

Abstract
Aim
Survival of traumatic out‐of‐hospital cardiac arrest (OHCA) is poor. Early use of advanced airway management (AAM) techniques, including endotracheal intubation and supraglottic devices, are expected to contribute to the improved survival of these patients. The aim of this study was to determine whether prehospital use of AAM improves the outcomes for emergency medical service (EMS)‐witnessed traumatic OHCA.
Methods
A nationwide retrospective study was carried out. Trauma patients with EMS‐witnessed cardiac arrest who received cardiopulmonary resuscitation during transport were included. Patients younger than 16 years and those with missing data were excluded. We compared two groups using propensity score matching. The primary outcome was survival to discharge. The secondary outcome was return of spontaneous circulation (ROSC) on hospital arrival. A logistic regression model was used to calculate odds ratios (OR) and confidence intervals (CI).
Results
After propensity score matching, 1,346 patients were enrolled (AAM 673 versus non‐AAM 673). Forty‐four AAM cases (6.5%) and 39 non‐AAM cases (5.8%) survived. Logistic regression analysis did not show a contribution of AAM for survival to discharge (AAM 44/673 (6.5%), non‐AAM 39/673 (5.8%); OR 1.12; 95% CI, 0.70–1.76; P = 0.64). However, AAM improved ROSC on admission (AAM 141/673 (21.0%), non‐AAM 77/673 (11.4%); OR 2.05; 95% CI, 1.51–2.78; P < 0.001). This tendency was consistent throughout our subgroup analysis categorized by body region of the severe injury (head trauma, torso trauma, and extremity/spine trauma).
Conclusions
Prehospital AAM among EMS‐witnessed traumatic OHCA patients was not associated with survival to discharge; however, ROSC on hospital admission improved for the AAM patients.
Keywords: AAM, Endotracheal intubation, JTDB, supraglottic airway, traumatic cardiac arrest
Conditional logistic regression analysis revealed that ROSC on admission was associated with prehospital AAM, but not associated with survival to discharge.
![]()
INTRODUCTION
Trauma is one of the most common causes of death worldwide. 1 Regardless of progress in traumatology and improvements in prehospital medical systems and intensive care medicine, salvaging traumatic out‐of‐hospital cardiac arrest (OHCA) patients is still one of the most difficult challenges. 2 Therefore, resuscitation efforts for traumatic OHCA have been occasionally considered futile in the prehospital setting and debate continues regarding the benefit of prehospital cardiopulmonary resuscitation (CPR) in trauma. 2 , 3 However, some subgroups of traumatic OHCA patients are indicated as potentially salvageable. 4
The pathophysiology of traumatic OHCA differs from that of nontraumatic (medical) OHCA. 5 As optimal oxygenation and ventilation by securing a definitive airway could be beneficial in the resuscitation process, we investigated whether secured airway management improved the outcomes of traumatic OHCA patients.
Advanced airway management (AAM), including endotracheal intubation (ETI) and the use of supraglottic airway (SGA) devices, is currently one of the most crucial methods used to secure airways for OHCA patients in the prehospital setting. The European Resuscitation Council Guidelines for Resuscitation recommend to secure airway and maximize oxygenation for patients with traumatic cardiac arrest. 6 Advanced Trauma Life Support guidelines recommend performing ETI for patients with a Glasgow Coma Scale (GCS) score less than or equal to 8 and for those with a GCS score more than or equal to 2 deterioration among traumatic patients without cardiac arrest. 7 However, there is still limited evidence regarding the use of AAM for traumatic OHCA patients, especially its early use and with consideration of the injured body region. Therefore, the current study aimed to determine whether early use of prehospital AAM improves the outcomes of traumatic OHCA patients using the Japan Trauma Data Bank (JTDB), a large‐scale, nationwide, multicenter trauma patient database. As various mechanisms are involved in traumatic OHCA, more robust designs are necessary to delineate whether AAM provides a survival advantage. To enhance the quality of the study and stratify the patients who might benefit the most from AAM use, this study was limited to emergency medical service (EMS)‐witnessed traumatic OHCA patients.
METHODS
Emergency medical system and providers
In Japan, the fire defense headquarters of each local government manages their own EMS. Japan implemented the Anglo‐American EMS system, where patients are brought to physicians by prehospital medical providers. All certified emergency medical technicians (emergency life‐saving technicians, ELSTs) are allowed to use SGA devices for cardiac arrest patients if the patient's airway is unsecured. Only specially trained ELSTs, who undergo additional training compared to basic emergency medical technicians, are allowed to perform ETI under instruction from physicians, who provide navigation over the telephone when patients are in cardiac arrest. They are also allowed to give fluid resuscitation to patients in shock or with crush syndrome. 8 When an ambulance staffed with physicians is dispatched, the physicians typically perform ETI if needed.
Study design and data collection
The Okayama University Ethics Committee approved the study (K2007‐002) and waived the requirement for written informed consent.
We reviewed the JTDB (2004–2017), a nationwide trauma registry. All trauma patients registered in the Data Bank were screened. The JTDB data are collected through a Web‐based form and registered by emergency physicians in cooperation with medical assistants. We included patients aged 16 years old or older with traumatic OHCA occurring after leaving the scene (EMS‐witnessed traumatic OHCA) who received CPR during transport. Mortality among traumatic OHCA patients is extremely low, which could give rise to selection bias. To minimize this bias and eliminate dead or nearly dead patient, we excluded patients with OHCA at the trauma scene, which was defined as patients having neither a blood pressure nor a heart rate. Also, for the same reason, patients with Abbreviated Injury Scale (AIS) scores of 6 (lethal trauma) or 9 for any body region (unknown or missing AIS), missing data on return of spontaneous circulation (ROSC) on hospital admission (ROSC defined as heart rate >0 and systolic blood pressure >0), and patients with burns and unknown prehospital AAM use were omitted.
The JTDB includes the following characteristics of patients who sustained injuries: vital signs on admission, heart rate, systolic blood pressure, respiratory rate, type and mechanism of trauma, GCS score, means of transportation (ambulance, ambulance staffed with physicians or other types of medical personnel), Injury Severity Score (ISS), AIS, Revised Trauma Score, emergent surgical intervention for hemorrhage (craniotomy, craterization, thoracotomy, celiotomy, bone fixation, arterial embolization, and operation for hemorrhage), need for transfusion within 24 h, ROSC on admission, and survival to discharge.
We compared two traumatic OHCA groups: the AAM group, defined as patients receiving AAM including prehospital ETI or use of SGA device, and the non‐AAM group, defined as patients not receiving AAM. Use of the AAM was identified from the JTDB registry on hospital arrival settings. The primary outcome was survival to discharge. The secondary outcome was ROSC on admission.
Data analysis
To minimize various confounders, we carried out propensity score (PS) matching. The PS was calculated using multivariable regression to predict the likelihood of AAM versus non‐AAM use based on patient characteristics that could influence the treatment assignment. 9 The PS model included patient characteristics (sex, age), mechanism of trauma (blunt or nonblunt), prehospital physician involvement (ambulance staffed with physicians or not), and head trauma, which could affect patients' prognosis for different physiological changes. A nearest neighbor matching algorithm without replacement was used. With evolving trauma care including permissive hypotension, restricted prehospital fluid resuscitation, and transfusion balance, improved survival rate was expected. Therefore, to achieve a good balance of patients' distribution, PS matching was binned with the year the patient was admitted to the hospital (2004–2008, 2009–2013, 2014–2017). Success of the PS matching process was evaluated using standardized differences for each PS variable, with an absolute standardized difference of <0.2 considered to represent good balance between the matched pairs. 10 , 11
After PS matching, we undertook a univariable comparison of the AAM and non‐AAM groups using conditional logistic regression to evaluate the effect of prehospital AAM on ROSC and survival to discharge. 12 The results of logistic regression are described using odds ratios (OR) and 95% confidence intervals (CI).
Furthermore, we undertook a subgroup analysis using conditional logistic regression analysis based on body regions where the severe injury occurred, as physiological impact could differ depending on the injury site (severe head injury, severe torso (chest or abdominal) injury, severe extremity/spine injury). 13 Severe injury was defined as AIS ≥ 3. The same analyses were applied for each respective subgroup.
Statistical analyses were carried out using STATA/IC 15 (StataCorp, Lakeway, TX, USA).
RESULTS
Patient flowchart and baseline characteristics
Among 294,274 available patients in the JTDB, 8,843 patients with EMS‐witnessed traumatic OHCA receiving CPR during transport were eligible. After excluding patients, a total of 5,144 patients were enrolled in the study. Of those patients, 740 had AAM performed in prehospital settings and 4,404 patients were transported without AAM (Fig. 1).
Fig. 1.
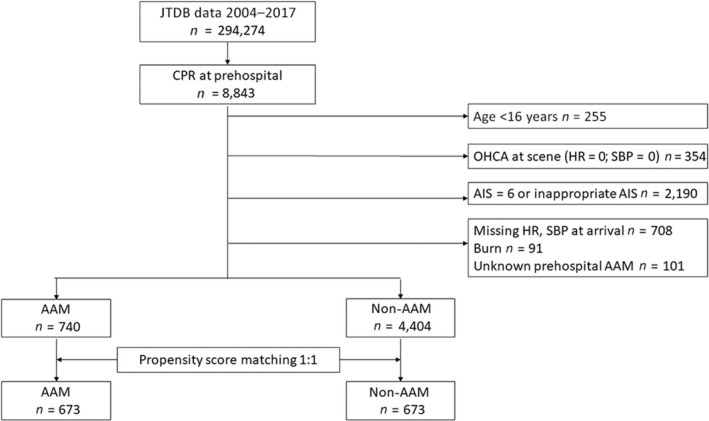
Flowchart of patients analyzed in the study. AAM, advanced airway management; AIS, Abbreviated Injury Scale; CPR, cardiopulmonary resuscitation; HR, heart rate; JTDB, Japan Trauma Data Bank; OHCA, out‐of‐hospital cardiac arrest; SBP, systolic blood pressure.
Table 1 shows patient characteristics. Patients in the AAM group were more frequently transported by ambulances staffed with physicians (non‐AAM, 4.5%; AAM, 30.1%). The AAM group patients received intravenous access (non‐AAM, 16.5%; AAM, 46.8%) and defibrillation (non‐AAM, 2.4%; AAM, 4.3%) more frequently. The incidence of severe chest injury was similar in both groups (non‐AAM, 68.7%; AAM, 68.8%), and consequently, thoracotomy was performed for some cases in both groups (non‐AAM, 14.1%; AAM, 18.2%). The AAM group was more likely to receive transfusion within 24 h compared to the non‐AAM group (non‐AAM, 15.8%; AAM, 22.0%).
Table 1.
Characteristics and epidemiology of enrolled patients with emergency medical service‐witnessed traumatic out‐of‐hospital cardiac arrest
| Non‐AAM | AAM | P‐value | |
|---|---|---|---|
| n = 4,404 | n = 740 | ||
| Age, years; mean (SD) | 52.9 (20.5) | 54.1 (20.5) | 0.140 |
| Gender, n (%) | |||
| Male | 2,999 (68.1) | 517 (69.9) | 0.430 |
| Time period | |||
| 2004–2008 | 851 (19.3) | 131 (17.7) | 0.061 |
| 2009–2013 | 2,265 (51.4) | 361 (48.7) | |
| 2014–2017 | 1,288 (29.2) | 248 (33.5) | |
| Type of trauma | |||
| Blunt | 4,029 (91.5) | 692 (93.5) | 0.089 |
| Penetrating | 263 (6.0) | 38 (5.1) | |
| Other | 112 | 10 | |
| Means of transportation | |||
| Ambulance | 4,051 (92.0) | 381 (51.5) | <0.001 |
| Car staffed with doctor | 199 (4.5) | 223 (30.1) | |
| Other | 112 | 136 | |
| EMS intervention | |||
| IV access | 725 (16.5) | 346 (46.8) | <0.001 |
| Defibrillation | 107 (2.4) | 32 (4.3) | 0.003 |
| ISS | 29 (20–41) | 29 (24–41) | 0.100 |
| AIS ≥ 3 | |||
| Head | 2,146 (48.7) | 355 (48.0) | 0.700 |
| Chest | 3,027 (68.7) | 509 (68.8) | 0.980 |
| Abdomen | 321 (7.3) | 76 (10.3) | 0.005 |
| Extremity/spine | 2,008 (45.6) | 329 (44.5) | 0.570 |
| Vitals on hospital admission, median (IQR) | |||
| SBP | 0 (0–0) | 0 (0–0) | <0.001 |
| HR | 0 (0–0) | 0 (0–0) | <0.001 |
| RR | 0 (0–0) | 0 (0–0) | <0.001 |
| GCS | 3 (3–3) | 3 (3–3) | 0.140 |
| Surgical intervention within 24 h | |||
| Craniotomy | 23 (0.52) | 6 (0.81) | 0.330 |
| Craterization | 30 (0.68) | 12 (1.6) | 0.009 |
| Thoracotomy | 622 (14.1) | 135 (18.2) | 0.003 |
| Celiotomy | 138 (3.1) | 42 (5.7) | <0.001 |
| Bone fixation | 34 (0.77) | 5 (0.68) | 0.780 |
| TAE | 50 (1.1) | 15 (2.0) | 0.044 |
| Arrest hemorrhage | 57 (1.3) | 25 (3.4) | <0.001 |
| Blood transfusion within 24 h | 694 (15.8) | 163 (22.0) | <0.001 |
| RTS, median (IQR) | 0 (0–0) | 0 (0–0) | <0.001 |
Data are shown n (%) unless otherwise indicated. AAM, advanced airway management; AIS, Abbreviated Injury Scale; EMS, emergency medical service; GCS, Glasgow Coma Scale; HR, heart rate; ISS, Injury Severity Score; IV, intravenous; RR, respiratory rate; RTS, Revised Trauma Score; SBP, systolic blood pressure; SD, standard deviation; TAE, transarterial embolization.
Propensity‐matched cohort analyses
Table 2 shows results of the PS matching. We matched 1,346 patients in a 1:1 ratio (non‐AAM, 673 patients; AAM, 673 patients). The mean ages were 55.2 (standard deviation, 20.9) years in the non‐AAM group and 53.7 (standard deviation, 20.5) years in the AAM group. The same number of patients (180) were transported by ambulances staffed with physicians in the AAM group and non‐AAM group, respectively. The median ISS was 26 (IQR, 21–41) in the non‐AAM group and 29 (IQR, 24–41) in the AAM group.
Table 2.
Demographics of patients with emergency medical service‐witnessed traumatic out‐of‐hospital cardiac arrest treated with advanced airway management (AAM group) and the non‐AAM group for matched data
| Non‐AAM n = 673 |
AAM n = 673 |
Absolute SMD | |
|---|---|---|---|
| Age, years; mean (SD) | 55.2 (20.9) | 53.7 (20.5) | 0.069 |
| Gender | |||
| Male | 470 (69.8) | 464 (68.9) | 0.019 |
| Time period | |||
| 2004–2008 | 101 (15.0) | 101 (15.0) | – |
| 2009–2013 | 342 (50.8) | 342 (50.8) | – |
| 2014–2017 | 230 (34.2) | 230 (34.2) | – |
| Type of trauma | |||
| Blunt | 621 (92.3) | 628 (93.3) | 0.040 |
| Prehospital physician involvement | 180 (26.7) | 180 (26.7) | 0.000 |
| ISS, median (IQR) | 26 (21–41) | 29 (24–41) | 0.049 |
| Head trauma | 343 (51.0) | 379 (56.3) | 0.107 |
Data are shown n (%) unless otherwise indicated. IQR, interquartile range; ISS, Injury Severity Score; SD, standard deviation; SMD, standardized mean difference.
The results of primary and secondary outcomes are shown in Table 3. Thirty‐nine cases (5.8%) in the non‐AAM group and 44 cases (6.5%) in the AAM group survived. As a secondary outcome, 77 cases (11.4%) in the non‐AAM and 141 cases (21.0%) in the AAM group had ROSC on hospital admission. Conditional logistic regression analysis revealed that prehospital AAM was associated with the increase in ROSC on hospital admission (OR 2.05; 95% CI, 1.51–2.78, P < 0.001); however, prehospital AAM was not associated with survival to discharge (OR 1.12; 95% CI, 0.70–1.76; P = 0.64) in this analysis.
Table 3.
Primary and secondary outcomes in this study of patients with emergency medical service‐witnessed traumatic out‐of‐hospital cardiac arrest
| Non‐AAM | AAM | OR | 95% CI | P‐value | |
|---|---|---|---|---|---|
| ROSC on admission | 77/673 (11.4%) | 141/673 (21.0%) | 2.05 | 1.51–2.78 | <0.001 |
| Survival to discharge | 39/673 (5.8%) | 44/673 (6.5%) | 1.12 | 0.70–1.76 | 0.64 |
Conditional logistic regression analysis revealed that return of spontaneous circulation (ROSC) on admission was associated with prehospital advanced airway management (AAM), but not associated with survival to discharge. CI, confidence interval; OR, odds ratio.
Table 4 shows the results of the subgroup analysis. Return of spontaneous circulation improved significantly in all groups (severe head injury: OR 1.68; 95% CI, 1.05–2.68; P = 0.03; severe torso injury: OR 2.46; 95% CI, 1.56–3.88; P < 0.001; severe extremity/spine injury: OR 2.73; 95% CI, 1.37–5.44; P = 0.004). However, survival to discharge did not improve (severe head injury: OR 1.17; 95% CI, 0.54–2.52; P = 0.70; severe torso injury: OR 1.00; 95% CI, 0.48–2.10; P = 1.00; severe extremity/spine injury: OR 1.13; 95% CI, 0.43–2.92; P = 0.81), respectively.
Table 4.
Subgroup analysis for return of spontaneous circulation (ROSC) and survival to discharge among trauma patients grouped by injured body part
| Cases | OR | 95% CI | P‐value | ||
|---|---|---|---|---|---|
| Head AIS ≥ 3 | 649 | ROSC on admission | 1.68 | 1.05–2.68 | 0.030 |
| Survival to discharge | 1.17 | 0.54–2.52 | 0.700 | ||
| Torso (chest or abdominal) AIS ≥ 3 | 1,007 | ROSC on admission | 2.46 | 1.56–3.88 | <0.001 |
| Survival to discharge | 1.00 | 0.48–2.10 | 1.000 | ||
| Extremity/spine AIS ≥ 3 | 628 | ROSC on admission | 2.73 | 1.37–5.44 | 0.004 |
| Survival to discharge | 1.13 | 0.43–2.92 | 0.810 |
AIS, Abbreviated Injury Scale; CI, confidence interval; OR, odds ratio.
DISCUSSION
Our results showed that the use of prehospital AAM did not improve survival to discharge for EMS‐witnessed traumatic OHCA patients. However, prehospital AAM was positively associated with ROSC for patients with EMS‐witnessed traumatic OHCA. Based on increasing evidence of exceedingly poor outcomes and low survival rates of traumatic OHCA even following CPR, these studies have defined criteria for prehospital withholding or termination of CPR for trauma patients. 14 , 15 Terminating resuscitation should be considered when there are no signs of life on the scene or no response to field resuscitation efforts with minimal interrupted CPR. 16
However, several studies have indicated that nonnegligible traumatic OHCA patients who might not be resuscitated if the proposed guidelines of termination of resuscitation rules are strictly applied, could survive. 4 , 17 Practices could differ depending on geographic region or trauma transport system. Because it would be quite difficult to identify predictors for survival among traumatic OHCA patients following CPR, treatment decisions should not be made on the scene, but rather in the well‐controlled atmosphere of the emergency department.
Our results suggest that AAM for selected trauma OHCA patients seems justifiable. We are aware of several studies showing that prehospital AAM is not beneficial for improving mortality in trauma patients. 2 , 13 , 18 Tsur et al. 19 showed prehospital definitive airway did not benefit the improvement of survival. However, the survival rates in their series were 77.6% for secured airway patients and 78.0% for failed definitive airway patients. Thus, the benefits of AAM for improved prognosis among OHCA patients have been controversial and could depend on the etiologies of traumatic OHCA.
Factors associated with favorable traumatic OHCA outcomes may include injury type (penetrating versus blunt trauma), presence of organized cardiac rhythm on first EMS arrival, short duration of CPR, and short prehospital time. 17 Several studies that undertook subgroup analyses of traumatic OHCA survivors found that traumatic OHCA with hypoxia is associated with relatively good outcomes. 20 , 21 Survivors with AAM in our study could be patients who suffered from hypoxic insult leading to traumatic OHCA.
Although injury severity and region might affect patient mortality, these factors have not been extensively analyzed in previous publications. 3 , 22 Prehospital AAM was reported to improve neurological functions among patients with severe traumatic brain injury, 23 which could indicate potential prehospital AAM benefits among traumatic OHCA in specific conditions. However, we failed to show the benefit of AAM in head trauma‐associated OHCA, because the frequency of head trauma in our study was similar between the AAM (56.3%) and non‐AAM (51.0%) groups.
Our study included levels of trauma severity as variables and eliminated unwitnessed OHCA. A previous study using the Japanese Utstein Registry data bank showed that advanced life support carried out by physicians was associated with a higher chance of 1‐month survival compared to those carried out by EMS. 24 Although this report recorded elapsed time, the information on trauma such as ISS or location of injury were limited. In addition, patients with unwitnessed OHCA were enrolled, which might cause a misunderstanding of the results. Our analysis including traumatic severity as a variable guarantees quality in the study of prehospital AAM use.
Prehospital activity of physicians could affect the prognosis of traumatic OHCA patients. The study addressing prehospital activity reported that ambulances staffed with physicians may improve the survival rate among severe trauma patients. 25 Furthermore, compared to patients transported by EMTs only, those transported by ambulances staffed with physicians are likely to receive not only airway protection, but also further aggressive resuscitation. To eliminate these biased factors, we applied this factor as a variable in the analysis, and PS matching was considered an ideal method to compare the effectiveness of AAM alone.
Japan's unique prehospital delivery system should be taken into account when adapting our results for other countries. The AAM rate among nontraumatic OHCA patients varies widely in Japan, 26 and AAM use depends on a number of factors including transfer time, patient characteristics, EMS personnel skill, and physicians' discretion in charge region‐specific online medical control. 27 Thus, the standard clinical criteria of AAM in Japan is not entirely established and could vary from region to region. Furthermore, treatments allowed for ELST differ in different regions/countries. Effectiveness of prehospital AAM use in different prehospital settings should be further discussed.
LIMITATIONS
Our study has several limitations. First, this is a retrospective study, which might cause information bias. Second, differentiation between ETI and SGA device use in the AAM group was not possible. Third, the time duration between OHCA onset and hospital admission could not be detected in this data. Finally, the etiology/nature of OHCA was not considered, although the causes of OHCA may often be complicated and complex.
CONCLUSIONS
Prehospital AAM among traumatic OHCA patients was not associated with survival to discharge; however, it was associated with improvement of ROSC. This tendency was consistent through all subgroups categorized by body regions of the severe injuries. Emergency care providers should be aware that ROSC was achieved with prehospital AAM in some patient subgroups with traumatic OHCA.
DISCLOSURE
Approval of the research protocol with approval no. and committee name: Approved by the Okayama University Ethics Committee (K2007‐002).
Informed consent: N/A.
Registry and registration no. of the study/trial: N/A.
Animal studies: N/A.
Conflict of interest: None.
ACKNOWLEDGMENT
The authors thank Christine Burr for editing the manuscript.
Funding information
None.
REFERENCES
- 1. Lozano R, Naghavi M, Foreman K et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2095–128. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Stockinger ZT, McSwain NE Jr. Prehospital endotracheal intubation for trauma does not improve survival over bag‐valve‐mask ventilation. J. Trauma 2004; 56: 531–6. [DOI] [PubMed] [Google Scholar]
- 3. Evans CC, Petersen A, Meier EN et al. Prehospital traumatic cardiac arrest: Management and outcomes from the resuscitation outcomes consortium epistry‐trauma and PROPHET registries. J. Trauma Acute Care Surg. 2016; 81: 285–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Willis CD, Cameron PA, Bernard SA, Fitzgerald M. Cardiopulmonary resuscitation after traumatic cardiac arrest is not always futile. Injury 2006; 37: 448–54. [DOI] [PubMed] [Google Scholar]
- 5. Shimazu S, Shatney CH. Outcomes of trauma patients with no vital signs on hospital admission. J. Trauma 1983; 23: 213–6. [DOI] [PubMed] [Google Scholar]
- 6. Lott C, Truhlar A, Alfonzo A et al. European Resuscitation Council Guidelines 2021: cardiac arrest in special circumstances. Resuscitation 2021; 161: 152–219. [DOI] [PubMed] [Google Scholar]
- 7. Committee on Trauma, American College of Surgeons . Advanced Trauma Life Support Student Course Manual. Chicago, IL: American College of Surgeons, 2018. [Google Scholar]
- 8. Nishimura T, Nojima T, Naito H, Ishihara S, Nakayama S, Nakao A. Prehospital emergency life‐saving technicians promote the survival of trauma patients: a retrospective cohort study. Am. J. Emerg. Med. 2022; 56: 218–22. [DOI] [PubMed] [Google Scholar]
- 9. Paul RR, Donald BR. The central role of the propensity score in observational studies for causal effects. Biometrika 1983; 70: 41–55. [Google Scholar]
- 10. Nishimura T, Guyette FX, Naito H, Nakao A, Brown JB, Callaway CW. Comparison of direct oral anticoagulant and vitamin K antagonists on outcomes among elderly and nonelderly trauma patients. J. Trauma Acute Care Surg. 2020; 89: 514–22. [DOI] [PubMed] [Google Scholar]
- 11. Austin PC. Optimal caliper widths for propensity‐score matching when estimating differences in means and differences in proportions in observational studies. Pharm. Stat. 2011; 10: 150–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Luo Z, Gardiner JC, Bradley CJ. Applying propensity score methods in medical research: pitfalls and prospects. Med. Care Res. Rev. 2010; 67: 528–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Ariss AB, Bachir R, El Sayed M. Factors associated with survival in adult patients with traumatic arrest: a retrospective cohort study from US trauma centers. BMC Emerg. Med. 2021; 21: 77. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Eckstein M. Termination of resuscitative efforts: medical futility for the trauma patient. Curr. Opin. Crit. Care 2001; 7: 450–4. [DOI] [PubMed] [Google Scholar]
- 15. Pepe PE, Swor RA, Ornato JP et al. Resuscitation in the out‐of‐hospital setting: medical futility criteria for on‐scene pronouncement of death. Prehosp. Emerg. Care 2001; 5: 79–87. [DOI] [PubMed] [Google Scholar]
- 16. Hopson LR, Hirsh E, Delgado J et al. Guidelines for withholding or termination of resuscitation in prehospital traumatic cardiopulmonary arrest. J. Am. Coll. Surg. 2003; 196: 475–81. [DOI] [PubMed] [Google Scholar]
- 17. Pickens JJ, Copass MK, Bulger EM. Trauma patients receiving CPR: predictors of survival. J. Trauma 2005; 58: 951–8. [DOI] [PubMed] [Google Scholar]
- 18. Hasegawa K, Hiraide A, Chang Y, Brown DF. Association of prehospital advanced airway management with neurologic outcome and survival in patients with out‐of‐hospital cardiac arrest. JAMA 2013; 309: 257–66. [DOI] [PubMed] [Google Scholar]
- 19. Tsur AM, Nadler R, Tsur N et al. Prehospital definitive airway is not associated with improved survival in trauma patients. J. Trauma Acute Care Surg. 2020; 89 (2S Suppl 2): S237–41. [DOI] [PubMed] [Google Scholar]
- 20. Lockey D, Crewdson K, Davies G. Traumatic cardiac arrest: who are the survivors? Ann. Emerg. Med. 2006; 48: 240–4. [DOI] [PubMed] [Google Scholar]
- 21. Di Bartolomeo S, Sanson G, Nardi G, Michelutto V, Scian F. HEMS vs. Ground‐BLS care in traumatic cardiac arrest. Prehosp. Emerg. Care 2005; 9: 79–84. [DOI] [PubMed] [Google Scholar]
- 22. Cera SM, Mostafa G, Sing RF, Sarafin JL, Matthews BD, Heniford BT. Physiologic predictors of survival in post‐traumatic arrest. Am. Surg. 2003; 69: 140–4. [PubMed] [Google Scholar]
- 23. Bernard SA, Nguyen V, Cameron P et al. Prehospital rapid sequence intubation improves functional outcome for patients with severe traumatic brain injury: a randomized controlled trial. Ann. Surg. 2010; 252: 959–65. [DOI] [PubMed] [Google Scholar]
- 24. Fukuda T, Ohashi‐Fukuda N, Kondo Y, Hayashida K, Kukita I. Association of prehospital advanced life support by physician with survival after out‐of‐hospital cardiac arrest with blunt trauma following traffic collisions: japanese registry‐based study. JAMA Surg. 2018; 153: e180674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Hirano Y, Abe T, Tanaka H. Efficacy of the presence of an emergency physician in prehospital major trauma care: a nationwide cohort study in Japan. Am. J. Emerg. Med. 2019; 37: 1605–10. [DOI] [PubMed] [Google Scholar]
- 26. Hasegawa K, Tsugawa Y, Camargo CA Jr, Hiraide A, Brown DF. Regional variability in survival outcomes of out‐of‐hospital cardiac arrest: the All‐Japan Utstein Registry. Resuscitation 2013; 84: 1099–107. [DOI] [PubMed] [Google Scholar]
- 27. Hongo T, Yumoto T, Naito H, Mikane T, Nakao A. Impact of different medical direction policies on prehospital advanced airway management for out‐of hospital cardiac arrest patients: a retrospective cohort study. Resusc Plus. 2022; 9: 100210. [DOI] [PMC free article] [PubMed] [Google Scholar]