. Ibuprofen is the first choice of drug for acute dental pain during COVID-19 | 153 (58.17) | 110 (41.8) |
| 5. Pulpectomy with endodontic instruments would be the choice for interim relief of vital teeth | 206 (78.32) | 57 (21.6) |
| 6. High volume suction reduces the exposure of endodontist to aerosols generated | 188 (71.4) | 75 (28.51) |
COVID-19: Corona virus disease-2019, PPE: Personal protective equipment
Figure 1.
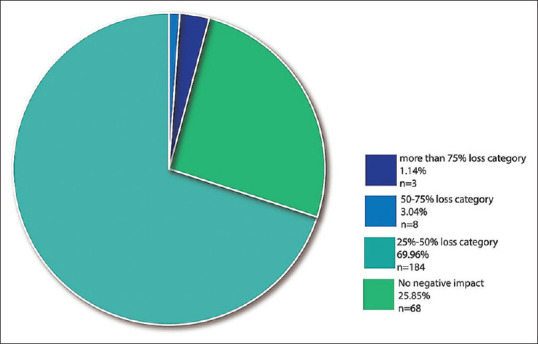
The financial impact of endodontists in South India due to the corona pandemic survey results indicates that due to the pandemic almost 75% had a negative impact with 1.14% reporting a loss of more than 75%
DISCUSSION
The main purpose of the study was to identify the changes in perception and methods in endodontic practices during the corona pandemic. Endodontists of around 300 across the southern states of India contributed the needed information. The sociodemographic factors included gender, level of experience, education, marital status, and residence area.
In our study, 92.01% of endodontists reported that they had made changes in the infection control protocol. Dentists in Switzerland and Liechtenstein were found to have similar levels of awareness, preventive measures, and economic effects in a study.[12] The ADA and the CDC have issued guidelines for dentists and dental employees in collaboration with the WHO. Personal Protective Equipment, hand sanitizers, and other measures to prevent the spread of COVID-19 include a thorough examination of the patient and the use of a rubber dam isolation, mouthwashing before dental operations and disinfection of all exposed surfaces are all recommended.[13] Almost 85.9% agreed to the statement that the total cost of endodontic treatment has increased. It is well acknowledged that the COVID-19 pandemic has posed a significant threat to all economic sectors.[14] 64.6% of the endodontist have increased the duration of the interval between appointments. Longer gap between dental appointments was followed in many countries.[15] The present study also identifies that In 79.8% of the dentist the corona pandemic has caused the increase in stress. A similar study also stated that Indian endodontists have a greater level of felt stress with COVID19 being a major stressor for nearly half of them.[16] It has already been established that using high-volume saliva ejectors could reduce the production of droplets and aerosols during dental procedures, thereby protecting dentists from infection. Furthermore, whenever high-or low-speed drilling is used, face shields and protective eyewear are required. In line with this study, 79.8% agreed with the statement high volume suction reduces the exposure of endodontists to aerosol generated. A similar survey states that aerosols are typically produced during the removal of caries and the opening of an endodontic access cavity they can be inhaled, absorbed through the skin, and absorbed through personal contact protective gear, or can be placed on nearby surfaces. As a result, SARS-CoV-2 was transmitted.[17] Many countries have issued declarations on operations involving aerosols.[18,19] Several studies[20,21,22] demonstrate that pulpotomy could be a quick and simple pain-relieving approach in endodontic emergency treatment. This may be the reason 74.1% of the general dental practitioners performed pulpotomy.
Ibuprofen was the most commonly used pain reliever (58.17% of all participants). This finding is similar to Mickel et al.'s finding that ibuprofen is a popular drug preferred by clinicians in the presence of endodontic pain.[23]
Dentists, especially endodontists, are on the front lines of the pandemic. A dental emergency can be a life-threatening situation that can lead to systemic infection. As a result, emergency dental care is required, posing a challenge in combining patient care with worker safety. Hygiene and cleaning care must be improved and monitored regularly as a result, dentists must adjust their practices and take extra precautions during this time.[24]
Limitations
Poorly chosen distribution channels can lead to unbiased data, low response rates, and a variety of other issues. It may be difficult to reach out to specific types of participants, such as those without internet access or noncustomer samples in specialty businesses. Statistical confidence and margins of error are called into question due to a lack of high-quality random sampling (if they exist at all).
CONCLUSION
During the COVID-19 pandemic, most dental professionals noticed changes in the routine of endodontic treatment. The emphasis should be on developing COVID19 lockdown exit strategies for dentists, better working protocols for sterilization/disinfection, cheaper, faster, more reliable screening and diagnostic tools, making barrier materials available, and a robust health support system that balances health worker protections while providing ideal dental types of assistance to patients in need of emergency intervention.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Ayub K, Alani A. Acute endodontic and dental trauma provision during the COVID-19 crisis. Br Dent J. 2020;229:169–75. doi: 10.1038/s41415-020-1920-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Malhão EC, Fabio de Almeida G, Ferreira CM, Lima DL, Casarin M, Pappen FG. Endodontic treatment during COVID-19 pandemic: Economic perception of dental professionals. Braz J Oral Sci. 2021;20:e213555. [Google Scholar]
- 3.Wiesmüller V, Bruckmoser E, Kapferer-Seebacher I, Fink K, Neururer S, Schnabl D, et al. Dentists' working conditions during the first COVID-19 pandemic lockdown: An online survey. Healthcare (Basel) 2021;9:364. doi: 10.3390/healthcare9030364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sim MR. The COVID-19 pandemic: Major risks to healthcare and other workers on the front line. Occup Environ Med. 2020;77:281–2. doi: 10.1136/oemed-2020-106567. [DOI] [PubMed] [Google Scholar]
- 5.Dave M, Seoudi N, Coulthard P. Urgent dental care for patients during the COVID-19 pandemic. Lancet. 2020;395:1257. doi: 10.1016/S0140-6736(20)30806-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ali K, Raja M. Coronavirus disease 2019 (COVID-19): Challenges and management of aerosol-generating procedures in dentistry. Evid Based Dent. 2020;21:44–5. doi: 10.1038/s41432-020-0088-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bai Y, Lin CC, Lin CY, Chen JY, Chue CM, Chou P. Survey of stress reactions among health care workers involved with the SARS outbreak. Psychiatr Serv. 2004;55:1055–7. doi: 10.1176/appi.ps.55.9.1055. [DOI] [PubMed] [Google Scholar]
- 8.Azim AA, Shabbir J, Khurshid Z, Zafar MS, Ghabbani HM, Dummer PM. Clinical endodontic management during the COVID-19 pandemic: A literature review and clinical recommendations. Int Endod J. 2020;53:1461–71. doi: 10.1111/iej.13406. [DOI] [PubMed] [Google Scholar]
- 9.Al-Shawi MM, Darwish MA, Abdel Wahab MM, Al-Shamlan NA. Misconceptions of parents about antibiotic use in upper respiratory tract infections: A survey in primary schools of the Eastern Province, KSA. J Family Community Med. 2018;25:5–12. doi: 10.4103/jfcm.JFCM_46_17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Matusitz J, Breen GM. Telemedicine: Its effects on health communication. Health Commun. 2007;21:73–83. doi: 10.1080/10410230701283439. [DOI] [PubMed] [Google Scholar]
- 11.Schwendicke F, Krois J, Gomez J. Impact of SARS-CoV2 (Covid-19) on dental practices: Economic analysis. J Dent. 2020;99:103387. doi: 10.1016/j.jdent.2020.103387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Wolf TG, Zeyer O, Campus G. COVID-19 in Switzerland and Liechtenstein: A cross-sectional survey among dentists' awareness, protective measures and economic effects. Int J Environ Res Public Health. 2020;17:9051. doi: 10.3390/ijerph17239051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Consolo U, Bellini P, Bencivenni D, Iani C, Checchi V. Epidemiological aspects and psychological reactions to COVID-19 of dental practitioners in the Northern Italy districts of Modena and Reggio Emilia. Int J Environ Res Public Health. 2020;17:3459. doi: 10.3390/ijerph17103459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nicola M, Alsafi Z, Sohrabi C, Kerwan A, Al-Jabir A, Iosifidis C, et al. The socio-economic implications of the coronavirus pandemic (COVID-19): A review. Int J Surg. 2020;78:185–93. doi: 10.1016/j.ijsu.2020.04.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Peng X, Xu X, Li Y, Cheng L, Zhou X, Ren B. Transmission routes of 2019-nCoV and controls in dental practice. Int J Oral Sci. 2020;12:9. doi: 10.1038/s41368-020-0075-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Roy D, Tripathy S, Kar SK, Sharma N, Verma SK, Kaushal V. Study of knowledge, attitude, anxiety & perceived mental healthcare need in Indian population during COVID-19 pandemic. Asian J Psychiatr. 2020;51:102083. doi: 10.1016/j.ajp.2020.102083. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.World Health Organization. Geneva: World Health Organization; 2020. Modes of Transmission of Virus Causing COVID-19: Implications for IPC Precaution Recommendations: Scientific Brief, 27 March, 2020. [Google Scholar]
- 18.Krithikadatta J, Nawal RR, Amalavathy K, Mclean W, Gopikrishna V. Endodontic and dental practice during COVID-19 pandemic: Position statement from the Indian Endodontic Society, Indian Dental Association, and International Federation of Endodontic Associations. Endodontology. 2020;32:55–66. [Google Scholar]
- 19.Bhanderi S, Lessani M, Morgan A, Tomson P, McLean W. Diagnosis and Management of Endodontic Emergencies, a British Endodontic Society Position Paper for Primary Dental Care and Other Healthcare Providers during the COVID-19 Pandemic; 2020. [Last accessed on 2022 Jan 06]. Available from: https://britishendodonticsociety.org.uk/wp-content/uploads/2020/03/BES-Emergency-Protocol-FINAL-DOCUMENT-29-MARCH-2020.pdf .
- 20.Nyerere JW, Matee MI, Simon EN. Emergency pulpotomy in relieving acute dental pain among Tanzanian patients. BMC Oral Health. 2006;6:1. doi: 10.1186/1472-6831-6-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Asgary S, Eghbal MJ. The effect of pulpotomy using a calcium-enriched mixture cement versus one-visit root canal therapy on postoperative pain relief in irreversible pulpitis: A randomized clinical trial. Odontology. 2010;98:126–33. doi: 10.1007/s10266-010-0127-2. [DOI] [PubMed] [Google Scholar]
- 22.Eren B, Onay EO, Ungor M. Assessment of alternative emergency treatments for symptomatic irreversible pulpitis: A randomized clinical trial. Int Endod J. 2018;51(Suppl 3):e227–37. doi: 10.1111/iej.12851. [DOI] [PubMed] [Google Scholar]
- 23.Mickel AK, Wright AP, Chogle S, Jones JJ, Kantorovich I, Curd F. An analysis of current analgesic preferences for endodontic pain management. J Endod. 2006;32:1146–54. doi: 10.1016/j.joen.2006.07.015. [DOI] [PubMed] [Google Scholar]
- 24.Passarelli PC, Rella E, Manicone PF, Garcia-Godoy F, D'Addona A. The impact of the COVID-19 infection in dentistry. Exp Biol Med (Maywood) 2020;245:940–4. doi: 10.1177/1535370220928905. [DOI] [PMC free article] [PubMed] [Google Scholar]