

Abstract
Background:
Previous research has shown an excess risk of COVID-19 among several occupations, but data on public transport workers are scarce. To investigate the occupational risk posed by contact with the public, we followed up the incidence of COVID-19 in a cohort of public transport workers.
Methods:
We identified the incident cases of COVID-19 between 1 September 2020 - 6 May 2021 in a cohort of 2,052 employees of a public transport agency in Sardinia, Italy. The diagnosis of COVID-19 was based on a positive molecular test. To calculate the expected events, we applied the age- and gender-specific incidence rates in the regional population at the same time frame to the correspondent strata of the study cohort. We estimated the age- and gender-adjusted relative risk (RR) of COVID-19 as the ratio between the observed and the expected events and its 95% confidence interval (95% C.I.) among the total cohort and in two sub-cohorts: bus drivers and the rest of the personnel (administrative staff, train and metro drivers, workers in the mechanical shop, and in the railroad maintenance, and security).
Results:
Bus drivers run an elevated risk of COVID-19 (RR = 1.4, 95% C.I. 1.07 - 1.79). There was no excess risk among the rest of the personnel.
Conclusions:
Our study suggests an excess risk of COVID-19 among bus drivers even in a relatively low incidence area, which could imply inadequacy of the preventive measures put in place. Additional studies of larger size with detailed information on personal and lifestyle characteristics are warranted.
Keywords: COVID-19, occupation, occupational disease, bus drivers, cohort study
1. Introduction
On 18 May 2022, the EU Advisory Committee for Safety and Health at Work adopted a recommendation on COVID-19 as an occupational disease for healthcare workers, workers in nursery homes, and in-home care [1]. However, several other essential occupations, including drivers and transport workers, touristic guides, services and sales workers, and cleaners also run an elevated risk [2]. While the evidence of an excess risk among healthcare workers is well consolidated, results have been scarce and contradictory in the public transport sector [3]. The contact with the public in these occupations was assumed to be responsible, because of implying a higher probability of transmission of the infection. Indeed, one of the first COVID-19 cases in Taiwan was a taxi driver who carried onboard a passenger arriving from continental China [2], and the risk was elevated in the large UK Office of National Statistics COVID-19 Infection survey [4].
Between March and May 2020, there were 4,761 COVID-19 deaths among the population of working age (between 20 and 64 years) in England and Wales. The analysis of their occupations identified 17 jobs with COVID-19 mortality rates above the expectation, particularly in males, including taxi drivers (65.3 deaths per 100,000) and bus drivers (44.2 deaths per 100,000) [5]. Another study reported that COVID-19 mortality was three times higher among Transport for London (TfL) drivers in respect to the rest of the occupations during the first epidemic wave between March and May 2020 [6].
To assess the occupational COVID-19 burden in the transport sector we explored the association between the occupations in a public transport agency covering urban and extra-urban routes and the risk of SARS-CoV-2 infection in Sardinia, a region of Italy that was less severely hit during the 2020 first epidemic wave [7].
2. Methods
With the collaboration of the management and the occupational health and safety department of a major agency of public transport in the region of Sardinia, Italy, we obtained anonymized aggregated data of the employees as of 1 September 2020. The cohort included 2,052 subjects, 1,893 men (1,161 bus drivers) and 159 women (24 bus drivers). The data set included the number of incident COVID-19 cases in each age and gender category, diagnosed among the cohort members from 1 September 2020 through 6 May 2021. We divided the cohort into two sub-cohorts: bus drivers and other jobs, including indoor (administrative offices, ticket hall, mechanical shop, traffic control room, train and metro drivers, and ticket clerks) and outdoor activities (workers engaged in railway maintenance or surveillance). The rest of the travelling personnel and metro drivers were very few and with much less opportunity of being in close contact with the public. Therefore, we combined them with the rest of the other jobs. We first plotted the number of incident cases in the two sub-cohorts by week of follow-up and compared the univariate regression curves. Then, we calculated the expected events for each category of age (10 years) and gender in each sub-cohort and in the total cohort based on the incidence in the general regional population observed along the same period of follow-up of the study cohort, estimated by applying the proportion of cases in each 10-year age and gender category over the total case observed nationwide [8] to the total number of cases observed at the regional level, which was the only available information. We used the following formula:
![]()
where E is the total expected events ni is the cohort size in the i age and gender subgroup; and ii is the incidence in the corresponding age and gender subgroup of the reference population.
We calculated the relative risk (RR) of COVID-19 with indirect standardization, as the ratio between the observed events (O) and the sum of the expected (E) in each age and gender subgroup. The chance probability associated with the O/E ratio was calculated with the Pearson’s x2 test:

The 95% C.I. confidence interval of the RR has been calculated according to Miettinen [9].

Ethical review and approval were waived for this study, due to the use of a database with data aggregated by age (10-year age-groups) and gender categories. Informed consent was not required as cohort members were unidentifiable.
3. Results
Table 1 shows the cohort size and the number of COVID-19 cases observed and expected by age, occupation, and gender. The incidence of COVID-19 was almost three-times higher among male bus drivers than the rest of the male sub-cohort (p<0.01), but there was no difference between the small female sub-cohorts. The excess cases concentrated among male bus drivers in the 40-49 age group (32 observed vs 13.11 expected). The average days of sick leave were 26.4 (standard deviation [sd] 19.8) and 24 (sd 6.7) among bus drivers and the other jobs sub-cohort, respectively, suggesting no substantial difference between the two groups (p=0.66). Figure 1 plots the number of weekly cases by sub-cohort along the 34 weeks of follow-up. In both sub-cohorts, a polynomial regression of 5th grade best depicts the evolution of the COVID-19 epidemic in this time course. The two curves are parallel, with that representing the bus drivers’ sub-cohort permanently uplifted in respect to the other jobs sub-cohort. As the vast majority of cases in the general population occurred above age 65, we judged that the crude number of events, the only available daily incidence information, was not comparable with that of the public transport cohort.
Table 1.
Size, observed and expected events, and cumulative incidence of COVID-19 by age and gender subgroups in the total cohort and sub-cohorts.
| Age and gender subgroups | Cohort size | Incidence rate per 1,000 | Observed/expected | Cohort size | Incidence rate per 1,000 | Observed/expected | Cohort size | Incidence rate per 1,000 | Observed/expected |
|---|---|---|---|---|---|---|---|---|---|
| Total cohort | Bus drivers | Other jobs | |||||||
| 20-29 males | 8 | 0.0 | 0/0.28 | 1 | 0.0 | 0/0.03 | 7 | 0.0 | 0/0.24 |
| 20-29 females | 2 | 0.0 | 0/0.07 | 0 | 0.0 | 0/0.0 | 2 | 0.0 | 0/0.07 |
| 30-39 males | 192 | 15.6 | 3/5.20 | 144 | 20.8 | 3/3.90 | 48 | 0.0 | 0/1.30 |
| 30-39 females | 7 | 0.0 | 0/0.20 | 1 | 0.0 | 0/0.03 | 6 | 0.0 | 0/0.18 |
| 40-49 males | 527 | 66.4 | 35/16.52 | 418 | 76.6 | 32/13.11 | 109 | 27.5 | 3/3.42 |
| 40-49 females | 36 | 27.8 | 1/1.22 | 10 | 0.0 | 0/0.29 | 26 | 0.0 | 1/0.88 |
| 50-59 males | 826 | 30.3 | 25/33.01 | 505 | 37.6 | 19/20.18 | 321 | 18.7 | 6/12.83 |
| 50-59 females | 80 | 12.5 | 1/3.20 | 12 | 83.3 | 1/0.42 | 68 | 0.0 | 0/2.72 |
| 60-69 males | 340 | 17.6 | 6/11.05 | 119 | 25.2 | 3/3.87 | 221 | 13.6 | 3/7.18 |
| 60-69 females | 34 | 29.4 | 1/0.96 | 1 | 0.0 | 0/0.02 | 33 | 30.3 | 1/0.93 |
| Total males 95% C.I. |
1,893 | 19.8 (13.6 - 26.1) |
69/66.06 | 1,187 | 24.3 (15.5 - 33.0) |
57/41.09 | 706 | 8.9 (2.0 - 15.8) |
12/24.97 |
| Total females1 | 159 | 9.9 | 3/5.66 | 24 | 12.0 | 1/0.76 | 135 | 9.9 | 2/4.78 |
1The 95% C.I. of the incidence rate in the female cohort and sub-cohorts has not been calculated because the number of events was <10.
Figure 1.
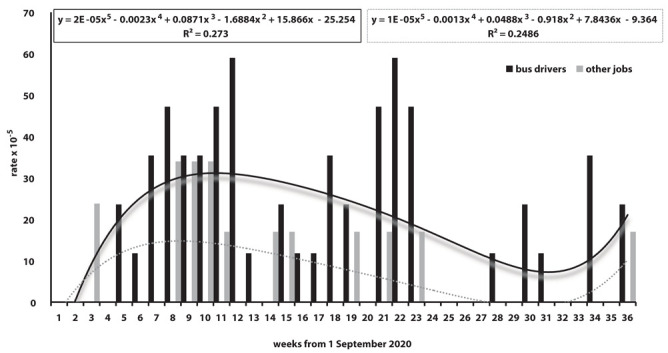
Covid-19 weekly rate by study sub-cohort along the 34 weeks of follow-up between 1 September 2020 and 6 May 2021.
The results of the follow-up (Table 2) showed no excess risk of COVID-19 among the total cohort (RR = 1.0, 95% C.I. 0.80 - 1.26), with a decrease in the small female sub-cohort of uncertain relevance (RR = 0.5, 95% C.I. 0.17 - 1.61). However, females were mainly employed as administrative clerks and accounted for a mere 8% of the total cohort. The risk was highest among bus drivers (RR = 1.4, 95% C.I. 1.07 - 1.79). The jobs other than bus drivers sub-cohort showed an inverse association with the risk of COVID-19 (RR = 0.5, 95% C.I. 0.28 - 0.78). The results did not substantially change when using the age- and gender-specific COVID-19 rates in the Italian population.
Table 2.
Age-adjusted relative risk of COVID-19 in the total cohort, bus drivers, and jobs other than bus drivers by gender and adjusted by age and gender over the total cohort.
| Total cohort | Bus drivers | Other jobs | |
|---|---|---|---|
| Cohort size | |||
| Males | 1,893 | 1,187 | 706 |
| Females | 159 | 24 | 135 |
| Total | 2,052 | 1,211 | 841 |
| Observed events | |||
| Males | 69 | 57 | 12 |
| Females | 3 | 1 | 2 |
| Total | 72 | 58 | 14 |
| Relative risk (95% C.I.) | |||
| Males | 1.0 (0.82 - 1.32) | 1.4 (1.07 - 1.80) | 0.5 (0.28 - 0.84) |
| Females | 0.5 (0.17 - 1.61) | 1.3 (0.19 - 9.27) | 0.4 (0.11 - 1.60) |
| Total | 1.0 (0.80 - 1.26) | 1.4 (1.07 - 1.79) | 0.5 (0.28 - 0.78) |
4. Discussion
Our results suggest a 40% increased probability of SARS-CoV-2 infection in the occupation of bus driver of urban and extra-urban routes in an Italian region with a relatively low incidence during the first COVID-19 wave. Risk was highest among male bus drivers aged 40-49 (RR = 2.4, 95% C.I. 1.97 - 3.02), possibly reflecting non occupational and social factors, including less cautionary health protection attitudes. Consistently, the fraction of complete adherence to the COVID-19 vaccination protocols among the Italian population was lower below age 50 than above that age [10]. Other jobs in the same public transport agency did not convey an excess risk. A personal contact between bus drivers and passengers, closer than other travelling staff, results from the driving cabin location within the same indoor environment with the passenger seats. Instead, several coaches compose trains and metro area convoys, where the driving cabin is in a locomotive or a separated driving area not accessible to the public. Another peculiar condition of bus drivers is being multitasking, as they must control the access to the coach. Instead, in the metro convoys the tickets are checked automatically and, in the train, this is the duty of the ticket clerks, whose contact with the public is limited to the short time required for checking or issuing the tickets. Other studies suggested that the pollution of the urban environment with traffic exhausts might have contributed to impairing the respiratory system defences and increasing the risk of SARS-COV-2 infection in the major urban areas [2, 11-17]. Bus drivers, taxi drivers, and traffic police would be mostly exposed. Other reports have consistently shown that public transport drivers run a higher risk of airborne transmissible diseases, and particularly COVID-19, in respect to the general population and to subjects engaged in other jobs in the same workplaces [2, 6, 18]. The association seems somewhat weaker in our study. Besides chance, plausible explanations would be the relatively low incidence of COVID-19 in the study area while recording the COVID-19 cases compared to the studies conducted elsewhere. Besides, the incidence of COVID-19 started to be surveyed on 1 September 2020, well after the end of the first epidemic wave in May 2020, and just at the beginning of the second 2020 epidemic wave, established at the end of September 2020 by the joint working group of the Italian National Institute of Statistics (ISTAT) and the National Institute of Health (Istituto Superiore di Sanità, ISS) [19]. Public transport was considered as an essential occupation, and it was never suspended even during the March-May 2020 lockdown in Italy. At that time, preventive measures for public transports were already in place, personal protective equipment was abundantly available, and restrictions on the number of passengers were in place. Further restrictions were introduced between 8 October and 3 November 2020, including a nationwide night-time curfew, prohibition of social events and mass gatherings, and the mandatory outdoor use of facial masks [7]. Therefore, during the survey period, the probability of contagion might have been substantially smaller than the previous months, which might have contributed to decrease the number of incident cases and the power of our study.
Limitations in our study include the small cohort size and the small number of female bus drivers, which did not allow to explore gender-related differences in the risk of COVID-19, or by occupations posing lesser risk from contact with the public. Also, we did not have access to additional informations, such as smoking habit, body mass index, or previous clinical conditions that might have been predisposing or susceptibility factors. However, being a public transport driver poses the responsibility of the public safety. For this reason, in Italy, the health conditions of public transport workers undergo a double check, by the occupational physician under a regular schedule and following any prolonged sick leave, and by a second, specially appointed occupational physician at specific ages with a 10-year interval below age 40 and by a 5-year-interval afterwards [20]. Therefore, the health conditions conferring greater susceptibility to COVID-19 would likely be rarer among public transport workers than the general population, and the risk of COVID-19 in our cohort underestimated due to the healthy worker effect.
Lessons from the COVID-19 epidemic are that public mass gatherings and crowding pose a serious hazard of transmission of aerial infections and that preventive measures taken at the workplace were not enough to protect bus drivers, who still run a 40% increase in risk of COVID-19. Therefore, upgrading the safety level of public transport drivers would be necessary. First, as it already happens in other countries, the driver seat should be completely isolated from the rest of the coach and with a separate air flow to further reducing the exposure to the salivary droplets, vectors of SARS-CoV-2 as well as other aerial pathogens. Buses should be equipped with temperature scanners along with those for credit cards, passes, and tickets to prevent people with transmissible diseases from entering the coach, and to exempt drivers from the manual control and stamp of the tickets. The use of adequate personal protective equipment inside the coach, especially high-level filtering facial masks, should be maintained. Also, to prevent overcrowding in the rush hours, the number, frequency, and size of the coaches should be flexible.
5. Conclusion
Our follow-up study of a cohort of public transport workers showed that bus drivers run an excess risk of COVID-19 even in a relatively low incidence area and despite the precautionary action taken. Our results support the existing evidence on the occupational nature of COVID-19 among bus drivers.
Acknowledgments:
The authors acknowledge the contribution of the management, the employees, the occupational physicians, and the occupational health and safety department of the Sardinian Agency for Public Transport.
Appendix
Supplemental Figure 1:
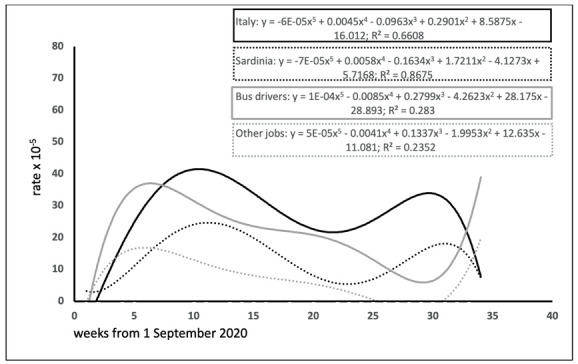
Time trend of the COVID-19 crude rate between 1 September 2020 and 6 May 2021 in Italy (black solid line), Sardinia (black dotted line), bus drivers (grey solid line) and other employees of the transport agency (grey dotted line).
Institutional Review Board Statement:
Ethical review and approval were waived for this study, due to the use of a database with data aggregated by age (10-year age-groups) and gender categories.
Declaration of Interest:
At the time of conducting this study, dr. Ilaria Pilia was the leading occupational physician of the Sardinian Agency for Public Transport. The Agency had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
References
- 1.The Advisory Committee on Safety and Health at Work. Opinion: Update of Commission Recommendation 2003/670/EC concerning the European schedule of occupational disease to include COVID-19. Adopted 18.05.2022. Brussels, Belgium: The European Commission, DG Employment, Social Affairs and Inclusion Working Conditions and Social Dialogue, Health and Safety at Work, EU OSHA. 2022 Available online at: https://ec.europa.eu/ commission/presscorner/detail/en/ip_22_3117 (last accessed 9 July 2022) [Google Scholar]
- 2.Lan FY, Wei CF, Hsu YT, et al. Work-related COVID-19 transmission in six Asian countries/areas: A follow-up study. PLoS One. 2020;15:e0233588. doi: 10.1371/journal.pone.0233588. Doi: 10.1371/journal.pone.0233588. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.De Matteis S. COVID-19: are not all workers ‘essential’? Occup Environ Med. 2021;78(5):305–306. doi: 10.1136/oemed-2020-107272. Doi: 10. 1136/oemed-2020-107272. [DOI] [PubMed] [Google Scholar]
- 4.Rhodes S, Wilkinson J, Pearce N, et al. Occupational differences in SARS-CoV-2 infection: analysis of the UK ONS COVID-19 infection survey. J Epidemiol Community Health. 2022 doi: 10.1136/jech-2022-219101. jech-2022-219101. Doi: 10.1136/jech-2022-219101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Office for National Statistics. Coronavirus (COVID-19) Related Deaths by Occupation, England and Wales Statistical Bulletins. Available online at: https://www.ons.gov.uk/peoplepopulationandcommunty/ healthandsocialcare/causesofdeath/bulletins/coronaviruscovid19relateddeathsbyoccupationenglandandwales/previousReleases. (Last Accessed: 16 June 2021) [Google Scholar]
- 6.Mutambudzi M, Niedwiedz C, Macdonald EB, et al. Occupation and risk of severe COVID-19: prospective cohort study of 120 075 UK Biobank participants. Occup Environ Med. 2020;78(5):307–314. doi: 10.1136/oemed-2020-106731. Doi: 10.1136/oemed-2020-106731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cocco P, De Matteis S. The determinants of the changing speed of spread of COVID-19 across Italy. Epidemiol Infect. 2022:1–26. doi: 10.1017/S095026882200084X. Doi: 10.1017/S095026882200084X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Presidenza del Consiglio dei Ministri. Dipartimento della Protezione Civile. COVID-19 Italian Situation. Available online at: https://opendatadpc.maps.arcgis.com/apps/dashboards/b0c68bce2cce478eaac82fe. 38d4138b1 [In Italian] (Last Accessed: 23 July 2022) [Google Scholar]
- 9.Miettinen O. Estimability and estimation in case referent studies. Am J Epidemiol. 1976;103(2):226–235. doi: 10.1093/oxfordjournals.aje.a112220. Doi: 10.1093/aje/kwx074. [DOI] [PubMed] [Google Scholar]
- 10.Italian COVID-19 Vaccine Campaign Unit. Anti-COVID-19 vaccination report. Available online at: https://www.governo.it/it/cscovid19/report-vaccini/ [In Italian] (Last Accessed: 4 August 2022) [Google Scholar]
- 11.Ogen Y. Assessing nitrogen dioxide (NO2) levels as a contributing factor to coronavirus (COVID-19) fatality. Sci Total Environ. 2020;726:138605. doi: 10.1016/j.scitotenv.2020.138605. Doi: 10.1016/j.scitotenv. 2020.138605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Villeneuve PJ, Goldberg MS. Methodological Considerations for Epidemiological Studies of Air Pollution and the SARS and COVID-19 Coronavirus Outbreaks. Environ Health Perspect. 2020;128(9):95001. doi: 10.1289/EHP7411. Doi: 10.1289/EHP7411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Wang B, Liu J, Fu S, et al. Airborne particulate matter, population mobility and COVID-19: a multi-city study in China. BMC Public Health. 2020;20(1):1585. doi: 10.1186/s12889-020-09669-3. Doi: 10.1186/ s12889-020-09669-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Zhu Y, Xie J, Huang F, Cao L. Association between short-term exposure to air pollution and COVID-19 infection: Evidence from China. Sci Total Environ. 2020;727:138704. doi: 10.1016/j.scitotenv.2020.138704. Doi. 10.1016/j.scitotenv.2020.138704. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Yao Y, Pan J, Liu Z, et al. Ambient nitrogen dioxide pollution and spread ability of COVID-19 in Chinese cities. Ecotoxicol Environ Saf. 2021;208:111421. doi: 10.1016/j.ecoenv.2020.111421. Doi:10.1016/j.ecoenv.2020.111421. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Liang D, Shi L, Zhao J, et al. Urban Air Pollution May Enhance COVID-19 Case-Fatality and Mortality Rates in the United States. Innovation. 2020;1(3):100047. doi: 10.1016/j.xinn.2020.100047. Doi: 10.1016/j.xinn.2020.100047. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Veronesi G, De Matteis S, Calori G, et al. Long-term exposure to air pollution and COVID-19 incidence: a prospective study of residents in the city of Varese, Northern Italy. Occup Environ Med. 2022;79(3):192–199. doi: 10.1136/oemed-2021-107833. Doi: 10.1136/oemed-2021-107833. [DOI] [PubMed] [Google Scholar]
- 18.Office for National Statistics. Coronavirus (COVID-19) Related Deaths by Occupation, England and Wales: deaths registered between 9 March and 28 December 2020. Available online at: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/causesofdeath/bulletins/coronaviruscovid19relateddeathsbyoccupationenglandandwales/deathsregisteredbetween9marchand28december2020#men-and-deaths-involving-covid-19-by-occupation. (Last Accessed: 16 June 2022) [Google Scholar]
- 19.Istituto Superiore di Sanità - Istituto Nazionale di Statistica. Impact of the COVID-19 epidemic on the total mortality of the resident population: January - November 2020. https://www.istat.it/it/files//2020/12/Rapp_Istat_Iss.pdf. . [In Italian] (Last Accessed: 11 April 2021) [Google Scholar]
- 20.Italian Ministry of Transportation and Navigation. Ministerial Decree No. 88 of 13 February 1999. [Regulation of the assessment and control of the physical and psycho-attitudinal fitness of the public transport personnel as stated by the article No. 9, points 3 and 4, of the President of the Republic Decree No. 753 of 11 July 1980] Gazz. Uff. No. 84 of 12 April 1999, [In Italian] [Google Scholar]