

Abstract
Background
Workflow interruptions are common in the emergency department (ED) of the hospitals for physicians, leading to an increased risk of errors.
Purpose
This study aims to understand the baseline activities of the ED doctors and how these are affected by workflow interruptions.
Methods
The study was conducted in two phases to collect the doctor’s perspective (through questionnaire survey) and observer’s perspective (through workflow observation study) about ED doctors’ baseline activities and workflow interruptions. Two different perspectives were obtained to make the insights clearer and more valuable. The point of view of the 223 doctors working in ED of the hospitals was recorded through a questionnaire survey. In the second phase, the observer’s point of view (authors) was obtained through a workflow observation study, and 13 doctors were observed for 160 hours.
Results
Direct communication with patients (37.1%) and ‘documentation and prescription’ (22.7%) were found to be the most frequent activities. The most common interruptions were visual and auditory distractions, rumination (mind-wandering) and intrusion (by co-workers). Also, the time consumed on indirect patient care (6.6%) was higher than direct patient care (4. 2%). Interruptions increase the chances of errors by making it hard for a doctor to resume a primary task after facing interruptions.
Conclusion
Interruptions increase the chances of errors and make it difficult for the doctors to resume primary tasks (after facing such incidents).
Keywords: interruptions, human factors, emergency department
What is already known on this topic.
Observational studies were conducted to study baseline activities and workflow interruptions faced by the physicians in the hospitals’ emergency departments (EDs).
What this study adds
This study investigated workflow interruptions and baseline activities of ED doctors in the perspective of the observer (through observation study) and doctors (through questionnaire survey).
Furthermore, it includes region-wise analysis of baseline activities and workflow interruptions in urban and suburban hospitals.
How this study might affect research, practice or policy
Occupational application of this study includes improving the overall performance of ED doctors that are often affected by workflow interruptions.
Introduction
Emergency departments (EDs) are challenging and complex work systems1 because of unpredictable demand.2 A worldwide spread of COVID-193 is a contemporary example of unpredictable workload in EDs of hospitals. Workflow interruptions are common in the working environment of EDs.4 Interruption is when the current (primary) task is suspended for performing secondary tasks.5 Workflow interruptions are assumed to hurt the working memory of clinicians. That is why these interruptions lead to an increase in the risk of errors,6 breaks in tasks,2 cognitive effect (eg, less accurate recall of information and memory loss), breaks in concentration7 and workload.8 Therefore, healthcare environments need to reduce workflow interruptions to efficiently and safely improve clinical outcomes.8 9
Different methodologies have been adopted to study interruption for medical staff working in EDs. For instance, interruptions and multitasking for the doctors working in EDs of the hospitals were examined using a workflow time study.10 Multitasking performed by clinicians in two Swedish EDs was observed through an observational study by employing two observers simultaneously to determine the accuracy of observations. The most common activity was information exchange.11 Interviews were also used to observe the physician’s perspective on workflow interruptions at Swedish EDs.12 A mixed-method study (involving observational and interview studies) monitored the interruptions in two Swedish ED works.13 Direct observation, semi-structured interviews and hospital surveys were used to explore US hospital nurses’ work environment and interruptions.14
In the extant body of literature, observational workflow time studies10 11 15 and semi-structured interview survey studies13 have been employed to study workflow interruptions in EDs of hospitals. However, this study aims to understand the baseline activities of ED doctors and how these are affected by workflow interruptions through the observer’s perspective (observational study) and doctors’ perspectives (using questionnaire survey method) to make the insights clear and valuable. Furthermore, workflow interruptions in clinical work across different settings, that is, urban versus suburban/rural hospitals, have been observed. The study is first in nature to explore and compare doctors’ perspectives with observations. In addition, the study also compares the baseline activities and workflow interruptions of ED doctors from urban and suburban hospitals to know if the types and frequencies of occurrences are different. Based on outcomes, a framework is proposed to improve the doctors’ performance by effectively managing interruptions.
The following research questions are developed for this study:
RQ1. What type of activities do the doctors have to perform during working hours?
RQ2. What types and frequency of interruptions are faced by the doctors working in EDs?
RQ3. To what extent do the findings of the survey differ from observations?
RQ4. Do the answers to the above three RQs vary for the doctors working in EDs of the urban and suburban hospitals?
RQ5. What factors (reduced working hours, relevant patients, etc) affect the overall performance of the doctors?
Data and methods
Data collection
As per the research requirement, as mentioned above, data for this study were collected using both questionnaire survey and observation study approaches. And participants in the questionnaire survey participated voluntarily. The data were collected through a questionnaire requiring the respondents to record their responses on a Likert scale in a questionnaire survey. Two hundred twenty-three responses were recorded through random sampling technique, including 118 from the doctors working in urban hospitals and 105 from the doctors working in the suburban region. Thirteen respondents (seven from urban and six from suburban) were the doctors under observation for an observational study. Consent was obtained from doctors for an observational study. Six doctors working in the ED of a suburban hospital were observed for 80.5 hours. Similarly, seven doctors working in the ED of an urban hospital were followed for 79.5 hours.
Based on previous studies, baseline activities were divided into 10 categories to ease the observation study.16 17 These 10 activities included social and personal activity, indirect patient care, direct patient care, documentation and prescribing, direct communication with patients, patient data analysis, professional communication, breaks, walking and waiting for patients’ diagnosis results or colleagues’16 17 were observed during the observational study.
The questionnaire was divided into two parts. The first part of the questionnaire consists of 13 factors, including interruptions (IN), patient care, multitasking (MT), personal/social activities in night shifts versus day shifts, task switching, task break-in, resumption of primary task (RT), professional communication, waiting, breaks, information exchange, social and personal task and overtime. The details are presented in the appendix (see online supplemental appendix A). Part 2 of the questionnaire consists of the doctors’ opinions about the effects of the number of patients, relevant patients, working hours, frequent breaks, visual and auditory distractions, multitasking and interruptions on the overall performance of doctors (see online supplemental appendix B).
bmjoq-2022-001813supp001.pdf (47.2KB, pdf)
Figure 1 presents the scheme of this study.
Figure 1.
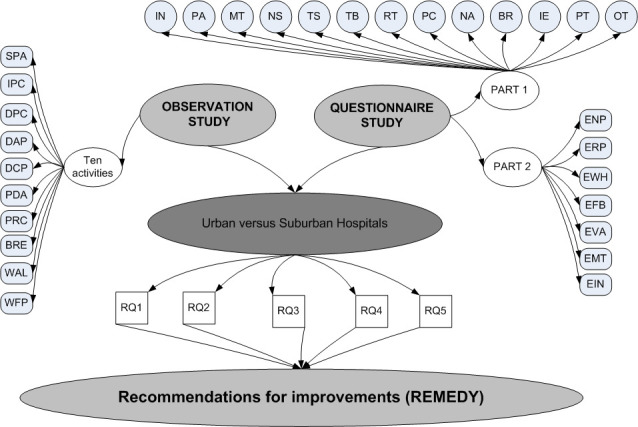
Scheme of study. BR, breaks; BRE, breaks; DPC, direct patient care; DAP, documentation and prescribing; DCP, direct communication with patients; ENP, effect of number of patients; ERP, effect of relevant patients; EWH, effect of working hours; EFB, effect of frequent breaks; EVA, effect of visual and auditory distractions; EMT, effect of multitasking; EIN, effect of interruptions; IN, interruptions; IE, information exchange; IPC, indirect patient care; MT, multitasking; NS, personal/social activities in night shifts; OT, overtime; PA, patient care; PC, professional communication; PT, social and personal task; PDA, patient data analysis; PRC, professional communication; RT, resumption of primary task; S, task switching; SPA, social and personal activity; TPC, professional communication; TB, task break-in; WAL, walking; WFP, waiting for patients’ diagnosis results or colleagues.
Methods for data analyses
The obtained data (discussed in detail under the subheading ‘Data collection’) is collected from urban and suburban hospitals. Therefore, the analyses section is divided into two parts to analyse the data in a better and clear way, including the (1) overall model (regardless of hospital’s location at urban and suburban hospitals) and (2) region-wise analysis (urban and suburban hospitals).
The data obtained from the observation study is analysed through descriptive statistics.16–18 The analyses of the data obtained from the questionnaire survey are made using SmartPLS to find significant interruptions in doctors’ work patterns and examine the relationship of interruptions to different factors.19 To compare urban and suburban hospitals, Kruskal-Wallis, pairwise Wilcoxon rank-sum and Spearman’s rank correlations tests were used in extant studies to compare interruptions in EDs of rural areas, urban and suburban hospitals.2 Wilcoxon rank-sum test has been used for comparison between two samples, whereas the Kruskal-Wallis test is for comparison among more than two samples.20 Therefore, in this study, the Wilcoxon rank-sum test compares the results of urban and suburban hospitals.
Patient and public involvement
This study investigates the baseline activities and interruptions faced by the doctors working in EDs of the hospitals by incorporating the doctor’s and observer’s perspectives. Research questions were developed based on the gap in the literature, that is, discussed earlier in the ‘Introduction’ section. The study was designed in a way that it will cover the doctor’s perspective through a questionnaire survey. Patients and public were not involved, however, perspectives of the doctors were recorded through a questionaire survey. The consent of the doctors was taken before participation.
Results
Survey results and analysis
The demographic detail of the respondent doctors from EDs of hospitals is provided in table 1. The values of Cronbach’s alpha for comprehensive data (regardless of hospitals located at urban or suburban sites) for the urban region and suburban region (0.787, 0.798 and 0.798) are within the acceptable range of 0.70–0.95,21 confirming the reliability of the data.
Table 1.
Demographic detail of respondent emergency department doctors
| Variable | Description | Frequency | Percentage (%) |
| Gender | Male | 127 | 57.0 |
| Female | 96 | 43.0 | |
| Age (years) | 20–25 | 48 | 21.5 |
| 26–30 | 78 | 35.0 | |
| 31–35 | 56 | 25.1 | |
| 35+ | 41 | 18.4 | |
| Experience (years) | 0–5 | 86 | 38.6 |
| 6–10 | 70 | 31.4 | |
| 11–15 | 51 | 22.9 | |
| 15+ | 16 | 7.2 | |
| Area of hospital | Urban | 118 | 52.9 |
| Suburban/Rural | 105 | 47.1 | |
| Department | Emergency | 223 | 100.0 |
| Other | 0 | 0.0 |
Overall model
For an overall model (regardless of hospital location at urban or suburban sites), the effect of interruptions on different factors using relative path coefficients is shown in figure 2. All path coefficients are positive, showing a direct impact of interruptions on other factors. Among all path coefficients, interruptions to personal/social activities in the night shift (IN-NS) have the highest path coefficient value. It represents that the rate of personal activities, including cell phone usage, is higher in night shifts than in day shifts. These findings confirmed the results of the previous study in different countries and settings.18 The next highest path coefficient is the effect of interruptions on the resumption of tasks (IN-RT). It represents that resuming the primary task after distraction or interruption is difficult for the doctors. The path coefficient of interruptions on multitasking (IN-MT) shows that interruptions and distractions result in multitasking, for example, a doctor is busy prescribing while listening to his colleagues. Among IN, visual and auditory distractions (IN2), rate of rumination such as mind-wandering (IN5) and rate of intrusions such as co-workers asking for something or emails that demand attention (IN4) are found to be significant interruptions (RQ2).
Figure 2.
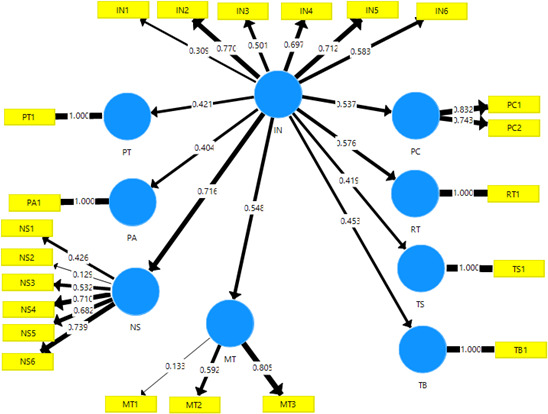
Overall model. IN, interruptions; MT, multitasking; NS, personal/social activities in night shifts; PA, patient care; RT, resumption of primary task; TS, task switching; TB, task break-in.
According to doctors’ opinion (obtained through part 2 of the questionnaire), the effect of visual and auditory distractions (1.794±0.779), multitasking (1.670±0.594) and interruptions (1.499±0.524) is negative on the overall performance of ED doctors because mean value of doctor’s responses for these variables is closer to ‘1’ in a 5-point Likert scale questionnaire. Whereas the effect of the relevant patient (4.236±0.513) and reduced number of patients (4.272±0.483), decreased working hours (4.264±0.538) and frequent breaks (3.998±0.798) are positive on the overall performance of doctors because the mean value of doctor’s responses is closer to ‘5’ for these variables.
Region-wise analysis: comparison between urban and suburban hospitals
Significance values from the Wilcoxon rank-sum test representing a difference in mean values for urban and suburban sites are presented in table 2. A p value ≤0.05 means that the difference in the mean value for urban and suburban sites is significant. The differences in mean values for interruptions, multitasking, personal activities in night shifts, task break-in, professional communication, waiting, breaks, social/personal tasks and overtime are significant. According to the results of the Wilcoxon rank-sum test, there is no significant difference in the opinion of the doctors working in EDs of urban and suburban hospitals regarding the effect of the number of patients, relevant patients, working hours, frequent breaks, visual and auditory distractions, multitasking and interruptions on performances of doctors (RQ4).
Table 2.
Results of Wilcoxon rank-sum test and descriptive statistics
| Factors | Urban versus suburban | Urban | Suburban |
| Wilcoxon rank-sum test (p value) | Mean±SD | Mean±SD | |
| Interruptions | 0 | 4.069±0.802 | 3.267±0.690 |
| Patient care | 0.327 | 3.822±1.059 | 3.962±0.820 |
| Multitasking | 0 | 4.091±0.729 | 3.670±0.542 |
| Personal/social activities in night shifts | 0 | 3.197±0.598 | 3.685±0.516 |
| Task switching | 0.188 | 4.137±1.074 | 4.295±0.929 |
| Task break-in | 0.004 | 3.632±1.111 | 4.029±0.853 |
| Resumption of task | 0.623 | 3.906±1.122 | 3.971±0.975 |
| Professional communication | 0 | 3.280±0.885 | 3.776±0.759 |
| Waiting | 0 | 3.521±1.171 | 4.152±0.830 |
| Breaks | 0.013 | 3.675±1.279 | 3.981±1.126 |
| Information exchange | 0.452 | 4.127±1.034 | 4.229±0.846 |
| Social/Personal tasks | 0.019 | 2.559±1.034 | 3.000±1.359 |
| Overtime | 0 | 3.511±0.657 | 3.867±0.595 |
| Effect of number of patients | 0.169 | 4.328±0.463 | 4.210±0.499 |
| Effect of relevant patients | 0.43 | 4.269±0.503 | 4.200±0.524 |
| Effect of working hours | 0.114 | 4.319±0.573 | 4.202±0.493 |
| Effect of frequent breaks | 0.143 | 4.088±0.763 | 3.897±0.826 |
| Effect of visual and auditory distractions | 0.995 | 1.806±0.850 | 1.781±0.697 |
| Effect of multitasking | 0.925 | 1.682±0.666 | 1.656±0.503 |
| Effect of interruptions | 0.691 | 1.485±0.521 | 1.514±0.5229 |
The factors with a significant difference are further investigated to know whether the mean value is higher for the urban or suburban site. Based on the above results (shown in table 2) and discussion, RQ4 concludes that multitasking and overtime are higher for urban hospitals than in suburban hospitals. In contrast, interruptions, personal activities during night shifts, task break-ins, professional communication, waiting, breaks and social/personal tasks are higher for suburban hospitals than urban hospitals. Table 3 details the type of interruptions faced by the doctors working in EDs of urban and suburban hospitals (RQ4).
Table 3.
Types of interruptions in urban and suburban hospitals
| Interruptions (IN) | Urban | Suburban | |
| Variable | Mean±SD | Mean±SD | |
| Visual and auditory | IN2 | 4.04±1.025 | 4.19±0.751 |
| Phone calls | IN3 | 2.85±1.311 | 3.65±1.038 |
| Intrusions | IN4 | 3.50±1.222 | 3.99±0.778 |
| Rumination | IN5 | 3.01±1.221 | 4.07±0.943 |
Results and analysis of the observational study
Overall model
Table 4 and figure 3, the doctors spend most of their time in direct communication with patients (37.1%, 11.89±2.577), and documentation and prescribing (22.7%, 7.27±2.324) are found to be significant activities (RQ1).
Table 4.
Descriptive statistics of activities performed by doctors every 30 min
| Activities | Overall model | Urban hospital | Suburban hospital | |
| Mean±SD | Percentage (%) | Mean±SD | Mean±SD | |
| Direct communication with patients | 11.89±2.577 | 37.10 | 11.27±1.951 | 12.50±2.954 |
| Documentation and prescribing | 7.27±2.324 | 22.70 | 8.33±1.840 | 6.23±2287 |
| Patient data analysis | 3.08±1.865 | 9.60 | 3.18±2.448 | 2.98±0.997 |
| Indirect patient care | 2.13±1.037 | 6.60 | 2.80±0.718 | 1.46±0.859 |
| Waiting for patient, result, colleague | 1.82±1.845 | 5.70 | 0.35±0.477 | 3.27±1.508 |
| Social and personal activity | 1.56±1.154 | 4.90 | 0.68±0.532 | 2.43±0.920 |
| Professional communication (with colleagues) | 1.48±0.947 | 4.60 | 1.31±0.893 | 1.66±0.969 |
| Direct patient care | 1.36±0.618 | 4.20 | 1.61±0.573 | 1.11±0.559 |
| Walking | 1.21±0.916 | 3.80 | 1.07±0.789 | 1.35±1.009 |
| Breaks | 0.21±0.493 | 0.243 | 0.22±0.535 | 0.20±0.449 |
Figure 3.
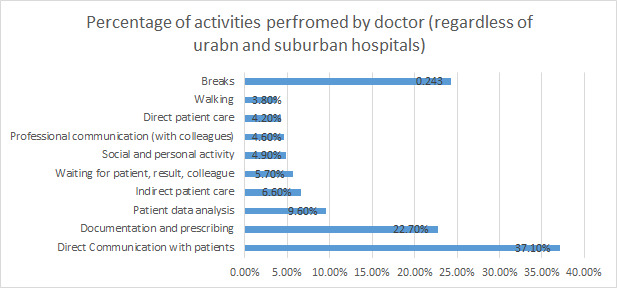
Percentage of activities performed by doctors (regardless of urban and suburban hospitals).
Region-wise analysis: comparison between urban and suburban hospitals
From table 4, it is evident that the frequency of direct communication with patients, waiting, social and personal activities, professional communication and walking are higher for the doctors working in suburban hospitals than in urban hospitals. In contrast, the frequency of documentation and prescription, patient data analysis, indirect patient care (including washing hands or sanitising before direct care), direct patient care (care that includes touching the patient) and breaks are higher for the doctors working in urban hospitals than in suburban hospitals (RQ4).
Discussion
Our results showed that the doctors spend most of their time in direct communication with patients (37.1%, 11.89±2.577) and documentation and prescribing (22.7%, 7.27±2.324) activities (RQ1). These findings confirmed previous studies in other countries and settings.5 Comparing the percentage of most frequent activities, that is, direct communication with patients, was even higher in a previous study (45.7%) than in the current study (37.1%). We separately analysed professional communication with colleagues (4.6%) and direct communication with patients (37.1%). And if we see the total percentage of communication activities, it becomes 41.7%, which is close to 45.7% of the previous study discussed above.5
Communication plays a fundamental role in the work environment of healthcare.17 It helps to perform teamwork to improve patient safety and outcomes,22 but at the same time, it can be an area of a critical issue when disruptive interruptions occur.17 This study found that resuming primary tasks after interruption was highly difficult for the doctors. These results confirmed the findings of previous studies.9 10 23 In ED work environments, visual and auditory distractions, ruminations and intrusions were frequent interruptions. The study found that the percentage of indirect care activities in the daily work pattern of ED doctors is higher than the direct care activities. Furthermore, the study found that the percentage of indirect care activities in the daily work pattern of ED doctors is higher than the direct care activities, confirming the findings of the previous studies.17
Based on the findings and results of this study, the results of the observation study are in line with the questionnaire survey. In both methods, direct communication with patients or information exchange was significant in the work pattern of the doctors working in EDs of hospitals. The comparison of indirect and direct care, and activities like professional communication, waiting and social and personal engagements among urban and suburban hospitals were also aligned (RQ3).
Recommendations for improvements in performance of the doctors
Multitasking and interruptions increase the risk of errors and significantly reduce the performance of doctors in EDs of hospitals.16 Based on the results of this study, a framework is proposed comprising recommendations to enhance the performance of ED doctors, as shown in figure 4.
Figure 4.
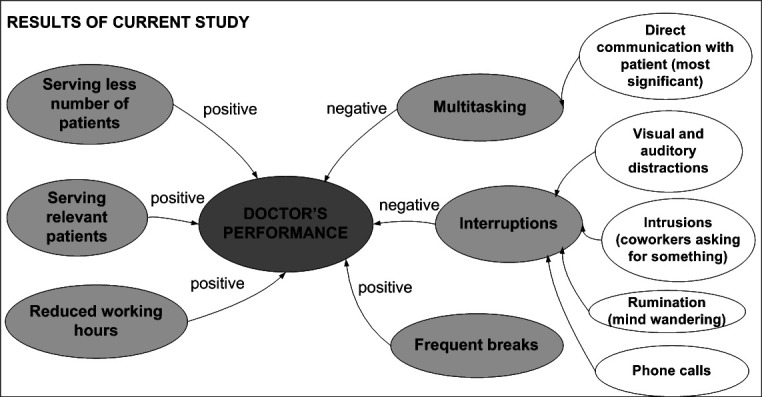
A proposed framework to improve doctors’ performances.
Acknowledgments
We would like to express our great appreciation to Muhammad Uzair and Munawar Irshad, who helped us get hospital permission to collect data for this study.
Footnotes
Contributors: All authors contributed equally to this research. AM and MJM conducted the study under the supervision and strong support of MS and MHA. AM is responsible for the overall content as the guarantor.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Provenance and peer review: Not commissioned; externally peer reviewed.
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Data availability statement
Data are available on reasonable request.
Ethics statements
Patient consent for publication
Not applicable.
Ethics approval
Ethical approval was obtained before the collection of data for the observation study. Participants in the questionnaire survey provided informed consent to researchers.
References
- 1.Weigl M, Müller A, Holland S, et al. Work conditions, mental workload and patient care quality: a multisource study in the emergency department. BMJ Qual Saf 2016;25:499–508. 10.1136/bmjqs-2014-003744 [DOI] [PubMed] [Google Scholar]
- 2.Chisholm CD, Collison EK, Nelson DR, et al. Emergency department workplace interruptions: are emergency physicians "interrupt-driven" and "multitasking"? Acad Emerg Med 2000;7:1239–43. 10.1111/j.1553-2712.2000.tb00469.x [DOI] [PubMed] [Google Scholar]
- 3.Chavez S, Long B, Koyfman A, et al. Coronavirus disease (COVID-19): a primer for emergency physicians. Am J Emerg Med 2021;44:220-229. 10.1016/j.ajem.2020.03.036 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Skaugset LM, Farrell S, Carney M, et al. Can you multitask? evidence and limitations of task switching and multitasking in emergency medicine. Ann Emerg Med 2016;68:189–95. 10.1016/j.annemergmed.2015.10.003 [DOI] [PubMed] [Google Scholar]
- 5.Göras C, Olin K, Unbeck M, et al. Tasks, multitasking and interruptions among the surgical team in an operating room: a prospective observational study. BMJ Open 2019;9:e026410. 10.1136/bmjopen-2018-026410 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Berg LM, Källberg A-S, Göransson KE, et al. Interruptions in emergency department work: an observational and interview study. BMJ Qual Saf 2013;22:656–63. 10.1136/bmjqs-2013-001967 [DOI] [PubMed] [Google Scholar]
- 7.Laarni J, Karvonen H, Pakarinen S, et al., eds. Multitasking and interruption management in control room operator work during simulated accidents. Springer: International Conference on Engineering Psychology and Cognitive Ergonomics, 2016. [Google Scholar]
- 8.Weigl M, Müller A, Vincent C, et al. The association of workflow interruptions and hospital doctors' workload: a prospective observational study. BMJ Qual Saf 2012;21:399–407. 10.1136/bmjqs-2011-000188 [DOI] [PubMed] [Google Scholar]
- 9.Westbrook JI, Coiera E, Dunsmuir WTM, et al. The impact of interruptions on clinical task completion. Qual Saf Health Care 2010;19:284–9. 10.1136/qshc.2009.039255 [DOI] [PubMed] [Google Scholar]
- 10.Walter SR, Dunsmuir WTM, Westbrook JI. Studying interruptions and multitasking in situ: the untapped potential of quantitative observational studies. Int J Hum Comput Stud 2015;79:118–25. 10.1016/j.ijhcs.2015.01.008 [DOI] [Google Scholar]
- 11.Berg LM, Ehrenberg A, Florin J, et al. An observational study of activities and multitasking performed by clinicians in two Swedish emergency departments. Eur J Emerg Med 2012;19:246–51. 10.1097/MEJ.0b013e32834c314a [DOI] [PubMed] [Google Scholar]
- 12.Berg LM, Källberg A-S, Ehrenberg A, et al. Factors influencing clinicians' perceptions of interruptions as disturbing or non-disturbing: a qualitative study. Int Emerg Nurs 2016;27:11–16. 10.1016/j.ienj.2016.01.003 [DOI] [PubMed] [Google Scholar]
- 13.Berg LM, Källberg A-S, Göransson KE, et al. Interruptions in emergency department work: an observational and interview study. BMJ Qual Saf 2013;22:656–63. 10.1136/bmjqs-2013-001967 [DOI] [PubMed] [Google Scholar]
- 14.Tucker AL, Spear SJ. Operational failures and interruptions in hospital nursing. Health Serv Res 2006;41:643–62. 10.1111/j.1475-6773.2006.00502.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Walter SR, Raban MZ, Dunsmuir WTM, et al. Emergency doctors' strategies to manage competing workload demands in an interruptive environment: an observational workflow time study. Appl Ergon 2017;58:454–60. 10.1016/j.apergo.2016.07.020 [DOI] [PubMed] [Google Scholar]
- 16.Raban MZ, Walter SR, Douglas HE, et al. Measuring the relationship between interruptions, multitasking and prescribing errors in an emergency department: a study protocol. BMJ Open 2015;5:e009076. 10.1136/bmjopen-2015-009076 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bellandi T, Cerri A, Carreras G, et al. Interruptions and multitasking in surgery: a multicentre observational study of the daily work patterns of doctors and nurses. Ergonomics 2018;61:40–7. 10.1080/00140139.2017.1349934 [DOI] [PubMed] [Google Scholar]
- 18.Arabadzhiyska PN, Baysari MT, Walter S, et al. Shedding light on junior doctors' work practices after hours. Intern Med J 2013;43:1321–6. 10.1111/imj.12223 [DOI] [PubMed] [Google Scholar]
- 19.Wong KK-K. Partial least squares structural equation modeling (PLS-SEM) techniques using SmartPLS. Marketing Bulletin 2013;24:1–32. [Google Scholar]
- 20.Chan Y. Biostatistics 102: quantitative data–parametric & non-parametric tests. Blood Press 2003;140:79. [PubMed] [Google Scholar]
- 21.Tavakol M, Dennick R. Making sense of Cronbach's alpha. Int J Med Educ 2011;2:53–5. 10.5116/ijme.4dfb.8dfd [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Deering S, Johnston LC, Colacchio K, eds. Multidisciplinary teamwork and communication training. Seminars in perinatology. Elsevier, 2011. [DOI] [PubMed] [Google Scholar]
- 23.Yen P-Y, Kelley M, Lopetegui M, et al., eds. Understanding and visualizing multitasking and task switching activities: a time motion study to capture nursing workflow. AMIA Annual Symposium Proceedings. American Medical Informatics Association, 2016. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjoq-2022-001813supp001.pdf (47.2KB, pdf)
Data Availability Statement
Data are available on reasonable request.