

Abstract
Colorectal carcinoma (CRC) rarely metastasizes to the urinary system in isolated form. It usually spreads through direct invasion with intra-ureteric growth or local ureter mucosal metastasis without involving the muscular layer. We present a case of a 63-year-old man who came with uraemic symptoms and a ballotable right kidney. Laboratory and imaging showed acute renal failure with right renal mass suspicious of malignancy and left ureteric stricture causing hydronephrosis. He underwent right radical nephrectomy and left open ureteric stenting plus biopsy sampling. Adenocarcinoma was detected through the evaluation of the specimen. In view that adenocarcinoma rarely occurs in the urinary system, an investigation was carried out to search for the primary source. Colonoscopy was performed, which later showed adenocarcinoma of the rectum. Adenocarcinoma in the renal system should always raise the suspicion of another primary source of malignancy, especially colorectal origin. The advanced stage of this cancer should be managed with the best palliative treatment rather than aggressive surgical intervention.
Keywords: Colorectal carcinoma, Metastasis, Adenocarcinoma, Renal, Ureter
INTRODUCTION
Colorectal carcinoma (CRC) is among the top 3 commonest malignancies in Malaysia and the 3rd leading cause of cancer death.1 Some patients present in the early stage while others present in the advanced stage with distant metastasis. Hematogenous spread to the liver, lung, and bone is the most commonly described route of metastasis. Extremely rare isolated urinary system metastasis of CRC had been reported before.2 The usual course of metastasis to other retroperitoneal organs, including kidneys and ureters, is either through direct invasion or invasion into the bladder and propagate via ureter up.
CASE REPORT
We report a case of rectal adenocarcinoma with isolated metastasis to the right kidney and bilateral ureters. A 63-year-old man initially presented with symptoms of acute renal failure, which required urgent hemodialysis support. His kidney failure was attributed to obstructive uropathy with the evidence of bilateral hydronephrosis and right renal mass from an ultrasound scan. Emergency contrast-enhanced computed tomography urogram was done, showing a right renal mass (size 7.0 × 8.3 cm) suspicious of renal cell carcinoma (RCC) (Figure 1a) and left proximal hydroureter with enhanced and thickened proximal ureteric wall with an area of strictures suggestive of ureteritis (Figure 1b). Cystourethroscopy, left retrograde-pyelography, and ureteric stenting were attempted but failed. Hence, a left nephrostomy was inserted. Unfortunately, his kidney function did not improve, and he still required regular hemodialysis. Since there was no interventional radiologist or urologist available, antegrade stenting was not offered.
Fig. 1:
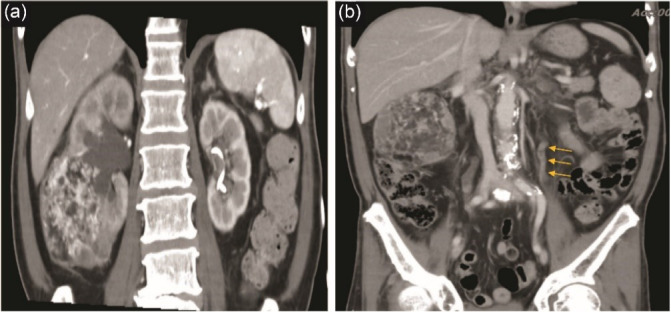
(a) Right heterogenous enhancing renal mass at the lower pole. Left Kidney post nephrostomy insertion; (b) Left proximal ureteric wall thickening and enhancement with area of narrowing suggestive of stricture.(arrow)
Right radical nephrectomy and left open ureteric stenting were carried out by the general surgeon with the impression of right RCC and bilateral ureteric stricture secondary to ureteritis. Intraoperatively, a left open ureterostomy was performed for antegrade stenting of the left ureter. However, during ureterostomy, we noticed whitish tissue-like structures coming out from the lumen, which was sampled and sent for histopathological examination (HPE). A left ureteric stent was then successfully inserted, bypassing the stricture site. To our surprise, the HPE and immunohistochemistry (IHC) results came back as adenocarcinoma on both the right kidney specimen and left ureteric tissue biopsy (Figure 2a and 2b). Adenocarcinoma is almost impossible to arise from the kidney and very rarely in the ureter. It is only present in 0.5-2.5% of all ureter carcinomas.3 These findings led us to further investigate the primary tumor. Evaluations for tumor markers were requested, which all were reported as normal. A pan-endoscopy examination was done for him. A histologically proven adenocarcinoma of rectal mass was found during colonoscopy, which was believed to be the primary tumor. The patient refused further treatment, and unfortunately, he succumbed to his illness six months later.
Fig. 2:
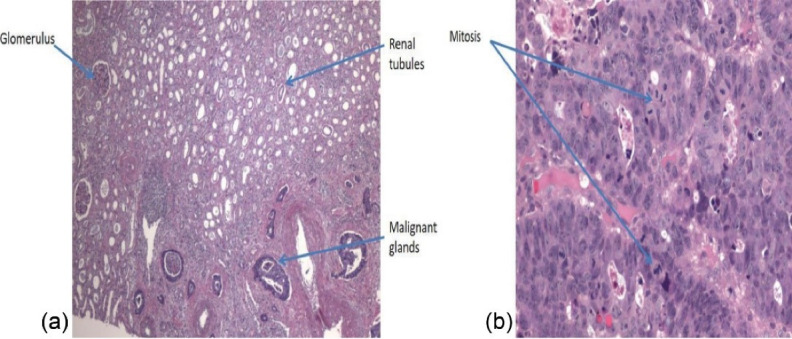
(a) HPE right nephrectomy specimen showing malignant gland resembling adenocarcinoma in kidney parenchymal; (b) HPE from the ureter biopsy showing malignant gland suggestive of adenocarcinoma.
DISCUSSION
The prognosis of patients with metastatic CRC has improved substantially over the last few decades. It comes with a price that more unusual sites of metastasis are seen, which include isolated urinary system metastasis. Isolated kidney and ureter metastasis is a very rare entity. Up to date, only 20 cases have been reported worldwide.2,4-6 It usually occurs through hematogenous spread. They can spread through direct invasion with intra-ureteric growth5,7 or local ureter mucosal metastasis without involving the muscular layer in rare cases.6 They remain asymptomatic and are consistently identified during surveillance computed tomography. For instance, our case is the only few detected on the first presentation. This was attributed to the obstructive uropathy secondary to ureteric stricture caused by bilateral ureteric metastasis. In a case report by Fitch and colleagues,8 ureteric metastasis occurred at different levels like a skip lesion. The uninvolved ureteric wall will undergo ischemic changes and form the stricture. In our case, intraoperatively, there were multifocal skip strictures identified causing difficulty in ureteric stenting, which is similar to the case reported by Fitch et al.8
An imaging conundrum study among secondary tumors in the urinary system was published by Karaosmanoglu and et al.9 He stated that the imaging alone might be challenging in differentiating primary and secondary renal tumors. In a healthy individual with both functioning kidneys, a tumor in one kidney will usually undergo resection for diagnostic and therapeutic purposes without a prior tissue biopsy. It does not always turn out to be a primary renal malignancy. There are possibilities of benign tumor or secondary malignancy similar to the present case. Perhaps imaging can assist in the biopsy of renal tumors for diagnostic purposes prior to the surgery in doubtful cases. HPE and IHC will help to identify whether it is a primary or secondary renal tumor. This will be very helpful in the patient’s treatment plan as primary RCC and selected patients with isolated renal metastatic CRC may benefit from nephrectomy.10 For instance, instead of a surgical approach, palliative chemo or minimally invasive procedures will be a better option for this current case. This might reduce morbidity.
In this case, in view of the radiological diagnosis of RCC, a radical nephrectomy was performed without a prior tissue biopsy for confirmation. Unfortunately, the renal tumor turned out to be a secondary tumor. Based on a few case reports by Melichar and colleagues10 and Nikolaos F and others,6 the most recommended mode of treatment for isolated kidney metastasis is systemic therapy rather than surgery. The decision for nephrectomy should be based on an individual basis and mainly depends on the patient’s expectations.
CONCLUSION
Adenocarcinoma found in the urinary system should be considered a secondary tumor until proven otherwise.3 Therapeutic strategies for patients with CRC and isolated urinary system metastasis should be based on an individual basis. So far, there are not enough cases reported for a large-scale study to identify the best treatment modalities for this group of patients. Based on expert opinion and literature reviews, systemic chemotherapy remains the mainstay of treatment.3
Please cite this paper as: Zhan Huai T, Ramely R, Mohamed Daud MA, Mokhtar MF, Mohammad H, Omar SZ. Isolated renal and ureter metastasis as the first manifestation of rectal adenocarcinoma. Middle East J Dig Dis 2022;14(2):254-257. doi: 10.34172/mejdd.2022.280.
Footnotes
ETHICAL APPROVAL
Written informed consent was obtained from the patient for the publication of any data included in this report.
CONFLICT OF INTEREST
The authors declare no conflict of interest related to this work.
References
- 1.Schliemann D, Paramasivam D, Dahlui M, Cardwell CR, Somasundaram S, Ibrahim Tamin NSB. et al. Change in public awareness of colorectal cancer symptoms following the Be Cancer Alert Campaign in the multi-ethnic population of Malaysia. BMC Cancer. 2020;20(1):252. doi: 10.1186/s12885-020-06742-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Aksu G, Fayda M, Sakar B, Kapran Y. Colon cancer with isolated metastasis to the kidney at the time of initial diagnosis. Int J Gastrointest Cancer. 2003;34(2-3):73–7. doi: 10.1385/ijgc:34:2-3:073. [DOI] [PubMed] [Google Scholar]
- 3.Chaudhary P, Agarwal R, Srinivasan S, Singh D. Primary adenocarcinoma of ureter: a rare histopathological variant. Urol Ann. 2016;8(3):357–9. doi: 10.4103/0974-7796.184885. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Zhou C, Urbauer DL, Fellman BM, Tamboli P, Zhang M, Matin SF. et al. Metastases to the kidney: a comprehensive analysis of 151 patients from a tertiary referral centre. BJU Int. 2016;117(5):775–82. doi: 10.1111/bju.13194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dulskas A, Bagurskas P, Sinkevicius Z, Samalavicius NE. Sigmoid adenocarcinoma with metastases to the kidney: report of a rare case and review of the literature. Oncol Lett. 2015;10(2):1191–3. doi: 10.3892/ol.2015.3290. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Nikolaos F, Panagiotis A, Konstantinos B, Vassilios S, Iraklis P. Distant ureteral metastasis from colon adenocarcinoma: report of a case and review of the literature. Case Rep Urol. 2014;2014:196425. doi: 10.1155/2014/196425. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dräger DL, Protzel C, Erbersdobler A, Hakenberg O. Late recurrence of colorectal adenocarcinoma as a renal tumour by direct spread via the ureter. Ther Adv Urol. 2017;9(5):121–2. doi: 10.1177/1756287217700033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Fitch WP, Robinson JR, Radwin HW. Metastatic carcinoma of the ureter. Arch Surg. 1976;111(8):874–6. doi: 10.1001/archsurg.1976.01360260042010. [DOI] [PubMed] [Google Scholar]
- 9.Karaosmanoglu AD, Onur MR, Karcaaltincaba M, Akata D, Ozmen MN. Secondary tumors of the urinary system: an imaging conundrum. Korean J Radiol. 2018;19(4):742–51. doi: 10.3348/kjr.2018.19.4.742. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Melichar B, Morávek P, Ferko A, Podhola M. Metastatic colorectal carcinoma and kidney tumors: a report of four cases. Tumori. 2010;96(3):483–6. doi: 10.1177/030089161009600318. [DOI] [PubMed] [Google Scholar]