

Sacubitril/valsartan was recently approved for the treatment of Heart Failure with Preserved Ejection Fraction (HFpEF). Although sacubitril/valsartan did not significantly reduce HF hospitalizations or deaths overall, a significant benefit in women was observed1. Characterization of sacubitril/valsartan response molecular biomarkers in patients with HFpEF and the mechanism underlying sex-biased response has not been described.
To address these knowledge gaps, we performed proteomic profiling for 369 plasma proteins using the Olink Cardiometabolic platform in 37 patients (males=18; females=19) prior to and 5 weeks after sacubitril/valsartan treatment. Patients’ age was 74 ± 7.6 years (males 74.1 ± 7.6; females 74.2 ± 7.7), mean left ventricular ejection fraction (LVEF) 59.7 ± 5.7% with no significant difference between males (58.3 ± 6.0%) and females (61.1 ± 4.8%) (P=0.16). Co-morbidities included hypertension, diabetes mellitus, atrial fibrillation, stroke, ischemic heart disease, and 12-month prior HF hospitalization in 89%, 43%, 73%, 8%, 27%, and 54% of patients, respectively. This study was approved by the Mayo Clinic Institutional Review Board. Data is available upon reasonable request to the corresponding author.
We performed a clinical assay (Electrochemiluminescence Immunoassay) for plasma NT-proBNP and found that sacubitril/valsartan treatment in the overall cohort resulted in a significant reduction in NT-proBNP (P=0.0013, N=37, average reduction=26%) (Figure A). We then obtained Normalized Protein Expression (NPX), a relative protein quantification logarithmically transformed for a more normal distribution, for 369 proteins from Olink. Fourteen proteins significantly changed after drug treatment base on paired student’s t-test at a 5% false discovery rate (Figure B). Nine of these 14 molecules were involved in the TGF-β signaling pathway. The most significantly upregulated molecule, CHRDL2, is an antagonist of TGF-β signaling, while the most significantly down-regulated molecule, ENG, and 7 other down-regulated molecules, IGFBP7, TGFBI, CD16, CDH6, ICAM5, NT-proBNP, and ST2, were activating factors of or molecules induced by TGF-β. This observation suggested that sacubitril/valsartan systematically dampened TGF-β signaling in our overall HFpEF cohort.
Proteomic profiling of HFpEF patients prior to and after 5 weeks of sacubitril/valsartan treatment.
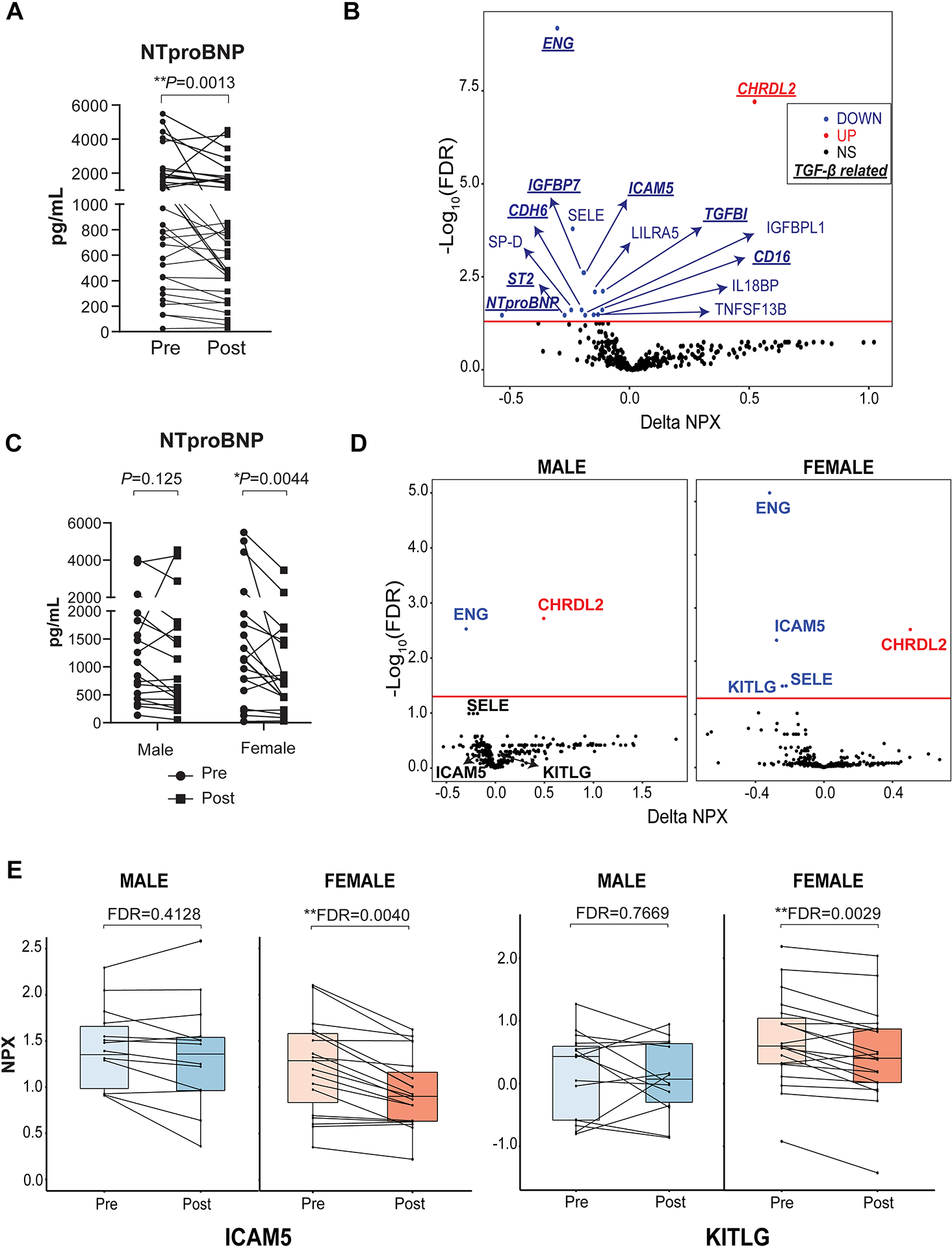
(A) Plasma level of NTproBNP in all patients before and after drug treatment measured by standard clinical electrochemiluminescence immunoassay. P-value reflected paired t-test of log2-transformed values. (B) Volcano plot of proteomic changes before and after 5 weeks of sacubitril/valsartan treatment (paired student’s t-test with Benjamini–Hochberg multiple comparison correction. All proteomic analyses were done with R version 4.1.1). Y axis represents -log 10 of false discovery rate (FDR). X axis represents Normalized Protein Expression (NPX) change. Red line in the plot represents significant cutoff at 5% FDR. (C) Plasma level of NTproBNP in female and male patients before and after drug treatment measured by standard clinical electrochemiluminescence immunoassay (P-value reflected paired t-test of log2-transformed values). (D) Volcano plot of changes before and after 5 weeks of sacubitril/valsartan treatment stratified by sex (paired student’s t-test with Benjamini–Hochberg multiple comparison correction). Y axis represents -log10 of FDR. X axis represents NPX change. Red line in the plot represents significant cutoff at 5% FDR. Because SELE showed a trend of being changed by sacubitril/valsartan in male patients, it was conservatively not considered female-specific response and not discussed in the main text. (E) Two proteins changed after sacubitril/valsartan treatment that were female specific. Each dot represents a patient.
We further stratified the samples by sex and conducted paired t-tests separately in men and women. There was no statistically significant difference (P=0.1445) between the downregulation of plasma NT-proBNP observed in women (−35%, N=19) and that observed in men (−16%, N=18) even though the downregulation was qualitatively more significant in women (Figure C). Additionally, soluble ICAM-5 and KITLG were more significantly down-regulated in women than in men (Figure D&E). Because females had larger and more consistent NT-proBNP reductions than males in our cohort, the differentially expressed proteins observed could be associated with NT-proBNP rather than sex. To test for sex-specific effect directly for these molecules, we ran a generalized linear model for post-treatment NPX with pre-treatment NPX, sex and NTproBNP level as predictor variables. Post-treatment NT-proBNP was not significantly associated with neither ICAM5 (P=0.0971) nor KITLG (P=0.793). Sex was a significant predictor for post-treatment ICAM5 levels (P= 0.0314) but was not for KITLG levels (P= 0.649), suggesting that the difference in statistical significance between men and women of the KITLG change is hypothesis-generating and would require validation in a larger sample. ICAM5 is highly expressed in brain and lung tissue, while KITLG is highly expressed in fibroblasts, gut and lung tissue (see https://gtexportal.org/). ICAM5 increases TGF-β1 expression in activated T-cells2, while KITLG is a cytokine that is upregulated in adverse left ventricular remodeling3. The mechanisms underlying the downregulation of these molecules in women but not in men and its association with therapeutic benefits in HFpEF with sacubitril/valsartan treatment remain to be determined.
To our knowledge this is the first reported plasma proteomic profiling of sacubitril/valsartan response in patients with HFpEF. Our findings indicate that sacubitril/valsartan’s mechanism of action in HFpEF may be mediated primarily via the TGF-β pathway. Of interest, TGF-β is a biomarker that differentiates HFpEF from other types of HF4, further supporting the observation that molecular mechanisms affected by sacubitril/valsartan are possibly targets of known HFpEF pathophysiology. Additionally, we observed that NT-proBNP was reduced in the overall cohort but more significantly in female than in male patients. The extent to which NT-proBNP decreases after sacubitril/valsartan treatment has been shown to predict risk for subsequent HF hospitalization and cardiovascular death5 and therefore our findings may provide a potential explanation for the beneficial effect of sacubitril/valsartan in females but not in males when treated for HFpEF. Correlated with this sex-mediated response, ICAM5, and possibly KITLG were identified to be downregulated by sacubitril/valsartan more significantly in females than males, possibly explaining its beneficial mechanism of action in females. Our findings provide new insights into mechanisms underlying sacubitril/valsartan action in HFpEF. Validation in larger sample sizes especially to detect smaller changes in protein markers, untargeted proteome analysis and mechanistic functional work are needed to determine if knowledge of the reported molecules and/or pathways could contribute to the precision treatment of HFpEF, particularly for women who are at higher risk for this disease.
Sources of Funding
This study was supported in part by the National Institute on Aging Grant R21AG53512 (NLP) and the Mayo Clinic Graduate School of Biomedical Sciences Fellowship (TTLN).
Abbreviations:
- HFpEF
Heart Failure with Preserved Ejection Fraction
- LVEF
Left Ventricular Ejection Fraction
- NPX
Normalized Protein Expression
Footnotes
Disclosure
Richard Weinshilboum is co-founder of and stockholder in OneOme, LLC. Other authors declared no conflict of interest
References
- 1.McMurray JJV, Jackson AM, Lam CSP, Redfield MM, Anand IS, Ge J, Lefkowitz MP, Maggioni AP, Martinez F, Packer M, Pfeffer MA, Pieske B, Rizkala AR, Sabarwal SV, Shah AM, Shah SJ, Shi VC, van Veldhuisen DJ, Zannad F, Zile MR, Cikes M, Goncalvesova E, Katova T, Kosztin A, Lelonek M, Sweitzer N, Vardeny O, Claggett B, Jhund PS and Solomon SD. Effects of Sacubitril-Valsartan Versus Valsartan in Women Compared With Men With Heart Failure and Preserved Ejection Fraction: Insights From PARAGON-HF. Circulation. 2020;141:338–351. [DOI] [PubMed] [Google Scholar]
- 2.Tian L, Lappalainen J, Autero M, Hanninen S, Rauvala H and Gahmberg CG. Shedded neuronal ICAM-5 suppresses T-cell activation. Blood. 2008;111:3615–25. [DOI] [PubMed] [Google Scholar]
- 3.McCutcheon K, Dickens C, van Pelt J, Dix-Peek T, Grinter S, McCutcheon L, Patel A, Hale M, Tsabedze N, Vachiat A, Zachariah D, Duarte R, Janssens S and Manga P. Dynamic Changes in the Molecular Signature of Adverse Left Ventricular Remodeling in Patients With Compensated and Decompensated Chronic Primary Mitral Regurgitation. Circ Heart Fail. 2019;12:e005974. [DOI] [PubMed] [Google Scholar]
- 4.Bielecka-Dabrowa A, Sakowicz A, Misztal M, von Haehling S, Ahmed A, Pietrucha T, Rysz J and Banach M. Differences in biochemical and genetic biomarkers in patients with heart failure of various etiologies. Int J Cardiol. 2016;221:1073–80. [DOI] [PubMed] [Google Scholar]
- 5.Cunningham JW, Vaduganathan M, Claggett BL, Zile MR, Anand IS, Packer M, Zannad F, Lam CSP, Janssens S, Jhund PS, Kober L, Rouleau J, Shah SJ, Chopra VK, Shi VC, Lefkowitz MP, Prescott MF, Pfeffer MA, McMurray JJV and Solomon SD. Effects of Sacubitril/Valsartan on N-Terminal Pro-B-Type Natriuretic Peptide in Heart Failure With Preserved Ejection Fraction. JACC Heart Fail. 2020;8:372–381. [DOI] [PubMed] [Google Scholar]