

Abstract
Background:
Musculoskeletal disorders (MSDs) and work-related stress are among the factors that can negatively affect work ability. Given the importance of midwives’ health, this study aims to evaluate the work ability of midwives and to investigate its association with the prevalence of MSDs and work-related stress in midwifery.
Methods:
Ninety-one midwives participated in this study. Three questionnaires, including Nordic musculoskeletal questionnaire (NMQ) plus body map, Persian version of work ability index (WAI) questionnaire, and Health and Safety Executive (HSE) job stress questionnaire, were used to collect data. Finally, the association of MSDs, work-related stress, and individual characteristics with WAI among midwives was investigated.
Results:
The highest rates of pain and discomfort were reported in the lower back and neck. The mean job stress was 116.08 with the highest scores on demand, role, and control subscales. The work ability among midwives was at an acceptable level of 39.07 on average. Inter-variable association analysis showed that the work ability was significantly associated with pain in the past 12 months and the number of coexisting MSDs. Job stress was not associated with work ability.
Conclusions:
Midwives’ WAI was at an acceptable level despite high prevalence of MSDs in midwives, the confirmation of the possible correlation between MSDs and work ability, as well as the high job stress in midwifery. Since the present study was conducted during the Covid-19 pandemic, the high stress in midwives may be partly due to the pandemic and may not be permanent. However, this level of stress may reduce the midwives' work ability over a long time.
Keywords: Work ability index, work-related stress, work-related musculoskeletal disorders, midwives
1. Introduction
Maintaining work ability and perseverant effort for improving work ability of employees has been a critical issue in most occupations [1]. According to previous studies, low work ability increases premature retirement in work environments, longer work absenteeism, and lower quality of work performed by employees [2]. Midwifery is an occupation in which maintaining work ability is of great importance.
Because of limitations in functionality or productivity in maternity, the lives of mother and baby can be endangered or critical and chronic damages may develop. According to some recent studies in London UK, a considerably large number of babies were lost or had severe brain damage because of some problems during labor; for example, this occurred for 1123 out of about 700,000 babies in 2016 [3]. The claims of maternity as result of preventable death cases or damages make up a considerable share (48%) of the total claims against the National Health Service (NHS); e.g., the value of such claims reached £2.1 billion between 2017 and 2018 [4].
Therefore, identifying the factors that can reduce the work ability of midwives can improve the health of midwives, mothers, and babies. Musculoskeletal disorders (MSDs) and work-related stress are among the factors that can adversely affect the workers’ work ability [5, 6]. Work-related MSDs are among the most important problems that have negative effect on work ability and quality of life and can lead to premature retirement [7]. In MSDs, one or more components of the musculoskeletal system are affected by injuries or disorders [8]. Epidemiological studies have shown that some physical factors, such as improper postures, bending, and frequent rotation, which are commonly found in the midwives’ duties [9], are determining factors in the development of MSDs [10].
Midwives may also be exposed to work-related stress due to the nature of their job responsibilities. According to the literature, various work-related stress can affect WAI. In a review study by van den Berg et al. [2], the mean WAI score can be adversely affected by job-induced high physical and mental demands and low control on the job. Other similar studies also showed that some factors are strongly related to low WAI. These include having no information about organizational changes [11], role ambiguity, and no support from supervisors [12].
Previous studies have shown that imbalance between individual characteristics and psychophysiological needs can increase MSDs and combination of these disorders and job stress can reduce the work ability in different occupations [13, 14]. Studies conducted by Phongamwong and Deema among healthcare providers [15] and by Bugajska and Sagan [7] indicated that MSDs reduce work ability. However, Akodu et al. conducted a study on nurses, which showed that despite the high prevalence of MSDs, there is no significant association between MSDs and WAI [16].
In many studies, the association between work-related psychosocial factors and WAI has been confirmed [5, 6, 17]. This association is frequent among health care workers. For example, Gharibi et al. conducted a study on the effects of work-related stress on WAI in Iranian employees who were working in five different workplaces, including two training and medical hospitals [13], Knezevic et al. studied WAI and work-related stress among Croatian midwives [18], and Mazloumi et al. investigated the association between psychosocial factors and WAI among workers in petrochemical industry [19]; these studies revealed the association between workplace stress and WAI.
To the best of our knowledge, despite the great importance of midwives’ work ability, few studies have been conducted on evaluating WAI and its association with important variables, such as MSDs and workplace stress, in midwifery. According to recent studies, midwives are exposed to different ergonomic risk factors more than other health care workers [9]. This is because of the special position of mothers during childbirth and breastfeeding, as well as the slippery and wet skin of newborn babies, which often force the midwives into maintaining inappropriate postures (rotation/flexion of trunk or neck, holding arms/forearms away from the body, and knee flexion) and expose them to MSDs. Furthermore, there are many psychosocial factors in the workplace that can lead to stress in midwives. Some of the stress factors in midwifery are talking to the mother about her positions and needs, answering the appropriate and sometimes inappropriate questions and demands of the companions, as well as the midwives may be worried about being sued or having complaints lodged against them [9].
To develop ergonomic and occupational health intervention programs for maintaining and improving the midwives’ health, it is necessary to evaluate the work ability and investigate its association with the prevalence of MSDs and work-related stress. Accordingly, the present study was conducted with the following objectives:
Determining WAI and its association with demographic characteristics in midwives;
Evaluating the prevalence of MSDs and its association with WAI among midwives;
Determining work-related stress associated with WAI in midwives.
It is worth mentioning that in various studies conducted during the Covid-19 pandemic, the possibility of the impact of this disease on the work ability of employees should be considered. This can also be considered for the results of the present study since it was conducted during the Covid-19 pandemic.
2. Methods
2.1. Participants
This cross-sectional descriptive study was conducted in August and September 2020. Ninety-one midwives who were working in maternity hospitals in Kerman, Iran, with at least two years of experience, participated in this study. The inclusion criteria for this study were the absence of a second job that would lead to musculoskeletal disorders, and individuals who developed musculoskeletal disorders as a result of an accident or any cause other than the intended job were excluded from the study. The volunteer midwives were selected for the study using the census method and based on inclusion criteria. The exclusion criteria were holding a second job that could cause MSDs and to have MSDs due to some previous accidents or any other reason. All participants signed their written informed consent before the study. This study was approved by the ethics committee of Kerman University of Medical Sciences.
2.2. Data collection tools
2.2.1. Demographic questionnaire
This questionnaire included age, weight, height, work experience, work shifts, second job, marital status, and educational level.
2.2.2. WAI questionnaire
Various techniques and tools have been used to measure the work ability of employees. As a valid self-report tool, WAI is widely used in different studies to evaluate work ability [14]. The purpose of using WAI, which was developed by the Finland Institute of Occupational Health Research, is to detect and avoid work-related disability and premature retirement [20]. WAI is determined as the total score from seven dimensions. These seven items include: current work ability compared with the lifetime best, work ability in relation to the demands of the job, number of current diseases diagnosed by a physician, estimated work impairment due to diseases, sick leave during the past 12 months, personal prognosis of work ability two years from now, and mental resources [14]. The best and worst estimates of WAI count to 49 and 7 points, respectively. Ultimately, the obtained scores are used as a basis for classifying the work ability into four groups, i.e. excellent (44-49), good (37-43), moderate (28-36), and poor (7-27) [21]. The translation of the WAI questionnaire into Persian was validated and its reliability was confirmed by Abdolalizadeh et al. in Iran [22].
2.2.3. Nordic musculoskeletal questionnaire
The general Nordic musculoskeletal questionnaire (NMQ) quantifies the reported MSDs separately in nine anatomical regions (neck, shoulders, lower back, upper back, wrists/hands, ankles/feet, knees, hips/thighs and elbows) for both left and right sides of the body. To determine the presence or absence of musculoskeletal complaints, the following question was used: “Have you had problems in…?” (The question being made for the regions of the body already described), giving the answer “Yes” or “No” [23]. The psychometric properties of the Persian version of NMQ were evaluated by Choobineh et al. [24]. It should be noted that the reported musculoskeletal symptoms during the last 12 months were considered. Given that musculoskeletal disorders during the last 7 days are more affected by daily factors at work and at home, as well as the importance of musculoskeletal disorders that accumulate in the limbs over time, when analyzing the data, disorders in the last 12 months and the number of combined disorders were considered.
2.2.4. Health and Safety Executive Stress Questionnaire
The UK Health and Safety Executive (HSE) has designed the HSE Job stress questionnaire to measure work-related stress. This questionnaire is a tool that can assess job stressors and is an advanced method for screening work-related stress. HSE measures seven occupational psychosocial stressors using 35 items: Demands (issues such as workload, work patterns and work environment), Control (it covers how much a person comments on how they do their job), Managerial support provided by managers/supervisors (support and resources provided by the organization and line managers), Peer support (support and resources provided by partners), Relationships (effective measures taken to prevent conflict and deal with inappropriate behavior), Role (clear understanding of employees of roles in the organization), and Changes (how to manage changes in the organization and inform employees). Employers can use the results of the index tool to calculate individual scores for seven subscales as well as an overall score of overall work-related stress. Respondents were asked questions in one of two 5-point scales (1 never, rarely, sometimes, often, 5 always, or 1 strongly disagree, disagree, neutral, agree, 5 strongly agree). This can be used by employers to calculate the overall work-related stress score for their organization. The overall HSE shows one-dimensional score percentiles based on an average of seven factors, which organizations may want to calculate and use in addition to factor metrics [25]. The overall score of job stress is between 0-175 and the high score in this questionnaire indicates the high level of stress, unfavorable job position and the low score indicates good job position, stress and low job pressure. Therefore, a score of 0-35 was considered as optimal, a score of 35-70 was considered mild stress, a score of 10-105 was moderate stress, a score of 105-140 was considered severe stress and a score of 140-175 was considered as very severe stress.
In Iran, Azad-Marzabadi and Fesharaki have investigated and confirmed the validity and reliability of this questionnaire [26].
2.3. Procedure
In this study, the prevalence of MSDs was assessed using NMQ. Body map was used to identify different body regions. Then, the psychosocial risk factors in midwifery were assessed using the HSE job stress questionnaire and the midwives’ work ability was assessed using the WAI questionnaire. The researcher visited the participants at their work and instructed them on how to complete the questionnaires, then the researcher received the completed questionnaires.
2.4. Statistical analysis
To analyze the collected data, SPSS version 20 was used. Descriptive statistical techniques were used to show the demographic characteristics of the subjects. Independent t-test and Pearson correlation were used to analyze the effect of demographic characteristics on WAI. Moreover, independent t-test and chi-square test were used to analyze the effect of demographic characteristics on MSDs. Independent t-test was used to evaluate the effect of MSDs on the WAI score. Pearson correlation was applied to find the association of job stress and seven subscales of Persian version of HSE with the WAI score. Additionally, t-test was used to analyze the effect of job stress and its subscales on MSDs. Finally, hierarchical multiple regression analysis was used to predict the WAI score. In the first step, MSDs and WAI were included in the regression model. Then, in the second step, job stress was included in the model. A significance level of p<0.05 was considered in this study.
3. Results
The demographic data of all 91 midwives who participated in this study are shown in Table 1. The mean age of the subjects was 35.70±6.089 years. Moreover, 44% of the participants had a normal body mass index (BMI) and 84% of them worked in shifts. Based on the results, the mean WAI in midwives was 39.07±5.217. According to the WAI scores, 2.2% of participants had poor work ability, 25.3% moderate, 53.8% good, and 18.7% excellent.
Table 1.
Demographic data and their correlations with WAI.
| Characteristics | N (%)/Mean±SD | P-value |
|---|---|---|
| Age (years) | 35/7±6.089 | 0.066 |
| Age <29 | 21 (23.1%) | |
| Age 30-40 | 57 (62.6%) | |
| Age >41 | 13 (14.3%) | |
| BMI | 26/395±6/089 | 0.484 |
| Underweight = BMI <18.5 | 2 (2.2%) | |
| Normal weight = 18.5–24.9 | 40 (44%) | |
| Overweight = 25–29.9 | 26 (28.6%) | |
| Obesity = BMI ≥30 | 23 (25.3%) | |
| Job tenure (years) | 9/93±5/416 | 0.0231 |
| <5 | 27 (29.7%) | |
| 5-10 | 28 (30.8%) | |
| ≥10 | 36 (39.5%) | |
| Marital status | 0.916 | |
| Single | 25 (27.5%) | |
| Married | 66 (72.5%) | |
| Educational level | 0.804 | |
| Associate Degree | 1 (1.1%) | |
| Associate | 82 (90.1%) | |
| BSc and above | 8 (8.8%) | |
| Work schedule | 0.957 | |
| Day-work | 15 (16%) | |
| Shift-work | 76 (84%) |
1 Correlation was significant at a level of 0.05.
The mean score of job stress was 116.08±14.625. Descriptive statistics on the HSE job stress subscales are presented in Table 3. Moderate stress, high stress and very high stress was reported in 26.4%, 70.3% and 3.3% of participants respectively.
Table 3.
Analysis of job stress as well as its subscales and their correlations with WAI.
| Mean±SD | Max-Min | Correlation coefficient | P-value | |
|---|---|---|---|---|
| WAI | 39.07±5.217 | 49-24 | 1 | 1 |
| HSE | 116.08±14.625 | 161-83 | 0.051 | 0.63 |
| Demand | 24.05±5.522 | 39-11 | -0.213 | 0.0431 |
| Control | 19.87±3.637 | 28-11 | 0.246 | 0.0191 |
| Supervisory Support | 17.40±3.574 | 24-10 | 0.112 | 0.291 |
| Coworker Support | 14.73±3.499 | 20-5 | 0.153 | 0.149 |
| Relationship | 10.34±3.416 | 20-4 | -0.195 | 0.065 |
| Role | 19.89±3.466 | 25-10 | 0.104 | 0.325 |
| Change | 9.84±2.626 | 15-4 | 0.156 | 0.14 |
1 Correlation was significant at a level of 0.05.
A total of 96.7% of participating midwives reported at least one MSD over the last 12 months. The most common region with pain and discomfort over the last 12 months was neck, while the back was affected by the most severe pain and discomfort within the last 7 days. Over the last 12-month period, 33% and 26.4% of the midwives were unable to work due to the pain/discomfort in the lower back and neck, respectively. Table 2 shows the prevalence of musculoskeletal symptoms reported during 12 months in 15 anatomical regions.
Table 2.
Prevalence of MSDs and their correlations with WAI.
| MSDs | N (%) | P-value |
|---|---|---|
| Neck | 41 (45.1%) | 0.727 |
| Right Shoulder | 24 (26.4%) | 0.453 |
| Left Shoulder | 17 (18.7%) | 0.235 |
| Right Elbow | 9 (9.9%) | 0.81 |
| Left Elbow | 7 (7.7%) | 0.479 |
| Right Wrist and Hand | 20 (22%) | 0.24 |
| Left Wrist and Hand | 17 (18.7%) | 0.353 |
| Upper Back | 32 (35.2%) | 0.0151 |
| Lower Back | 39 (42.9%) | 0.479 |
| Right Hip and Thigh | 7 (7.7%) | 0.0171 |
| Left Hip and Thigh | 2 (2.2%) | 0.485 |
| Right Knee | 15 (16.5%) | 0.031 |
| Left Knee | 14 (15.4%) | 0.828 |
| Right Feet and Ankle | 7 (7.7%) | 0.136 |
| Left Feet and Ankle | 5 (5.5%) | 0.559 |
1 Correlation was significant at a level of 0.05.
Some participants reported more than one MSD over the last 12 months. Only 3.3% of participants reported no disorder. The largest number of participants reported two coexisting disorders, and 27.5% of participants reported four or more coexisting disorders (Figure 1).
Figure 1.
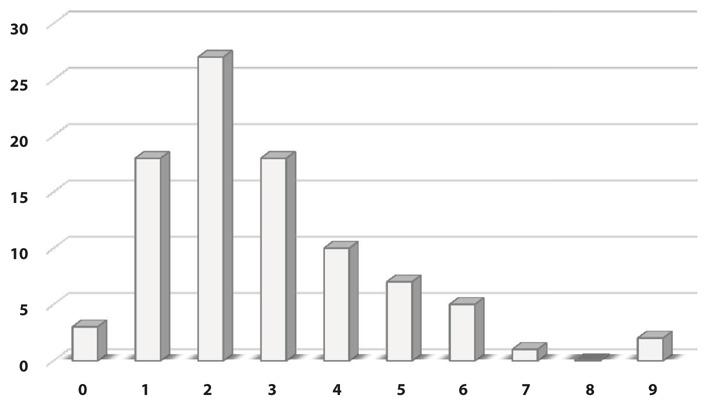
Frequency of the number of musculoskeletal disorders.
The correlation analyses showed that WAI was associated with individual factors, such as work experience and pain, over the last 12 months in some body regions (Tables 1 and 2). MSDs within the last 7 days were mainly affected by routine factors at work and home. Moreover, cumulative MSDs were of great importance. Consequently, in the data analysis, the disorders within the last 12 months and the number of coexisting disorders were considered.
The analysis of the association between job stress and pain over the last 12 months showed no significant association between job stress and MSDs, while the job stress subscales such as role, demand, control, and change had significant association with MSDs in some of the body regions. There is a meaningful relationship between: sub-scale of role and pain in the last 12 months in the neck and ankle area of the right foot, sub-scale of demand and pain in the last 12 months in the right and left ankle, sub-scale of control and pain in the last 12 months in the upper back, sub-scale changes and pain in the last 12 months in the lower back. Additionally, the study of the association of individual factors with pain over the last 12 months showed that age, BMI, work experience, and marital status were the predictors of MSDs. The results showed a statistical correlation between age and pain in the last 12 months in the left shoulder and right knee, between height and pain in the last 12 months in the wrist, left hand, foot and ankle of the right and left legs, between body mass index and pain in the last 12 months. Looking at feet and ankles we observed a significant correlation between work experience and pain. There was a relationship between left shoulder pain and marital status of 4.89 with a significance level of 0.034 and between foot and ankle pain of the left foot and marital status of 7.326 with a significance level of 0.019.
The analysis of the association between WAI and psychosocial factors showed that job stress was not associated with WAI, while demand and control subscales were the predictors of WAI (Table 3).
The linear regression analysis and the modeling of the relationship between WAI and the number of MSDs showed that there was a significant but inverse relationship between WAI and the number of MSDs with a value of 0.27. However, with the inclusion of job stress in the model, which addresses the relationship between WAI and the number of MSDs, no significant change was observed in the β coefficient. Therefore, job stress had no effect on the midwives’ work ability and only the coexisting MSDs were the most important negative predictors of the WAI (Table 4).
Table 4.
Modeling the correlations of MSDs and job stress with WAI.
| Predictors | β | P-Value | 95% Confidence interval | |
|---|---|---|---|---|
| Lower | Upper | |||
| The number of coexisting MSDs | -0.793 | 0.0091 | -1.38 | -0.0205 |
| HSE | 0.016 | 0.669 | -0.057 | 0.088 |
1 Correlation was significant at a level of 0.05.
4. Discussion
The present study aims to evaluate the WAI among midwives and its association with important variables, such as MSDs and stress at work. To the best of our knowledge, the present study is the first of its kind that focuses on these relationships in midwifery.
The results of this study showed that based on the classification of WAI [21], 72.5% of participants had an appropriate level of work ability (WAI≥37), while almost two thirds of participants reported high work-related stress (HSE>105). A total of 76.9% of the subjects reported more than one MSD. A significant and inverse relation was observed between MSDs and the mean WAI score. Job stress was not associated with WAI, while only the demand and control subscales had a significant relationship with WAI.
The WAI in this study with a mean of 39.07 was close to the WAI in Croatian midwives (60 midwives with an average age of 33.5 years) with a mean of 40 [18]. According to the WAI classification, the mean WAI of the participants was at a desirable level (WAI≥37). However, given that about 71% of midwives were between 28 and 42 years of age, their work ability was not appropriate for their age. Because according to the study of Kujala et al., a WAI score of less than 40 is inappropriate for those in their early 30s [27].
In studies on other occupational groups of health care providers, such as nurses, an acceptable level of work ability has been reported [28]. For example, Fischer et al. reported a mean WAI of 39.7 [29] among health care personnel, and Rotenberg et al. reported WAIs in the range of 37-44 among US nurses [30].
Differences in work ability can be attributed to the differences in the type of the work, working conditions, and characteristics of the study population. Varianou-Mikellidou et al. found that workplace, work demands (such as manual handling), work organization, environmental stressors, and individual characteristics, affect individuals’ work ability [18]. However, it should be noted that this study was conducted during the Covid-19 pandemic, so the use of protective equipment, such as respirators, or stress of being affected by the disease can also affect the work ability of individuals.
Numerous studies have confirmed the effects of individual factors, such as age, gender, and work experience, on the employees’ work ability [5]. Accordingly, Monteiro et al. proved the effect of age, educational level, and work experience on WAI among employees of a health institution in Brazil [31], and Chiu et al. confirmed the effect of age on WAI among nurses [28].
In the present study, no direct association was found between work experience and WAI. However, Gharibi et al. reported an inverse relationship between work experience and WAI among workers from five different work sectors [13]. This disagreement can be ascribed to differences in the subjects and their job responsibilities. Those tasks that require more skill are usually carried out by more experienced employees, so less physical and mental demands are needed. Moreover, two thirds of the subjects were less than 40 years of age and could acquire good knowledge and skills. Therefore, greater work experience (job tenure) may prevent the work ability decline through acquiring experience and skills. Okuyucu et al. found that more experienced midwives maintain more proper postures during their work and are more successful in communicating with mothers [9].
The present study showed that the prevalence of MSDs was high in the participants, particularly in the neck and lower back. These results agree with those of other studies conducted on midwives [9] and other occupational health care groups, such as physiotherapists, physicians, and paramedics [32]. In a review on MSDs in midwives, Okuyucu et al. indicated that work conditions can significantly affect the development of musculoskeletal symptoms and the risk of MSD is high in midwifery [9]. The results of the present study agree with findings of these studies. The high prevalence of MSDs can be attributed to the nature of midwifery duties since during many midwifery tasks, the midwives have to maintain inappropriate postures. Some studies have reported that work postures can potentially lead to the development of MSDs [33]. Nowotny-Czupryna et al. found that the spinal posture during childbirth is often inappropriate, which leads to high pain prevalence in different regions of the spine [33].
Some previous studies have shown the effect of individual factors on MSDs [34], and the present study also indicated the association of age, BMI, work experience, and marital status with MSDs. Our results showed an inverse relationship between WAI and the number of MSDs. Kun Ou et al. also investigated the possibility of a relationship between the prevalence of MSDs and work ability among nurses and confirmed the existence of this relationship [35]. Rashid et al. studied the work ability of women with chronic pain in the neck, shoulders, and back. These authors showed that the severity of pain and job pressure are two predictors of work ability, and work ability decreases with increasing pain intensity [6].
The results of linear regression and the modeling of the relationship between WAI and the number of coexisting MSDs showed that when an (extra) MSD is added, work ability decreases by 0.79. This is because the discomfort of participants increases with the number of regions affected by MSDs, so work ability decreases. Furthermore, this is also associated with the diseases that are effective in determining the work ability [5]. Given that the hypothesis of association between the prevalence of MSDs and the work ability among midwives was confirmed in this study and that maintaining the work ability of midwives is of great importance. further studies have to be conducted to accurately assess the biomechanical risk factors, such as, working postures, the duration of midwife’s exposure to postural loads, and the time of receiving ergonomic interventions.
The job stress of the studied midwives was at a high level (HSE≥ 105) [36]. The study on Croatian midwives conducted by Knezevic et al., as well as a study on Australian midwives conducted by Lein weber et al., revealed the presence of stress in midwifery [18]. Several other studies have also reported moderate to severe job stress among the employees of other occupational groups, such as nurses and health care providers [37].
Several studies have found an association between MSDs and psychosocial factors [34]. Based on the data analysis in these studies, the job stress subscales, including role, demand, control and change, are significantly associated with MSDs in some body regions. Bernal et al. investigated the association between work-related psychosocial factors and MSDs among nurses and assistant nurses. According to these authors, psychosocial factors, such as high demand and low control/support, are significantly associated with disorders and pain in different body regions in these occupational groups [38].
Several studies have shown that work-related stress is an important risk factor in work ability [39]. According to results of this study, there was no association between job stress and work ability. However, some studies conducted on other occupational groups have confirmed an association between job stress and work ability. This association was reported for Iranian workers by Gharibi et al. [13] and for Brazilian nurses by Fischer et al. [29].
It is worth mentioning that some dimensions of job stress (demand and control) individually have significant association with the WAI. This agrees with the results of many studies [13, 14] including the one conducted by Mazloumi et al. in which demand was identified as a negative predictor of work ability, while ability to skill discretion and social support were identified as factors that are directly associated with work ability [19].
Demand is one of the psychosocial factors that negatively affect the work ability because an increase in job demands increases the workload of individuals and, thus, reduces the work ability. Midwifery has sensitive tasks and requires maintaining special postures (during childbirth), so it has a different workload compared to other occupational groups and a possible imbalance between the workload and the professional/individual characteristics of midwives can affect their work ability. Additionally, this study was conducted during the Covid-19 pandemic. Under these conditions, the illness and the changes in shift schedules due to the reduction in the number of health care workers increased the midwives' workload while their rest hours decreased. Consequently, it is possible that the midwives’ work ability was adversely affected by these changes.
While demand had a negative effect on work ability, control was directly related to work ability. Midwives need the mother’s cooperation to effectively perform their duties and they can work better if they have proper control over their duties. As a result of high job stress, these two factors probably reduced the work ability of the midwives who participated in this study.
It should also be noted that job stress can reduce the work ability in the long run. Given that the study was conducted during the Covid-19 pandemic, the high stress of midwives during the study may have been due, in part, to the pandemic and may have been temporary. As revealed by some studies in other occupational groups, the Covid-19 pandemic has increased the employees’ job stress [40].
Given that this study was conducted during the Covid-19 pandemic, so the use of protective equipment, such as respirators, or stress of being affected by the disease can also affect the work ability of individual. To our knowledge, only one study prior to the Covid-19 pandemic assessed the Midwifery Workability Index, in which the Working Ability Index in the study group was 40, which is slightly higher than the present study [17].
5. Conclusions
The highest rates of pain and discomfort corresponded to the lower back and neck. Job stress of midwives was at a high level. Despite the high prevalence of MSDs and high stress in midwifery, the midwives’ work ability was at an acceptable level. No association between WAI and job stress of midwives in this study can be attributed to the coincidence of the Covid-19 pandemic and this study. Given that the present study was conducted during the Covid-19 pandemic, it is likely that the midwives’ high stress during the study was partly due to the pandemic and not permanent since the pandemic has increased the physical and mental workload of midwives. However, this level of stress may reduce the midwives’ work ability in the long run.
Acknowledgments:
This article was extracted from a thesis written by Mrs. Maryam Amirmahani, MSc student of Ergonomics, and financially supported by Kerman University of Medical Sciences via grant No. 98000723.
Funding:
This research received no external funding.
Informed Consent Statement:
Informed consent was obtained from all subjects involved in the study.
Declaration of Interest:
The authors declare no conflict of interest.
References
- 1.Saedpanah K, Eskandary T, Moatamedzade M. Study the relation between Work Ability Index and Life Style in Mechanics of Thermal power plant. J Occup Hyg Eng. 2016;3(3):47–55. [Google Scholar]
- 2.van den Berg T, Elders L, de Zwart B, Burdorf A. The effects of work-related and individual factors on the Work Ability Index: a systematic review. Occup Environ Med. 2008 doi: 10.1136/oem.2008.039883. Doi: 10.21859/johe-03033. [DOI] [PubMed] [Google Scholar]
- 3.Robertson L, Knight H, Prosser-Snelling E, et al. Each baby counts in 2018 – lessons learned and future directions. Obstet Gynaecol Reprod Med. 2018;28(8):253–7. Doi: 10.1016/j.ogrm.2018.07.004. [Google Scholar]
- 4.Resolution NJPoJ. Annual report and accounts 2017/18. 2018 [Google Scholar]
- 5.Mokarami H, Mortazavi SB, Asgari A, Choobineh A, Stallones L. Multiple dimensions of work-related risk factors and their relationship to work ability among industrial workers in Iran. Int J Occup Saf Ergon. 2017;23(3):374–9. doi: 10.1080/10803548.2016.1262602. Doi: 10.1080/10803548.2016.1262602. [DOI] [PubMed] [Google Scholar]
- 6.Rashid M, Kristofferzon M-L, Heiden M, Nilsson A. Factors related to work ability and well-being among women on sick leave due to long-term pain in the neck/shoulders and/or back: a cross-sectional study. BMC Public Health. 2018;18(1):1–8. doi: 10.1186/s12889-018-5580-9. Doi: 10.1186/s12889-018-5580-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bugajska J, Sagan A. Chronic musculoskeletal disorders as risk factors for reduced work ability in younger and ageing workers. Int J Occup Saf Ergon. 2014;20(4):607–15. doi: 10.1080/10803548.2014.11077069. Doi: 10.1080/10803548.2014.11077069. [DOI] [PubMed] [Google Scholar]
- 8.Ramírez-Sepúlveda KA, Gómez-Arias MY, Agudelo-Suárez AA, Ramírez-Ossa DM. Musculoskeletal Disorders and Related Factors in the Colombian Orthodontists’ Practice. Int J Occup Saf Ergon. 2020:1–28. doi: 10.1080/10803548.2020.1857975. Doi: 10.1080/10803548.2020.1857975. [DOI] [PubMed] [Google Scholar]
- 9.Okuyucu K, Hignett S, Gyi D, Doshani A. Midwives’ thoughts about musculoskeletal disorders with an evaluation of working tasks. Appl Ergon. 2021;90:103263. doi: 10.1016/j.apergo.2020.103263. Doi: 10.1016/j.apergo.2020.103263. [DOI] [PubMed] [Google Scholar]
- 10.Lorusso A, Bruno S, L'abbate N. A review of low back pain and musculoskeletal disorders among Italian nursing personnel. Ind Health. 2007;45(5):637–44. doi: 10.2486/indhealth.45.637. Doi: 10.2486/indhealth.45.637. [DOI] [PubMed] [Google Scholar]
- 11.Guidi S, Bagnara S, Fichera G. The HSE indicator tool, psychological distress and work ability. Occup Med. 2012;62(3):203–9. doi: 10.1093/occmed/kqs021. Doi: 10.1093/occmed/kqs021. [DOI] [PubMed] [Google Scholar]
- 12.Sugimura H, Thériault G. Impact of supervisor support on work ability in an IT company. Occup Med. 2010;60(6):451–7. doi: 10.1093/occmed/kqq053. Doi: 10.1093/occmed/kqq053. [DOI] [PubMed] [Google Scholar]
- 13.Gharibi V, Mokarami H, Taban A, Aval MY, Samimi K, Salesi M. Effects of work-related stress on work ability index among Iranian workers. Saf Health Work. 2016;7(1):43–8. doi: 10.1016/j.shaw.2015.10.005. Doi: 10.1016/j.shaw.2015.10.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.van den Berg TI, Alavinia SM, Bredt FJ, Lindeboom D, Elders LA, Burdorf A. The influence of psychosocial factors at work and life style on health and work ability among professional workers. Int Arch Occup Environ Health. 2008;81(8):1029–36. doi: 10.1007/s00420-007-0296-7. Doi: 10.1007/s00420-007-0296-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Phongamwong C, Deema H. The impact of multi-site musculoskeletal pain on work ability among health care providers. J Occup Med Toxicol. 2015;10(1):1–5. doi: 10.1186/s12995-015-0063-8. Doi: 10.1186/s12995-015-0063-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Akodu AK, Ashalejo ZO. Work-related musculoskeletal disorders and work ability among hospital nurses. J Taibah Univ Medical Sci. 2019;14(3):252–61. doi: 10.1016/j.jtumed.2019.02.009. Doi: 10.1016/j.jtumed.2019.02.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Varianou-Mikellidou C, Boustras G, Nicolaidou O, Dimopoulos C, Anyfantis I, Messios P. Work-related factors and individual characteristics affecting work ability of different age groups. Saf Sci. 2020;128:104755. Doi: 10.1016/j.ssci.2020.104755. [Google Scholar]
- 18.Knezevic B, Milosevic M, Golubic R, Belosevic L, Russo A, Mustajbegovic J. Work-related stress and work ability among Croatian university hospital midwives. Midwifery. 2011;27(2):146–53. doi: 10.1016/j.midw.2009.04.002. Doi: 10.1016/j.midw.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 19.Mazloumi A, Rostamabadi A, Saraji JN, Foroushani AR. Work ability index (WAI) and its association with psychosocial factors in one of the petrochemical industries in Iran. J Occup Health. 2012:1202130234. doi: 10.1539/joh.11-0150-oa. Doi: 10.1539/joh.11-0150-OA. [DOI] [PubMed] [Google Scholar]
- 20.Ilmarinen J. Work ability - a comprehensive concept for occupational health research and prevention. Scand J Work Environ Health. 2009;35(1):1–5. doi: 10.5271/sjweh.1304. [DOI] [PubMed] [Google Scholar]
- 21.Ilmarinen J. The work ability index (WAI) Occup Med. 2007;57(2):160. Doi: 10.1093/occmed/kqm008. [Google Scholar]
- 22.Abdolalizadeh M, Arastoo A, Ghsemzadeh R, Montazeri A, Ahmadi K, Azizi AJ. The psychometric properties of an Iranian translation of the Work Ability Index (WAI) questionnaire. J Occup Rehabil. 2012;22(3):401–8. doi: 10.1007/s10926-012-9355-3. Doi: 10.1007/s10926-012-9355-3. [DOI] [PubMed] [Google Scholar]
- 23.Kuorinka I, Jonsson B, Kilbom A, et al. Standardized Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–7. doi: 10.1016/0003-6870(87)90010-x. Doi: 10.1016/0003-6870(87)90010-X. [DOI] [PubMed] [Google Scholar]
- 24.Choobineh A, Lahmi M, Shahnavaz H, Khani Jazani R, Hosseini M. Musculoskeletal symptoms as related to ergonomic factors in Iranian hand-woven carpet industry and general guidelines for workstation design. Int J Occup Saf Ergon. 2004;10(2):157–68. doi: 10.1080/10803548.2004.11076604. Doi: 10.1080/10803548.2004.11076604. [DOI] [PubMed] [Google Scholar]
- 25.Health Executive S. Managing the Causes of Work-Related Stress: A Step-by-Step Approach Using the Management Standards. HSE Books Norwich, UK: 2007. [Google Scholar]
- 26.Azad-Marzabadi E, Salimi S. Study on job stress in a military unit. Mil Med. 2005;6(4):279–84. [Google Scholar]
- 27.Kujala V, Remes J, Ek E, Tammelin T, Laitinen J. Classification of Work Ability Index among young employees. Occup Med. 2005;55(5):399–401. doi: 10.1093/occmed/kqi075. Doi: 10.1093/occmed/kqi075. [DOI] [PubMed] [Google Scholar]
- 28.Chiu M-C, Wang M-JJ, Lu C-W, Pan S-M, Kumashiro M, Ilmarinen J. Evaluating work ability and quality of life for clinical nurses in Taiwan. Nurs Outlook. 2007;55(6):318–26. doi: 10.1016/j.outlook.2007.07.002. Doi: 10.1016/j.outlook.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 29.Marina Fischer F, Notarnicola da Silva Borges F, Rotenberg L, et al. Work ability of health care shift workers: What matters? Chronobiol Int. 2006;23(6):1165–79. doi: 10.1080/07420520601065083. Doi: 10.1080/07420520601065083. [DOI] [PubMed] [Google Scholar]
- 30.Rotenberg L, Portela LF, Banks B, Griep RH, Fischer FM, Landsbergis P. A gender approach to work ability and its relationship to professional and domestic work hours among nursing personnel. Appl Ergon. 2008;39(5):646–52. doi: 10.1016/j.apergo.2008.02.013. Doi: 10.1016/j.apergo.2008.02.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Monteiro MS, Ilmarinen J, Filho HRC. Work ability of workers in different age groups in a public health institution in Brazil. Int J Occup Saf Ergon. 2006;12(4):417–27. doi: 10.1080/10803548.2006.11076703. Doi: 10.1080/10803548.2006.11076703. [DOI] [PubMed] [Google Scholar]
- 32.Karahan A, Kav S, Abbasoglu A, Dogan N. Low back pain: prevalence and associated risk factors among hospital staff. J Adv Nurs. 2009;65(3):516–24. doi: 10.1111/j.1365-2648.2008.04905.x. Doi: 10.1111/j.1365-2648.2008.04905.x. [DOI] [PubMed] [Google Scholar]
- 33.Nowotny-Czupryna O, Naworska B, Brzęk A, et al. Professional experience and ergonomic aspects of midwives' work. J Occup Med Environ Health. 2012;25(3):265–74. doi: 10.2478/S13382-012-0034-6. Doi: 10.2478/S13382-012-0034-6. [DOI] [PubMed] [Google Scholar]
- 34.Liu H-C, Cheng Y, Ho J-J. Associations of ergonomic and psychosocial work hazards with musculoskeletal disorders of specific body parts: A study of general employees in Taiwan. Int J Ind Ergon. 2020;76:102935. Doi: 10.1016/j.ergon.2020.102935. [Google Scholar]
- 35.Ou Y-K, Liu Y, Chang Y-P, Lee B-O. Relationship between Musculoskeletal Disorders and Work Performance of Nursing Staff: A Comparison of Hospital Nursing Departments. Int J Environ Res. 2021;18(13):7085. doi: 10.3390/ijerph18137085. Doi: 10.3390/ijerph18137085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gebriné KÉ, Lampek K, Sárváry A, Sárváry A, Takács P, Zrínyi M. Impact of sense of coherence and work values perception on stress and self-reported health of midwives. Midwifery. 2019;77:9–15. doi: 10.1016/j.midw.2019.06.006. Doi: 10.1016/j.midw.2019.06.006. [DOI] [PubMed] [Google Scholar]
- 37.Klein CJ, Weinzimmer LG, Cooling M, Lizer S, Pierce L, Dalstrom M. Exploring burnout and job stressors among advanced practice providers. Nurs Outlook. 2020;68(2):145–54. doi: 10.1016/j.outlook.2019.09.005. Doi: 10.1016/j.outlook.2019.09.005. [DOI] [PubMed] [Google Scholar]
- 38.Bernal D, Campos-Serna J, Tobias A, Vargas-Prada S, Benavides FG, Serra C. Work-related psychosocial risk factors and musculoskeletal disorders in hospital nurses and nursing aides: A systematic review and meta-analysis. Int J Nurs Stud. 2015;52(2):635–48. doi: 10.1016/j.ijnurstu.2014.11.003. Doi: 10.1016/j.ijnurstu.2014.11.003. [DOI] [PubMed] [Google Scholar]
- 39.Benavides F. Ill health, social protection, labour relations, and sickness absence. Occup Environ Med. 2006;63(4):228–9. doi: 10.1136/oem.2005.025817. Doi: 10.2307/27732710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Eweida RS, Rashwan ZI, Desoky GM, Khonji LM. Mental strain and changes in psychological health hub among intern-nursing students at pediatric and medical-surgical units amid ambience of COVID-19 pandemic: A comprehensive survey. Nurse Educ Pract. 2020;49:102915. doi: 10.1016/j.nepr.2020.102915. Doi: 10.1016/j.nepr.2020.102915. [DOI] [PMC free article] [PubMed] [Google Scholar]