

Abstract
Purpose
This study provides a comprehensive analysis of research trends on the etiology, mechanisms, potential risk factors, diagnosis, prognosis, surgical and non-surgical treatment of varicocele, and clinical outcomes before and after varicocele repair.
Materials and Methods
Varicocele studies published between 1988 and 2020 were retrieved from the Scopus database on April 5, 2021. Original studies on human varicocele were included, irrespective of language. Retrieved articles were manually screened for inclusion in various sub-categories. Bibliometric data was subjected to scientometric analysis using descriptive statistics. Network, heat and geographic mapping were generated using relevant software.
Results
In total, 1,943 original human studies on varicocele were published. These were predominantly from the northern hemisphere and developed countries, and published in journals from the United States and Germany. Network map analysis for countries showed several interconnected nodal points, with the USA being the largest, and Agarwal A. from Cleveland Clinic, USA, being a center point of worldwide varicocele research collaborations. Studies of adolescents were underrepresented compared with studies of adults. Studies on diagnostic and prognostic aspects of varicocele were more numerous than studies on varicocele prevalence, mechanistic studies and studies focusing on etiological and risk factors. Varicocele surgery was more investigated than non-surgical approaches. To evaluate the impact of varicocele and its treatment, researchers mainly analyzed basic semen parameters, although markers of seminal oxidative stress are being increasingly investigated in the last decade, while reproductive outcomes such as live birth rate were under-reported in the literature.
Conclusions
This study analyzes the publication trends in original research on human varicocele spanning over the last three decades. Our analysis emphasizes areas for further exploration to better understand varicocele’s impact on men’s health and male fertility.
Keywords: Analysis, bibliometric; Clinical research; Infertility, male; Publications; Varicocele; Varicocele repair
INTRODUCTION
Varicocele is defined as an abnormal enlargement and tortuosity of veins in the pampiniform plexus [1]. One in 7 adolescents over 15 years of age is reported to have a varicocele [2]. While this prevalence is the same as that observed in the general population (approximately 15%), it is higher in infertile men [3,4,5]. In fact, varicocele is considered as a frequent cause of correctable infertility in males [6] as it affects up to 35% to 44% of men with primary infertility [1,3] and 45% to 80% of men with secondary infertility [7,8].
Varicoceles can have a negative impact on spermatogenesis through multiple pathways, thus resulting in a progressive decline in male fertility. The abnormalities of semen quality in infertile men with varicocele are variable ranging from oligozoospermia to complete azoospermia [9]. It is now accepted that oxidative stress (OS) is a central and common pathogenic mediator of testicular damage in varicocele, and that the exposure to scrotal heat, hypoxia, and toxic adrenal and renal metabolites enhances the generation of reactive oxygen species (ROS) [10]. Potential genetic predisposition factors and a decreased ability to fight against the effects of seminal OS have also been described to explain clinical variations of varicocele impact on sperm parameters and fertility [11,12,13,14,15,16,17,18]. Although seminal ROS in physiological amounts are essential for sperm capacitation, acrosome reaction, hyperactivation, and fertilization, increased ROS may lead to OS and result in lipid peroxidation, protein oxidation and DNA damage [19].
During the last few decades, basic research on the pathophysiological mechanisms involved in varicocele has made it possible to answer certain clinical questions, but still some grey areas remain. For example, while the prevalence of varicocele is higher in infertile men, particularly in men with secondary infertility [1,3,7,8], it has been shown that some men can have a clinical (palpable) varicocele without affecting their sperm parameters or fertility [1,6]. It has been estimated that up to 45% of all males with clinical varicocele have normal semen parameters [1], and approximately 80% of men with varicocele are fertile [20]. Thus, despite advances in the understanding of the mechanisms involved in the pathophysiology of varicocele, it remains difficult to predict clinically which varicocele will be associated with an impairment of sperm parameters and fertility.
Regarding treatment, some questions also remain unanswered. If, according to the guidelines of the American Urological Association (AUA)/American Society for Reproductive Medicine (ASRM) and European Association of Urology (EAU) [21,22], infertility with altered sperm parameters is an indication for varicocele repair, it is difficult to predict which patient will have an improvement in sperm parameters compared to another. Similarly, it is still difficult to predict spontaneous fertility and reproductive outcomes after varicocele repair. This requires longitudinal cohort studies taking into account the grade and laterality of varicocele and the female partner’s fertility status. Randomized controlled studies on varicocele are challenging to carry out due to difficulties encountered in selecting the control arm. On the other hand, animal models are not representative of human physiology because, in animals, varicocele is artificially induced and the exposure to the varicocele is limited in duration compared to that seen in humans [16]. These reasons may explain why some questions remain unresolved and why the gap between basic research and clinical applications is not always bridged.
Scientometrics is a quantitative analysis of written scientific publications through the analysis of bibliometric data (such as authors, institutions, countries, and journals in which studies are published in specific scientific fields). It permits the investigation of developments within a specific field of research as indicated by the thematic pattern of its publications [23]. The generation of network mapping based on publication distribution and keywords is also useful in understanding the dynamics of the field of interest [24]. There are a few scientometric studies that have been conducted with regard to male infertility. These studies have mainly examined the impact of sperm DNA fragmentation (SDF) [25] and OS [26] in male infertility, the role of antioxidants in improving semen parameters [27], the contribution of assisted reproductive technologies (ART) in addressing infertility [28], and the employment of innovative tools such as proteomics in managing male infertility [29].
However, to date, there is no study available evaluating the scientific trends in the context of varicocele. Hence, the aim of this study is to perform a comprehensive analysis of publication trends in human varicocele research. This analysis will detail i) demographics of studies (countries, institutions, journals, and authors), ii) most recurrent keywords used in scientific publications on varicocele, and iii) topics of publications. The topics present in publications in the last 33 years are classified according to the following criteria: i) varicocele in adolescents and adults; ii) prevalence, pathophysiology, etiology, and risk factors of varicocele; iii) diagnosis and prognosis of varicocele; iv) methods of varicocele treatment (surgical/non-surgical interventions); and v) impact of varicocele and varicocele treatment on reproductive outcomes. Analyzing published articles from a scientometric perspective could reveal the current trends and intensity in research interest on specific areas in human varicocele, which in turn would sketch the wider landscape of male infertility.
MATERIALS AND METHODS
1. Ethics statement
This scientometric study was performed by analyzing data retrieved from the Scopus database (https://www.elsevier.com/solutions/scopus) and therefore an approval by the Ethics Committee was not necessary.
2. Data source
Scopus is a bibliographic database containing abstracts and citations for academic journal articles. It covers approximately 21,000 titles from over 5,000 publishers, including 20,000 scientific, technical, medical, and social journals. An advantage of using the Scopus database is the ability to automatically analyze the literature search and generate graphs and tables based on bibliometric metrics (e.g. number of documents by year, author, affiliation, journal, country, type of document, subject area).
3. Data retrieval strategy
Data was collected on April 5, 2021 and included scientific articles from 1988 to 2020 (33 years). Articles published in 2021 were excluded by using the Scopus filter. The keyword “varicoc*” was searched as an entry term in ‘TITLE-ABSTRACT-KEYWORDS’ fields to retrieve all relevant publications. Additional keywords (“man” OR “men” OR “adolescent*” OR “patient*” OR “human”) were used to exclusively limit the search to human studies. The query AND NOT TITLE (“review*” OR “meta-analysis”) AND (LIMIT-TO (DOCTYPE, “ar”)) was used to retrieve only original studies. We used the asterisk ‘*’ after the word to include all variants of the term. All retrieved publications were saved as comma-separated value (CSV) files and subsequently converted to Microsoft Excel files. The extracted studies were manually screened to exclude non-relevant articles. Only original studies on humans were included, while reviews, meta-analyses, and other types of publications (case-reports, editorials, etc.) were excluded by using Scopus filters and manual screening.
Afterward, the collected articles were manually validated by independent researchers for inclusion in different subcategories: varicocele in adolescents or adults, prevalence, pathophysiology, etiology and risk factors, prognostic/diagnostic studies, surgical and non-surgical interventions, impact of varicocele or treatment on semen parameters, seminal OS, sperm DNA damage and/or SDF, testicular histology, testicular inflammation and cytokines, hormones, vasculature and blood flow, reproductive outcomes (pregnancy rate, PR; live birth rate, LBR) in natural conception or ART (Fig. 1). As each article can be included in more than one subgroup, data is reported as the number of publications and percentage out of the total number of publications identified. Data retrieved were analyzed based on the year of publication, journal, author, affiliation, and country of origin.
Fig. 1. Flow diagram representing the scientometric analysis framework of original human studies on varicocele. TESE: testicular sperm extraction, SDF: sperm DNA fragmentation, ICSI: intracytoplasmic sperm injection, LBR: live birth rate, PR: pregnancy rate, IUI: intrauterine insemination, IVF: in vitro fertilization.

4. Network, heat, and geomap analysis
Network and heat maps were generated by using the VOSviewer software (freely available at https://vosviewer.com) [30]. The relatedness of each node was calculated by using co-authorship as criteria, while their size reflected the number of publications. Geographic mapping was created by using the Tableau Public software (freely available at https://public.tableau.com/en-us/s/).
RESULTS
From 1988 to 2020, 1,943 original human studies on varicocele were identified when the Scopus database was used as a search tool. The publication trend in original human studies on varicocele during these years is shown in Fig. 2.
Fig. 2. Trend of publications in original human studies on varicocele from 1988 to 2020 (Scopus database). In parenthesis, guidelines published on the topic of varicocele [35,36,37,38,39,40,62,71].

1. Demographics of publications (countries, institutions, journals & authors)
Italy (n=285), the United States (n=255), and Turkey (n=214) have published the most on varicocele compared to other countries (Fig. 3). These three countries are also the ones that have shown to be most connected with other countries in their research on varicocele (Fig. 4). The top 10 institutions and journals with the largest number of articles are reported in Table 1, 2a and 2b, respectively. The top 10 institutions publishing original human studies on varicocele are more distributed throughout the continents (Table 1). They include North America (3 institutions in USA and 2 in Canada), Europe (3 different institutions in Italy), and other institutions in the continents of Asia (Iran, Israel, Taiwan), Africa (Egypt) and South America (Brazil).
Fig. 3. Geographic map illustrating the origin of publications in scientific research on varicocele in original human studies.

Fig. 4. Network map illustrating international research collaborations between countries in original human studies on varicocele.

Table 1. Top 10 institutions publishing original human studies on the topic of varicocele.
| Ranking | Top 10 institutions | Number of publications |
|---|---|---|
| 1 | Cairo University, Egypt | 75 |
| 2 | Sapienza Università di Roma, Italy | 36 |
| 3 | Cleveland Clinic Foundation, USA | 30 |
| 4 | New York Presbyterian Hospital, USA | 25 |
| 5 | Royan Institute, Iran | 22 |
| 6 | University of Toronto, Canada | 21 |
| 7 | Università degli Studi di Verona, Italy | 18 |
| 8 | Mount Sinai Hospital of University of Toronto, Canada | 17 |
| 9 | Università degli Studi di Siena, Italy | 16 |
| National Yang-Ming University, Taiwan | ||
| 10 | Tel Aviv University, Israel | 15 |
| Weill Cornell Medicine, USA | ||
| Universidade de São Paulo, Brazil | ||
| Rabin Medical Center, Israel |
Table 2a. Top 10 journals publishing original human studies on the topic of varicocele.
| Ranking | Top 10 journals | Country of origin | Journal impact factor (2021) | SJR quartile (overall) | SJR quartileb (subject-based) | Number of publications |
|---|---|---|---|---|---|---|
| 1 | Journal of Urology | US | 7.450 | Q1 | Q1 | 132 |
| 2 | Andrologia | Germany | 2.775 | Q3 | Q2 | 126 |
| 3 | Urology | US | 2.649 | Q3 | Q2 | 124 |
| 4 | Fertility and Sterility | US | 7.329 | Q1 | Q1 | 82 |
| 5 | Zhonghua Nan Ke Xue (National Journal of Andrology) | China | NA | NA | Q4 | 46 |
| 6 | BJU International a | England | 5.588 | Q1 | Q1 | 36 |
| 7 | British Journal of Urology a | England | - | - | - | 33 |
| 8 | International Urology and Nephrology | Netherlands | 2.370 | Q3 | Q2 | 31 |
| 9 | Urologia Internationalis | Switzerland | 2.089 | Q3 | Q2 | 30 |
| 10 | European Urology | Netherlands | 20.096 | Q1 | Q1 | 28 |
aBJU International was formerly known as the British Journal of Urology (1929–1999).
bAll subject-based SJR quartiles are based on the subject of Urology, except for Fertility and Sterility (Reproductive Medicine) and Zhonghua Nan Ke Xue National Journal of Andrology (Medicine [miscellaneous]).
SJR: Scimago Journal Ranking (based on Scopus data as of April 2021), NA: not available.
Table 2b. Top 10 journals publishing original human studies on the topic of varicocele.
| Ranking | Top 10 journals | Semen parameters | Oxidative stress | Sperm DNA fragmentation | Prediction of clinical outcomes | Postoperative recurrence | Biochemical markers | Indication of surgical or medical treatment in varicocele diagnosis | Number of publications |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Journal of Urology | 62 (47.0) | 6 (4.5) | 3 (2.3) | 70 (53.0) | 37 (28.0) | 12 (9.1) | 46 (34.8) | 132 |
| 2 | Andrologia | 84 (66.7) | 24 (19.0) | 11 (8.7) | 44 (34.9) | 9 (7.1) | 37 (29.4) | 18 (14.3) | 126 |
| 3 | Urology | 61 (49.2) | 4 (3.2) | 2 (1.6) | 60 (48.4) | 17 (13.7) | 8 (6.5) | 37 (29.8) | 124 |
| 4 | Fertility and Sterility | 57 (69.5) | 8 (9.8) | 8 (9.8) | 27 (32.9) | 5 (6.1) | 11 (13.4) | 24 (29.3) | 82 |
| 5 | Zhonghua Nan Ke Xue National Journal of Andrology | 30 (65.2) | 2 (4.3) | 5 (10.9) | 24 (52.2) | 8 (17.4) | 3 (6.5) | 15 (32.6) | 46 |
| 6 | BJU International a | 15 (41.7) | 4 (11.1) | 3 (8.3) | 13 (36.1) | 7 (19.4) | 3 (8.3) | 6 (16.7) | 36 |
| 7 | British Journal of Urologya | 23 (69.7) | 0 (0.0) | 1 (3.0) | 21 (63.6) | 11 (33.3) | 2 (6.1) | 22 (66.7) | 33 |
| 8 | International Urology and Nephrology | 11 (35.5) | 1 (3.2) | 2 (6.5) | 14 (45.2) | 6 (19.4) | 8 (25.8) | 11 (35.5) | 31 |
| 9 | Urologia Internationalis | 14 (46.7) | 0 (0.0) | 0 (0.0) | 11 (36.7) | 6 (20.0) | 3 (10.0) | 9 (30.0) | 30 |
| 10 | European Urology | 13 (46.4) | 0 (0.0) | 0 (0.0) | 11 (39.3) | 8 (28.6) | 3 (10.7) | 7 (25.0) | 28 |
Values are presented as number of publications (%).
aBJU International was formerly known as the British Journal of Urology (1929–1999).
Comparatively, out of the top 10 journals, 6 originate from the continent of Europe (2 each from the Netherlands and England, and 1 each from Germany and Switzerland), 3 are from North America, while only 1 is from Asia (China) (Table 2a). Most of the top 10 journals listed in Table 2a are either in the first (Q1) or second (Q2) quartile rankings for Urology based on the Scimago Journal Ranking (SJR) [31]. Those categorized as Q1 include European Urology (#1), Journal of Urology (#3), British Journal of Urology (BJU) International (#7), whereas those in Q2 comprise Urology (#28), Urologia Internationalis (#33), Andrologia (#46), and International Urology and Nephrology (#48). Fertility and Sterility is a Q1 journal of the SJR subject category for Reproductive Medicine [32] (#4), while Zhonghua Nan Ke Xue (National Journal of Andrology) is a Q4 journal in Medicine (miscellaneous) [33].
The top 10 authors with the highest number of publications in topics related to human studies on varicocele were Mostafa T. (n=29), Agarwal A. (n=25), Goldstein M. (n=24), Zini A. (n=24), Fujisawa M. (n=20), Glassberg K.I. (n=18), Shiraishi K. (n=16), Jarvi K. (n=15), Zampieri N. (n=15), and Tavalaee M. (n=14). Network analysis showed Agarwal A. as the author contributing the most on varicocele research through collaboration with multiple different research teams (Fig. 5).
Fig. 5. Network map illustrating international research collaborations between authors in original human studies on varicocele.

2. Keywords analysis
A network analysis was conducted to identify the most recurrent keywords present in the title of publications. Based on the node sizes, 6 out of 65 words were found to be the most frequently used in the original studies on human varicocele: in order of frequency, these include “laparoscopic varicocelectomy”, “technique”, “experience”, “child”, “varicocele repair”, “adolescent varicocele”, and “improvement” (Fig. 6). This word analysis has limitations because sometimes synonymous keywords decrease the frequency of occurrence of a particular keyword. Hence, based on word associations (associated words belong to the same cluster and are of the same color), it appears that the two most frequently used keyword domains are adolescence (in red, Fig. 6a) and infertility (in green, Fig. 6a). Based on the period of publication, two broad periods were defined (Fig. 6b): 1988–2008 (blue, green, Fig. 6b) and 2008–2020 (light green-yellow, Fig. 6b). Keywords related to adolescence, as well as keywords for laparoscopic surgical techniques appear as older words (used before 2008). Words such as “oxidative stress”, “infertile”, “efficacy”, “expression”, “association”, “body mass index” or those concerning “subinguinal microsurgical techniques” were used in studies published in recent years.
Fig. 6. Network map reporting the terms which are most commonly reported in the title of original scientific literature on varicocele. Colors represent (A) the organization of words in clusters based on their recurrence, and (B) the date of publication.

3. Varicocele publications in adolescents and adults
Published reports on varicocele in adolescents included 355 (n=18.3%) articles, with the highest yearly trend of publications in 2013 (n=21). All remaining manuscripts (n=1,588; 81.7%) focused on adults.
4. Prevalence, pathophysiology, etiology, and risk factors
There were 32 studies on varicocele prevalence (1.6%). In mechanistic studies (n=552), 377 (68.3%) articles investigated varicocele pathophysiology, 246 (44.6%) spermatogenesis/spermiogenesis, and 106 (19.2%) molecular interactions (Table 3). A total of 222 (11.4%) articles investigated the etiology and risk factors of varicocele. The yearly publication trend was highest in 2014 with 20 published articles.
Table 3. Publications investigating non-surgical and surgical approaches for varicocele treatment, mechanistic studies, and prognostic/diagnostic studies.
| Topic of publications | Value | ||
|---|---|---|---|
| Mechanistic studies (n=552) | |||
| Spermatogenesis/spermiogenesis | 246 (44.6) | ||
| Molecular interactions | 106 (19.2) | ||
| Pathophysiology | 377 (68.3) | ||
| Prediction of clinical outcomes | 841 (65.4) | ||
| Post-operative recurrence | 381 (29.6) | ||
| Biochemical markers | 226 (17.6) | ||
| Indication of surgical or medical treatment in varicocele diagnosis | 571 (44.4) | ||
| Studies investigating non-surgical and surgical approaches for varicocele treatment (n=1,271) | |||
| Non-surgical approaches | 260 (20.5) | ||
| Non-surgical pharmaceutical | 46 (17.7) | ||
| Non-surgical antioxidants | 24 (9.2) | ||
| Radiological approaches and complementary medicine | 199 (76.5) | ||
| Surgical approaches for varicocele | 1,130 (88.9) | ||
Data are reported as number of publications (n) and percentage (%) out of the total number of publications collected in Scopus.
5. Prognostic and diagnostic studies
All included publications were analyzed based on prognostic or diagnostic studies on varicocele, which included the prediction of clinical outcomes, post-operative recurrence of varicocele, biochemical markers, and indication of surgical or medical treatment in varicocele diagnosis. From a total of 1,285 publications, results indicate that the most reported area was on the prediction of clinical outcomes (n=841, 65.4%), followed by the indication of surgical or medical treatment in varicoceles (n=571, 44.4%) and the post-operative recurrence (n=381, 29.6%), whereas biochemical markers were reported less frequently (n=226, 17.6%) (Table 3).
6. Methods of varicocele treatment
Out of 1,943 articles retrieved by Scopus, 1,271 (65.4%) articles discussed various approaches to treat varicocele (Table 3). Surgical approaches were well studied (n=1,130, 88.9% of cases). The non-surgical approaches for varicocele analyzed (n=260, 20.5%) included three different sub-classifications such as pharmaceutical treatment (n=46, 17.7%), treatment with antioxidants (n=24, 9.2%) as well as radiological and complementary approaches (n=199, 76.5%).
7. Impact of varicocele and varicocele treatment
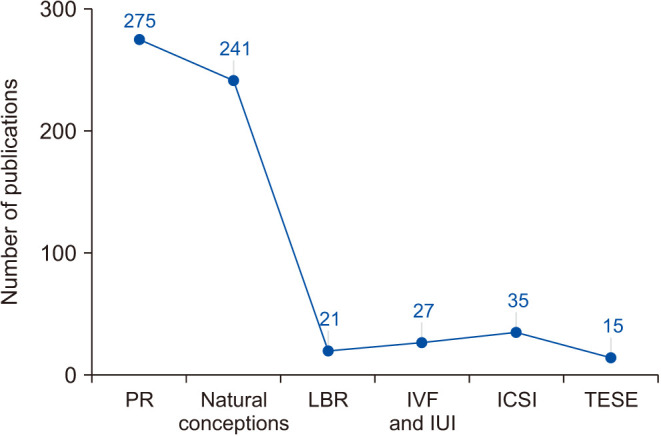
Among studies reporting the impact of varicocele and its treatment on outcomes (n=1,447), semen parameters are the most covered outcomes being mentioned in 915 (63.2%) articles (Fig. 7). The interest in the subject has risen steadily over time, with 2015 being the most productive year. The second most reported outcome has been vasculature and blood flow, being addressed in 314 (21.7%) articles. The interest in seminal OS is comparable to the interest in sperm DNA damage or SDF, reported in 98 (6.8%) and 92 (6.4%) publications, respectively. The interest in both seminal OS and SDF in varicocele publications has increased over time. PR and natural conception were reported in 275 (19.0%) and 241 (16.7%) articles, respectively (Fig. 8). Interestingly, LBR has been reported in only 21 (1.5%) articles.
Fig. 7. Trend of publications in original human studies investigating the impact of varicocele/varicocele treatment on several different outcomes. SDF: sperm DNA fragmentation.

Fig. 8. Trend of publications in original human studies investigating the impact of varicocele/varicocele treatment on reproductive outcomes. PR: pregnancy rate, LBR: live birth rate, IVF: in vitro fertilization, IUI: intrauterine insemination, ICSI: intracytoplasmic sperm injection, TESE: testicular sperm extraction.
DISCUSSION
Based on our review of the literature, this scientometric analysis is the first of its kind focusing on varicocele. Our data showed that the trend of publication of original human studies on varicocele particularly increased during the period 2002 to 2014. Previous scientometric studies showed increasing research in male infertility in general, and hence in varicocele as a common clinical concern and cause of infertility [26,29,34]. Interestingly, the years 2002 to 2014 correspond to the years of publications of guidelines on varicocele. These include the practice guidelines on varicocele and male infertility issued by the EAU in 2002 [35] and 2005 [36], the AUA in 2004 [37], as well as ASRM in 2006 [38], 2008 [39], and 2014 [40]. Additionally, possible factors contributing to the increasing number of publications might be the increasing availability of ultrasonography that has improved the diagnosis of varicocele as well as the implementation of new surgical techniques and the need for comparison between them. The increased trend of original articles on varicocele may be an indication of intensified interest to unfold the dynamics of varicocele and male infertility.
1. Demographics of publications (countries, institutions, journals, authors)
The articles published on varicocele treatment are predominantly from top institutions in the northern hemisphere and developed countries, while only one is located in the southern hemisphere. This may result in a bias in outcomes that may not be generalized to other countries. Excluding the USA and China, research teams from Italy, Turkey, and Japan lead the total number of published papers per year in science and technology [41]. One of the contributing factors for this interest is the existence of specialized journals in these countries, particularly periodicals of national scope. Another significant factor may be the competitiveness between groups working within the same country.
The majority of original human studies on varicocele were published in journals from the USA (The Journal of Urology and Urology) and Germany (Andrologia). These journals belong to either the first or second quartile of the subject category for Urology, indicating that human studies on varicocele were published in key journals within the field. The publications in the top three journals (Journal of Urology, Andrologia, and Urology) were mainly prognostic/diagnostic studies and those related to surgical techniques. The journal with the highest impact factor (IF) in the top 10 list was the Q1 journal, European Urology (IF=20.096 in 2021).
Although network map analysis for countries showed several interconnected nodal points, with the USA being the largest, this analysis also revealed that Agarwal A. from Cleveland Clinic, USA, is a center point of worldwide varicocele research collaborations, connecting three other individually isolated groups of researchers. With a prolific extent of research collaborations, Agarwal A. facilitated a global approach to the conceptualization and management of varicocele, linking the leads in varicocele research from South America (with Hallak J., Bertolla R.P., and Pasqualotto F.F.), Spain (with Gosálvez J. and Amengual M.J.), and Italy (with Gentile V. and Mazzoni G.), as well as many other established scientists (Fig. 5). Previous scientometric studies also highlighted Agarwal A. as the highest contributor in male infertility research, specifically on topics such as SDF and male infertility [25], OS in male fertility [26], the role of antioxidants in improving semen parameters [27], the contribution of ART in addressing infertility [28], as well as employing innovative tools such as proteomics to investigate and manage male infertility [29].
2. Publication topics
The analysis of the recurrent keywords provides insights into the fields towards which the research is evolving [42,43,44]. Word co-occurrence analysis is a method for detecting major themes in a given research field. It is used to determine the intellectual structure and the main topics of studies by using visual maps [45,46]. This analysis can even provide precise information on the topics of the studies and their evolution over time. According to this network analysis, the word “laparoscopic” has been the most used in the last few decades. As this technique has been progressively replaced by the microsurgical technique, the keywords perfectly reflect the advances in this field. Similarly, the main areas studied are adolescence and fertility, which correspond to the state of clinical practice on varicocele management. Interestingly, the words concerning adolescence and laparoscopic techniques have been replaced in the last ten years by words concerning fertility, the efficacy of microsurgical techniques, infertility, and the associations of varicocele with clinical factors such as body mass index and OS. This shows a change in the research and clinical practice of varicocele in humans in recent years.
3. Varicocele in adolescents and adults
Studies of varicoceles in adolescents are underrepresented compared with studies of varicoceles in adults (ratio around 1:4). Since the 1990s, the management of varicocele in adolescents has been a dilemma [7,47]. In adolescents, ASRM/AUA recommend repair of varicoceles associated with a persistent reduction in testicular size homolateral to the varicocele or with semen abnormalities. EAU recommends varicocele repair in cases of ipsilateral reduction in testicular volume and evidence of progressive testicular dysfunction (weak recommendation, level of evidence 2a) [22,40]. EAU guidelines also caution against possible overtreatment of varicocele in adolescents [22], noting that many adolescents with varicocele will not experience fertility problems (level of evidence 3), and providing a reminder that in the literature long-term studies of adolescents are still rare. Additionally, ensuring follow-up in adulthood for these patients is a major challenge [48]. Furthermore, adolescent varicoceles are usually diagnosed incidentally, and the presentation of symptomatic cases may differ during pubertal development [49]. Some adolescents may be reluctant to access urologic care even if they are symptomatic and delay genital examination. In addition, collection of semen samples from post-pubertal patients is not always feasible [50] and there are no reference standards for interpreting semen analysis in this population [49]. All of the above-mentioned reasons could explain the difficulties in conducting high-quality studies on adolescent varicocele and hence explain why the management of varicocele in adolescents is still subject to question or caution today. Controversies on this topic may still remain unresolved, as our keyword analysis indicates that the focus of research has recently shifted from adolescent to adult fertility.
4. Prevalence, pathophysiology, etiology, and risk factors
Varicocele is relatively common in men, developing anytime between puberty and late adulthood, but mostly detected amongst men of reproductive age [51]. Despite this, reports on varicocele prevalence are very rare, accounting for about 1.6% of all studies. This stems from the asymptomatic nature of varicocele and the need for large and well-designed studies with more emphasis on the studied population [3].
Mechanistic studies are relatively numerous, they are mainly interested in the pathophysiology of varicocele and the mechanisms of action on spermatogenesis. Fewer studies were interested in investigating molecular markers. This may be explained considering that mechanistic studies in humans are more difficult than in animals. Studies on risk factors are also underrepresented, accounting for 11.4% of all studies. According to the scientometric analysis of keywords, the associations between varicocele and body mass index or OS seem to be the most studied ones in the last 10 years. To understand why relatively few studies have focused on etiological factors involved in the genesis of varicocele, and risk factors associated with varicocele, it should be noted that long-term cohort studies are difficult to conduct, particularly in adolescents, since follow-up should be extended to the age of fatherhood. This probably explains why etiological and risk factors are poorly studied, although these may be helpful to urologists to act preventively, adapt their follow-up and make decisions about whether or not to treat varicocele [52]. Although the latest ASRM/AUA/EAU guidelines deal well with recommendations for varicocele repair, the notion of risk factors is not addressed [21,22]. According to the keyword mapping, it is possible that these topics will be addressed in the coming years and be the focus of future guidelines.
5. Prognostic and diagnostic studies
Results emerging from the current analysis indicate that studies predicting clinical outcomes, and indications of varicocele repair, accounted for 65.4% and 44.4% of all retrieved publications on prognosis and diagnosis, respectively. Such findings reflect a great interest of researchers towards the identification and definition of predictors of success following varicocele repair. This is particularly true in the context of male infertility where the choice of the proper management plan helps select patients that would benefit from varicocele repair, and avoid performing unnecessary surgery in others. Despite numerous studies on this subject, it is still impossible to distinguish those patients who will be infertile from those who will be able to conceive spontaneously. It is also impossible to predict which patient will benefit the most from varicocele repair.
According to our analysis, varicocele recurrence is also well studied (29.6% of articles on prognosis and diagnosis). The rate of varicocele recurrence following repair ranges between 0.6% and 28.0%, depending on the chosen technique [53,54,55,56]. However, the exact factors that predispose patients to a recurrence are not clear and warrant additional research. On the other hand, biochemical markers were reported in only 17.6% of all retrieved studies on varicocele. These studies focused on understanding the pathophysiological mechanisms underlying the detrimental effects of varicocele on the reproductive health of some men. This relatively low frequency could be explained by the fact that our bibliometric analysis focused on humans, whereas biochemical markers are probably more investigated in animals.
6. Methods of varicocele treatment
Our study has shown higher interest (88.9%) in choosing surgical rather than non-surgical options (20.5%) in the management of varicocele. In 1951, varicocele repair was introduced by Tulloch [57] as a way to treat male infertility and, in 1975, this was further confirmed in 504 infertile patients using the internal spermatic vein high ligation technique [58]. This could be explained by the desire to achieve quick and more reliable therapeutic results [59] and the lack of strong evidence of the role of medical therapy [60]. The publication trend with the preference for surgical treatment is consistent with the recommendations of professional societies [21,40,61]. There is indeed a common consensus regarding the management of varicocele in infertile men among the international societies. However, the guidelines differ in the grade of evidence and in the detailed description of varicocele management. The AUA/ASRM [21] and the EAU [22,62] agree on the surgical management of clinical (palpable) varicocele in non-azoospermic infertile men with impaired sperm parameters associated with otherwise non-explained infertility (moderate recommendation and evidence level B for the AUA/ASRM, strong recommendation and level of evidence 1a for the EAU). There is also a consensus among professional societies that the gold standard for the treatment of varicocele is surgical repair using microsurgical techniques [21,63]. From our keyword analysis, it is possible to clearly see the shift in the research focus around the world over the last 10 years, where the keyword “laparoscopic” has been replaced by “microsurgical” in publications.
Currently, there is a lack of data on the comparison of the efficacy of antioxidant treatment versus surgical repair in the management of infertile men with varicocele. Compared to placebo, antioxidants have been shown to improve semen parameters but not to increase PR in infertile patients with varicocele [64]. However, a recent randomized controlled trial indicated a significant increase in PR in patients treated with antioxidants after varicocelectomy than those treated solely by surgery (29% vs. 17.9%, p=0.029) [65]. Additionally, a meta-analysis showed that antioxidant therapy can improve semen quality after varicocelectomy [66]. Finally, with the terms “efficacy” and “oxidative stress” becoming more commonly used, it is likely that the role of antioxidants in this setting is becoming more popular.
7. Impacts of varicocele and varicocele repair
Manuscripts that have looked at the impact of varicocele and varicocele repair have used sperm parameters as the primary outcome measured in the majority of cases. Being a simple test, semen analysis has proved to be a useful guide to fertility and is therefore helpful in diagnosis, prognosis and as a gauge of efficacy of varicocele repair [67]. It is also more advantageous than other tests in terms of time, cost and applicability [68], and less financially burdening as a test compared to the more advanced fertility tests, justifying its common utilization in clinical practice. In order to increase the strength of evidence that semen parameters improve after varicocele repair, various studies have tried to group the available data into meta-analyses [69]. The limitation of considering the improvement of semen parameters at follow-up as the primary outcome is that improved semen parameters is not the ultimate goal for the infertile couple. Also, as the guidelines and standard values utilized vary according to the different editions of the World Health Organization (WHO) manual referred to, as a variation in results can be expected when a particular edition is followed versus the other [70,71]. Furthermore, conventional semen analysis does not assess the sperm changes taking place in the female tract prior to fertilization or advanced parameters such as DNA integrity and OS [72].
In the current analysis, PR and natural conception, as well as LBR were less investigated outcomes (19.0%, 16.7%, and 1.5% of all articles, respectively). Interest in this realm has increased over the time with the highest results in 2015, although other outcome variables like testicular histology remained constant. Including the reproductive outcomes in a study requires longer time and more effort than examining the semen parameters. Hence, evaluating and reporting reproductive outcomes in a large study with an adequate sample size is particularly challenging. Also, assisted reproduction outcomes are influenced by several parameters other than semen quality, such as the ovarian response to stimulation protocols, quality of oocytes, experience and technical skills of the embryologist, therefore introducing more confounders in the analysis [73,74]. Natural conception and PR can be assessed at one time without the need for follow-up till the end of pregnancy. On the contrary, LBR is a complex outcome to measure because of the longer follow-up duration. This may hinder a large-scale study and explain why so few studies have reported this outcome over the past decades.
Finally, several factors may explain why studies pertaining to varicocele and their impact on SDF and seminal OS are low in the current literature. There are several tests evaluating SDF which are laborious, require high precision and expensive equipment along with skilled technicians, and mostly they lack in standardization, which raises the difficulty of interpretation [75,76,77,78]. There is also a lack of consensus amongst experts about which clinical scenarios these tests should be used in as well as some debate regarding whether varicocele treatment can help improve elevated SDF and OS [79]. Although it is well established that SDF and OS play a fundamental role in varicocele-induced male infertility, the opposite is not true. Elevated SDF or OS values do not necessarily lead to a diagnosis of varicocele [1,80].
8. Limitations
Despite interesting data emerging from the current study, few limitations are noted. First, our study utilized a single bibliographic database (Scopus), and therefore varicocele articles which were not indexed in this database are excluded. Future studies could endeavor to incorporate other databases such as Web of Science and PubMed. Second, although our study was able to analyze separately the publications concerning adolescents from those concerning adults, it was not able to analyze the trends in the studied parameters among males with advanced age. Finally, an inherent limitation of the scientometric method is the retrospective nature of this analysis.
CONCLUSIONS
This study has provided an in-depth, detailed analysis of the publication trends in original human studies on varicocele, showing a general upward trend over a span of 33 years. The varicocele research landscape appears to have progressed from that of adolescent varicocele and laparoscopic varicocele repair in the early years to male fertility status, clinical efficacy of microsurgical repair, and the association between varicocele and factors such as body mass index or seminal OS in the past decade.
Our results suggest that although some aspects of varicocele are well studied, there are still many facets of varicocele and male infertility that have not been fully elucidated and therefore require greater attention. In fact, the prevalence of varicocele and risk factors remain little investigated. Similarly, the impact of varicocele and its treatment is largely analyzed through basic sperm parameters, but fewer studies have focused on seminal OS and SDF, a gap which might be filled in the coming years. In addition, the scientometric analysis showed that fewer studies looked at reproductive outcome rates of different ARTs. The paternity endpoint is rarely chosen in the current publication on varicocele, even though it would address several important questions about the impact of varicocele and its management on spontaneous or assisted fertility.
Besides well-designed, large-scale clinical studies with long-term follow-up, greater traction on the various aspects of varicocele research could be achieved through global collaborations between clinical and research institutions alike. These types of collaborative studies could help i) clarify the long-standing question of why varicocele impairs fertility only in certain males and what makes them predisposed to these changes, ii) elucidate the fundamental reasons of how and when varicocele-mediated damage develops in these males, and ultimately iii) contribute towards better clinical practice in managing varicocele throughout the world.
Acknowledgements
Authors are thankful to the artists from the Cleveland Clinic’s Center for Medical Art & Photography for their help with the illustrations. The study was supported by the American Center for Reproductive Medicine.
Footnotes
Conflict of Interest: The authors have nothing to disclose.
Funding: None.
- Conceptualization: AA, RF, DD, KL, RH.
- Writing – original draft: All the authors.
- Writing – review & editing: All the authors.
References
- 1.Su JS, Farber NJ, Vij SC. Pathophysiology and treatment options of varicocele: an overview. Andrologia. 2021;53:e13576. doi: 10.1111/and.13576. [DOI] [PubMed] [Google Scholar]
- 2.Akbay E, Cayan S, Doruk E, Duce MN, Bozlu M. The prevalence of varicocele and varicocele-related testicular atrophy in Turkish children and adolescents. BJU Int. 2000;86:490–493. doi: 10.1046/j.1464-410x.2000.00735.x. [DOI] [PubMed] [Google Scholar]
- 3.Alsaikhan B, Alrabeeah K, Delouya G, Zini A. Epidemiology of varicocele. Asian J Androl. 2016;18:179–181. doi: 10.4103/1008-682X.172640. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Clavijo RI, Carrasquillo R, Ramasamy R. Varicoceles: prevalence and pathogenesis in adult men. Fertil Steril. 2017;108:364–369. doi: 10.1016/j.fertnstert.2017.06.036. [DOI] [PubMed] [Google Scholar]
- 5.Saypol DC. Varicocele. J Androl. 1981;2:61–71. [Google Scholar]
- 6.Jensen CFS, Østergren P, Dupree JM, Ohl DA, Sønksen J, Fode M. Varicocele and male infertility. Nat Rev Urol. 2017;14:523–533. doi: 10.1038/nrurol.2017.98. [DOI] [PubMed] [Google Scholar]
- 7.Gorelick JI, Goldstein M. Loss of fertility in men with varicocele. Fertil Steril. 1993;59:613–616. [PubMed] [Google Scholar]
- 8.Jarow JP, Coburn M, Sigman M. Incidence of varicoceles in men with primary and secondary infertility. Urology. 1996;47:73–76. doi: 10.1016/s0090-4295(99)80385-9. [DOI] [PubMed] [Google Scholar]
- 9.Sofikitis NV, Miyagawa I, Incze P, Andrighetti S. Detrimental effect of left varicocele on the reproductive capacity of the early haploid male gamete. J Urol. 1996;156:267–270. [PubMed] [Google Scholar]
- 10.Agarwal A, Hamada A, Esteves SC. Insight into oxidative stress in varicocele-associated male infertility: part 1. Nat Rev Urol. 2012;9:678–690. doi: 10.1038/nrurol.2012.197. [DOI] [PubMed] [Google Scholar]
- 11.Ichioka K, Nagahama K, Okubo K, Soda T, Ogawa O, Nishiyama H. Genetic polymorphisms in glutathione S-transferase T1 affect the surgical outcome of varicocelectomies in infertile patients. Asian J Androl. 2009;11:333–341. doi: 10.1038/aja.2008.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Omar SS, Mahfouz W, Dawood W, Abo El-Wafa RAH, Ghazala RA, Zahran AM. Relation of nitric oxide synthase gene (NOS3) polymorphisms to varicocele risk and post-varicocelectomy seminal oxidative stress reduction. Andrologia. 2020;52:e13525. doi: 10.1111/and.13525. [DOI] [PubMed] [Google Scholar]
- 13.Gentile V, Nicotra M, Scaravelli G, Antonini G, Ambrosi S, Saccucci P, et al. ACP1 genetic polymorphism and spermatic parameters in men with varicocele. Andrologia. 2014;46:147–150. doi: 10.1111/and.12059. [DOI] [PubMed] [Google Scholar]
- 14.Nayeri M, Talebi AR, Heidari MM, Seifati SM, Tabibnejad N. Polymorphisms of sperm protamine genes and CMA3 staining in infertile men with varicocele. Rev Int Androl. 2020;18:7–13. doi: 10.1016/j.androl.2018.07.005. [DOI] [PubMed] [Google Scholar]
- 15.Allamaneni SS, Naughton CK, Sharma RK, Thomas AJ, Jr, Agarwal A. Increased seminal reactive oxygen species levels in patients with varicoceles correlate with varicocele grade but not with testis size. Fertil Steril. 2004;82:1684–1686. doi: 10.1016/j.fertnstert.2004.04.071. [DOI] [PubMed] [Google Scholar]
- 16.Naughton CK, Nangia AK, Agarwal A. Pathophysiology of varicoceles in male infertility. Hum Reprod Update. 2001;7:473–481. doi: 10.1093/humupd/7.5.473. [DOI] [PubMed] [Google Scholar]
- 17.Razi M, Tavalaee M, Sarrafzadeh-Rezaei F, Moazamian A, Gharagozloo P, Drevet JR, et al. Varicocoele and oxidative stress: new perspectives from animal and human studies. Andrology. 2021;9:546–558. doi: 10.1111/andr.12940. [DOI] [PubMed] [Google Scholar]
- 18.Agarwal A, Prabakaran S, Allamaneni SS. Relationship between oxidative stress, varicocele and infertility: a meta-analysis. Reprod Biomed Online. 2006;12:630–633. doi: 10.1016/s1472-6483(10)61190-x. [DOI] [PubMed] [Google Scholar]
- 19.Baskaran S, Finelli R, Agarwal A, Henkel R. Reactive oxygen species in male reproduction: a boon or a bane? Andrologia. 2021;53:e13577. doi: 10.1111/and.13577. [DOI] [PubMed] [Google Scholar]
- 20.Hamada A, Esteves SC, Agarwal A. Insight into oxidative stress in varicocele-associated male infertility: part 2. Nat Rev Urol. 2013;10:26–37. doi: 10.1038/nrurol.2012.198. [DOI] [PubMed] [Google Scholar]
- 21.Schlegel PN, Sigman M, Collura B, De Jonge CJ, Eisenberg ML, Lamb DJ, et al. Diagnosis and treatment of infertility in men: AUA/ASRM guideline part II. Fertil Steril. 2021;115:62–69. doi: 10.1016/j.fertnstert.2020.11.016. [DOI] [PubMed] [Google Scholar]
- 22.Salonia A, Bettocchi C, Carvalho J, Corona G, Jones TH, Kadioǧlu A, et al. Sexual and reproductive health [Internet] Arnhem: European Association of Urology; c2020. [cited 2021 Oct 15]. Available from: https://uroweb.org/guideline/sexual-and-reproductive-health/ [Google Scholar]
- 23.Kim MC, Zhu Y. In: Scientometrics. Jibu M, Osabe Y, editors. London: IntechOpen; 2018. Scientometrics of scientometrics: mapping historical footprint and emerging technologies in scientometrics. [Google Scholar]
- 24.Leydesdorff L, Milojević S. In: International encyclopedia of the social & behavioral sciences. 2nd ed. Wright JD, editor. Oxford: Elsevier; 2015. Scientometrics; pp. 322–327. [Google Scholar]
- 25.Baskaran S, Agarwal A, Panner Selvam MK, Finelli R, Robert KA, Iovine C, et al. Tracking research trends and hotspots in sperm DNA fragmentation testing for the evaluation of male infertility: a scientometric analysis. Reprod Biol Endocrinol. 2019;17:110. doi: 10.1186/s12958-019-0550-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Agarwal A, Baskaran S, Panner Selvam MK, Finelli R, Barbarosie C, Robert KA, et al. Scientific landscape of oxidative stress in male reproductive research: a scientometric study. Free Radic Biol Med. 2020;156:36–44. doi: 10.1016/j.freeradbiomed.2020.05.008. [DOI] [PubMed] [Google Scholar]
- 27.Agarwal A, Selvam MKP, Baskaran S, Finelli R, Leisegang K, Barbăroşie C, et al. Highly cited articles in the field of male infertility and antioxidants: a scientometric analysis. World J Mens Health. 2021;39:760–775. doi: 10.5534/wjmh.200181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Agarwal A, Panner Selvam MK, Baskaran S, Finelli R, Leisegang K, Barbăroşie C, et al. A scientometric analysis of research publications on male infertility and assisted reproductive technology. Andrologia. 2021;53:e13842. doi: 10.1111/and.13842. [DOI] [PubMed] [Google Scholar]
- 29.Agarwal A, Baskaran S, Panner Selvam MK, Barbăroşie C, Master K. Unraveling the footsteps of proteomics in male reproductive research: a scientometric approach. Antioxid Redox Signal. 2020;32:536–549. doi: 10.1089/ars.2019.7945. [DOI] [PubMed] [Google Scholar]
- 30.Van Eck NJ, Waltman L. Text mining and visualization using VOSviewer. ISSI Newsl. 2011;7:50–54. [Google Scholar]
- 31.Scimago. Journal rankings on urology [Internet] Madrid: Scimago; c2021. [cited 2021 Oct 15]. Available from: https://www.scimagojr.com/journalrank.php?category=2748 . [Google Scholar]
- 32.Scimago. Journal rankings on reproductive medicine [Internet] Madrid: Scimago; c2021. [cited 2021 Oct 15]. Available from: https://www.scimagojr.com/journalrank.php?category=2743 . [Google Scholar]
- 33.Scimago. Zhonghua nan ke xue = National journal of andrology [Internet] Madrid: Scimago; c2021. [cited 2021 Oct 15]. Available from: https://www.scimagojr.com/journalsearch.php?q=61342&tip=sid&clean=0 . [Google Scholar]
- 34.Baskaran S, Agarwal A, Leisegang K, Pushparaj PN, Panner Selvam MK, Henkel R. An in-depth bibliometric analysis and current perspective on male infertility research. World J Mens Health. 2021;39:302–314. doi: 10.5534/wjmh.180114. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Weidner W, Colpi GM, Hargreave TB, Papp GK, Pomerol JM, Ghosh C EAU Working Group on Male Infertility. EAU guidelines on male infertility. Eur Urol. 2002;42:313–322. doi: 10.1016/s0302-2838(02)00367-6. [DOI] [PubMed] [Google Scholar]
- 36.Dohle GR, Colpi GM, Hargreave TB, Papp GK, Jungwirth A, Weidner W EAU Working Group on Male Infertility. EAU guidelines on male infertility. Eur Urol. 2005;48:703–711. doi: 10.1016/j.eururo.2005.06.002. [DOI] [PubMed] [Google Scholar]
- 37.Male Infertility Best Practice Policy Committee of the American Urological Association; Practice Committee of the American Society for Reproductive Medicine. Report on varicocele and infertility. Fertil Steril. 2004;82 Suppl 1:S142–S145. doi: 10.1016/j.fertnstert.2004.05.057. [DOI] [PubMed] [Google Scholar]
- 38.Practice Committee of the American Society for Reproductive Medicine. Report on varicocele and infertility. Fertil Steril. 2006;86(5 Suppl 1):S93–S95. doi: 10.1016/j.fertnstert.2006.07.1486. [DOI] [PubMed] [Google Scholar]
- 39.Practice Committee of American Society for Reproductive Medicine. Report on varicocele and infertility. Fertil Steril. 2008;90(5 Suppl):S247–S249. doi: 10.1016/j.fertnstert.2008.08.050. [DOI] [PubMed] [Google Scholar]
- 40.Practice Committee of the American Society for Reproductive Medicine; Society for Male Reproduction and Urology. Report on varicocele and infertility: a committee opinion. Fertil Steril. 2014;102:1556–1560. doi: 10.1016/j.fertnstert.2014.10.007. [DOI] [PubMed] [Google Scholar]
- 41.National Science Foundation. Scientific and technical journal articles [Internet]. Washington, D.C.: World Bank Group; c2021. [cited 2021 Oct 15]. Available from: https://data.worldbank.org/indicator/IP.JRN.ARTC.SC?end=2018&start=2000&view=chart&year_low_desc=true . [Google Scholar]
- 42.Sun Y, Li C, Zhao Y, Sun J. Trends and developments in oral health literacy: a scientometric research study (1991-2020) BDJ Open. 2021;7:13. doi: 10.1038/s41405-021-00066-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Briones-Bitar J, Carrión-Mero P, Montalván-Burbano N, Morante-Carballo F. Rockfall research: a bibliometric analysis and future trends. Geosciences. 2020;10:403 [Google Scholar]
- 44.Courtial JP. A coword analysis of scientometrics. Scientometrics. 1994;31:251–260. [Google Scholar]
- 45.Carrión-Mero P, Montalván-Burbano N, Paz-Salas N, Morante-Carballo F. Volcanic geomorphology: a review of worldwide research. Geosciences. 2020;10:347 [Google Scholar]
- 46.Dong D, Chen ML. Publication trends and co-citation mapping of translation studies between 2000 and 2015. Scientometrics. 2015;105:1111–1128. [Google Scholar]
- 47.Zundel S, Szavay P, Stanasel I. Management of adolescent varicocele. Semin Pediatr Surg. 2021;30:151084. doi: 10.1016/j.sempedsurg.2021.151084. [DOI] [PubMed] [Google Scholar]
- 48.Suson KD. Transitional urology for male adolescents: what adult urologists should know. Curr Urol Rep. 2016;17:71. doi: 10.1007/s11934-016-0630-2. [DOI] [PubMed] [Google Scholar]
- 49.Chung JM, Lee SD. Current issues in adolescent varicocele: pediatric urological perspectives. World J Mens Health. 2018;36:123–131. doi: 10.5534/wjmh.170053. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Daudin M, Rives N, Walschaerts M, Drouineaud V, Szerman E, Koscinski I, et al. Sperm cryopreservation in adolescents and young adults with cancer: results of the French national sperm banking network (CECOS) Fertil Steril. 2015;103:478–486.e1. doi: 10.1016/j.fertnstert.2014.11.012. [DOI] [PubMed] [Google Scholar]
- 51.Canales BK, Zapzalka DM, Ercole CJ, Carey P, Haus E, Aeppli D, et al. Prevalence and effect of varicoceles in an elderly population. Urology. 2005;66:627–631. doi: 10.1016/j.urology.2005.03.062. [DOI] [PubMed] [Google Scholar]
- 52.Sack BS, Schäfer M, Kurtz MP. The dilemma of adolescent varicoceles: do they really have to be repaired? Curr Urol Rep. 2017;18:38. doi: 10.1007/s11934-017-0686-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Goldstein M, Gilbert BR, Dicker AP, Dwosh J, Gnecco C. Microsurgical inguinal varicocelectomy with delivery of the testis: an artery and lymphatic sparing technique. J Urol. 1992;148:1808–1811. doi: 10.1016/s0022-5347(17)37035-0. [DOI] [PubMed] [Google Scholar]
- 54.Homonnai ZT, Fainman N, Engelhard Y, Rudberg Z, David MP, Paz G. Varicocelectomy and male fertility: comparison of semen quality and recurrence of varicocele following varicocelectomy by two techniques. Int J Androl. 1980;3:447–458. doi: 10.1111/j.1365-2605.1980.tb00133.x. [DOI] [PubMed] [Google Scholar]
- 55.Kaufman SL, Kadir S, Barth KH, Smyth JW, Walsh PC, White RI., Jr Mechanisms of recurrent varicocele after balloon occlusion or surgical ligation of the internal spermatic vein. Radiology. 1983;147:435–440. doi: 10.1148/radiology.147.2.6836122. [DOI] [PubMed] [Google Scholar]
- 56.Marmar JL, Kim Y. Subinguinal microsurgical varicocelectomy: a technical critique and statistical analysis of semen and pregnancy data. J Urol. 1994;152:1127–1132. doi: 10.1016/s0022-5347(17)32521-1. [DOI] [PubMed] [Google Scholar]
- 57.Tulloch WS. A consideration of sterility factors in the light of subsequent pregnancies. II. Sub fertility in the male. (Tr. Edinburgh Obst. Soc. Session 104) Edinb Med J. 1951-1952;59:29–34. [PMC free article] [PubMed] [Google Scholar]
- 58.Dubin L, Amelar RD. Varicocelectomy as therapy in male infertility: a study of 504 cases. Fertil Steril. 1975;26:217–220. doi: 10.1016/s0015-0282(16)40988-x. [DOI] [PubMed] [Google Scholar]
- 59.Watanabe M, Nagai A, Kusumi N, Tsuboi H, Nasu Y, Kumon H. Minimal invasiveness and effectivity of subinguinal microscopic varicocelectomy: a comparative study with retroperitoneal high and laparoscopic approaches. Int J Urol. 2005;12:892–898. doi: 10.1111/j.1442-2042.2005.01142.x. [DOI] [PubMed] [Google Scholar]
- 60.Garg H, Kumar R. An update on the role of medical treatment including antioxidant therapy in varicocele. Asian J Androl. 2016;18:222–228. doi: 10.4103/1008-682X.171657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Jarow JP, Sharlip ID, Belker AM, Lipshultz LI, Sigman M, Thomas AJ, et al. Male Infertility Best Practice Policy Committee of the American Urological Association Inc. Best practice policies for male infertility. J Urol. 2002;167:2138–2144. [PubMed] [Google Scholar]
- 62.Jungwirth A, Giwercman A, Tournaye H, Diemer T, Kopa Z, Dohle G, et al. European Association of Urology Working Group on Male Infertility. European Association of Urology guidelines on male infertility: the 2012 update. Eur Urol. 2012;62:324–332. doi: 10.1016/j.eururo.2012.04.048. [DOI] [PubMed] [Google Scholar]
- 63.Jungwirth A, Diemer T, Kopa Z, Krausz C, Minhas S, Tournaye H. Male infertility [Internet] Arnhem: European Association of Urology; c2019. [cited 2021 Oct 15]. Available from: https://uroweb.org/guideline/male-infertility/ [Google Scholar]
- 64.Pyrgidis N, Sokolakis I, Palapelas V, Tishukov M, Mykoniatis I, Symeonidis EN, et al. The effect of antioxidant supplementation on operated or non-operated varicocele-associated infertility: a systematic review and meta-analysis. Antioxidants (Basel) 2021;10:1067. doi: 10.3390/antiox10071067. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Kızılay F, Altay B. Evaluation of the effects of antioxidant treatment on sperm parameters and pregnancy rates in infertile patients after varicocelectomy: a randomized controlled trial. Int J Impot Res. 2019;31:424–431. doi: 10.1038/s41443-018-0109-4. [DOI] [PubMed] [Google Scholar]
- 66.Wang J, Wang T, Ding W, Wu J, Wu G, Wang Y, et al. Efficacy of antioxidant therapy on sperm quality measurements after varicocelectomy: a systematic review and meta-analysis. Andrologia. 2019;51:e13396. doi: 10.1111/and.13396. [DOI] [PubMed] [Google Scholar]
- 67.Agarwal A, Sharma R, Harlev A, Esteves SC. Effect of varicocele on semen characteristics according to the new 2010 World Health Organization criteria: a systematic review and meta-analysis. Asian J Androl. 2016;18:163–170. doi: 10.4103/1008-682X.172638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Flint M, Lampiao F, Agarwal A, du Plessis SS. In: Practical manual of in vitro fertilization: advanced methods and novel devices. Nagy ZP, Varghese AC, Agarwal A, editors. New York: Springer; 2012. Sperm assessment: traditional approaches and their indicative value; pp. 185–192. [Google Scholar]
- 69.Shridharani A, Owen RC, Elkelany OO, Kim ED. The significance of clinical practice guidelines on adult varicocele detection and management. Asian J Androl. 2016;18:269–275. doi: 10.4103/1008-682X.172641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Ford WC. Comments on the release of the 5th edition of the WHO Laboratory Manual for the Examination and Processing of Human Semen. Asian J Androl. 2010;12:59–63. doi: 10.1038/aja.2008.57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.World Health Organization (WHO) WHO laboratory manual for the examination and processing of human semen. 5th ed. Geneva: WHO; 2010. [Google Scholar]
- 72.Wang C, Swerdloff RS. Limitations of semen analysis as a test of male fertility and anticipated needs from newer tests. Fertil Steril. 2014;102:1502–1507. doi: 10.1016/j.fertnstert.2014.10.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Gao H, Liu DE, Li Y, Wu X, Tan H. Early prediction of live birth for assisted reproductive technology patients: a convenient and practical prediction model. Sci Rep. 2021;11:331. doi: 10.1038/s41598-020-79308-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Go KJ. ‘By the work, one knows the workman’: the practice and profession of the embryologist and its translation to quality in the embryology laboratory. Reprod Biomed Online. 2015;31:449–458. doi: 10.1016/j.rbmo.2015.07.006. [DOI] [PubMed] [Google Scholar]
- 75.Esteves SC, Zini A, Coward RM, Evenson DP, Gosálvez J, Lewis SEM, et al. Sperm DNA fragmentation testing: summary evidence and clinical practice recommendations. Andrologia. 2021;53:e13874. doi: 10.1111/and.13874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Agarwal A, Panner Selvam MK, Baskaran S, Cho CL. Sperm DNA damage and its impact on male reproductive health: a critical review for clinicians, reproductive professionals and researchers. Expert Rev Mol Diagn. 2019;19:443–457. doi: 10.1080/14737159.2019.1614916. [DOI] [PubMed] [Google Scholar]
- 77.Esteves SC, Agarwal A, Cho CL, Majzoub A. A strengths-weaknesses-opportunities-threats (SWOT) analysis on the clinical utility of sperm DNA fragmentation testing in specific male infertility scenarios. Transl Androl Urol. 2017;6(Suppl 4):S734–S760. doi: 10.21037/tau.2017.08.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Evenson DP, Jost LK, Marshall D, Zinaman MJ, Clegg E, Purvis K, et al. Utility of the sperm chromatin structure assay as a diagnostic and prognostic tool in the human fertility clinic. Hum Reprod. 1999;14:1039–1049. doi: 10.1093/humrep/14.4.1039. [DOI] [PubMed] [Google Scholar]
- 79.Agarwal A, Majzoub A, Esteves SC, Ko E, Ramasamy R, Zini A. Clinical utility of sperm DNA fragmentation testing: practice recommendations based on clinical scenarios. Transl Androl Urol. 2016;5:935–950. doi: 10.21037/tau.2016.10.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Gill K, Kups M, Harasny P, Machalowski T, Grabowska M, Lukaszuk M, et al. The negative impact of varicocele on basic semen parameters, sperm nuclear DNA dispersion and oxidation-reduction potential in semen. Int J Environ Res Public Health. 2021;18:5977. doi: 10.3390/ijerph18115977. [DOI] [PMC free article] [PubMed] [Google Scholar]