

Abstract
Objective
Femoral fractures are a common cause of mortality and functional loss, mainly among older people, and there are few studies about the age in relation to traumatic femoral fractures. The aim of this study was to investigate the effect of age on the patterns of traumatic femoral fractures in patients presenting to our regional tertiary hospital.
Methods
The records of 2020 patients who presented with traumatic femoral fractures between 2013 and 2019 were retrospectively reviewed. The patients' clinical and radiographic records were reviewed. Univariate and multivariable logistic regression were used to identify independent risk factors for associated injuries and complications.
Results
The patients were divided into a child group (CH group, n = 342) aged under 18 years, a young adult group (YA group, n = 484) aged 18–60 years, and an older people group (OP group, n = 1194) aged 60 years and over. There were significant differences among the three groups in several indexes, such as sex ratio (χ 2 = 301.699, p < 0.001), osteoporosis (χ 2 = 375.463, p < 0.001), injury time of day (χ 2 = 114.913, p < 0.001), injury cause (χ 2 = 748.187, p < 0.001), injury location (χ 2 = 490.153, p < 0.001), fracture side (χ 2 = 57.000, p < 0.001), fracture site (χ 2 = 806.650, p < 0.001), associated injuries (χ 2 = 322.921, p < 0.001), coma after injury (χ 2 = 147.814, p < 0.001), non‐surgery‐related complications (χ 2 = 7.895, p = 0.019), and surgery‐related complications (χ 2 = 82.186, p < 0.001). The YA group had a significantly higher percentage of patients with surgery‐related complications than the OP group. The OP group had a higher frequency of non‐surgery‐related complications than the YA group and CH group. The most common non‐surgery‐related complications were pneumonia (7.1%) in the OP group and deep venous thrombosis (6.4%) in the YA group. Multivariable logistic regression showed that young adults, high‐energy injury, outdoors, coma after injury, and fracture sites except for the proximal region were independent risk factors for associated injuries. Older age, male, and fracture site except for the proximal region were independent risk factors for complications.
Conclusions
Traumatic femoral fractures are mostly the result of low‐energy trauma and predominantly affect the proximal site of the femur among older people. A higher rate of shaft fractures, fractures occurring outdoors, and associated injuries were observed among young adults and children than among older people.
Keywords: Age, Femoral fracture, Older people, Trauma, Young adult
Traumatic femoral fractures are mostly the result of low‐energy trauma and affect predominantly the proximal site of the femur among older people. A higher rate of shaft fractures, fractures occurring outdoors, and associated injuries were observed among the young adults and children than among the older people. Multivariable logistic regression showed that young adults, high‐energy injury, outdoors, coma after injury, fracture sites except for proximal region were independent risk factors for associated injuries. Older and male patients, fracture sites except for proximal region were independent risk factors for complications.
Introduction
Femoral fractures are a common cause of mortality and functional loss, mainly among older people. 1 , 2 , 3 , 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 Aging, which includes age‐related biomechanical changes in bone strength, and falling from a standing height or a lower height are the most common mechanisms of fragility‐related fractures among older people, and the incidence of these fractures is increasing. 1 , 2 , 3 , 4 , 5 The consequences of falls in elderly people often include fractures, immobility, and impairment and sometimes include death. In recent years, there have been many reports about traumatic femoral fractures. 4 , 5 , 6 , 7 , 8 , 9 , 10 , 11 , 12 However, there are few studies about the age differences related to traumatic femoral fractures. 5 , 12 , 13 , 14 Determination of the influence of age on the incidence of femoral fractures is complex, because many age‐related factors, including gender, trauma mechanism, would also have impact on the occurrence of the femoral fracture.
The factors influencing femoral fracture are interrelated and are not independent. Some researchers revealed that the older patients were, the higher the risk of developing proximal fractures, while they were at a lower risk of developing fractures in the shaft and distal femur. This incidence of fracture site can largely be explained by age‐related factors, including a decrease in bone strength and falling being the most common mechanism of trauma in older patients. 5 Increasing age is associated with osteoporotic bone changes, which are believed to increase the rate of femoral fracture; falls occur more frequently in the elderly. 12 , 13 Fractures in elderly patients caused by fall accidents presented with a bodily injury pattern that differs from that of adult patients and have a higher severe injury score, worse outcome, and higher mortality than those of adult patients. 13 Traffic‐related fractures caused by motorcycle or bicycle accidents occur more often in younger adults and the rate of its occurrence differs between genders. 12 , 14
It is very important to investigate the age difference in the general characteristics of traumatic femoral fracture to take preventive measures according to different age groups. At the same time, we discuss the age difference of associated injuries and complications, which is helpful for discussing the early, timely diagnosis and treatment of associated injuries and effective prevention and treatment of complications. Understanding the age differences in traumatic femoral fractures is important for the allocation of public resources, the development of preventative strategies, and efficient diagnosis and treatment. The aim of this study was to investigate the age differences in the clinical characteristics of traumatic femoral fractures, with an emphasis on the differences among children under 18 years old, young adults aged 18–60 years, and older people aged 60 years and over. Two topics have been discussed in depth: (i) To investigate the age differences of general characteristics such as injury season, cause and location, fracture side and site, associated injuries, and complications of traumatic femoral fractures; (ii) To investigate the risk factors for associated injuries and complications in the patients presented with traumatic femoral fractures.
Materials and Methods
Study Population
We retrospectively identified 2125 patients presenting to our tertiary hospital with femoral fractures between January 1, 2013, and December 31, 2019. One hundred and five patients were excluded, so 2020 patients were finally included in the study. The study was performed according to the Declaration of Helsinki and approved by the Ethics Committee of General Hospital of Northern Theater Command (approval no. Y‐2021‐009). The inclusion criteria for patients in this study were as follows: (i) patients who presented with femoral fractures on X ray, CT, and/or magnetic resonance imaging (MRI); and (ii) hospitalization for the treatment of femoral fractures between January 1, 2013, and December 31, 2019. The exclusion criteria were as follows: (i) patients with pathologic fractures; (ii) repeated hospitalizations due to injuries at the same fracture site; and (iii) patients with incomplete data. According to juveniles (under 18 years old), young adults (aged 18–60 years), and seniors (aged 60 years and over), all patients were divided into three age groups.
General Characteristics
The patients’ clinical and radiographic records were reviewed, and the general patient characteristics; cause of injury, including a high‐height fall (height ≥ 2 m), a low‐height fall (height <2 m), and road traffic crashes (RTCs); injury season (spring, summer, autumn, winter); injury time of day (0.00–6:00, 6:00–12:00, 12:00–18:00, 18:00–24:00); injury location (indoors, outdoors); fracture side (left side, right side, both sides); fracture site (proximal, shaft, distal, multiple sites) were recorded.
Associated Injuries
Associated injuries (fractures involving the leg and foot, pelvic fractures, fractures of ribs and vertebrae, skull and facial fracture, upper limb fractures, craniocerebral injury, intrathoracic injuries, intraabdominal injuries), the presence of a chronic disease (heart/brain/lung, diabetes mellitus, osteoporosis), and whether the patient was in a coma after injury was recorded.
Complications
Complications including surgery‐related complications (postoperative infections, nonunion, malunion, bone defects, internal fixation failure) and non‐surgery complications (deep venous thrombosis, pneumonia, pressure sores) were collected.
Statistical Analysis
The mean age was expressed as the mean ± SD. All data were analyzed using SPSS software (version 24.0, SPSS Inc., America). Differences in the mean value were analyzed using Student's t test. The chi‐square test was used for frequency data. p < 0.05 was considered statistically significant. Univariate and multivariable logistic regression were used to identify independent risk factors for associated injuries and complications.
Results
Age Differences of General Characteristics, Associated Injuries, and Complications
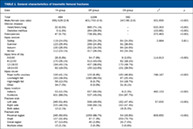
A total of 2020 patients were divided into a child group (CH group, n = 342) under 18 years old, a young adult group (YA group, n = 484) aged 18–60 years, and an older people group (OP group, n = 1194) aged 60 years and over. There were significant differences among the three groups in several indexes, such as sex ratio (χ 2 = 301.699, p < 0.001), osteoporosis (χ 2 = 375.463, p < 0.001), injury time of day (χ 2 = 114.913, p < 0.001), injury cause (χ 2 = 748.187, p < 0.001), injury location (χ 2 = 490.153, p < 0.001), fracture side (χ 2 = 57.000, p < 0.001), and fracture site (χ 2 = 806.650, p < 0.001).
The OP group included a significantly higher percentage of females and patients with chronic disease than did the YA group and CH group. Forty‐seven patients (n = 47; 9.7%) in the YA group and a total of 734 patients (n = 734; 61.5%) in the OP group were diagnosed with osteoporosis. The OP group had the highest frequency of winter fractures (n = 317; 26.5%), the YA group had the highest frequency of autumn fractures (n = 130; 26.9%), and the CH group had the highest frequency of summer fractures (n = 91; 26.6%). The OP group had the highest frequency of fractures occurring 06:00 a.m. –12:00 p.m. (n = 513; 43.0%), caused by low‐height falls (n = 1080; 90.5%), occurring indoors (n = 657; 55.0%) and occurring at a proximal site (n = 1061; 88.9%); the YA group had the highest frequency of fractures occurring 12:00–6:00 p.m. (n = 194; 40.1%), caused by road traffic accidents (n = 199; 41.1%), occurring outdoors (n = 431; 89.0%) and occurring at a proximal site (n = 245; 50.6%); and the CH group had the highest frequency of fractures occurring in the summer (n = 91; 26.6%), occurring 12:00–6:00 p.m. (n = 170; 49.7%), caused by road traffic accidents (n = 160; 46.8%), occurring outdoors (n = 334; 99.7%), and occurring in the PM shaft (n = 259%; 75.7%) (Table 1).
TABLE 1.
General characteristics of traumatic femoral fractures
| Data | YA group | OP group | CH group | χ 2 | p |
|---|---|---|---|---|---|
| Total | 484 | 1194 | 342 | ||
| Male/female (sex ratio) | 355/129 (2.8) | 401/793 (0.5) | 247/95 (2.6) | 301.699 | <0.001 |
| Chronic disease | |||||
| Heart/brain/lung | 32 (6.6%) | 885 (74.1%) | – | 633.303 | <0.001 |
| Diabetes mellitus | 9 (1.9%) | 264 (29.9%) | – | 103.681 | <0.001 |
| Osteoporosis | 47 (9.7%) | 738 (61.8%) | – | 375.463 | <0.001 |
| Injury season | |||||
| Spring | 119 (24.6%) | 289 (24.2%) | 84 (24.6%) | 2.984 | 0.811 |
| Summer | 123 (25.4%) | 296 (24.8%) | 91 (26.6%) | ||
| Autumn | 130 (26.9%) | 292 (24.5%) | 84 (24.6%) | ||
| Winter | 112 (23.1%) | 317 (26.5%) | 83 (24.3%) | ||
| Injury time of day | |||||
| 0‐6:00 | 28 (5.8%) | 94 (7.9%) | 9 (2.6%) | 114.913 | <0.001 |
| 6‐12:00 | 170 (35.1%) | 513 (43.0%) | 62 (18.1%) | ||
| 12‐18:00 | 194 (40.1%) | 437 (36.6%) | 170 (49.7%) | ||
| 18‐24:00 | 92 (19.0%) | 150 (12.6%) | 101 (29.5%) | ||
| Injury cause | |||||
| Road traffic crashes | 199 (41.1%) | 100 (8.4%) | 160 (46.8%) | 748.187 | <0.001 |
| Low‐height fall | 193 (39.9%) | 1080 (90.5%) | 87 (25.4%) | ||
| High‐height fall | 58 (12.0%) | 8 (0.7%) | 64 (18.7%) | ||
| Other | 34 (7.0%) | 6 (0.5%) | 31 (9.1%) | ||
| Injury location | |||||
| Indoors | 53 (11.0%) | 657 (55.0%) | 8 (2.3%) | 490.153 | <0.001 |
| Outdoors | 431 (89.0%) | 537 (45.0%) | 334 (97.7%) | ||
| Fracture side | |||||
| Left side | 249 (51.4%) | 596 (49.9%) | 162 (47.4%) | 57.000 | <0.001 |
| Right side | 225 (46.5%) | 598 (50.1%) | 162 (47.4%) | ||
| Both sides | 10 (2.1%) | 0 | 18 (5.3%) | ||
| Fracture site | |||||
| Proximal region | 245 (50.6%) | 1059 (88.7%) | 54 (15.8%) | 806.650 | <0.001 |
| Shaft | 157 (32.4%) | 87 (7.3%) | 259 (75.7%) | ||
| Distal region | 67 (13.8%) | 45 (3.8%) | 26 (7.6%) | ||
| Multiple sites | 15 (3.1%) | 3 (0.3%) | 3 (0.9%) | ||
There were significant differences among the three groups in several indexes, such as associated injuries (χ 2 = 322.921, p < 0.001) and coma after injury (χ 2= 147.814, p < 0.001). The YA group had a significantly higher percentage of patients with associated injuries, and coma after injury, than the OP group (p<0.001). The most common fracture‐associated injuries were fractures involving the leg and foot (n = 127; 26.2%), intrathoracic injuries (n = 92; 19.0%), and upper limb fractures (n = 88; 18.2%) in the YA group; upper limb fractures (n = 59; 4.9%), fractures of the ribs and vertebrae (n = 59; 4.9%), and fractures involving the leg and foot (n = 41; 3.4%) in the OP group; and fractures involving the leg and foot (n = 55; 16.1%), upper limb fractures (n = 32; 9.4%), and skull and facial fractures (n = 32; 9.4%) in the CH group (Table 2).
TABLE 2.
Associated injuries and complications of traumatic femoral fractures
| Data | YA group | OP group | CH group | χ 2 | p |
|---|---|---|---|---|---|
| Total | 484 | 1194 | 342 | ||
| Associated injuries | 272 (56.2%) | 169 (14.2%) | 135 (39.5%) | 322.921 | <0.001 |
| Fractures involving the leg/foot | 127 (26.2%) | 41 (3.4%) | 55 (16.1%) | ||
| Pelvic fractures | 74 (15.3%) | 27 (2.3%) | 21 (6.1%) | ||
| Fractures of ribs and vertebrae | 62 (12.8%) | 59 (4.9%) | 16 (4.7%) | ||
| Skull and facial fracture | 57 (11.8%) | 6 (0.5%) | 32 (9.4%) | ||
| Upper limb fractures | 88 (18.2%) | 59 (4.9%) | 32 (9.4%) | ||
| Craniocerebral injury | 68 (14.0%) | 30 (2.5%) | 17 (5.0%) | ||
| Intra‐thoracic injuries | 92 (19.0%) | 32 (2.7%) | 17 (5.0%) | ||
| Intra‐abdominal injuries | 43 (8.9%) | 2 (0.2%) | 6 (1.8%) | ||
| Coma after injury | 73 (15.1%) | 9 (0.8%) | 40 (11.7%) | 147.814 | <0.001 |
| Non‐surgery‐related complications | 58 (12.0%) | 185 (15.5%) | 35 (10.2%) | 7.895 | 0.019 |
| Deep venous thrombosis | 31 (6.4%) | 78 (6.5%) | 0 | ||
| Pneumonia | 23 (4.8%) | 85 (7.1%) | 3 (0.9%) | ||
| Pressure sores | 1 (0.2%) | 8 (0.7%) | 3 (0.9%) | ||
| Urinary infection | 1 (0.2%) | 16 (1.3%) | 0 | ||
| Dead | 0 | 1 (0.1%) | 1 (0.3%) | 1.801 | 0.406 |
| Surgery‐related complications | 54 (10.7%) | 15 (1.3%) | 20 (5.8%) | 82.186 | <0.001 |
There were significant differences among the three groups in several indexes, such as non‐surgery‐related complications (χ 2 = 7.895, p = 0.019) and surgery‐related complications (χ 2 = 82.186, p < 0.001). The OP group had a higher frequency of non‐surgery‐related complications than the YA group and CH group. The most common non‐surgery‐related complications were pneumonia (n = 85; 7.1%) in the OP group and deep venous thrombosis (n = 31; 6.4%) in the YA group (Table 2).
Risk Factors for Associated Injuries and Complications
In the univariate analysis, age, sex, injury cause, injury location, coma after injury, fracture side and site, presentation of heart/brain/lung disease, diabetes, and osteoporosis were associated with associated injuries. After univariate analysis, all statistically or clinically significant variables were entered into the multivariable model. A multivariable logistic regression analysis showed that the independent predictors for associated injuries were young adults, high‐energy injury, outdoors, coma after injury, and fracture sites except for the proximal region (Table 3).
TABLE 3.
Univariate and multivariable logistic regression analysis of independent risk factors for associated injuries
| Data | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | ||||
| OP group | Ref | Ref | ||
| YA group | 7.782 (6.107‐9.915) | <0.001 | 1.712 (1.216‐2.410) | 0.002 |
| CH group | 3.955 (3.016‐5.187) | <0.001 | 0.393 (0.253‐0.612) | <0.001 |
| Gender | ||||
| Female | Ref | |||
| Male | 2.349 (1.924‐2.869) | <0.001 | ||
| Injury season | ||||
| Winter | Ref | |||
| Spring | 0.875 (0.663‐1.154) | 0.344 | ||
| Summer | 1.064 (0.813‐1.391) | 0.652 | ||
| Autumn | 0.950 (0.724‐1.247) | 0.714 | ||
| Injury time of day | ||||
| 18‐24:00 | Ref | |||
| 0‐6:00 | 0.889 (0.581‐1.361) | 0.588 | ||
| 6‐12:00 | 1.250 (0.822‐1.899) | 0.297 | ||
| 12‐18:00 | 1.555 (0.992‐2.436) | 0.054 | ||
| Injury cause | ||||
| Low‐height fall | Ref | Ref | ||
| Road traffic crashes | 18.459 (14.192‐24.008) | <0.001 | 12.018 (8.467‐17.059) | <0.001 |
| High‐height fall | 21.267 (14.020‐32.261) | <0.001 | 16.956 (10.209‐28.163) | <0.001 |
| Drifting‐down injury | 16.313 (8.323‐31.976) | <0.001 | 13.095 (6.139‐27.935) | <0.001 |
| Others | 3.055 (1.341‐6.961) | 0.008 | 2.257 (0.923‐5.519) | 0.074 |
| Injury location | ||||
| Outdoors | Ref | Ref | ||
| Indoors | 0.136 (0.102‐0.181) | <0.001 | 0.599 (0.416‐0.861) | 0.006 |
| Coma after injury | ||||
| No | Ref | Ref | ||
| Yes | 21.735 (12.535‐37.685) | <0.001 | 5.271 (2.828‐9.822) | <0.001 |
| Fracture side | ||||
| Both side | Ref | |||
| Right side | 0.155 (0.067‐0.356) | <0.001 | ||
| Left side | 0.155 (0.067‐0.356) | <0.001 | ||
| Fracture site | ||||
| Proximal region | Ref | Ref | ||
| Shaft | 4.609 (3.681‐5.771) | <0.001 | 1.456 (1.019‐2.081) | 0.039 |
| Distal region | 7.550 (5.215‐10.929) | <0.001 | 3.328 (2.045‐5.414) | <0.001 |
| Multiple sites | 12.134 (4.659‐31.603) | <0.001 | 5.260 (1.594‐17.356) | 0.006 |
| Heart/brain/lung | ||||
| No | Ref | |||
| Yes | 0.202 (0.161‐0.254) | <0.001 | ||
| Diabetes | ||||
| No | Ref | |||
| Yes | 0.305 (0.209‐0.445) | <0.001 | ||
| Osteoporosis | ||||
| No | Ref | |||
| Yes | 0.200 (0.156‐0.256) | <0.001 | ||
In the univariate analysis, age, sex, injury cause, fracture sites, and presentation of associated injuries were associated with complications. After univariate analysis, all statistically or clinically significant variables were entered into the multivariable model. A multivariable logistic regression analysis showed that the independent predictors for complications were older age, male, and fracture site, except for the proximal region (Table 4).
TABLE 4.
Univariate and multivariable logistic regression analysis of independent risk factors for complications
| Data | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age | ||||
| OP group | Ref | Ref | ||
| YA group | 1.394 (1.071–1.814) | 0.014 | 0.790 (0.561–1.112) | 0.177 |
| CH group | 0.567 (0.387–0.830) | 0.003 | 0.245 (0.151–0.399) | <0.001 |
| Gender | ||||
| Female | Ref | Ref | ||
| Male | 1.379 (1.091–1.743) | 0.007 | 1.403 (1.082–1.819) | 0.011 |
| Injury season | ||||
| Winter | Ref | |||
| Spring | 0.986 (0.699–1.390) | 0.935 | ||
| Summer | 1.320 (0.954–1.827) | 0.094 | ||
| Autumn | 1.154 (0.828–1.609) | 0.398 | ||
| Injury time of day | ||||
| 18‐24:00 | Ref | |||
| 0‐6:00 | 1.067 (0.650–1.751) | 0.798 | ||
| 6‐12:00 | 0.995 (0.607–1.632) | 0.985 | ||
| 12‐18:00 | 0.905 (0.526–1.560) | 0.720 | ||
| Injury cause | ||||
| Low‐height fall | Ref | Ref | ||
| Road traffic crashes | 1.454 (1.113–1.898) | 0.006 | 1.087 (0.737–1.605) | 0.674 |
| High‐height fall | 0.806 (0.474–1.369) | 0.424 | 0.681 (0.364–1.276) | 0.230 |
| Drifting‐down injury | 1.339 (0.609–2.945) | 0.468 | 0.967 (0.404–2.315) | 0.940 |
| Others | 0.793 (0.275–2.290) | 0.669 | 0.740 (0.243–2.249) | 0.595 |
| Injury location | ||||
| Outdoors | Ref | |||
| Indoors | 0.966 (0.757–1.234) | 0.784 | ||
| Coma after injury | ||||
| No | Ref | |||
| Yes | 1.508 (0.972–2.340) | 0.067 | ||
| Fracture side | ||||
| Both side | Ref | |||
| Right side | 0.960 (0.360–2.559) | 0.934 | ||
| Left side | 0.908 (0.340–2.422) | 0.847 | ||
| Fracture site | ||||
| Proximal region | Ref | Ref | ||
| Shaft | 1.621 (1.248–2.105) | <0.001 | 2.556 (1.811–3.606) | <0.001 |
| Distal region | 1.647 (1.069–2.536) | 0.024 | 1.771 (1.105–2.839) | 0.018 |
| Multiple sites | 2.964 (1.182–7.437) | 0.021 | 3.357 (1.273–8.848) | 0.014 |
| Heart/brain/lung | ||||
| No | Ref | |||
| Yes | 1.047 (0.829–1.322) | 0.703 | ||
| Diabetes | ||||
| No | Ref | |||
| Yes | 1.059 (0.757–1.481) | 0.739 | ||
| Osteoporosis | ||||
| No | Ref | |||
| Yes | 0.893 (0.702–1.137) | 0.360 | ||
| Associated injuries | ||||
| No | Ref | Ref | ||
| Yes | 1.527 (1.194–1.953) | 0.001 | 1.232 (0.881–1.722) | 0.223 |
Discussion
In the current study, we have shown that traumatic femoral fractures are mostly the result of low‐energy trauma and predominantly affect the proximal site of the femur among older people. A higher rate of shaft fractures, fractures occurring outdoors, and associated injuries was observed among young adults and children than among older people. This study demonstrates the age‐specific clinical characteristics of traumatic femoral fractures and reveals a significant relationship among different ages and associated injuries, complications.
Age Differences of General Characteristics, Associated Injuries, and Complications
To the best of our knowledge, no studies have systematically assessed the differences in traumatic femoral fractures among young adults, children, and elderly people. 5 , 15 Age‐related bone loss occurs in both men and women, 16 , 17 , 18 although women have more bone loss than men. 19 In the present study, 47 patients (9.7%) in the YA group and a total of 734 patients (61.5%) in the OP group were diagnosed with osteoporosis. Older women are more likely to have a traumatic femoral fracture, mainly due to accidental falls from low heights (50.8%). The mechanism of hip fractures involves more factors other than the simple loss of bone mass with age. Equally important, and perhaps even more so with increasing age, is the tendency to fall and to fall in a different way. 15 , 20 Visual acuity, hypofunction of the nervous and motor systems, and a loss of coordination increase the occurrence of spinal fractures, 21 , 22 which are also important causes of femoral fractures in older people.
The most common injury causes were road traffic crashes (41.4%) in the YA group, road traffic crashes (46.8%) in the CH group, and low‐height falls (90.5%) in the OP group. Our results also show a male predominance in the YA group and CH group, which is probably associated with a higher likelihood of being engaged in higher risk labor and RTCs. Children not only fall when climbing play equipment and furniture but also mostly fall because of slipping or physical activity. With increasing age, the most common injury mechanism shifted from falls to traffic accidents. Patients in the OP group were predominately female, which is probably associated with a higher likelihood of suffering from femoral fractures because of osteoporosis and low‐energy trauma. Therefore, it is necessary to help prevent older people from experiencing osteoporosis and falling and to prevent young adults and children from experiencing RTCs to reduce the increasing occurrence and burden of these age‐related fractures.
In addition, there seem to be some seasonal variations in the occurrence of femoral fracture. Traumatic femoral fractures most frequently occurred in autumn for young adults and summer for children. The results are consistent with those of previous studies. 23 , 24 , 25 Traumatic femoral fractures usually occur outdoors from 12–6 p.m. among young adults and children. Reasons for this variation are unclear and will require further study. We speculate that children are more likely to be playing outside during warm weather months, with an increased incidence during summer. Traffic accidents increased during the summer and autumn months. In a study of nonspecific traffic injuries in urban children, it was reported that the peak incidence of pedestrian and bicyclist injuries occurred during summer months, whereas motor vehicle occupant injuries showed little seasonal variation. 26 Based on these results, there is a need for greater attention to motor vehicle safety in adolescents. We should increase the education of parents and children regarding falls, bicycle and pedestrian safety in children, and enforce drivers' licenses for adolescent drivers. 27 , 28 , 29 Making behaviors, roads, and vehicles safer can significantly reduce RTC‐related traumatic femoral fractures among children and young adults.
Traumatic femoral fractures most frequently occur in winter and occur indoors from 6 a.m.–12 p.m. for elderly adults. Reasons for this variation remain uncertain, and possible hypotheses have been shown as follows 30 , 31 , 32 , 33 , 34 : winters are darker and colder, 31 slipping on ice and snow, 32 and fractures occur in indoor environments. 33 , 34 Hypothermia among older people with undernutrition could lead to impairment of judgments and coordination and then lead to injury. 33 Hindrances of free movements and increased clumsiness of older people with many layers of clothes on leads to falls. 34 Therefore, modifying the environment to decrease the chance of tripping or slipping and providing more education for older people on home safety as well as fall avoidance may reduce the incidence of femoral fractures among older people. 21 , 22
The OP group (88.9%) and YA group (50.6%) had the highest frequency of proximal fractures, while the CH group (75.7%) had the highest frequency of shaft fractures. There were significant differences among the three groups in the distribution of cases by fracture site. Similarly, in previous studies, femoral shaft fractures were found to be the most commonly diagnosed femoral fractures in a pediatric population, 28 , 35 , 36 , 37 approximately 90% of femur fractures occur in the proximal femur in adults, 38 and older patients were found to be at a higher risk of developing proximal fractures. 4 , 5 , 6 Potential factors that may explain the difference in femur fracture patterns in pediatric patients compared to adult femur fractures are osteoporosis and a different manner of falling, including an increased risk of falling due to medication or impaired balance. 39 Therefore, we should pay much more attention to the medical research and development, diagnosis, and treatment of femoral shaft fractures among the pediatric population, proximal femur fractures among young adults, and proximal femur fractures among older people.
The incidence of associated injuries in our cohort was within the range of 25.3–68.3% reported previously. 36 , 37 , 40 The YA group (56.2%) had a significantly higher frequency of associated injuries than the OP group (14.2%). A total of 135 patients in the CH group (39.5%) presented with associated injuries. The YA group had a significantly higher percentage of patients with surgery‐related complications than the OP group. The OP group had a higher frequency of non‐surgery‐related complications than the YA group and CH group. The most common non‐surgery‐related complications were pneumonia (7.1%) and deep venous thrombosis (6.5%) in the OP group and deep venous thrombosis (6.4%) and pneumonia (4.8%) in the YA group. The most common subsequent comorbidities were pneumonia and new upper‐limb fractures in younger adults and pneumonia in the elderly.
Risk Factors for Associated Injuries and Complications
A multivariable logistic regression analysis showed that the independent predictors for associated injuries were young adults, high‐energy injury, outdoors, coma after injury, and fracture sites except for the proximal region. The most common fracture‐associated injuries were fractures involving the leg and foot in the YA group; upper limb fractures, fractures of the ribs and vertebrae in the OP group; and fractures involving the leg and foot, upper limb fractures, and skull and facial fractures in the CH group. Patients with femoral fractures have a higher incidence of organ damage and an increased incidence of upper and lower limb fractures. 40 , 41 Thus, in children and young adults with femoral fractures resulting from a high‐energy trauma, it is strongly recommended to carefully check the head, leg, and foot and intrathoracic and craniocerebral injuries since the rapid detection and adequate treatment of severe injuries associated with these areas improves patient outcome and reduces mortality. In older people with femoral fractures, it is strongly recommended to carefully check the ribs and vertebrae to avoid misdiagnosis. It is helpful for us to provide early, timely diagnosis and treatment of associated injuries for patients with traumatic femoral fractures.
A multivariable logistic regression analysis showed that the independent predictors for complications were older age, male sex, and fracture sites except for the proximal region. Hip fractures are high‐energy blunt injuries, and most elderly patients sustaining hip fractures are at high risk for associated thrombosis, which strongly influences their outcome after fractures. 42 Respiratory complications contributed greatly to mortality in elderly patients with femoral fracture after a fall from ground level. Thus, aggressive chest‐protective measures are encouraged to decrease the respiratory complications associated with femoral fracture in elderly patients. 6
Limitations
The study has some limitations that need to be acknowledged. First, the retrospective design of the study may have led to selection bias. Second, the lack of information about bone mineral density (BMD), serum calcium and vitamin D levels, body mass index (BMI), and the patients' medical history are important limitations of this study. Third, the patients came from a regional tertiary hospital, but the General Hospital of Northern Theater Command is one of the largest tertiary hospitals located in the center of Shenyang, the large number of outpatients and emergency patients were included in our study. Fourth, the patients had been divided into juveniles (under 18 years old), young adults (aged 18–60 years), and seniors (aged 60 years and over), the age span of young adults (aged 18–60 years) was large which may lead to undetailed research results, more detailed age groups will be defined in future studies. Despite these limitations, we believe that this valuable information about age differences of traumatic femoral fractures and risk factors for associated injuries and complications can be used as guidance for the prevention, diagnosis, and treatment of traumatic femoral fractures in children, young adults, and older people, and provide reference for future high‐level multicenter study.
Conclusions
In conclusion, in this study, traumatic femoral fractures were mostly the result of low‐energy trauma and predominantly affected the proximal region of the femur among older people. A higher rate of shaft fractures, fractures occurring outdoors, and associated injuries was observed among young adults and children than among older people. Multivariable logistic regression showed that young adults, high‐energy injury, outdoors, coma after injury, and fracture sites except for the proximal region were independent risk factors for associated injuries. Older age, male, and fracture site except for the proximal region were independent risk factors for complications. Understanding the age differences in traumatic femoral fractures is important for the allocation of public resources, the development of preventative strategies, and efficient diagnosis and treatment.
Ethical Approval
The study protocol and this manuscript were approved by the ethics committee and the institutional review board of our institution, and the study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Author Contributions
Hong Yuan, Hailong Yu, Yunpeng Zhu: Conceptualization, Methodology, Software, Data curation, Writing—Original draft preparation. Liangbi Xiang: Formal analysis, Software, Validation, Writing—Original draft preparation. Hongwei Wang: Conceptualization, Methodology, Software, Supervision, Writing—Reviewing and Editing.
Acknowledgements
This work was supported by the Liaoning Provincial Natural Science Foundation of China (2019‐ZD‐1063) and the Shenyang Science and Technology Project (21‐173‐9‐70).
Hong Yuan, Hailong Yu, and Yunpeng Zhu contributed equally to this work.
Disclosure: All listed authors have made substantial contributions to the manuscript and do not have any conflicts of interest.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request
References
- 1. Hadji P, Hardtstock F, Wilke T, et al. Estimated epidemiology of osteoporosis diagnoses and osteoporosis‐related high fracture risk in Germany: a German claims data analysis. Arch Osteoporos. 2020;15(1):127. [DOI] [PubMed] [Google Scholar]
- 2. Iihara N, Ohara E, Bando Y, Yoshida T, Ohara M, Kirino Y. Fragility fractures in older people in Japan based on the National Health Insurance Claims Database. Biol Pharm Bull. 2019;42(5):778–85. [DOI] [PubMed] [Google Scholar]
- 3. Bouyer B, Leroy F, Rudant J, Weill A, Coste J. Burden of fractures in France: incidence and severity by age, gender, and site in 2016. Int Orthop. 2020;44(5):947–55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Nieves JW, Bilezikian JP, Lane JM, et al. Fragility fractures of the hip and femur: incidence and patient characteristics. Osteoporos Int. 2010;21(3):399–408. [DOI] [PubMed] [Google Scholar]
- 5. Wu SC, Rau CS, Kuo SCH, Chien PC, Hsieh CH. The influence of ageing on the incidence and site of trauma femoral fractures: a cross‐sectional analysis. BMC Musculoskelet Disord. 2019;20(1):413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Chou SE, Rau CS, Tsai YC, Hsu SY, Hsieh HY, Hsieh CH. Risk factors and complications contributing to mortality in elderly patients with fall‐induced femoral fracture: a cross‐sectional analysis based on trauma registry data of 2,407 patients. Int J Surg. 2019;66:48–52. [DOI] [PubMed] [Google Scholar]
- 7. Lundin N, Huttunen TT, Enocson A, Marcano AI, Felländer‐Tsai L, Berg HE. Epidemiology and mortality of pelvic and femur fractures‐a nationwide register study of 417,840 fractures in Sweden across 16 years: diverging trends for potentially lethal fractures. Acta Orthop. 2021;92(3):323–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Elsoe R, Ceccotti AA, Larsen P. Population‐based epidemiology and incidence of distal femur fractures. Int Orthop. 2018;42(1):191–6. [DOI] [PubMed] [Google Scholar]
- 9. Larsen P, Ceccotti AA, Elsoe R. High mortality following distal femur fractures: a cohort study including three hundred and two distal femur fractures. Int Orthop. 2020;44(1):173–7. [DOI] [PubMed] [Google Scholar]
- 10. Dragomir‐Daescu D, Rossman TL, Rezaei A, et al. Factors associated with proximal femur fracture determined in a large cadaveric cohort. Bone. 2018;116:196–202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Byrne JP, Nathens AB, Gomez D, Pincus D, Jenkinson RJ. Timing of femoral shaft fracture fixation following major trauma: a retrospective cohort study of United States trauma centers. PLoS Med. 2017;14(7):e1002336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Chang MW, Liu HT, Huang CY, Chien PC, Hsieh HY, Hsieh CH. Location of femoral fractures in patients with different weight classes in fall and motorcycle accidents: a retrospective cross‐sectional analysis. Int J Environ Res Public Health. 2018;15(6):1082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Rau CS, Lin TS, Wu SC, Yang JC, Hsu SY, Cho TY, et al. Geriatric hospitalizations in fall‐related injuries. Scand J Trauma Resusc Emerg Med. 2014;22:63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Hsieh CH, Hsu SY, Hsieh HY, Chen YC. Differences between the sexes in motorcycle‐related injuries and fatalities at a Taiwanese level I trauma center. Biom J. 2017;40(2):113–20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Tanner DA, Kloseck M, Crilly RG, Chesworth B, Gilliland J. Hip fracture types in men and women change differently with age. BMC Geriatr. 2010;10:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Rao SS, Budhwar N, Ashfaque A. Osteoporosis in men. Am Fam Physician. 2010;82(5):503–8. [PubMed] [Google Scholar]
- 17. Kanis JA, Bianchi G, Bilezikian JP, et al. Towards a diagnostic and therapeutic consensus in male osteoporosis. Osteoporos Int. 2011;22(11):2789–98. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Frost M, Wraae K, Abrahamsen B, et al. Osteoporosis and vertebral fractures in men aged 60‐74 years. Age Ageing. 2012;41(2):171–7. [DOI] [PubMed] [Google Scholar]
- 19. Sigurdsson G, Aspelund T, Chang M, et al. Increasing sex difference in bone strength in old age: the age, gene/environment susceptibility‐Reykjavik study (AGES‐REYKJAVIK). Bone. 2006;39(3):644–51. [DOI] [PubMed] [Google Scholar]
- 20. Talbot LA, Musiol RJ, Witham EK, Metter EJ. Falls in young, middle‐aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health. 2005;5:86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Wang H, Li C, Xiang Q, Xiong H, Zhou Y. Epidemiology of spinal fractures among the elderly in Chongqing, China. Injury. 2012;43(12):2109–16. [DOI] [PubMed] [Google Scholar]
- 22. Wang H, Xiang L, Liu J, Zhou Y, Ou L. Gender differences in the clinical characteristics of traumatic spinal fractures among the elderly. Arch Gerontol Geriatr. 2014;59(3):657–64. [DOI] [PubMed] [Google Scholar]
- 23. Crawford JR, Parker MJ. Seasonal variation of proximal femoral fractures in the United Kingdom. Injury. 2003;34(3):223–5. [DOI] [PubMed] [Google Scholar]
- 24. Chesser TJ, Howlett I, Ward AJ, Pounsford JC. The influence of outside temperature and season on the incidence of hip fractures in patients over the age of 65. Age Ageing. 2002;31(5):343–8. [DOI] [PubMed] [Google Scholar]
- 25. Pueyo‐Sánchez MJ, Larrosa M, Suris X, et al. Secular trend in the incidence of hip fracture in Catalonia, Spain, 2003‐2014. Age Ageing. 2017;46(2):324–8. [DOI] [PubMed] [Google Scholar]
- 26. Durkin MS, Laraque D, Lubman I, Barlow B. Epidemiology and prevention of traffic injuries to urban children and adolescents. Pediatrics. 1999;103(6):e74. [DOI] [PubMed] [Google Scholar]
- 27. Cvijanovich NZ, Cook LJ, Mann NC, Dean JM. A population‐based study of crashes involving 16‐ and 17‐year‐old drivers: the potential benefit of graduated driver licensing restrictions. Pediatrics. 2001;107(4):632–7. [DOI] [PubMed] [Google Scholar]
- 28. Loder RT, O'Donnell PW, Feinberg JR. Epidemiology and mechanisms of femur fractures in children. J Pediatr Orthop. 2006;26(5):561–6. [DOI] [PubMed] [Google Scholar]
- 29. Wang H, Zhou Y, Liu J, et al. Traumatic fractures as a result of motor vehicle collisions in children and adolescents. Int Orthop. 2018;42(3):625–30. [DOI] [PubMed] [Google Scholar]
- 30. Souza MM, Souza EM, Nunes AA, Martinez EZ. Seasonal variation of femoral fractures in the state of São Paulo, Southeast Brazil. Rev Saude Publica. 2019;53:55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Douglas S, Bunyan A, Chiu KH, Twaddle B, Maffulli N. Seasonal variation of hip fracture at three latitudes. Injury. 2000;31(1):11–9. [DOI] [PubMed] [Google Scholar]
- 32. Al‐Azzani W, Adam Maliq Mak D, Hodgson P, Williams R. Epidemic of fractures during a period of snow and ice: has anything changed 33 years on? BMJ Open. 2016;6(9):e010582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33. Bastow MD, Rawlings J, Allison SP. Undernutrition, hypothermia, and injury in elderly women with fractured femur: an injury response to altered metabolism? Lancet. 1983;1(8317):143–6. [DOI] [PubMed] [Google Scholar]
- 34. Johnson NA, Stirling E, Alexander M, Dias JJ. The relationship between temperature and hip and wrist fracture incidence. Ann R Coll Surg Engl. 2020;102(5):348–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Engström Z, Wolf O, Hailer YD. Epidemiology of pediatric femur fractures in children: the Swedish fracture register. BMC Musculoskelet Disord. 2020;21(1):796. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Valaikaite R, Tabard‐Fougère A, Steiger C, Samara E, Dayer R, Ceroni D. A retrospective epidemiological study of paediatric femoral fractures. Swiss Med Wkly. 2020;150:w20360. [DOI] [PubMed] [Google Scholar]
- 37. Rewers A, Hedegaard H, Lezotte D, et al. Childhood femur fractures, associated injuries, and sociodemographic risk factors: a population‐based study. Pediatrics. 2005;115(5):e543–52. [DOI] [PubMed] [Google Scholar]
- 38. Court‐Brown CM, Caesar B. Epidemiology of adult fractures: a review. Injury. 2006;37(8):691–7. [DOI] [PubMed] [Google Scholar]
- 39. Marks R, Allegrante JP, Ronald MacKenzie C, Lane JM. Hip fractures among the elderly: causes, consequences and control. Ageing Res Rev. 2003;2(1):57–93. [DOI] [PubMed] [Google Scholar]
- 40. Anyaehie UE, Ejimofor OC, Akpuaka FC, Nwadinigwe CU. Pattern of femoral fractures and associated injuries in a Nigerian tertiary trauma Centre. Niger J Clin Pract. 2015;18(4):462–6. [DOI] [PubMed] [Google Scholar]
- 41. Adili A, Bhandari M, Lachowski RJ, Kwok DC, Dunlop RB. Organ injuries associated with femoral fractures: implications for severity of injury in motor vehicle collisions. J Trauma. 1999;46(3):386–91. [DOI] [PubMed] [Google Scholar]
- 42. Lin KB, Yang NP, Lee YH, et al. The incidence and factors of hip fractures and subsequent morbidity in Taiwan: an 11‐year population‐based cohort study. PLoS One. 2018;13(2):e0192388. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request