

Abstract
Evidence on the efficacy of women's empowerment to improve child growth and minimum dietary diversity (MDD) in the Eastern Africa (EA) region is limited. This cross‐sectional study used recent Demographic and Health Survey data of mother–child dyads from seven countries in EA to examine the associations between women's empowerment measures, child growth and MDD. Length‐for‐age z‐scores, weight‐for‐length z‐scores and weight‐for‐age z‐scores were used to categorize growth indicators of 6–23 months old children. Multivariable logistic regression was used to identify significant associations. Among all countries, 32%–59% of children experienced growth failure. Children meeting MDD were 18%–45%. Women having self‐esteem were associated with lower odds of stunting (adjusted odds ratio [AOR] = 0.62 in Rwanda), wasting (AOR = 0.38 in Uganda), underweight (AORs = 0.60 and 0.57 in Tanzania and Uganda, respectively) and growth failure (AOR = 0.64 in Rwanda). Having health decision control in Burundi was associated with lower odds of stunting (AOR = 0.49) and child growth failure (AOR = 0.52) and higher odds of meeting MDD (AOR = 2.50). Having Legal empowerment among women increased the odds of stunting (AOR = 1.79 in Burundi), underweight (AOR = 1.77 in Uganda) and growth failure (AOR = 1.87 in Burundi). Economic empowerment showed mixed associations with child growth and MDD among some countries. Women's self‐esteem and health decision control were associated with better child growth and MDD for some countries in EA. Nutrition‐sensitive interventions aimed at improving child growth and MDD should consider local contexts when addressing women's empowerment.
Keywords: child dietary diversity, child growth, Eastern Africa, Women's empowerment
Key messages
Understanding the associations between women's empowerment, child growth and child dietary diversity is important for most nutrition‐sensitive interventions seeking to improve child feeding practices and growth by targeting mothers.
In this study, for women to have self‐esteem and health decision control was consistently beneficial for child growth and minimum dietary diversity (MDD). Mixed associations existed among other women's empowerment measures, child growth and MDD across the seven East African countries investigated.
For improved child growth and better child dietary diversity, targeting specific women's empowerment measures based on local context may be beneficial in the East African region.
1. INTRODUCTION
Globally, children are suffering from undernutrition, overnutrition and micronutrient deficiency, as countries face the triple burden of malnutrition (R. E. Black et al., 2013; UNICEF, 2019). Despite a decline in child stunting and wasting (De Onis et al., 2019), undernutrition rates remain high among children. In 2020, over 149.2 million children under 5 years were estimated to be stunted while another 45.4 million experienced wasting (Russell, 2021; World Health Organization, UNICEF, 2021). Further, in Eastern Africa (EA), stunting among children under 5 years remains unacceptably high at 32.6%, and even though child wasting was low (5.2%) as a region compared to southern Asia (14.1%), 3.5 million EA children were estimated to be wasted in 2020 (World Health Organization, UNICEF, 2021). Child mortality and morbidity rates due to malnutrition remain highly associated with disparities in dietary intake and feeding patterns (Perez‐Escamilla et al., 2018). In 2021, the UNICEF reported that about a quarter (24%) of the infants and children (6–23 months of age) in Eastern and Southern Africa had inadequate nutrition quality assessed by failure to consume the minimum five food groups of the recommended eight (World Health Organization, UNICEF, 2021).
Notwithstanding these nutrition challenges, nutrition‐specific interventions such as the promotion of infant and young child feeding (IYCF) practices have shown positive outcomes in reducing child mortality; however, financial support for widespread scale‐up of effective nutrition programmes is limited (Bhutta et al., 2013). Further, due to the complexity of the causes contributing to malnutrition, other sectoral strategies including those that directly and indirectly address immediate determinants of undernutrition such as livelihoods programmes, WASH, women's empowerment and education may be required in interventions to improve child nutrition (Bhutta et al., 2020; Chipili et al., 2020; Kadiyala et al., 2014; Luby et al., 2018; H. J. L. Malapit et al., 2015; Null et al., 2018; Russell, 2021).
The World Health Organization (WHO) defines women's empowerment as an ‘increase in political, social and economic status which enables equal access to resources and guarantees women the right to make strategic decisions over their lives’ (World Health Organization [WHO], 2008). Women's empowerment refers to women's freedom and ability to determine life choices as well as generate and control resources (Alsop et al., 2004; Lee‐Rife, 2010; United Nations Population Fund [UNFPA], 2014). Previous studies in Ethiopia (Fafchamps et al., 2009), India (Kadiyala et al., 2014) and Nepal (Cunningham et al., 2015; H. J. L. Malapit et al., 2015) highlighted positive associations between women's empowerment and improved child feeding practices and child nutrition. Additionally, women's health and socioeconomic status at the household level positively influenced their children's growth (Bhagowalia et al., 2012). Therefore, interventions focusing on women's empowerment may support efforts toward improving nutrition at the household level that could reduce the intergenerational cycle of undernutrition (Smith et al., 2013). Agriculture is one of the main socioeconomic activities that influence household nutrition among countries in EA (Issala, 2013). In 2017, the Food and Agricultural Organization (FAO) reported more than half (53.5%) of East African women depended on agriculture as a source of food (United Nations Food and Agriculture Organization [FAO], 2017). However, women engage in various livelihoods including farming, horticulture, selling in the market, and small and large scale businesses which provide a backbone of household earnings and food security for their families (Issala, 2013; Timalsina & Singh, 2020). Nonetheless, gender‐based inequity still exists (Azmanova, 2016; Hallward‐Driemeier et al., 2013; Huyer, 2016) due to factors such as unequal access to education, employment, health services and financial control.
Recent gender‐based studies among African and Asian countries have reported that women's access and control over resources improved child health and growth (Assan, 2013; Bhagowalia et al., 2015; Jones et al., 2019; H. J. L. Malapit et al., 2015; Pratley, 2016; Quisumbing & Smith, 2012). In Ethiopia, intrahousehold welfare was positively associated with female bargaining power, an economic empowerment measure and improved child nutritional status (Fafchamps et al., 2009). In Bangladesh, women's empowerment attributes such as mobility freedom, decision‐making power and self‐esteem (measured by the attitude toward abuse) were associated with higher length‐for‐age z‐scores and better child dietary diversity (minimum dietary diversity [MDD]) (Bhagowalia et al., 2015). Further, in rural India, a women's empowerment‐centred intervention showed that women's ability to make household decisions was positively associated with reduced child wasting and underweight; similarly, in Zambia (Kumar et al., 2018) and Ghana (H. J. L. Malapit & Quisumbing, 2015), nutrition‐sensitive interventions targeting women's empowerment improved child growth. However, women's freedom of mobility was associated with increased child wasting (M. R. Shroff et al., 2011).
Not all measures of women's empowerment are associated with benefits for young children in different contexts. In Kenya, women's autonomy in controlling resources at the household and the societal level was not significantly associated with wasting in children (0–35 months), although there were significant associations for older children (3–10 years) (Brunson et al., 2009). In that study, the variation in child wasting was attributed to severe resource constraints preventing women to influence child feeding practices. Furthermore, a recent cross‐sectional study in Benin (Alaofè et al., 2017) reported negative associations between women's economic autonomy and child dietary diversity. These two studies (Alaofè et al., 2017; Brunson et al., 2009) contradict results from a qualitative study in Ghana where economically empowered mothers were more likely to provide a variety of foods to malnourished children than well‐nourished children (Davis et al., 2003). Overall, socioeconomic, cultural and population differences among regions may create disparities in associations between women's empowerment measures and child nutrition (Alaofè et al., 2017).
Inconsistencies among studies indicate the need for further investigation of women's empowerment measures and their associations with child dietary diversity and child growth using nationally representative data. Therefore, the purpose of this study was to examine the associations between women's empowerment measures and child nutrition based on seven national surveys from EA. The results may inform future nutrition‐focused programmes implemented through women's empowerment as another sectoral strategy (Bhutta et al., 2020) targeting the improvement of child growth and dietary diversity in EA.
2. MATERIALS AND METHODS
The associations between women's empowerment measures and child growth and MDD in the EA region were analyzed using Demographic and Health Survey (DHS) data of Burundi 2016–2017, Ethiopia 2016, Kenya 2014, Malawi 2015–2016, Rwanda 2014–2015, Tanzania 2015–2016 and Uganda 2016. Nationally representative data for each country on child feeding practices and child health were acquired through weighted‐stratified, cluster probability sampling described elsewhere (Macro International, 2018).
2.1. Inclusion criteria
All countries conventionally and politically defined in the East African region with recent DHS data sets were included in the study.
Dyads of children (6–23 months) and mothers (15–49 years) who answered either yes or no to feeding their child solid/semisolid foods in the past 24 h were included (Figure 1).
Figure 1.
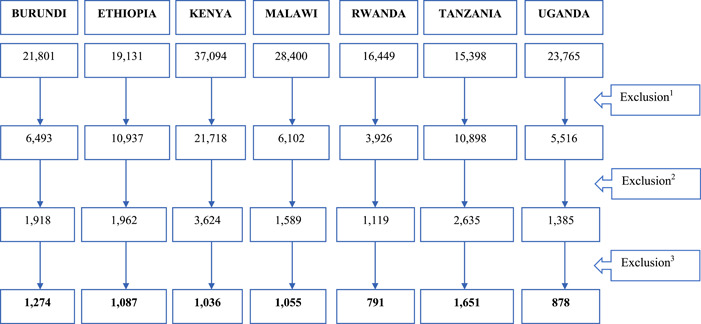
Inclusion of participants in the study sample for each country. 1. Excluded case ID missing variables, maternal variables missing and children above 24 months from the data set. 2. Child, mother and household variables were combined. 3. Data sets of children less than 6 months, missing anthropometric measurements and missing information on provision of solid, semisolid foods to children excluded.
2.2. Exclusion criteria
Data of mother–child dyads with missing case identification numbers or child anthropometric measures were excluded.
2.3. Women's empowerment measures
Using questions available from the DHS, principal component analysis (PCA) was performed (Anin et al., 2020) to determine the weight of each item as a measure of women's empowerment in each country (detailed data in Supporting Information: Table S6). The Kaiser–Meyer–Olkin was used to test sampling adequacy at a cut‐off of >0.60 for the internal consistency of the items to be included in the scale. Bartlett's test of sphericity was statistically significant indicating both sufficient sample size and that those items were significantly correlated among the variables in the data sets (Supporting Information: Table S7). A multiple factor retention method was used to retain measures to assess women's empowerment. Additionally, we considered items with eigenvalues >1, visually examined the scree plot, and further conducted parallel analyses to ascertain the factors to be retained. After the parallel analyses, five measures were retained based on comparison of the initial eigenvalues against the mean scores of the random data eigenvalues in the parallel analysis output. The initial PCA was followed by the Promax rotation for the five measures that provided the optimum value in obtaining the simplest structure. Items with factor loadings less than 0.3 were suppressed (Field, 2013). The selected items had communality scores that ranged from 0.31 to 0.91 for each measure (Supporting Information: Table S6).
DHS items were selected to form each variable representing different women's empowerment measure as shown in Table 1. Economic empowerment was measured by two items that indicated participation in income generation, decision autonomy was indicated by five items on control or participation in household decisions, self‐esteem was measured by four items that focused on the women's perception and experience of intimate physical violence or abuse, health decision empowerment was shown by three items on medical access decisions, and legal empowerment was determined by four items on ownership of property. Women's empowerment measures were developed consistent with previous literature (Allendorf, 2007; Bhagowalia et al., 2015; Golub, 2010; Hallward‐Driemeier et al., 2013). Subsequently, binary scores were formed. For decision autonomy, self‐esteem and health decision control, only women that had affirmative responses for all items received a score of ‘1’, else a code of ‘0’ was assigned. For legal and economic empowerment, women who achieved any one of the DHS items (Golub, 2010; Hallward‐Driemeier et al., 2013) were coded as ‘1’, else a code ‘0’ was assigned.
Table 1.
Definition of variables
| Empowerment measure | Variables representing empowerment | DHS Items considered for variable |
| Economic empowermenta | Participates in income generation |
Type of earnings from work, Employed all year or seasonally |
| Decision autonomyb | Controls/participates in decisions |
Involved in decisions on husband's earnings Spends their own earnings Decides own health care Decides on visiting family Decided on large household purchases |
| Self‐esteemb | Mothers' perception and experience of intimate physical violence or abuse |
Beating justified if goes out without telling husband Beating justified if argues with husband Beating justified if refuses to have sex with husband Beating justified if food gets burnt |
| Health decision controlb | Medical access decision control |
Can go to a health facility Gets funds needed for treatment Decides who accompanies them to the health facility |
| Legal empowermenta | Ownership of property |
Owned a house alone or jointly Owned land alone or jointly Owned land usable for agriculture Owned livestock |
| Child minimum dietary diversity scores (MDD) | Food groups used in calculating the score (≥5 of 8 food groups was optimum) | Currently breastfeeding; Roots and tubers; grains; flesh foods (meat, fish, poultry and organ meats); legumes and nuts; dairy products; vitamin A‐rich fruits and vegetables; eggs; other fruits and vegetables (UNICEF, WHO & World Bank Group, 2021) |
| Child growth | Length‐for‐age z‐scores (LAZ) |
Stunting (less than −2 z‐scores) underweight (less than ‐2 z‐scores) to reflect that it covers all the indicators in the child growth assessment |
| Weight‐for‐length z‐scores (WLZ) |
Wasting (less than −2 z‐scores) |
|
| Weight‐for‐age z‐scores (WAZ) |
Underweight (less than −2 z‐scores) |
|
| Composite Index of Anthropometric Failure | Growth failure | Child who is wasted, stunted or underweight. Included children with a height and weight less than −2 z‐scores and had any other anthropometric failure (Nandy & Svedberg, 2012). |
One item required for a score of ‘1’, else score was ‘0’.
All items required for a score of ‘1’, else score was ‘0’.
2.4. Conceptual framework
A conceptual framework (Figure 2) for possible pathways linking women's empowerment, child dietary diversity and child growth was adapted from previous frameworks (M. M. Black et al., 2020; Herforth & Harris, 2014; Petesch et al., 2005). Women's empowerment is mediated by physical factors such as economic empowerment and legal empowerment, then environmental factors such as self‐esteem and developmental factors including decision autonomy and health decision control. These three mediating factors influence childcare and household interactions, as well as the dietary diversity and health status of the child, culminating in child growth and survival (Bhutta et al., 2020). The women's empowerment measures as described in Table 1 were similar to the majority of domains also used by other investigators to describe women's empowerment (Charmes & Wieringa, 2003; Kishor, 2000; Kritz et al., 1997; Malhotra & Schuler, 2005).
Figure 2.
A conceptual framework on the associations among women's empowerment, child growth and minimum dietary diversity. Source: M. M. Black et al. (2020); Herforth and Harris (2014); Petesch et al. (2005).
2.5. Child MDD
The dependent variables were child MDD and child growth. Children met MDD if they were given a minimum of five food groups (≥5 food groups out of 8) (Table 1) in the past 24 h as recommended by WHO (UNICEF, WHO & World Bank Group, 2021). Individual MDD scores were used to form binary variables; ‘0’ represented suboptimal practices while ‘1’ represented consuming at least five food groups.
2.6. Child growth indicators
Child growth was defined using the WHO growth standards (De Onis et al., 2006) (Table 1). Child stunting, wasting and underweight were defined by lower than −2 z‐scores for length‐for‐age, weight‐for‐length and weight‐for‐age, respectively. Further, child growth failure was assessed using the composite index of anthropometric failure (CIAF) (Nandy & Svedberg, 2012). CIAF was coded as 1 if the child displayed any or a combination of growth failure indicators by WHO standards and as 0 if the child was neither wasted, stunted, underweight alone or in any combination (De Onis et al., 2006; Nandy & Svedberg, 2012).
2.7. Statistical analysis
Weighted descriptive statistics including percentages or sample means for parental, household and child characteristics, and for women's empowerment measures we calculated by country. Bivariate logistic regression analyses of each empowerment measure were determined for MDD and child growth by each country. Associations reaching p < 0.10 were included in the adjusted models. Multivariable analyses were adjusted for strata, cluster and for covariates including child's sex, age, had diarrhoea, maternal age, height, education, literacy, exposure to media, number of living children, household head, wealth index and paternal–maternal age difference (Bhutta et al., 2020; World Health Organization [WHO], 2020). Variance inflation factor and tolerance test were acceptable (below 10 and 0.2, respectively). Variables that maintained a p ≤ 0.05 in the multivariable analyses were considered significant. Data analyses were performed using SAS, v. 9.4 (SAS Institute Inc.).
3. RESULTS
3.1. Descriptive characteristics
Parental, household and child characteristics are summarized by country in Tables 2 and 3, while the prevalence of women's empowerment measures is summarized in Table 4. Ethiopia had the highest proportion (63.6%) of women with no formal education compared with women among other analyzed countries in EA, which varied between 8.9% and 44.7%. Similarly, Ethiopian women had the highest illiteracy levels (75.2%) compared with other countries (17.3% and 37.4%). The proportion of mothers engaged in working outside of the home in all countries was more than half (57.4% and 87.8%) except in Ethiopia where only 24.7% of mothers worked outside the home. Body mass index (BMI) of less than 18.5 kg/m2 was reported for <17.5% of mothers in all countries except Ethiopia where 26.2% were classified as underweight.
Table 2.
Selected parental and household characteristics among seven countries in Eastern Africa
| BURUNDI | ETHIOPIA | KENYA | MALAWI | RWANDA | TANZANIA | UGANDA | |
|---|---|---|---|---|---|---|---|
| % (n = 1274) | % (n = 1087) | % (n = 1036) | % (n = 1055) | % (n = 791) | % (n = 1651) | % (n = 878) | |
| Maternal variables | |||||||
| Education level | |||||||
| No education | 44.7 | 63.6 | 11.3 | 11.0 | 115 | 20.1 | 8.9 |
| Literacy | |||||||
| Cannot read at all | 37.4 | 75.2 | 17.3 | 31.3 | 18.9 | 29.9 | 31.9 |
| Maternal working status | |||||||
| Working | 87.8 | 24.7 | 57.4 | 67.4 | 83.8 | 76.9 | 76.4 |
| Maternal BMI | |||||||
| Normal | 75.7 | 68.4 | 59.8 | 80.0 | 72.1 | 70.7 | 68.2 |
| Underweight | 17.5 | 26.2 | 9.3 | 6.1 | 5.4 | 9.2 | 9.8 |
| Overweight and obese | 6.8 | 5.4 | 30.8 | 13.9 | 22.5 | 20.1 | 22.0 |
| Marital status | |||||||
| Married/living together | 90.5 | 93.6 | 83.2 | 84.8 | 82.4 | 82.6 | 84.7 |
| Household variables | |||||||
| HH head sex | |||||||
| Female | 19.3 | 14.4 | 28.2 | 27.5 | 21.0 | 17.6 | 24.9 |
| Wealth Index | |||||||
| Poor | 45.3 | 46.1 | 38.0 | 49.3 | 48.7 | 74.5 | 49.1 |
| Middle | 20.7 | 22.8 | 15.9 | 19.7 | 17.9 | 18.6 | 20.3 |
| Rich | 34.0 | 31.1 | 46.0 | 31.0 | 33.3 | 33.9 | 40.6 |
| Place of residence | |||||||
| Rural | 91.9 | 88.6 | 56.0 | 87.7 | 83.8 | 74.8 | 75.9 |
| Paternal variables | |||||||
| Partner's education | |||||||
| No education | 34.9 | 44.2 | 6.9 | 9.7 | 15.3 | 13.2 | 7.1 |
Table 3.
Child growth, composite index of anthropometric failure, child dietary diversity scores of seven countries in Eastern Africa
| BURUNDI | ETHIOPIA | KENYA | MALAWI | RWANDA | TANZANIA | UGANDA | |
|---|---|---|---|---|---|---|---|
| % (n = 1274) | % (n = 1087) | % (n = 1036) | % (n = 1055) | % (n = 791) | % (n = 1651) | % (n = 878) | |
| Child variables | |||||||
| Sex of Child | |||||||
| Female | 49.9 | 52.3 | 52.2 | 49.3 | 51.6 | 52.3 | 50.3 |
| Age (months) (mean± SD) | 12.7 ± 4.9 | 12.3 ± 4.7 | 12.5 ± 4.9 | 13.0 ± 4.8 | 13.0 ± 5.0 | 12.6 ± 4.8 | 13.2 ± 5.2 |
| WHO child growth indicators | |||||||
| Stunted | 55.5 | 38.8 | 27.5 | 35.8 | 36.1 | 37.7 | 32.6 |
| Wasted | 10.1 | 13.1 | 4.8 | 3.1 | 3.7 | 6.1 | 5.9 |
| Underweight | 33.5 | 25.0 | 10.4 | 10.0 | 11.4 | 16.7 | 13.0 |
| Composite index of anthropometric failure (CIAF) | |||||||
| Growth failure | 59.8 | 49.0 | 32.4 | 38.1 | 40.1 | 42.1 | 37.2 |
| Wasting only | 0.5 | 4.5 | 1.7 | 1.2 | 1.1 | 1.2 | 1.5 |
| Wasting and underweight | 2.4 | 3.8 | 2.1 | 0.4 | 1.7 | 1.7 | 2.0 |
| Wasting, stunting and underweight | 7.2 | 5.4 | 0.9 | 1.5 | 1.0 | 3.2 | 2.4 |
| Stunting and underweight | 22.9 | 14.8 | 6.9 | 7.9 | 7.9 | 10.8 | 7.7 |
| Stunting only | 25.5 | 19.1 | 19.8 | 26.8 | 27.5 | 23.8 | 22.7 |
| Underweight only | 1.3 | 1.6 | 0.9 | 0.4 | 1.0 | 1.3 | 0.9 |
| Child dietary diversity score | |||||||
| Minimum ≥5 of 8 food groups | |||||||
| Met | 31.2 | 18.2 | 45.2 | 27.7 | 33.1 | 31.1 | 34.0 |
| Did not meet | 68.8 | 81.8 | 54.8 | 72.3 | 66.9 | 68.9 | 66.0 |
Abbreviation: SD, standard deviation.
Table 4.
Prevalence of women's empowerment measures among seven countries in Eastern Africa
| BURUNDI | ETHIOPIA | KENYA | MALAWI | RWANDA | TANZANIA | UGANDA | |
|---|---|---|---|---|---|---|---|
| % (n = 1274) | % (n = 1087) | % (n = 1036) | % (n = 1055) | % (n = 791) | % (n = 1651) | % (n = 878) | |
| Women Empowerment variables | |||||||
| Economic empowerment | |||||||
| Participates in income generation | 83.2 | 37.1 | 60.5 | 67.1 | 68.2 | 78.0 | 75.2 |
| Decision autonomy | |||||||
| Controls/participates in decisions | 63.0 | 73.2 | 51.8 | 53.0 | 64.9 | 41.7 | 51.6 |
| Self‐esteem | |||||||
| Free from physical abuse | 46.9 | 34.8 | 61.9 | 75.6 | 64.1 | 41.5 | 57.9 |
| Health decision control | |||||||
| Health service access | 83.4 | 61.0 | 94.0 | 85.2 | 88.1 | 78.0 | 86.5 |
| Legal empowerment | |||||||
| Owned property | 52.8 | 40.5 | 25.4 | 25.6 | 29.7 | 26.1 | 21.6 |
The proportion of married women and those living together with their spouses ranged from 82.4% to 93.6%. Additionally, Kenya, Malawi and Uganda had a quarter or more (24.9%–28.2%) female‐headed households while other countries had lower proportions of female‐headed households ranging from 14.4% to 19.3%. Fewer than half (≤49.3%) of the households in all countries were classified as poor except in Tanzania (74.5%). Most of the sampled households in all countries were in rural areas with a range from 56.0% to 91.9%. Nearly 85% of the husbands/partners in all countries had attained some level of formal education except for Burundi (34.9%) and Ethiopia (44.2%).
3.2. Child characteristics, growth and growth failure
The proportion of female to male children was about half ranging from 49.3% to 52.3% in all countries, and the child mean age ranged from 12.3 ± 4.7 to 13.2 ± 5.2 in all countries (Table 3). The prevalence of stunting was highest in Burundi (55.5%) with other countries between 27.5% and 38.8%. Wasting among Kenyan, Rwandese and Malawian children was lowest (3.1% to 4.8%), while wasting was highest in Ethiopia at 13.1%. Burundian and Ethiopian children had a high prevalence of underweight (33.5% and 25.0%, respectively) while other countries ranged between 10.0% and 16.7%. Burundian (59.8%) and Ethiopian (49.0%) children experienced the highest CIAF. All other countries had CIAF ranging from 32.4% to 42.1%.
3.3. Child dietary diversity scores
In all countries, 18.2%–45.2% of infants and young children consumed five and more food groups. The lowest prevalence of children that met MDD was in Ethiopia (18.2%) while Kenya had the highest proportion (45.2%) of children that met MDD (Table 3).
3.4. Women's empowerment measures
The empowerment domains used in this study were economic, decision autonomy, self‐esteem, health decision control and legal empowerment. The economic empowerment measure was indicated by either of the two items on household income generation shown in Table 1. Our results in Table 4 show that the proportion of women who were economically empowered was lowest in Ethiopia (37.1%). More than three‐quarters (75.2%–83.2%) of the women in Uganda, Tanzania and Burundi were economically empowered. Tanzania had the lowest proportion (41.7%) of women with decision autonomy; however, in other countries more than half (51.6%–73.2%) of the women had the autonomy to make or participate in household decisions.
Women's self‐esteem was measured through women's perceptions of freedom from intimate physical violence. In Malawi, more than three‐quarters (75.6%) of mothers reported self‐esteem while fewer women had self‐esteem in Ethiopia (34.8%), Tanzania (41.5%) and Burundi (46.9%). In almost all countries included in this study, over three‐quarters (78.0%–94.0%) of the women had control over decisions regarding their health; Ethiopia had the least proportion of women with health decision control in comparison to other countries in this study, yet, they were still represented by more than half (61.0%) of the sample. Women's proportion with legal empowerment was higher in Burundi and Ethiopia (52.8% and 40.5%, respectively) than in other countries where women with legal empowerment ranged from 21.6% to 29.7%.
3.5. Women's empowerment and child growth
In all countries except Ethiopia, at least one women's empowerment measure was significantly associated with child growth after controlling for cofounders but not all of these were associated with benefits to the child. Women's empowerment measures were associated with child stunting in Burundi, Kenya and Rwanda (Table 5). Women who were economically empowered in Burundi were more likely to have stunted children (adjusted odds ratio [AOR] = 1.78; 95% confidence interval [CI]: 1.03, 3.06; p = 0.039), while, children of economically empowered Kenyan women were less likely to be stunted (AOR = 0.59, 95% CI: 0.35, 0.99, p = 0.049). Rwandese children of women with self‐esteem were less likely to be stunted (AOR = 0.62, 95% CI: 0.40, 0.94, p = 0.026). Similarly, Burundian women with health decision control had children less likely to be stunted (AOR = 0.49, 95% CI: 0.28, 0.86, p = 0.014), even though, women with legal empowerment in Burundi were more likely to have stunted children (AOR = 1.79, 95% CI: 1.22, 2.61, p = 0.003).
Table 5.
Significant associations between women's empowerment and child growth among seven countries in Eastern Africa
| Women empowerment measures | Child growth indicatorsa | |||
|---|---|---|---|---|
| Unadjusted odds ratios | Adjusted odds ratios | |||
| OR | 95% CI | AOR | 95% CI | |
| Economic empowerment | ||||
| Stunting | ||||
| Burundi | 1.34 | 0.98–1.84 | 1.78 | 1.03–3.06* |
| Kenya | 0.64 | 0.43–0.96* | 0.59 | 0.35–0.99* |
| Wasting | ||||
| Kenya | 0.52 | 0.26–1.05 | 0.30 | 0.11–0.82* |
| Underweight | ||||
| Burundi | 1.40 | 0.98–1.97 | 1.87 | 1.01–3.45* |
| Malawi | 1.68 | 0.96–2.95 | 2.53 | 1.23–5.18* |
| Growth failureb | ||||
| Burundi | 1.32 | 0.98–1.79 | 1.84 | 1.08–3.13* |
| Kenya | 0.62 | 0.43–0.89** | 0.50 | 0.31–0.82** |
| Self‐esteem | ||||
| Stunting | ||||
| Rwanda | 0.73 | 0.54–0.98* | 0.62 | 0.40–0.94* |
| Wasting | ||||
| Uganda | 0.51 | 0.27–0.95* | 0.38 | 0.16–0.93* |
| Underweight | ||||
| Tanzania | 0.65 | 0.46–0.92* | 0.60 | 0.38–0.93* |
| Uganda | 0.51 | 0.33–0.79** | 0.57 | 0.33–0.98* |
| Growth failureb | ||||
| Rwanda | 0.70 | 0.53–0.94* | 0.64 | 0.43–0.96* |
| Health decision control | ||||
| Stunting | ||||
| Burundi | 0.82 | 0.59–1.13 | 0.49 | 0.28–0.86* |
| Growth failureb | ||||
| Burundi | 0.80 | 0.57–1.13 | 0.52 | 0.30–0.95* |
| Legal empowerment | ||||
| Stunting | ||||
| Burundi | 1.59 | 1.25–2.02*** | 1.79 | 1.22–2.61** |
| Underweight | ||||
| Uganda | 1.93 | 1.20–3.10** | 1.77 | 1.01–3.12* |
| Growth failureb | ||||
| Burundi | 1.63 | 1.27–2.08*** | 1.87 | 1.28–2.75*** |
Note: Results from logistic regression controlled for child sex, age, recent diarrhoea; maternal age, height (for stunting & CIAF), highest education level, literacy level, listened to the radio recently; household number of living children, sex of head, wealth index, and mother and father age difference. Reference group for women's empowerment measure coded ‘0’.
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Coded 1 for stunted, wasted, underweight and CIAF; Coded 0 for adequate growth (>−2 z‐scores).
Composite index of anthropometric failure (CIAF).
p ≤ 0.05;
p ≤ 0.01;
p ≤ 0.001.
Specific women's empowerment measures were associated with child wasting in only Kenya and Uganda. Economically empowered Kenyan women were less likely to have children who were wasted (AOR = 0.30, 95% CI: 0.11, 0.82, p = 0.019). Similarly, Uganda women with self‐esteem had children less likely to be wasted (AOR = 0.38, 95% CI: 0.16, 0.93, p = 0.033).
None of the women's empowerment measures were associated with child underweight in Ethiopia, Kenya and Rwanda. Women who were economically empowered in Burundi and Malawi were more likely to have children who were underweight (AOR = 1.87, 95% CI: 1.01, 3.45, p = 0.046 and AOR = 2.53, 95% CI: 1.23, 5.18, p = 0.012, respectively). Tanzanian and Ugandan women with self‐esteem empowerment were less likely to have underweight children (AOR = 0.60, 95% CI: 0.38, 0.93, p = 0.024 and AOR = 0.57, 95% CI: 0.33, 0.98, p = 0.041, respectively). Differently, Ugandan women with legal empowerment were more likely to have underweight children (AOR = 1.77, 95% CI: 1.01, 3.12, p = 0.047). The detailed information by country on associations between women's empowerment measures and child growth are included as Supporting Information: Tables S1–S3.
3.6. Women's empowerment measures and child growth failure
Significant associations between women's empowerment measures and the CIAF are presented in Table 5. Specific women's empowerment measures were associated with CIAF in only Burundi, Kenya and Rwanda. Women who were economically empowered in Burundi were more likely to have children with CIAF (AOR = 1.84, 95% CI: 1.08, 3.13, p = 0.026). However, in Kenya economically empowered women were less likely to have children with CIAF (AOR = 0.50, 95% CI: 0.31, 0.82, p = 0.006). Similarly, Rwandese women with self‐esteem and Burundian women with health decision control were less likely to have children experiencing CIAF (AOR = 0.64, 95% CI: 0.43, 0.96, p = 0.030) and (AOR = 0.52, 95% CI: 0.30, 0.95, p = 0.032), respectively. In contrast, children of women who had legal empowerment in Burundi had a higher likelihood of CIAF (AOR = 1.87, 95% CI: 1.28, 2.75, p = 0.001). The detailed information by country on associations between women's empowerment measures and child growth failure are included as Supporting Information: Table S4.
3.7. Women's empowerment measures and child dietary diversity
Significant associations between women's empowerment measures and child MDD were shown in Burundi, Ethiopia and Rwanda (Table 6). Women with economic empowerment were more likely to have children who met the MDD in Ethiopia (AOR = 3.02, 95% CI: 1.34, 6.78, p = 0.008). Differently, children of women who had economic empowerment in Burundi were less likely to have met MDD (AOR = 0.47, 95% CI: 0.26, 0.83, p = 0.010).
Table 6.
Significant associations between women's empowerment measures and child minimum dietary diversity among seven countries in Eastern Africa
| Women empowerment measures | Child minimum dietary diversity (MDD)a | |||
|---|---|---|---|---|
| Unadjusted odds ratios | Adjusted odds ratios | |||
| OR | 95% CI | AOR | 95% CI | |
| Economic empowerment | ||||
| Burundi | 0.92 | 0.63–1.35 | 0.47 | 0.26–0.83** |
| Ethiopia | 1.89 | 1.13–3.15* | 3.02 | 1.34–6.78** |
| Decision autonomy | ||||
| Burundi | 1.59 | 1.20–2.10*** | 1.55 | 1.00–2.41* |
| Rwanda | 0.99 | 0.73–1.34 | 0.60 | 0.37–0.97* |
| Health decision control | ||||
| Burundi | 1.27 | 0.87–1.85 | 2.50 | 1.35–4.63** |
| Legal Empowerment | ||||
| Ethiopia | 0.86 | 0.49–1.53 | 0.30 | 0.11–0.86* |
Note: Results from logistic regression controlled for child sex, age, recent diarrhoea; maternal age, highest education level, literacy level, listened to the radio recently; household number of living children, sex of head, wealth index, and mother and father age difference. Reference group for women's empowerment measure coded ‘0’.
Abbreviations: AOR, adjusted odds ratio; CI, confidence interval.
Coded 1 for adequate MDD (≥5 of 8 food groups); Coded 0 for inadequate MDD (<5 of 8 food groups).
p ≤ 0.05;
p ≤ 0.01;
p ≤ 0.001.
Mixed associations with MDD were related to decision autonomy. In Burundi, decision autonomy was positively associated with MDD (AOR = 1.55, 95% CI: 1.00, 2.41, p = 0.049), while decision autonomy was negatively associated with MDD (AOR = 0.60, 95% CI: 0.37, 0.97, p = 0.037) in Rwanda. Health decision control was positively associated with child MDD for Burundian women (AOR = 2.50, 95% CI: 1.35, 4.63, p = 0.004). Differently in Ethiopia, legal empowerment was negatively associated with MDD (AOR = 0.30, 95% CI: 0.11, 0.86, p = 0.025). Detailed information by country on associations between women's empowerment and MDD are included in Supporting Information: Table S5.
4. DISCUSSION
4.1. Women's empowerment measures and child growth
This study showed mixed associations between different women's empowerment measures and child growth. Women with economic empowerment were more likely to have children experiencing stunting (Burundi), underweight (Burundi and Malawi) and CIAF (Burundi). These findings agreed with previous studies in Benin (Alaofè et al., 2017), and Ethiopia, Vietnam and Peru (De Silva & Harpham, 2007) that ascribed the increased likelihood of impaired growth to variations in population and environmental characteristics, and differences in attributes assigned to women's economic empowerment. Also, a study conducted in Kenya (Brunson et al., 2009) reported that women may be categorized as economically empowered, but still the lack of control of resources at household and societal levels reduces their capacity to supplement diets in their households for improved child growth. However, in our study, Kenyan women who were economically empowered had children who were less likely to experience child stunting and CIAF. The current findings were similar to a review of women's empowerment and food insecurity in sub‐Saharan Africa (Assan, 2013) where women's economic empowerment improved food availability for household use and child growth due to increased resources for agriculture and livelihoods.
These mixed findings demonstrate that women's economic empowerment among countries in EA may be influenced by socioeconomic and cultural factors specific to varying geographic locations that may affect child growth between countries. For example, there often are discriminatory laws in low‐income countries that hinder women's right to work and earn an income independent of their husband's permission. Such laws may restrict the use of earnings for personal and household needs as perceived by the woman rather than priorities insisted upon by the husband (Azmanova, 2016; Hallward‐Driemeier et al., 2013; Huyer, 2016). Nevertheless, strategic policies and interventions toward women's control over household resources, similar income generation resources, and behavioural change programmes of equity and equality to men may potentially improve child growth (Bhutta et al., 2020; H. J. L. Malapit et al., 2015). Also, the evaluation of women's economic empowerment may be better addressed with a more comprehensive women's empowerment scale that has more diverse indicators to capture the majority of the economic determinants among women within EA. Assessing economic empowerment in EA may need to include more parameters involving agriculture, small and medium business enterprises, and casual labour. Possibly, the indicators used in our analysis were not sufficient to uniformly capture women's economic empowerment across individual local contexts in all seven countries in EA.
Children of women with self‐esteem were less likely to be stunted or experience CIAF in Rwanda; neither were they wasted in Uganda nor underweight in either Uganda or Tanzania. Women with self‐esteem may be more proactive in making better childcare decisions. They may be more likely to take initiative in providing better nutrition for their children thus improving child growth (Arulampalam et al., 2016; Issala, 2013; Yaya et al., 2020). Further, the present study showed that Burundian women with health decision control had children who were less likely to be stunted or underweight, even though no significant associations were found between health decision control and child growth in other countries. These findings are consistent with studies in some developing countries (Arulampalam et al., 2016; Carlson et al., 2015; Kumar et al., 2018; Pratley, 2016; M. Shroff et al., 2009; M. R. Shroff et al., 2011) showing that health decision‐making had the potential to improve child health and growth. Nonetheless, a study conducted on health‐seeking behaviour in Senegal (Franckel & Lalou, 2009) explained that decisions related to health services access were not individualistic but were rather a process integrating inputs from several persons that support the woman. Therefore, an individual's capacity may not translate to increased health‐seeking behaviour. In the current study, self‐esteem and health decision control were the only women's empowerment measures that consistently showed beneficial associations with child growth for all countries in which they were significant. These findings on self‐esteem and health decision control suggests increased expansion of nutrition‐sensitive programmes (Bhutta et al., 2020) such as increasing women's awareness and assertiveness (Bishop, 2013); policy interventions targeting these distinct measures may result in better growth for children within the selected countries although situational differences need to be considered for higher impact on child growth across the countries included in our study.
In our study, women who were legally empowered were more likely to have children who experienced stunting, and CIAF in Burundi, as well as underweight in Uganda. These findings on women's legal empowerment may be explained by the variability and lack of comprehensiveness in legal empowerment across community settings. If traditional laws restrict women's access and full ownership of assets, ownership of property may not necessarily translate to property control (McKenna et al., 2019; United Nations, 2015). Such marginalizing and disempowering customary practices and laws, mostly in low‐income countries (Hallward‐Driemeier et al., 2013; Huyer, 2016), contribute to reduced self‐esteem, poor maternal care and inadequate childcare affecting the nutritional status of both the mother and child. Furthermore, our study demonstrated that in Ethiopia none of the women's empowerment measures were associated with child growth. Nevertheless, studies in various countries have shown these empowerment measures to be positively associated with child health and growth (Bhagowalia et al., 2012; Fafchamps et al., 2009; Kadiyala et al., 2014; H. J. L. Malapit et al., 2015). A study in Kenya (Brunson et al., 2009) suggested that the variability in women's empowerment measures by setting makes it difficult to associate differences in societal characteristics with child growth.
Overall, our findings showed selective associations for different women's empowerment measures with child growth, and MDD in the seven countries analyzed in EA. Women's empowerment measures used were consistent with indicators in the definition of women's empowerment by the WHO (World Health Organization [WHO], 2008) and as used by previous studies (Alsop et al., 2004; Lee‐Rife, 2010; United Nations Population Fund [UNFPA], 2014). However, there may be a need to build on recently created scales such as the project‐level Women's Empowerment in Agriculture Index (pro‐WEAI) (H. Malapit et al., 2019) to include additional domains that widely assess women's empowerment outside of a specific project setting to contextualize more communal or habitual setting indicators. Also, while some of the variables used were similar to those used in the survey‐based women's empowerment index (SWPER) (Ewerling et al., 2017, 2020), additional variables available from the DHS data for the countries in our study were included.
4.2. Women's empowerment measures and child dietary diversity
Mixed associations between women's empowerment measures and child MDD were found only in Burundi and Ethiopia. Additional significant associations were shown in Rwanda. The other four countries examined did not show significant associations of women's empowerment with child MDD which may be explained by the complexity in cultural variations within local contexts regarding the role of women's empowerment measures on child growth and MDD (Carlson et al., 2015). In our study, children of economically empowered women in Ethiopia were three times more likely to meet MDD. Studies in Ghana (Davis et al., 2003) and Nepal (H. J. L. Malapit et al., 2015) reported that economically empowered women provided more diverse foods to their children which was attributed to increased control of income, reduced gender disparities and higher production diversity in the household. On the contrary, the present study also showed that children of Burundian women who were economically empowered and Rwandese women who had decision autonomy were less likely to meet the MDD. Similarly, legally empowered Ethiopian women were less likely to have children that met MDD. A study on selected sub‐Saharan countries (Na et al., 2015) suggested that even though the majority of the women had an agrarian livelihood with a high production burden, the utility of the food produced for the household was not guaranteed as a result of lack of decision control. This discrepancy may offer some explanation for the variability of associations between women's empowerment domains and MDD. The lack of decision control on food produced from the land may not allow a focus household nutritional insecurity leading to an inability to meet the MDD. Additionally, our study findings showed Burundian women who had health decision control were more likely to have children that met the MDD. These findings were consistent with a study of developing countries using DHS data that reported maternal utilization of health services to be associated with better infant and young child nutrition, as well as reduced infant morbidity and mortality (Ahmed et al., 2010).
Several insights can be gained from the significant associations between women's empowerment measures and child growth and MDD among the specific EA countries. For example, economically empowered women may have the capacity to provide different high‐quality foods in the household thus improving household dietary practices. The reverse associations on the same economic empowerment measure may indicate that it is not enough for women to be only economically empowered. Women may also require additional forms of empowerment such as health decision control and self‐esteem to effectively utilize the economic resources to improve child health and dietary practices. The balance of specific women's empowerment efforts may be promoted or modified through informing country‐specific policies and programmes targeting improving IYCF practices, especially MDD.
Some of the women's empowerment measures in our study were different from other scales used in women's empowerment evaluations (H. J. L. Malapit et al., 2015; H. J. L. Malapit & Quisumbing, 2015; Stern et al., 2016). Our independent measures approach through factor analysis was based on variables available through the DHS and had notable differences from some of the recently developed women's empowerment tools. For example, the pro‐WEAI (H. Malapit et al., 2019) often used to evaluate women's empowerment interventions in agriculture, focuses on three domains. Some variables used in the WEAI, such as membership of women in groups, were not collected in the DHS. Other variables such as work‐time limits and access to credit also were not directly included in the DHS. Such differences between variables limited the use of the pro‐WEAI in our study. Another scale, the summative index used for women's empowerment assessment has been challenged for discounting item‐level distinctions in measuring women's empowerment (Alaofè et al., 2017) and has been shown to have high variability in measuring indicators based on individual associations (Ghuman, 2002) and therefore, was not used in this study. Also, while the SWPER (Ewerling et al., 2017, 2020) is a viable index for women's empowerment assessment, we included additional items available in DHS data sets from the seven countries in EA, precluding the use of the SWPER. These indicators, such as women's earnings from work, decisions on household purchases, and ownership of house or land, formed integral parts of specific domains used in this study and were consistent with evaluations used in previous studies (Alsop et al., 2004; Lee‐Rife, 2010; United Nations Population Fund [UNFPA], 2014) of women's empowerment.
4.3. Study limitations
The cross‐sectional DHS data does not provide the depth of understanding of women's empowerment that might be provided with data collected through qualitative, longitudinal or mixed methods women's empowerment studies (Creswell & Clark, 2017). A qualitative study might help to explain the existing gaps or the reverse association between some of our women's empowerment measures, MDD and child growth. Further, the DHS survey questions may need to be expanded to adequately capture women's specific productive and economic influences on household health and nutrition. Questions addressing women's community leadership and women's rights to access and utilize food as a contributor to household nutrition may be needed in the DHS for future women's empowerment assessments. Questions about access and utilization of credit and financial services may also improve assessment of women's empowerment with DHS data. Also, questions on other forms of abuse to women such as emotional violence, for example, questions targeting how a husband may belittle or devalue his wife could provide important data for assessment of emotional violence, and subsequently the self‐esteem empowerment measure. Although recall or social desirability biases may have affected responses to indicators that inform women's empowerment, strengths of this study included the use of empowerment measures developed by factor analysis from several variables in the DHS data as well as the nationally representative samples from seven countries in EA. Future studies may consider investigating the strength of the women's empowerment measures and their effects on the severity of undernutrition in children across different regions.
5. CONCLUSION
In specific EA countries, women's self‐esteem and health decision control consistently showed beneficial associations with child growth and MDD, compared to the negative associations with legal empowerment, and mixed associations with economic empowerment. The beneficial associations between child growth and health decision control in Burundi and self‐esteem in Rwanda, Uganda and Tanzania may support designing interventions aimed at reducing child undernutrition within those countries. Also, the positive associations between MDD and women's health decision control in Burundi and economic empowerment in Ethiopia have the potential to inform national‐level programmes and policies targeting the dietary quality of children.
These indirect approaches aimed at improving child nutrition through women's empowerment strategies in EA have potential to transform individual behaviour, interpersonal relations, local institutions, the community and public policy in a social‐ecological approach. Further, specific empowerment initiatives using a country‐centred approach to improving child growth and MDD, especially within countries that showed significant positive associations, would prioritize country‐level resources. Such area‐specific planning would leverage meager resources, promote wider‐scale interventions and potentially create sustainable improvements in child health.
AUTHOR CONTRIBUTIONS
The authors responsibilities were as follows: Joel J. Komakech, Christine N. Walters, Hasina Rakotomanana, Deana A. Hildebrand, Barbara J. Stoecker designed the study. Joel J. Komakech and Hasina Rakotomanana conducted statistical analysis. Hasina Rakotomanana, Deana A. Hildebrand, Barbara J. Stoecker advised on data analysis. Joel J. Komakech developed first draft of manuscript. Christine N. Walters, Hasina Rakotomanana, Deana A. Hildebrand, Barbara J. Stoecker critically reviewed and revised manuscript. All authors read and approved the final manuscript.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
ETHICS STATEMENT
Ethical approval for secondary analysis of this deidentified data was obtained from the DHS program. The approval for use of the survey data sets was initially provided on 8/27/2018 and reapproved on 10/22/2021.
Supporting information
Supplementary information.
ACKNOWLEDGEMENTS
The authors thank the DHS Program and ICF Macro for allowing access and use the data. We would like also to thank the Department of Nutritional Sciences in the College of Education & Human Sciences at Oklahoma State University.
Komakech, J. J. , Walters, C. N. , Rakotomanana, H. , Hildebrand, D. A. , & Stoecker, B. J. (2022). The associations between women's empowerment measures, child growth and dietary diversity: Findings from an analysis of demographic and health surveys of seven countries in Eastern Africa. Maternal & Child Nutrition, 18, e13421. 10.1111/mcn.13421
DATA AVAILABILITY STATEMENT
The data used for this study is available at https://dhsprogram.com/Data/. Cleaned data sets can be made available by J. J. K.
REFERENCES
- Ahmed, S. , Creanga, A. A. , Gillespie, D. G. , & Tsui, A. O. (2010). Economic status, education, and empowerment: Implications for maternal health service utilization in developing countries. PLoS One, 5, 11190. 10.1371/journal.pone.0011190 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alaofè, H. , Zhu, M. , Burney, J. , Naylor, R. , & Douglas, T. (2017). Association between women's empowerment and maternal and child nutrition in Kalale District of Northern Benin. Food and Nutrition Bulletin, 38, 302–318. 10.1177/0379572117704318 [DOI] [PubMed] [Google Scholar]
- Allendorf, K. (2007). Do women's land rights promote empowerment and child health in Nepal? World Development, 35(11), 1975–1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Alsop, R. , Heinsohn, N. , & Somma, A. (2004). Measuring empowerment: An analytic framework. Power, Rights, and Poverty: Concepts and Connections, 23, 120. [Google Scholar]
- Anin, S. K. , Saaka, M. , Fischer, F. , & Kraemer, A. (2020). Association between infant and young child feeding (IYCF). Indicators and the nutritional status of children (6–23 months) in Northern Ghana. Nutrients, 12, 2565. 10.3390/nu12092565 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arulampalam, W. , Bhaskar, A. , & Srivastava, N. (2016). Does greater autonomy among women provide the key to better child nutrition? Institute for the Study of Labor (IZA) Discussion Paper, Paper No. 9781. 10.2139/ssrn.2742569 [DOI]
- Assan, N. (2013). Women empowerment as a tool against food insecurity in Sub Saharan Africa. Scientific Journal of Review, 2, 329–339. [Google Scholar]
- Azmanova, A. (2016). Empowerment as surrender: How women lost the battle for emancipation as they won equality and inclusion. Social Research: An International Quarterly, 83, 749–776. [Google Scholar]
- Bhagowalia, P. , Kadiyala, S. , & Headey, D. (2012). Agriculture, income, and nutrition linkages in India: Insights from a nationally representative survey. IFPRI Working Paper, 1195, 1‐ 31. [Google Scholar]
- Bhagowalia, P. , Menon, P. , Quisumbing, A. R. , & Soundararajan, V. (2015). What dimensions of women's empowerment matter most for child nutrition? Evidence using nationally representative data from Bangladesh. International Food Policy Research Institute. [Google Scholar]
- Bhutta, Z. A. , Akseer, N. , Keats, E. C. , Vaivada, T. , Baker, S. , Horton, S. E. , Katz, J. , Menon, P. , Piwoz, E. , Shekar, M. , & Victora, C. (2020). How countries can reduce child stunting at scale: Lessons from exemplar countries. American Journal of Clinical Nutrition, 112, 894–904. 10.1093/ajcn/nqaa153 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhutta, Z. A. , Das, J. K. , Rizvi, A. , Gaffey, M. F. , Walker, N. , Horton, S. , Webb, P. , Lartey, A. , Black, R. E. , & Group, T. L. (2013). Evidence‐based interventions for improvement of maternal and child nutrition: What can be done and at what cost? The Lancet, 382, 452–477. 10.1016/S0140-6736(13)60996-4 [DOI] [PubMed] [Google Scholar]
- Bishop, S. (2013). Develop your assertiveness (pp. 1–20). Kogan Page Publishers. [Google Scholar]
- Black, M. M. , Lutter, C. K. , & Trude, A. C. (2020). All children surviving and thriving: Re‐envisioning UNICEF's conceptual framework of malnutrition. The Lancet Global Health, 8, 766–767. 10.1016/S2214-109X(20)30122-4 [DOI] [PubMed] [Google Scholar]
- Black, R. E. , Victora, C. G. , Walker, S. P. , Bhutta, Z. A. , Christian, P. , De Onis, M. , Ezzati, M. , Grantham‐McGregor, S. , Katz, J. , Martorell, R. , & Uauy, R. (2013). Maternal and child undernutrition and overweight in low‐income and middle‐income countries. The Lancet, 382, 427–451. 10.1016/S0140-6736(13)60937-X [DOI] [PubMed] [Google Scholar]
- Brunson, E. K. , Shell‐Duncan, B. , & Steele, M. (2009). Women's autonomy and its relationship to children's nutrition among the Rendille of northern Kenya. American Journal of Human Biology, 21, 55–64. 10.1002/ajhb.20815 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson, G. J. , Kordas, K. , & Murray‐Kolb, L. E. (2015). Associations between women's autonomy and child nutritional status: A review of the literature. Maternal & Child Nutrition, 11(4), 452–482. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Charmes, J. , & Wieringa, S. (2003). Measuring women's empowerment: An assessment of the gender‐related development index and the gender empowerment measure. Journal of Human Development, 4, 419–435. 10.1080/1464988032000125773 [DOI] [Google Scholar]
- Chipili, G. , Msuya, J. , Pacific, R. , & Majili, S. Z. (2020). Women empowerment and the nutrition status of children aged between 6–59 months. Journal of Nutrition and Health Sciences, 5, 208. [Google Scholar]
- Creswell, J. W. , & Clark, V. L. P. (2017). Designing and conducting mixed methods research (3rd ed.). Sage publications. [Google Scholar]
- Cunningham, K. , Ploubidis, G. B. , Menon, P. , Ruel, M. , Kadiyala, S. , Uauy, R. , & Ferguson, E. (2015). Women's empowerment in agriculture and child nutritional status in rural Nepal. Public Health Nutrition, 18, 3134–3145. 10.1017/S1368980015000683 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davis, P. , Tagoe‐Darko, E. , & Mukuria, A. (2003). Water koko and appetite: Complementary feeding practices in Kumasi Ghana. ORC Macro. [Google Scholar]
- De Silva, M. J. , & Harpham, T. Maternal social capital, and child nutritional status in four developing countries. Health & Place, 13, 341–355. 10.1016/j.healthplace.2006.02.005 [DOI] [PubMed] [Google Scholar]
- De Onis, M. , Borghi, E. , Arimond, M. , Webb, P. , Croft, T. , Saha, K. , De‐Regil, L. M. , Thuita, F. , Heidkamp, R. , Krasevec, J. , & Hayashi, C. (2019). Prevalence thresholds for wasting, overweight and stunting in children under 5 years. Public Health Nutrition, 22, 175–179. 10.1017/S1368980018002434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- De Onis, M. , Onyango, A. W. , Borghi, E. , Garza, C. , Yang, H. , & WHO Multicentre Growth Reference Study Group . (2006). Comparison of the World Health Organization (WHO) child growth standards and the national center for health statistics/WHO international growth reference: Implications for child health programmes. Public Health Nutrition, 9, 942–947. 10.1017/PHN20062005 [DOI] [PubMed] [Google Scholar]
- Ewerling, F. , Lynch, J. W. , Victora, C. G. , van Eerdewijk, A. , Tyszler, M. , & Barros, A. J. D. (2017). The SWPER index for women's empowerment in Africa: Development and validation of an index based on survey data. The Lancet Global Health, 5, 916–923. 10.1016/S2214-109X(17)30292-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ewerling, F. , Raj, A. , Victora, C. G. , Hellwig, F. , Coll, C. V. N. , & Barros, A. J. D. (2020). SWPER Global: A survey‐based women's empowerment index expanded from Africa to all low‐ and middle‐income countries. Journal of Global Health, 10, 020343. 10.7189/jogh.10.020434 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fafchamps, M. , Kebede, B. , & Quisumbing, A. R. (2009). Intrahousehold welfare in rural Ethiopia. Oxford Bulletin of Economics and Statistics, 71, 567–599. 10.1111/j.1468-0084.2009.00553.x [DOI] [Google Scholar]
- Field, A. (2013). Discovering statistics using IBM SPSS statistics (4th ed.). SAGE. [Google Scholar]
- Franckel, A. , & Lalou, R. (2009). Health‐seeking behaviour for childhood malaria: Household dynamics in rural Senegal. Journal of Biosocial Science, 41, 1–19. 10.1017/S0021932008002885 [DOI] [PubMed] [Google Scholar]
- Ghuman, S. J. (2002). Women's autonomy and child survival in five Asian countries [PhD dissertation]. University of Pennsylvania, Population Studies Center.
- Golub, S. (2010). What is legal empowerment? An introduction. In McInerney T., & Golub S. (Eds.), Legal empowerment: Practitioners' perspectives (Vol. 2, pp. 9 ‐17). International Development Law Organization. [Google Scholar]
- Hallward‐Driemeier, M. , Hasan, T. , & Rusu, A. B. (2013). Women's legal rights over 50 years: Progress, stagnation or regression? World Bank Policy Research Working Paper , 6616. 10.1596/1813-9450-6616 [DOI]
- Herforth, A. , & Harris, J. (2014). Understanding and applying primary pathways and principles. Brief #1 Improving Nutrition through Agriculture Technical Brief Series USAID—SPRING Project: Arlington.
- Huyer, S. (2016). Closing the gender gap in agriculture (pp. 105–116). SAGE. 10.1177/0971852416643872 [DOI] [Google Scholar]
- Issala, B. (2013). Agriculture in Africa: Transformation and outlook. NEPAD. Retrieved from https://www.nepad.org/caadp/publication/agriculture-africa-transformation-and-outlook
- Jones, R. , Haardörfer, R. , Ramakrishnan, U. , Yount, K. M. , Miedema, S. , & Girard, A. W. (2019). Women's empowerment and child nutrition: The role of intrinsic agency. SSM Popul. Health, 9, 100475. 10.1016/j.ssmph.2019.100475 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kadiyala, S. , Harris, J. , Headey, D. , Yosef, S. , & Gillespie, S. (2014). Agriculture and nutrition in India: Mapping evidence to pathways. Annals of the New York Academy of Sciences, 1331, 43–56. 10.1111/nyas.12477 [DOI] [PubMed] [Google Scholar]
- Kishor, S. (2000). Empowerment of women in Egypt and links to the survival and health of their infants. In Presser H., & Sen G. (Eds.), Women's empowerment and demographic processes: Moving beyond Cairo (pp. 119‐156). Oxford University Press. [Google Scholar]
- Kritz, M. M. , Makinwa‐Adebusoye, P. , & Gurak, D. T. (1997). Wife's empowerment and fertility in Nigeria: The role of context. Paper presented at the female empowerment and demographic processes: Moving beyond Cairo, Lund, Sweden.
- Kumar, N. , Nguyen, P. H. , Harris, J. , Harvey, D. , Rawat, R. , & Ruel, M. T. (2018). What it takes: Evidence from a nutrition‐ and gender‐sensitive agriculture intervention in rural Zambia. Journal of Development Effectiveness, 10(3), 341–372. 10.1080/19439342.2018.1478874 [DOI] [Google Scholar]
- Lee‐Rife, S. M. (2010). Women's empowerment and reproductive experiences over the lifecourse. Social Science and Medicine, 71, 634–642. 10.1016/j.socscimed.2010.04.019 [DOI] [PubMed] [Google Scholar]
- Luby, S. P. , Rahman, M. , Arnold, B. F. , Unicomb, L. , Ashraf, S. , Winch, P. J. , Stewart, C. P. , Begum, F. , Hussain, F. , Benjamin‐Chung, J. , & Leontsini, E. (2018). Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Bangladesh: A cluster randomised controlled trial. The Lancet Global Health, 6, 302–315. 10.1016/S2214-109X(17)30490-4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Macro International . (2018). Demographic and Health Surveys (DHS). Retrieved from https://dhsprogram.com/
- Malapit, H. , Quisumbing, A. , Meinzen‐Dick, R. , Seymour, G. , Martinez, E. M. , Heckert, J. , Rubin, D. , Vaz, A. , Yount, K. M. , Phase, G. A. , & Team, S. (2019). Development of the project‐level Women's Empowerment in Agriculture Index (pro‐WEAI). World Development, 122, 675–692. 10.1016/j.worlddev.2019.06.018 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Malapit, H. J. L. , Kadiyala, S. , Quisumbing, A. R. , Cunningham, K. , & Tyagi, P. (2015). Women's empowerment mitigates the negative effects of low production diversity on maternal and child nutrition in Nepal. The Journal of Development Studies, 51, 1097–1123. 10.1080/00220388.2015.1018904 [DOI] [Google Scholar]
- Malapit, H. J. L. , & Quisumbing, A. R. (2015). What dimensions of women's empowerment in agriculture matter for nutrition in Ghana? Food Policy, 52, 54–63. 10.1016/j.foodpol.2015.02.003 [DOI] [Google Scholar]
- Malhotra, A. , & Schuler, S. R. (2005). Women's empowerment as a variable in international development. Measuring Empowerment: Cross‐disciplinary Perspectives, 1, 71–88. [Google Scholar]
- McKenna, C. G. , Bartels, S. A. , Pablo, L. A. , & Walker, M. (2019). Women's decision‐making power and undernutrition in their children under age five in the Democratic Republic of the Congo: A cross‐sectional study. PLoS One, 14, 0226041. 10.1371/journal.pone.0226041 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Na, M. , Jennings, L. , Talegawkar, S. A. , & Ahmed, S. (2015). Association between women's empowerment and infant and child feeding practices in sub‐Saharan Africa: An analysis of Demographic and Health Surveys. Public Health Nutrition, 18, 3155–3165. 10.1017/S1368980015002621 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nandy, S. , & Svedberg, P. (2012). The Composite Index of Anthropometric Failure (CIAF): An alternative indicator for malnutrition in young children. In Handbook of anthropometry (pp. 127–137). Springer. 10.1007/978-1-4419-1788-1_6 [DOI] [Google Scholar]
- Null, C. , Stewart, C. P. , Pickering, A. J. , Dentz, H. N. , Arnold, B. F. , Arnold, C. D. , Benjamin‐Chung, J. , Clasen, T. , Dewey, K. G. , Fernald, L. C. , & Hubbard, A. E. (2018). Effects of water quality, sanitation, handwashing, and nutritional interventions on diarrhoea and child growth in rural Kenya: A cluster‐randomised controlled trial. The Lancet Global Health, 6, 316–329. 10.1016/S2214-109X(18)30005-6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perez‐Escamilla, R. , Bermudez, O. , Buccini, G. S. , Kumanyika, S. , Lutter, C. K. , Monsivais, P. , & Victora, C. (2018). Nutrition disparities and the global burden of malnutrition. BMJ, 361, k2252. 10.1136/bmj.k2252 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Petesch, P. , Smulovitz, C. , & Walton, M. (2005). Evaluating empowerment: A framework with cases from Latin America. In Narayan‐Parker D. (Ed.), Measuring empowerment: Cross‐disciplinary perspectives (pp. 39–67). World Bank. [Google Scholar]
- Pratley, P. (2016). Associations between quantitative measures of women's empowerment and access to care and health status for mothers and their children: A systematic review of evidence from the developing world. Social Science and Medicine, 169, 119–131. 10.1016/j.socscimed.2016.08.001 [DOI] [PubMed] [Google Scholar]
- Quisumbing, A. R. , & Smith, L. C. (2012). Intrahousehold allocation, gender relations, and food security in developing countries. In Pinstrup‐Andersen P., & Cheng F. (Eds.), Food policy for developing countries: Case studies (pp. 4–5). Cornell University. [Google Scholar]
- Russell, S. A. (2021). Within our grasp: Childhood malnutrition worldwide and the revolution taking place to end it (1st ed., pp. 4–6). Pantheon. [Google Scholar]
- Shroff, M. , Griffiths, P. , Adair, L. , Suchindran, C. , & Bentley, M. (2009). Maternal autonomy is inversely related to child stunting in Andhra Pradesh, India. Maternal & Child Nutrition, 5, 64–74. 10.1111/j.1740-8709.2008.00161.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shroff, M. R. , Griffiths, P. L. , Suchindran, C. , Nagalla, B. , Vazir, S. , & Bentley, M. E. (2011). Does maternal autonomy influence feeding practices and infant growth in rural India. Social Science and Medicine, 73, 447–455. 10.1016/j.socscimed.2011.05.040 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Smith, L. C. , Khan, F. , Frankenberger, T. R. , & Wadud, A. A. (2013). Admissible evidence in the court of development evaluation? The impact of CARE's SHOUHARDO project on child stunting in Bangladesh. World Development, 41, 196–216. 10.1016/j.worlddev.2012.06.018 [DOI] [Google Scholar]
- Stern, M. , Jones‐Renaud, L. , & Hillesland, M. (2016). Intervention guide for the Women's Empowerment in Agriculture Index (WEAI): Practitioner's guide to selecting and designing WEAI interventions. United States Agency for International Development.
- Timalsina, Y. , & Singh, S. (2020). Impact of rural development initiatives on women empowerment and sustainable livelihood—“A Case of Machhapucchre Village, Kaski”. 8th IOE Graduate Conference, Tribhuvan University.
- UNICEF . (2019). “The State of The World's Children 2019.” Children, food and nutrition: Growing well in a changing world (pp. 9–20). United Nations Children's Fund. [Google Scholar]
- UNICEF, WHO, & World Bank Group . (2021). Levels and trends in child malnutrition: Key findings of the 2021 edition of the joint child malnutrition estimates. United Nations Children's Fund, World Health Organization, and International Bank for Reconstruction and Development/The World Bank (W. H. O. United Nations Children's Fund, World Bank Group, Ed.). WHO press. Retrieved March 2022 from. https://www.who.int/publications/i/item/9789240025257
- United Nations . (2015). Department of Economic Social Affairs, Statistics Division. The world's women 2015. Trends and statistics. United Nations Publications. Retrieved from https://www.un.org/development/desa/publications/the-worlds-women-2015.html
- United Nations Food and Agriculture Organization [FAO] . (2017). The future of food and agriculture–Trends and challenges. Annual Report (p. 296). FAO Rome. [Google Scholar]
- United Nations Population Fund [UNFPA] . (2014). Gender equality, equity and empowerment of women. United Nations Population Information Network (pp. 28–36). United Nations Inter‐Agency Task Force on the Implementation of the ICPD Program of Action. 10.18356/6eaaf944-en [DOI] [Google Scholar]
- World Health Organization, UNICEF . (2021). Indicators for assessing infant and young child feeding practices: Definitions and measurement methods.
- World Health Organization [WHO] . (2008). Women's empowerment and gender equality: Essential goals for saving women's lives. Retrieved from http://wwwwhoint/gender/documents/EN_womens_emppdf
- World Health Organization [WHO] . (2020). UNICEF/WHO/The World Bank Group Joint Child Malnutrition Estimates: Levels and trends in child malnutrition: Key findings of the 2020 edition. Retrieved from https://apps.who.int/iris/bitstream/handle/10665/331621/9789240003576-eng.pdf
- Yaya, S. , Odusina, E. K. , Uthman, O. A. , & Bishwajit, G. (2020). What does women's empowerment have to do with malnutrition in Sub‐Saharan Africa? Evidence from Demographic and Health Surveys from 30 countries. Global Health Research and Policy, 5, 1–11. 10.1186/s41256-019-0129-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplementary information.
Data Availability Statement
The data used for this study is available at https://dhsprogram.com/Data/. Cleaned data sets can be made available by J. J. K.