

Learning objectives.
To review the pathophysiology of heart failure with reduced ejection fraction (HFrEF) and how this relates to clinical management.
To review the critical role of key pharmacological therapies and implanted cardiac devices in reducing morbidity and mortality
To recognise the deteriorating patient with HFrEF and to gain understanding of the important advanced therapies, in addition to the key role played by appropriate palliative care in refractory heart failure.
Introduction
Heart failure is a syndrome characterised by a triad of symptoms, signs and objective evidence of cardiac dysfunction. The syndrome is divided into subtypes based on left ventricular ejection fraction (LVEF). Where the LVEF is below 40% this is termed heart failure with reduced ejection fraction (HFrEF). This differentiation from those patients with an LVEF greater than 40% (termed heart failure with mildly reduced EF (HFmrEF)) and greater than 50% (termed heart failure with preserved EF (HFpEF)) is the result of discrete LVEF cut-offs being used as inclusion/exclusion criteria in clinical trials evaluating therapeutic interventions in these patients. HFpEF represents a complex and heterogeneous group of patients, and the aetiology is largely related to comorbidities. Trials in these cohorts have failed to identify specific therapeutic strategies which influence prognosis and management is focused on achieving and maintaining euvolaemia, primarily to alleviate symptoms. Otherwise, treatment of comorbidities, anticoagulation for atrial fibrillation (AF) and strategies to reduce cardiovascular risk are recommended. Patients with HFmrEF phenotypically resemble those with HFrEF, and the clinical consensus is that they should benefit from the same drug therapies.
HFrEF is characterised by the overactivation of the neurohormonal axis—particularly of the sympathetic nervous system and the renin–angiotensin–aldosterone system. Initially this is an adaptive response but one that becomes maladaptive and results in salt and water retention and then a cascade of deleterious consequences related to haemodynamic effects and fibrosis. The importance of diuretics to relieve congestion and improve morbidity should be remembered in all patients butover the last four decades, key trials have established the importance of pharmacological antagonism of these axes in improving morbidity and mortality in patients with HFrEF.
More recently, pharmacological agents targeting other neurohormonal pathways have demonstrated further opportunities for improved outcomes in patients with HFrEF—chief among these are combined angiotensin receptor antagonism with neprilysin inhibition (ARNI) and inhibitors of the sodium–glucose transport protein 2 (sodium–glucose cotransporter 2 inhibitors (SGLT2i)).
Diagnosis of HFrEF
Heart failure is not a diagnosis but a syndrome with a variety of potential causes. Symptoms generally relate to reduced cardiac output, and signs typically to elevated filling pressures (see table 1). Unfortunately, the non-specific nature of symptoms means that identification of HFrEF is often made at a later stage when the patient is admitted to hospital acutely. Often, this represents the end of a long process of chronic pressure/volume overload of the left ventricle with subacute decompensation on a background of chronic myocardial disease. Acute, de novo heart failure—triggered by acute ischaemia, myocarditis, toxin or arrhythmia—is an alternative presentation, and a careful history often identifies the clinical problem. Where heart failure is suspected, serum B-type natriuretic peptide (BNP) or its N-terminal component (NT-proBNP) should be measured and is highly sensitive but poorly specific for heart failure.1 It is used as a gatekeeper for echocardiography, and individuals with a normal BNP can be investigated for other causes of symptoms. BNP is released from the myocardium in response to stretching forces related to elevated filling pressures and it promotes natriuresis, diuresis, vasodilatation and suppresses the sympathetic nervous axis, restoring normal loading conditions. However, levels are chronically elevated in cases of heart failure and higher concentrations are associated with increased risk of hospitalisation and death. In the UK, National Institute for Health and Care Excellence (NICE) has recommended a rapid access pathway based on NT pro-BNP (figure 1).2
Table 1.
Common symptoms and signs of heart failure
| Symptoms | Signs |
|
|
Figure 1.

NICE guideline for the treatment of suspected heart failure. Reproduced under the NICE UK Open Content licence. NT-proBNP, N-terminal component of B-type natriuretic peptide.
The American College of Cardiology/American Heart Association (ACC/AHA) has developed a concept of heart failure staging—see table 2. In practice, presenting patients with heart failure are those in Stage C or D. Such patients are assessed according to their symptoms and identified as being in one of four New York Heart Association (NYHA) classifications—see table 3.3 The principal goals of management are to relieve symptoms, avoid hospitalisation and improve prognosis, and clinical trials have concentrated on these three aspects.
Table 2.
ACC/AHA stages of HF
| Stage | Description | Examples |
| A | Patients at risk of developing HF because of the presence of conditions that are strongly associated with the development of HF. Such patients have no identified structural or functional abnormalities of the pericardium, myocardium or cardiac valves and have never shown symptoms or signs of HF. | Systemic hypertension; coronary artery disease; diabetes mellitus; history of cardiotoxic drug therapy or alcohol abuse; personal history of rheumatic fever; family history of cardiomyopathy. |
| B | Patients who have developed structural heart disease that is strongly associated with the development of HF but who have never shown signs or symptoms of HF. | Left ventricular hypertrophy or fibrosis; left ventricular dilatation of hypocontractility; asymptomatic valvular heart disease; previous myocardial infarction. |
| C | Patients who have current or prior symptoms of HF associated with underlying structural heart disease. | Dyspnoea or fatigue due to left ventricular systolic dysfunction; asymptomatic patients who are undergoing treatment for prior symptoms of HF. |
| D | Patients with advanced structural heart disease and marked symptoms of HF at rest despite maximal medical therapy and who require specialised interventions. | Patients who are frequently hospitalised for HF or cannot be safely discharged from the hospital; patients in the hospital awaiting heart transplantation; patients at home receiving continuous intravenous support for symptom relief or being supported with a mechanical circulatory assist device; patients in a hospice setting for the management of HF. |
ACC/AHA, American College of Cardiology/American Heart Association; HF, heart failure.
Table 3.
NYHA classification
| NYHA class | Level of impairment |
| I | No limitation of physical activity. Ordinary physical activity does not cause undue breathlessness, fatigue or palpitations. |
| II | Slight limitation of physical activity. Comfortable at rest but ordinary physical activity results in undue breathlessness, fatigue or palpitations. |
| III | Marked limitation of physical activity. Comfortable at rest, but less than ordinary physical activity results in undue breathlessness, fatigue or palpitations. |
| IV | Unable to carry out any physical activity without discomfort. Symptoms at rest can be present. If any physical activity is undertaken, discomfort is increased. |
NYHA, New York Heart Association.
Occasionally an LVEF of <40% is detected incidentally in individuals who are truly asymptomatic—this is not heart failure by definition and is termed asymptomatic left ventricular systolic dysfunction (LVSD), equivalent to ACC/AHA Stage B. ACE inhibition has an evidence base and is generally recommended in such cases, and most heart failure specialists would advocate the use of βB and MRA, particularly given the recognised heterogeneity observed when assessing severity of symptoms.
Once a patient has been identified as having HFrEF, the underlying aetiology of their LVSD should be sought. Most commonly this will relate to ischaemic heart disease or an idiopathic dilated cardiomyopathy.4 Patients with chronic impairment of LV systolic function may well have complete resolution of symptoms and LVEF with appropriate therapy but be at risk of recurrent decompensation and continuing medical therapy is supported by experience and randomised trial evidence.5 More rarely, patients may present with a reversible underlying cause of LVSD such as Takotsubo cardiomyopathy, tachycardia-related cardiomyopathy, thyrotoxicosis and others. Critical ischaemia corrected by revascularisation may reverse HFrEF in carefully selected patients but identifying individuals in this category is challenging and the literature would not support routine revascularisation in the absence of anginal symptoms.
The key to understanding the aetiology underlying HFrEF is a careful history and physical examination combined with appropriate investigations. Cardiac MRI is increasingly used to identify specific appearances related to various potential aetiologies, according to patterns of myocardial scar following the administration of gadolinium contrast (figure 2).6
Figure 2.

Hyperenhancement (HE) patterns following administration of gadolinium contrast at MRI according to aetiology of left ventricular systolic dysfunction. Reprinted with permission from Shah.34 HTN, hypertension.
Treating HFrEF
Patients with HFrEF should be engaged with a disease management programme. Acute HF begets chronic heart failure and follow-up after stabilisation of symptoms is key to improving outcome. Prognostically beneficial medications require multiple dose titrations with careful monitoring. The wider healthcare team is critical to delivering the best care for patients and heart failure specialist nurses are the cornerstone of services, with input from heart failure cardiologists, electrophysiologists, specialist cardiac physiologists, physiotherapists, pharmacists and palliative care specialists.7 A wide range of treatment options exist and patients should be regularly reviewed to determine their eligibility for each of these as per figure 3.
Figure 3.
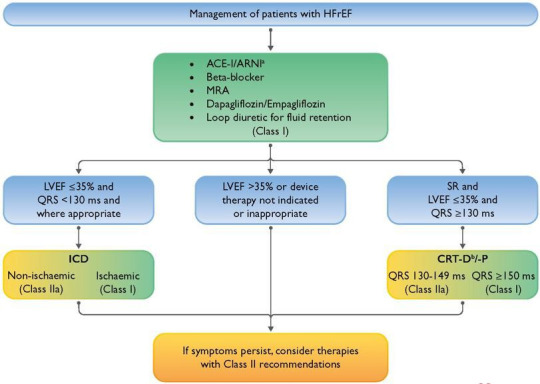
ESC 2021 Therapeutic algorithm of Class I Therapy Indications for a patient with heart failure with reduced ejection fraction. Reproduced from McDonagh et al.7 ACE-I = angiotensin-converting enzyme inhibitor; ARNI = angiotensin receptor-neprilysin inhibitor; CRT-D =cardiac resynchronization therapy with defibrillator; CRT-P = cardiac resynchronization therapy pacemaker; ICD = implantable cardioverter-defibrillator; HFrEF = heart failure with reduced ejection fraction; MRA = mineralocorticoid receptor antagonist; QRS = Q, R, and S waves of an ECG; SR = sinus rhythm. aAs a replacement for ACE-I. bWhere appropriate. Class I = green. Class IIa = Yellow.
Pharmacological management
Diuretics
While almost universally used in the management of HFrEF to relieve symptoms and signs of congestion, there is little evidence for a mortality benefit associated with diuretic use. Loop diuretics are first-line treatments and recommended in cases of acute heart failure.8 Dose escalation may be necessary during decompensations associated with times of intercurrent infection, acute coronary syndrome or acute arrhythmia.9 High doses or intravenous administration may be required with renal impairment, where patients are diuretic resistant, or where there is reduced bioavailability associated with gut oedema. In the congested state, elevated serum creatinine commonly relates to reduced glomerular flow rates due to higher pressures in the efferent arterioles—a consequence of elevated central venous pressure. Escalation of intravenous diuretic therapy rather than dose reduction is indicated in this context.10 Where cardiac function is improved by other therapies, diuretic dose may need to be reduced, as well as at times of insensible fluid losses—for example, during periods of extreme heat or diarrhoeal illness.
Addition of a thiazide diuretic to encourage natriuresis by blocking reabsorption in the distal convoluted tubules can be helpful in diuretic-resistant patients. These patients will need closer monitoring of electrolytes and a low threshold for potassium replacement.
Four pillars of disease-modifying treatment
The neurohormonal model of heart failure is key to understanding the efficacy of disease-modifying medical therapy and is summarised in figure 4. More recent evidence for the significant benefits related to reducing heart failure admissions associated with SGLT2i expands our understanding of the pathophysiology of heart failure and cements these agents as fundamental keystones in the management of HFrEF.
Figure 4.

Overview of homeostatic mechanisms in HFREF. BNP, B-type natriuretic peptide; HFrEF, heart failure with reduced ejection fraction.
Many patients with HFrEF have a degree of renal impairment prior to commencing therapy. Due to their mode of action, some further deterioration in renal function is to be expected with renin–angiotensin–aldosterone system inhibitors (RAASi)—this usually stabilises and ultimately is renoprotective. Pragmatic UK consensus guidelines are available when assessing renal impairment in the patient with HFrEF. Acute kidney injury is often cited as a cause for discontinuing RAASi but such reflex response should be avoided in favour of careful monitoring and consideration of other factors leading to reductions in estimated glomerular filtration rate.11 Occasionally hyperkalaemia may limit RAASi and newer potassium-binding agents may have a role here, but the prognostic benefit of this approach is yet to be determined.
Pillar 1: ACEi/ARB/ARNI
Impaired cardiac output reduces renal perfusion triggering renin release from the juxtaglomerular apparatus which promotes the conversion of angiotensinogen (from the liver) to angiotensin I. ACE metabolises angiotensin I to angiotensin II resulting in the reabsorption of sodium and water, rising aldosterone and ADH levels and causing arteriolar vasoconstriction. These mechanisms initially maintain cardiac output via increased filling pressures, but they ultimately result in increasing volume expansion overwhelming the Frank-Starling mechanism.
ACE inhibitors (ACEi) are recommended as first-line treatment (see table 4) demonstrating overall reductions in mortality of ~23% and of worsening symptoms by ~35% compared with placebo.12–14 Some patients cannot tolerate ACEi (most commonly due to a dry cough). Angiotensin II receptor blockers (ARBs)have been used as second-line agents due to less robust mortality data from clinical trials15 but in the modern era conversion to sacubitril/valsartan should be considered before resorting to use of ARB alone.
Table 4.
ACEi indicated in HFrEF
| ACEi | Initiation dose (mg) | Target dose (mg) |
| Captopril | 6.25 three times a day | 50 three times a day |
| Enalapril | 2.5 two times a day | 20 two times a day |
| Lisinopril | 2.5 once a day | 35 once a day |
| Ramipril | 1.25 once a day | 10 once a day |
| Trandolapril | 0.5 once a day | 4 once a day |
ACEi, ACE inhibitor; HFrEF, heart failure with reduced ejection fraction.
Combined ARB+ARNI therapy with sacubitril/valsartan (Entresto) has more recently demonstrated superiority to ACEi in well-treated patients with HFrEF. Sacubitril inhibits neprilysin, which is responsible for the breakdown of natriuretic peptides, thus increasing circulating levels and promoting natriuresis and the other positive effects of BNP described above. Sacubitril/valsartan has a 16% relative risk reduction in mortality compared with enalapril and guidelines recommend switching from ACEi/ARB to ARNI in ongoing HFrEF despite optimal therapy. Combination therapy with ACEi and ARNI is contraindicated due to a risk of angioedema, and a washout period of at least 36 hours between the last ACEi dose and first ARNI dose is mandated. Otherwise, the side-effect profile is similar to ACEi but with higher rates of symptomatic hypotension (the most common problem observed in clinical practice) and the potential for over-diuresis. Most often the effects of sacubitril/valsartan are beneficial, and many report rapid symptomatic and quality of life benefits. In addition, the incidence of cough, hyperkalaemia and elevated creatinine are all lower in patients on Entresto than those on ACEi.16
At present, it is a common practice to establish patients on ACEi/ARB and the other three pillars of heart failure therapy prior to switching to ARNI in those who do not respond (in line with NICE guidelines). This is driven by the cost-effectiveness of this strategy. The data for superiority of ARNI are convincing and in territories where NICE guidelines do not determine funding arrangements, the practice of using ARNI as first-line therapy is becoming more common. Further data and cost-effective analysis in this area is needed to inform a more uniform approach.
Pillar 2: mineralocorticoid receptor antagonism
MRAs block the effects of aldosterone, which ordinarily promotes salt and water retention and has direct profibrotic effects on the myocardium. Spironolactone and eplerenone both reduce relative mortality in HFrEF by ~30% when added to ACEi.17 18 Spironolactone is a broad-spectrum mineralocorticoid blocker with side effects relating to its antiandrogen property—particularly in men. It is also an effective antihypertensive agent and can be prescribed with dual indication. Eplerenone is a specific aldosterone blocker so is better tolerated, particularly in males and in those with lower blood pressure. Eplerenone specifically hasbeen shown to reduce mortality in patients with heart failure after myocardial infarction. MRAs (acting as potassium sparing diuretics) can be useful to prevent hypokalaemia but are contraindicated in those with hyperkalaemia and monitoring of electrolytes is essential.
Pillar 3: Antagonism of the sympathetic system with selected beta-blockers
Sympathetic overactivity is a hallmark of HFrEF. Increased peripheral vasoconstriction and elevated heart rates attempt to maintain cardiac output and vital organ perfusion but are ultimately maladaptive. It may worsen myocardial ischaemia, and high catecholamine levels may increase myocyte automaticity, increasing the risk of malignant ventricular arrhythmia. The use of selected βB is, therefore, recommended for HFrEF (table 5) and results in a relative mortality reduction of 35% when compared with placebo.19 20
Table 5.
Beta-blockers indicated in HFrEF
| Beta-blocker | Initiation dose (mg) | Target dose (mg) |
| Bisoprolol | 1.25 once daily | 10 once daily |
| Carvedilol | 3.125 two times a day | 25–50 two times a day* |
| Metoprolol succinate (CR/XL)† | 12.5 once daily | 200 once daily |
| Nebivolol | 1.25 once daily | 10 once daily |
*50 mg two times a day if weight >85 kg.
†Extended-release preparations not available in the UK—no data to support the use of standard-release preparations of metoprolol tartarate.
HFrEF, heart failure with reduced ejection fraction.
The use of βB may worsen acute heart failure and so clinical assessment is required to ensure that the patient with HFrEF is not decompensated at the time of βB initiation. Patients may often feel less well for 48–72 hours following initiation of βB or dose escalation and they should be warned of this to improve compliance with life-saving therapy. Where patients with HFrEF have decompensated on stable doses of βB, they should be continued at the same dose, while managing the decompensation. Dose titration should be to the maximum tolerated (starting at low dose) with a target resting heart rate of 60–70 bpm in sinus rhythm. Use of βB in patients with HFrEF with AF is recommended, although prognostic benefits are less well proven and aggressive rate control does not appear to provide any significant benefits when compared with more modest rate control. Some patients may not tolerate βB at higher doses and where the heart rate remains above 70 bpm then the I f channel blocker, Ivabradine, may be used to slow the sinus rate and improve symptoms and mortality.21
Pillar 4: Sodium–glucose cotransporter 2 inhibitors
SGLT2i are well-established hypoglycaemic agents used in the management of type II diabetes. These promote glycosuria and natriuresis by reducing reuptake of glucose and sodium in the proximal renal tubule. Recent evidence has established this class of medication as a key therapy in HFrEF. Both dapagliflozin and empagliflozin have demonstrated ~25% relative risk reduction when compared with placebo in a combined endpoint of worsening heart failure or cardiovascular death in otherwise well-treated patients with HFrEF, both with and without diabetes.22 23 Current ACC/AHA and ESC guidelines strongly support the use of SGLT2i at an early stage in HFrEF and they are approved for use in the UK by NICE. There is a potential for over-diuresis with concomitant use of ARNI and loop diuretic and careful clinical assessment is required in these circumstances.22
From a practical perspective, starting four drugs simultaneously in a patient group who often have significant comorbidity or frailty can be challenging. An approach which concentrates on the phenotype of the individual patient with the goal to establish the four pillars of treatment as rapidly as possible should be the ambition for all individuals with HFrEF. This underscores the pivotal role of the heart failure nurse specialist who can support and educate the patient, their caregivers and the general practitioner through this process and the necessary follow-up and monitoring after each titration. Side effects and complications are commonly encountered and if these occur without ready access to advice, cessation or delays in therapy are very likely.
Adjunctive therapies and the impact of comorbidity
Comorbidities are common in a patient with HFrEF24 and their management should be optimised alongside initial heart failure therapy.
Cardioselective βB are safe to prescribe in all patients with chronic obstructive pulmonary disease.25
ACEi are generally recommended where renal dysfunction complicates HFrEF. Advice from a renal physician in cases of significant chronic kidney disease is often helpful. Where ACEi cannot be used due to concerns over renal dysfunction, then the combination of a nitrate and hydralazine has some evidence for benefit.
A direct oral anticoagulant will generally be recommended in all cases of HFrEF complicated by AF. Restoration of sinus rhythm may confer benefit in HFrEF but this remains a controversial area. Cardioversion, often facilitated by amiodarone, may be considered to improve symptoms. Dronedarone and flecainide should be avoided. Catheter ablation may have a role in improving prognosis but data remain conflicted and careful patient selection by an appropriate multidisciplinary team (MDT) review is recommended.
Digoxin can be useful in addition to βB to improve rate control in AF particularly in less ambulant patients. It can also be used (even in sinus rhythm) in those who remain symptomatic despite OMT where even 62.5 μg once daily can give some symptomatic relief and is associated with a reduction in hospitalisation.26
Device therapy
Patients with HFrEF are at increased risk of death from both progressive pump failure and sudden arrhythmia. The risk of sudden cardiac death is influenced by ejection fraction, ischaemic aetiology, scar burden, age and gender.
Preventing sudden cardiac death
Implanted cardioverter defibrillator (ICD) therapy can abort sudden cardiac death via rapid detection and treatment of malignant ventricular arrhythmia. Such devices are recommended for ‘primary prevention’ where overall prognosis is otherwise estimated to be at least 1 year and LVEF is <35% despite best-tolerated medical therapy with ACEi, βB and MRA (figure 5).27 ICDs can be delivered transvenously or subcutaneously.
Figure 5.

UK NICE decision grid regarding device therapy in individuals with HFrEF according to NYHA class and QRS duration. Reproduced with the NICE UK Open Content licence. CRT, cardiac resynchronisation therapy; CRT-D, cardiac resynchronisation therapy defibrillator; ICD, implanted cardioverter defibrillator; CRT-P, cardiac resynchronisation therapy pacemaker; NICE, National Institute for Health and Care Excellence.
Preventing pump failure
Cardiac resynchronisation therapy (CRT) can be delivered as a pacing system alone (CRT-P) or combined with an ICD (CRT-D). The procedure involves delivering an LV lead via the coronary sinus. A QRS duration of greater than 140 ms on the resting ECG is a strong predictor of response to CRT in terms of improvement in symptoms, prevention of heart failure admissions and improved prognosis.28 Correction of dyssynchrony is a complex phenomenon and dependent on multiple factors, including LV and RV lead position, as well as optimum device programming. All patients with HFrEF with prolonged QRS should be considered for CRT±ICD. Consensus statements recommend the use of CRT earlier in the heart failure pathway and consider it as complementary to medical therapy if dyssynchrony is significant.
Remote monitoring
All commercially available implanted devices have the capacity to monitor various physiological parameters (including daytime and nocturnal heart rate, patient activity levels, burden of arrhythmia and measures of thoracic impedance, etc). Various algorithms have been developed in an effort to support the management of patients with HFrEF—principally by trying to alert the clinical team to potential decompensation. Such data are routinely available and individual heart failure teams should develop their own approach to managing these due to an absence of robust data for overall clinical benefit.
The Cardiomems system is a unique implanted pulmonary artery pressure monitoring system, which allows for evidence-based, goal-directed treatment of the patient with highly symptomatic (NYHA class III) heart failure. By monitoring trends in pulmonary artery diastolic pressure over time, and adjusting therapy accordingly, admissions are avoided.29 The system is widely used in North America, and NICE has recently updated its guideline and it can now be used in clinically indicated patients in the UK.
Supported self-management and cardiac rehabilitation
Integrated heart failure teams are key to supporting the best possible management of the patient with HFrEF. Data are widely available for the importance of heart failure specialist nurses and cardiologists leading MDTs to ensure that individual patients get access to the best management.30 Education around the syndrome of HFrEF for patients and their carers allows them to understand the reality of living with heart failure. The benefits of cardiac rehabilitation and exercise training in HfrEF are well established, and all patients should be referred to an appropriate programme, although provision in the UK remains suboptimal and should be a key focus for newly established integrated care systems.31
Advanced therapies and palliative care
Patients deteriorating despite optimal medical and device therapy may follow one of two trajectories. A small group of patients may be eligible for mechanical circulatory support, according to INTERMACS classification, and consideration of cardiac transplantation. Early discussion±referral for specialist assessment at a transplant centre in an appropriate patient should always be considered. Prompts for referral include frequent hospitalisation, worsening symptoms, reduced ability to tolerate medical therapy and requirement for inotropic support.32 Many patients with HFrEF are elderly or will have comorbidity which precludes consideration of cardiac transplantation. These patients require good palliative care, hand-in-hand with their ongoing supported self-management. Experience shows that involvement of these services earlier in the care pathway can be highly beneficial. Recognising the deteriorating patient and developing an appropriate advanced care plan should be the natural progression of care for all members of the wider MDT.33
Future directions
The last 5 years have seen two major new medications added to guideline-directed therapy. In addition, the role and scope of device therapy are evolving in terms of remote monitoring, diagnostics and therapeutics. Despite this there is a considerable unmet need. Heart failure hospitalisation rates are still increasing year on year and the mortality rate remains worse than most cancers. It is clear that further breakthroughs are needed and with them the heart failure MDT will be paramount to deliver increasingly specialised and complex care to a growing population.
Conclusion
We have reviewed the core principles of up-to-date HFrEF management and this is timely with two recent and very significant changes in standard of care (ARNI and SGLT2i) which both represent major advances in the field. The hierarchy of medical treatments for HFrEF is a current area for guideline development in the UK, but the most recent European and North American guidelines are unequivocal in recommending the rapid initiation of all four drug classes (ACEi/ARNI, βB, MRA and SGLT2i) in HFrEF. This highlights the need for integrated heart failure services to be involved in the care of patients with HFrEF from the point at which the syndrome is diagnosed to direct further investigation and optimum management. The misconception among some in the wider cardiology community that heart failure is ‘just four drugs’ needs to be robustly challenged and evidence supports the concept that all patients with HFrEF should have their care directed by a physician with a subspeciality interest in heart failure and involving a wider MDT with heart failure specialist nurses at its core.
Key messages.
Heart failure with reduced ejection fraction is distinct from that of preserved ejection fraction in its therapeutic goals. These are predominated by the four pillars of disease-modifying therapy.
The four pillars consist of ACE inhibitors/sacubitril–valsartan, beta-blockers, mineralocorticoid receptor antagonists and sodium–glucose cotransporter 2 inhibitors.
An approach which concentrates on the phenotype of the individual patient with the goal to establish the four pillars of treatment as rapidly as possible should be employed for all patients with HFrEF.
Heart failure nurse specialists along with involvement of other members of the multidisciplinary team are important to ensure these goals can be met as part of a supported self-management programme.
All patients with HFrEF and who are on optimal medical therapy should be considered for device therapy. Those with a broad QRS are highly likely to benefit from cardiac resynchronisation therapy and many patients stand to benefit from implantable defibrillators.
CME credits for Education in Heart.
Education in Heart articles are accredited for CME by various providers. To answer the accompanying multiple choice questions (MCQs) and obtain your credits, click on the 'Take the Test' link on the online version of the article. The MCQs are hosted on BMJ Learning. All users must complete a one-time registration on BMJ Learning and subsequently log in on every visit using their username and password to access modules and their CME record. Accreditation is only valid for 2 years from the date of publication. Printable CME certificates are available to users that achieve the minimum pass mark.
Footnotes
Twitter: @pmhaydock
Contributors: ASF and PH planned the manuscript equally. PH authored the first draft. ASF contributed to the content and edited manuscript and figures and carried out the submission.
Funding: The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests: None declared.
Provenance and peer review: Commissioned; internally peer reviewed.
Author note: References which include a * are considered to be key references.
Ethics statements
Patient consent for publication
Not required.
Ethics approval
Not applicable.
References
- 1. Zaphiriou A, Robb S, Murray-Thomas T, et al. The diagnostic accuracy of plasma BNP and NTproBNP in patients referred from primary care with suspected heart failure: results of the UK natriuretic peptide study. Eur J Heart Fail 2005;7:537–41. 10.1016/j.ejheart.2005.01.022 [DOI] [PubMed] [Google Scholar]
- 2. Chronic heart failure in adults: diagnosis and management NICE guideline [NG106] 2018. [PubMed]
- 3. Yancy CW, Jessup M, Bozkurt B, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. J Am Coll Cardiol 2017;70:776–803. 10.1016/j.jacc.2017.04.025 [DOI] [PubMed] [Google Scholar]
- 4. Cleland JGF, Swedberg K, Follath F, et al. The EuroHeart Failure survey programme-- a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J 2003;24:442–63. 10.1016/S0195-668X(02)00823-0 [DOI] [PubMed] [Google Scholar]
- 5. Halliday BP, Wassall R, Lota AS, et al. Withdrawal of pharmacological treatment for heart failure in patients with recovered dilated cardiomyopathy (TRED-HF): an open-label, pilot, randomised trial. Lancet 2019;393:61–73. 10.1016/S0140-6736(18)32484-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. American College of Cardiology Foundation Task Force on Expert Consensus Documents, Hundley WG, Bluemke DA, et al. ACCF/ACR/AHA/NASCI/SCMR 2010 expert consensus document on cardiovascular magnetic resonance: a report of the American College of cardiology Foundation Task force on expert consensus documents. Circulation 2010;121:2462–508. 10.1161/CIR.0b013e3181d44a8f [DOI] [PMC free article] [PubMed] [Google Scholar]
- *7. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021;42:3599–726. 10.1093/eurheartj/ehab368 [DOI] [PubMed] [Google Scholar]
- 8. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC)Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J 2016;37:2129–200. 10.1093/eurheartj/ehw128 [DOI] [PubMed] [Google Scholar]
- 9. Gheorghiade M, Pang PS. Acute heart failure syndromes. J Am Coll Cardiol 2009;53:557–73. 10.1016/j.jacc.2008.10.041 [DOI] [PubMed] [Google Scholar]
- *10. Mullens W, Damman K, Harjola V-P, et al. The use of diuretics in heart failure with congestion - a position statement from the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2019;21:137–55. 10.1002/ejhf.1369 [DOI] [PubMed] [Google Scholar]
- 11. Clark AL, Kalra PR, Petrie MC, et al. Change in renal function associated with drug treatment in heart failure: national guidance. Heart 2019;105:904. 10.1136/heartjnl-2018-314158 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. The Consensus Trial Study Group* . Effects of enalapril on mortality in severe congestive heart failure. N Engl J Med 1987;316:1429–35. 10.1056/NEJM198706043162301 [DOI] [PubMed] [Google Scholar]
- 13. Pfeffer MA, Braunwald E, Moyé LA, et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med 1992;327:669–77. 10.1056/NEJM199209033271001 [DOI] [PubMed] [Google Scholar]
- 14. Anon . Effect of ramipril on mortality and morbidity of survivors of acute myocardial infarction with clinical evidence of heart failure. the acute infarction ramipril efficacy (AIRE) study Investigators. Lancet 1993;342:821–8. [PubMed] [Google Scholar]
- 15. Granger CB, McMurray JJV, Yusuf S, et al. Effects of candesartan in patients with chronic heart failure and reduced left-ventricular systolic function intolerant to angiotensin-converting-enzyme inhibitors: the CHARM-Alternative trial. Lancet 2003;362:772–6. 10.1016/S0140-6736(03)14284-5 [DOI] [PubMed] [Google Scholar]
- 16. McMurray JJV, Packer M, Desai AS, et al. Angiotensin–neprilysin inhibition versus enalapril in heart failure. N Engl J Med 2014;371:993–1004. 10.1056/NEJMoa1409077 10.1056/NEJMoa1409077 [DOI] [PubMed] [Google Scholar]
- 17. Pitt B, Zannad F, Remme WJ, et al. The effect of spironolactone on morbidity and mortality in patients with severe heart failure. N Engl J Med Overseas Ed 1999;341:709–17. 10.1056/NEJM199909023411001 [DOI] [PubMed] [Google Scholar]
- 18. Zannad F, McMurray JJV, Krum H, et al. Eplerenone in patients with systolic heart failure and mild symptoms. N Engl J Med Overseas Ed 2011;364:11–21. 10.1056/NEJMoa1009492 [DOI] [PubMed] [Google Scholar]
- 19. Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. N Engl J Med 1996;334:1349–55. 10.1056/NEJM199605233342101 [DOI] [PubMed] [Google Scholar]
- 20. Anon . The cardiac insufficiency bisoprolol study II (CIBIS-II): a randomised trial. Lancet 1999;353:9–13. 10.1016/S0140-6736(98)11181-9 [DOI] [PubMed] [Google Scholar]
- 21. Swedberg K, Komajda M, Böhm M, et al. Ivabradine and outcomes in chronic heart failure (SHIFT): a randomised placebo-controlled study. Lancet 2010;376:875–85. 10.1016/S0140-6736(10)61198-1 [DOI] [PubMed] [Google Scholar]
- 22. McMurray JJV, Solomon SD, Inzucchi SE, et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019;381:1995–2008. 10.1056/NEJMoa1911303 [DOI] [PubMed] [Google Scholar]
- 23. Packer M, Anker SD, Butler J, et al. Empagliflozin in Patients With Heart Failure, Reduced Ejection Fraction, and Volume Overload: EMPEROR-Reduced Trial. J Am Coll Cardiol 2021;77:1381–92. 10.1016/j.jacc.2021.01.033 [DOI] [PubMed] [Google Scholar]
- 24. Nieminen MS, Brutsaert D, Dickstein K, et al. EuroHeart failure survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J 2006;27:2725–36. 10.1093/eurheartj/ehl193 [DOI] [PubMed] [Google Scholar]
- 25. Gulea C, Zakeri R, Alderman V, et al. Beta-blocker therapy in patients with COPD: a systematic literature review and meta-analysis with multiple treatment comparison. Respir Res 2021;22:64. 10.1186/s12931-021-01661-8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Group, T. D. I . The effect of digoxin on mortality and morbidity in patients with heart failure. N Engl J Med 1997;336:525–33. 10.1056/NEJM199702203360801 [DOI] [PubMed] [Google Scholar]
- 27. Implantable cardioverter defibrillators and cardiac resynchronisation therapy for arrhythmias and heart failure Technology appraisal guidance [TA314].
- 28. Cleland JG, Abraham WT, Linde C, et al. An individual patient meta-analysis of five randomized trials assessing the effects of cardiac resynchronization therapy on morbidity and mortality in patients with symptomatic heart failure. Eur Heart J 2013;34:3547–56. 10.1093/eurheartj/eht290 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Abraham WT, Adamson PB, Bourge RC, et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011;377:658–66. 10.1016/S0140-6736(11)60101-3 [DOI] [PubMed] [Google Scholar]
- 30. Morton G, Masters J, Cowburn PJ. Multidisciplinary team approach to heart failure management. Heart 2018;104:1376–82. 10.1136/heartjnl-2016-310598 [DOI] [PubMed] [Google Scholar]
- 31. UK National heart failure audit, 2019. Available: https://www.nicor.org.uk/national-cardiac-audit-programme/heart-failure-heart-failure-audit/
- *32. Banner NR, Bonser RS, Clark AL, et al. UK guidelines for referral and assessment of adults for heart transplantation. Heart 2011;97:1520–7. 10.1136/heartjnl-2011-300048 [DOI] [PubMed] [Google Scholar]
- *33. McIlvennan CK, Allen LA. Palliative care in patients with heart failure. BMJ 2016;353:i1010. 10.1136/bmj.i1010 [DOI] [PubMed] [Google Scholar]
- 34. Shah . Clinical magnetic resonance imaging. 3rd ed. New York: Elsevier Press, 2005. [Google Scholar]