

Abstract
Background:
With the drastically aging population in the U.S., chronic subdural hematomas (cSDHs) are projected to represent the most common neurosurgical diagnosis requiring treatment within the next two decades. There is lack of contemporary outcome data in patients treated for nontraumatic and nonacute subdural hematoma. We aim to portray current mortality rates, complication rates, length of stay, and costs associated with inpatient cSDH care.
Methods:
The Premier Health-care Database, Premier Inc., Charlotte/NC was queried for encounters October 2016–December 2020 with the ICD-10 diagnoses of nontraumatic nonacute subdural hematoma as the principal diagnosis among patients age ≥40 years. Per database in-hospital mortality is defined as mortality in an inpatient who is not discharged. Complications represent medical conditions not present on admission that affects mortality, length of stay, and costs within the database.
Results:
The query identified 14,136 inpatient encounters. Between October 2016 and December 2020, in-hospital mortality rates averaged 10.9% in the medical group (MG) and 3.6% in the surgical group (SG) (P < 0.001). Complication rates averaged between 8.9 % in the MG and 19.9% in the SG (P < 0.001). LOS averaged 3.0 days in the MG and 5.7 days in the SG (P < 0.001). Total costs averaged $ 10,233 in the MG and $ 26,658 in the SG.
Conclusion:
The standardized outcomes presented represent an objective benchmark of contemporary cSDH treatment outcomes in the U.S. With the projected substantial increase of cSDH cases within the next decades, new treatment strategies such as middle meningeal embolization need to be explored and outperform current outcome metrics.
Keywords: Complications, Health-care database, Mortality, Subdural hematoma
INTRODUCTION
Chronic subdural hematoma (cSDH) represents a prototypical disease of the elderly. Due to the demographic changes driven by an aging population with increased life expectancies, cSDH incidence has been increasing worldwide. Projections quantified cSDH to become the most prevalent neurosurgical diagnosis requiring treatment by 2030, hence, putting a substantial burden on the health-care systems.[1,15,18,19,24,25] Indications for surgical treatment are based on symptomatology and mass effect in the form of hematoma thickness or midline shift. Craniotomy or surgical burr-hole evacuation with irrigation and placement of a drain for 24–48 h is considered standard of care.[16,21,23] However, on average, 10–20% of patients suffer recurrence of the cSDH with a substantial portion requiring reoperation. Among the elderly or patients with significant comorbidities or coagulopathies, the recurrence rates are even higher.[7,13,22,26,27] Recently, neuroendovascular embolization of the middle meningeal artery (MMA) has been shown to be a safe and effective treatment modality for subsets of cSDHs. Either as an adjunct to surgery or stand-alone treatment, recurrence rates as well as surgical re-treatment rates have been significantly reduced.[2,4,9,11,12] Shortened length of inpatient stay and decreased retreatment rates translated into significantly decreased 1-year hospital costs.[5] However, high class evidence for MMA embolization from randomized-controlled trials is yet pending. Multiple trials are proposed or already underway to elucidate the efficacy of MMA embolization.[6]
Optimizing outcomes by reducing hematoma recurrence, length of inpatient stays, and complications as well as improving functional outcomes are fundamental to mitigate the clinical, economic, and health-care burden of cSDHs. Contemporary outcome data for inpatient cSDH patients are lacking. The present study aimed to provide a comprehensive understanding of in-hospital mortality, complication rates, length of stay, and costs that portray the contemporary burden of cSDH in the U.S.
The authors queried the Premier Health-care Database (PHD, Premier Inc., Charlotte, NC) to provide outcomes of more than 14,000 U.S. inpatient cases with nontraumatic and nonacute subdural hematomas treated between 2016 and 2020.
MATERIALS AND METHODS
The PHD, Premier Inc, Charlotte, NC is an all-payer database that collects U.S. hospital-based information. To date, the database exceeds 1 billion patient encounters from over 230 million unique patients and 120 million inpatient admissions. Supplied by more than 800 U.S. hospitals, about 20% of all U.S. inpatient discharges over the past decade are congregated in the PHD. For this analysis, the authors queried the database for all patients between October 2016 and December 2020 using the parameters of ICD-10 I62.00, I62.02, and I62.03 as the principal diagnosis. For all eligible patients, outcome data elements for in-hospital mortality, complications, length of stay, and costs were collected. Data were grouped into surgically and medically treated patients and further stratified by age, sex, race, and year of treatment.
Per PHD, in-hospital mortality is defined as a mortality in an inpatient who is not discharged to another facility, hospital, or center. Complications are defined as medical conditions not present on admission that affect mortality, length of stay, and costs. Eighteen predefined hospital acquired conditions – such as infections, falls, venous thromboembolism, and serious preventable events – plus another 82 conditions identified by Premier comprise these clinical conditions. Length of stay represents time spent as inpatient. Costs are obtained from either data submitted by the hospital’s or health-care system’s accounting system or are calculated based on annual Medicare cost reports. Medical and surgical treatment groups were compared using Student’s t-tests within the PHD.
RESULTS
Dataset
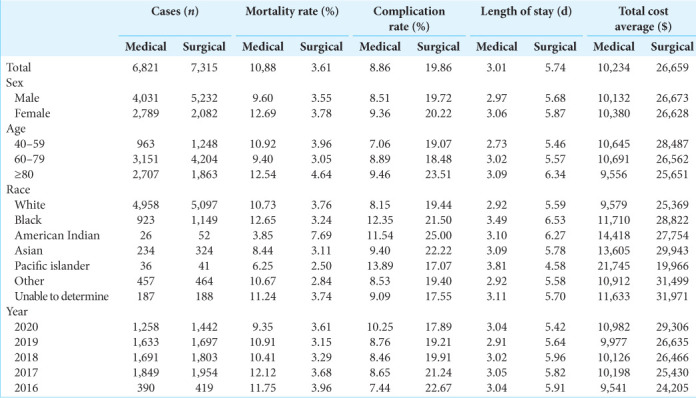
In the study period October 2016–December 2020, a total of 14,136 inpatient cases were available for analysis with 6821 in the medical group (MG) and 7315 in the surgical group (SG). In the MG, 59.1% were male, 72.7% were Caucasian, 46.2% were between 60 and 79 years old, and 36.7% were ≥80 years old. In the SG, 71.5% were male, 69.7% were Caucasian, 57.5% were between 60 and 70 years old, and 25.5% were ≥80 years old [Table 1].
Table 1:
Outcome metrics among chronic subdural hematomas in the U.S.
In-hospital mortality
Collectively, in-hospital mortality rate was 10.88% in the MG and 3.61% in the SG (P < 0.001). Descriptively, in the MG, it was highest in females, patients ≥80 years and Afro-American race, while its annual average trended toward a decline during the study period 2016–2020. In the SG, the in-hospital mortality was similar in males and females. It was higher in patients ≥80 years and highest among the American Indian race which, however, represented only a small fraction of all cases (52/7315, 0.71% of surgical cases). The in-hospital mortality rates remained stable during the study period [Table 1 and Figure 1].
Figure 1:

Observed outcomes among chronic subdural hematomas in the U.S.
Complications
The complication rate in the MG was 8.86% and 19.86% in the SG (P < 0.001). In the MG, it was higher in females, patients ≥80 years, and nonCaucasians. The annual average during the study period was stable with a marked increase from about 8–10% in 2020. In the SG, the averaged complication rate was 19.86% and similar in males and females. It was higher in patients ≥80 years and highest among the American Indian race which, however, represented only a small fraction of all cases. The average complication rate declined annually during the study period [Table 1 and Figure 1].
Length of stay
Average length of stay in the MG was 3.01 days and significantly shorter than average length of stay in the SG with 5.74 (P < 0.001). Overall, among subgroups of sex, age, race, and year, lengths of stay were similar within the surgical and medical subgroups.
Costs
Total cost average was $10,234 in the MG and $26,659 in the SG (P < 0.001). While among subgroups of sex, age, and year costs were similar, there was considerable disparity of costs in both the medical and SGs among races.
DISCUSSION
While there are numerous studies exploring outcomes in acute and traumatic subdural hematomas, contemporary data of U.S. inpatient treatment for nonacute and nontraumatic subdural hematomas are lacking. The aim of this study was therefore to provide contemporary objective outcome descriptive of surgically and medically treated inpatients ≥40 years suffering from cSDH. These data points provide an objective benchmark for yet to come prospective trials that aim to elucidate the efficacy of MMA embolization.
Medical complications and comorbidities are the predominant driver of in-hospital mortality among cSDH patients. Intracranial hemorrhage and infection such as subdural empyema represent severe but rare complications generating poor outcomes among surgically treated cSDH patients.[20] The rate of complications in the presented PHD query averaged 20% in the SG demonstrating that despite an average mortality rate of 3.6% in the SG, still one out of five patients suffers a medical condition that negatively affects length of stay, overall costs, and eventually functional outcome. Previously, the Nationwide Inpatient Sample (NIS) and University Health System Consortium (UHC) provided objective outcomes metrics of nontraumatic subdural hematoma[3,10] In the U.S. NIS analysis, 14,093 cases hospitalized for nontraumatic subdural hematoma between 2007 and 2009 were analyzed. The surgically treated group comprised 51.4% in line with the presented PHD query. The authors identified an overall in-hospital mortality of 11.8%. Surgically treated patients had significantly lower odds ratio for mortality.[3] An analysis of the inpatients treated for nontraumatic subdural hematoma from the UHC identified 16,928 cases treated between 2011 and 2015. Overall mortality was reported 9.5% averaged by 5.6% in the SG and 12.5% in the MG. Length of stay averaged 6.8 days and was longer in the surgical compared to the MG (8.6 days vs. 3.2 days).[10] Importantly, both databases included patients age ≥18 as well as acute nontraumatic subdural hematoma patients. Adding the nontraumatic, acute subdural hematoma ICD code to the presented PHD query, in a total of 25,169 cases, the overall mortality was 9.1% (5.6% in the SG and 12.7% in the MG), and thus on par with the observations of the UHC. The significant gap between in-hospital and reported one-year mortality rates (up to ~30%) mirror that cSDH represents a sentinel health-care event and that the post-hospital period is yet to be further explored as well.[8,14,17]
There herein presented PHD query provided contemporary descriptive outcomes of nontraumatic nonacute SDH ≥40 years which may represent typical candidates for MMA embolization trials. In the unmatched comparison, medically treated cSDH had significantly higher mortality compared to surgically treated patients. In contrast, the complication rate, length of stay, and costs were significantly higher in the SG.
Limitations
Allocation of patients into the medical or SGs is likely to be highly biased by criteria such as hematoma thickness, midline shift, neurological status, and comorbidities. Administrative database such as the NIS or PHD is subject to recruitment bias since only a subset of nationwide health systems are affiliated with databases. Despite these shortcomings, database queries such as the one presented here delineate objective aggregated data that portrays baseline data supporting generation of future study designs and facilitating appropriate power calculations. The lack of access to further individual patient level data did not allow further dataset analysis.
CONCLUSION
The standardized outcomes presented represent an objective benchmark of contemporary cSDH treatment outcomes in the U.S. With the projected substantial increase of cSDH cases within the next decades, new treatment strategies need to be explored and outperform current outcome metrics.
Footnotes
How to cite this article: Hendrix P, Goren O, Dalal S, Kanmounye US, Weiner GM, Schirmer CM, et al. In-hospital mortality rates, complication rates, length of stay, and total costs of >14,000 chronic subdural hematomas treated in the U.S. between 2016 and 2020: Query of the premier health-care database. Surg Neurol Int 2022;13:364.
Contributor Information
Philipp Hendrix, Email: phendrix@geisinger.edu.
Oded Goren, Email: ogoren@geisinger.edu.
Shamsher Dalal, Email: ssdalal@geisinger.edu.
Ulrick Sidney Kanmounye, Email: ukanmounyekouokam@geisinger.edu.
Gregory M. Weiner, Email: gweiner@geisinger.edu.
Clemens M. Schirmer, Email: cmschirmer@geisinger.edu.
Itay Melamed, Email: imelamed@geisinger.edu.
Declaration of patient consent
Patients’ consent not required as patients’ identities were not disclosed or compromised.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Balser D, Farooq S, Mehmood T, Reyes M, Samadani U. Actual and projected incidence rates for chronic subdural hematomas in United States veterans administration and civilian populations. J Neurosurg. 2015;123:1209–15. doi: 10.3171/2014.9.JNS141550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ban SP, Hwang G, Byoun HS, Kim T, Lee SU, Bang JS, et al. Middle meningeal artery embolization for chronic subdural hematoma. Radiology. 2018;286:992–9. doi: 10.1148/radiol.2017170053. [DOI] [PubMed] [Google Scholar]
- 3.Busl KM, Prabhakaran S. Predictors of mortality in nontraumatic subdural hematoma. J Neurosurg. 2013;119:1296–301. doi: 10.3171/2013.4.JNS122236. [DOI] [PubMed] [Google Scholar]
- 4.Catapano JS, Ducruet AF, Nguyen CL, Cole TS, Baranoski JF, Majmundar N, et al. A propensity-adjusted comparison of middle meningeal artery embolization versus conventional therapy for chronic subdural hematomas. J Neurosurg. 2021:1–6. doi: 10.3171/2020.9.JNS202781. Online ahead of print. [DOI] [PubMed] [Google Scholar]
- 5.Catapano JS, Koester SW, Srinivasan VM, Rumalla K, Baranoski JF, Rutledge C, et al. Total 1-year hospital cost of middle meningeal artery embolization compared to surgery for chronic subdural hematomas: A propensity-adjusted analysis. J Neurointerv Surg. 2022;14:804–6. doi: 10.1136/neurintsurg-2021-018327. [DOI] [PubMed] [Google Scholar]
- 6.Catapano JS, Nguyen CL, Wakim AA, Albuquerque FC, Ducruet AF. Middle meningeal artery embolization for chronic subdural hematoma. Front Neurol. 2020;11:557233. doi: 10.3389/fneur.2020.557233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Chon KH, Lee JM, Koh EJ, Choi HY. Independent predictors for recurrence of chronic subdural hematoma. Acta Neurochir (Wien) 2012;154:1541–8. doi: 10.1007/s00701-012-1399-9. [DOI] [PubMed] [Google Scholar]
- 8.Dumont TM, Rughani AI, Goeckes T, Tranmer BI. Chronic subdural hematoma: A sentinel health event. World Neurosurg. 2013;80:889–92. doi: 10.1016/j.wneu.2012.06.026. [DOI] [PubMed] [Google Scholar]
- 9.Ironside N, Nguyen C, Do Q, Ugiliweneza B, Chen CJ, Sieg EP, et al. Middle meningeal artery embolization for chronic subdural hematoma: A systematic review and meta-analysis. J Neurointerv Surg. 2021;13:951–7. doi: 10.1136/neurintsurg-2021-017352. [DOI] [PubMed] [Google Scholar]
- 10.Joseph JR, Smith BW, Williamson CA, Park P. Seizure correlates with prolonged hospital stay, increased costs, and increased mortality in nontraumatic subdural hematoma. World Neurosurg. 2016;92:366–70. doi: 10.1016/j.wneu.2016.05.033. [DOI] [PubMed] [Google Scholar]
- 11.Joyce E, Bounajem MT, Scoville J, Thomas AJ, Ogilvy CS, Riina HA, et al. Middle meningeal artery embolization treatment of nonacute subdural hematomas in the elderly: A multiinstitutional experience of 151 cases. Neurosurg Focus. 2020;49:E5. doi: 10.3171/2020.7.FOCUS20518. [DOI] [PubMed] [Google Scholar]
- 12.Kan P, Maragkos GA, Srivatsan A, Srinivasan V, Johnson J, Burkhardt JK, et al. Middle meningeal artery embolization for chronic subdural hematoma: A multi-center experience of 154 consecutive embolizations. Neurosurgery. 2021;88:268–77. doi: 10.1093/neuros/nyaa379. [DOI] [PubMed] [Google Scholar]
- 13.Knopman J, Link TW, Navi BB, Murthy SB, Merkler AE, Kamel H. Rates of repeated operation for isolated subdural hematoma among older adults. JAMA Netw Open. 2018;1:e183737. doi: 10.1001/jamanetworkopen.2018.3737. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Miranda LB, Braxton E, Hobbs J, Quigley MR. Chronic subdural hematoma in the elderly: Not a benign disease. J Neurosurg. 2011;114:72–6. doi: 10.3171/2010.8.JNS10298. [DOI] [PubMed] [Google Scholar]
- 15.Neifert SN, Chaman EK, Hardigan T, Ladner TR, Feng R, Caridi JM, et al. Increases in subdural hematoma with an aging population-the future of American cerebrovascular disease. World Neurosurg. 2020;141:e166–74. doi: 10.1016/j.wneu.2020.05.060. [DOI] [PubMed] [Google Scholar]
- 16.Peng D, Zhu Y. External drains versus no drains after burr-hole evacuation for the treatment of chronic subdural haematoma in adults. Cochrane Database Syst Rev. 2016;2016:CD011402. doi: 10.1002/14651858.CD011402.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Posti JP, Luoto TM, Sipilä JOT, Rautava P, Kytö V. Prognosis of patients with operated chronic subdural hematoma. Sci Rep. 2022;12:7020. doi: 10.1038/s41598-022-10992-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rauhala M, Helén P, Huhtala H, Heikkilä P, Iverson GL, Niskakangas T, et al. Chronic subdural hematoma-incidence, complications, and financial impact. Acta Neurochir (Wien) 2020;162:2033–43. doi: 10.1007/s00701-020-04398-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Rauhala M, Luoto TM, Huhtala H, Iverson GL, Niskakangas T, Öhman J, et al. The incidence of chronic subdural hematomas from 1990 to 2015 in a defined Finnish population. J Neurosurg. 2019;132:1147–57. doi: 10.3171/2018.12.JNS183035. [DOI] [PubMed] [Google Scholar]
- 20.Rohde V, Graf G, Hassler W. Complications of burr-hole craniostomy and closed-system drainage for chronic subdural hematomas: A retrospective analysis of 376 patients. Neurosurg Rev. 2002;25:89–94. doi: 10.1007/s101430100182. [DOI] [PubMed] [Google Scholar]
- 21.Santarius T, Kirkpatrick PJ, Ganesan D, Chia HL, Jalloh I, Smielewski P, et al. Use of drains versus no drains after burr-hole evacuation of chronic subdural haematoma: A randomised controlled trial. Lancet. 2009;374:1067–73. doi: 10.1016/S0140-6736(09)61115-6. [DOI] [PubMed] [Google Scholar]
- 22.Schmidt L, Gørtz S, Wohlfahrt J, Melbye M, Munch TN. Recurrence of subdural haematoma in a population-based cohort risks and predictive factors. PLoS One. 2015;10:e0140450. doi: 10.1371/journal.pone.0140450. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Soleman J, Lutz K, Schaedelin S, Kamenova M, Guzman R, Mariani L, et al. Subperiosteal vs subdural drain after burr-hole drainage of chronic subdural hematoma: A randomized clinical trial (cSDH-Drain-Trial) Neurosurgery. 2019;85:E825–34. doi: 10.1093/neuros/nyz095. [DOI] [PubMed] [Google Scholar]
- 24.Stubbs DJ, Vivian ME, Davies BM, Ercole A, Burnstein R, Joannides AJ. Incidence of chronic subdural haematoma: A single-centre exploration of the effects of an ageing population with a review of the literature. Acta Neurochir (Wien) 2021;163:2629–37. doi: 10.1007/s00701-021-04879-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Tommiska P, Luostarinen T, Kaprio J, Korja M, Lönnrot K, Kivisaari R, et al. Incidence of surgery for chronic subdural hematoma in Finland during 1997-2014: A nationwide study. J Neurosurg. 2022;136:1186–93. doi: 10.3171/2021.3.JNS21281. [DOI] [PubMed] [Google Scholar]
- 26.Torihashi K, Sadamasa N, Yoshida K, Narumi O, Chin M, Yamagata S. Independent predictors for recurrence of chronic subdural hematoma: A review of 343 consecutive surgical cases. Neurosurgery. 2008;63:1125–9. doi: 10.1227/01.NEU.0000335782.60059.17. [DOI] [PubMed] [Google Scholar]
- 27.Weigel R, Schmiedek P, Krauss JK. Outcome of contemporary surgery for chronic subdural haematoma: Evidence based review. J Neurol Neurosurg Psychiatry. 2003;74:937–43. doi: 10.1136/jnnp.74.7.937. [DOI] [PMC free article] [PubMed] [Google Scholar]