

I. INTRODUCTION
Accurate head impact kinematic data are required to further the understanding of repetitive head impact exposure in sports. Several laboratory studies have evaluated multiple sensors for the same impacts to anthropomorphic test device (ATD) headforms [1–2]. Linear acceleration is transformed to the centre of gravity of the 50th percentile male headform, but the validity of such a transformation for female youth athletes is unknown. Wu, et al. [3] compared the sensor-to-skull coupling of an instrumented mouthguard, skin patch and skullcap sensors for a human subject during soccer heading using high-speed video tracking. It was found that the skullcap overestimated the peak head accelerations, which was attributed to poor skull coupling and out-of-plane motion. Only one study has compared two sensors in live sport [4], which found that the Head Impact Telemetry System (HITS) recorded higher peak linear acceleration and lower peak angular acceleration values compared to an instrumented mouthguard. The aim of the current study was to: (a) compare transformations using subject-specific and 50th percentile male anthropometrics and (b) compare head impact kinematics recorded by a headband-mounted sensor to a mouthguard-mounted sensor worn by female high school soccer players during a routine heading drill.
II. METHODS
Soccer Heading Drill
Three female high school athletes completed five soccer headers. An experienced collegiate soccer player performed throw-ins from a distance of 15 m. Athletes were instructed to strike the ball with the forehead to direct the ball back towards the launch location. Head circumference was measured for each athlete with a soft tape measure.
Head impact sensors
Athletes wore both the Triax Smart Impact Sensor (SIM-G) headband and the Stanford mouthguard (MIG). Both sensors use a triaxial accelerometer and gyroscope to measure linear acceleration and angular velocity, respectively. The SIM-G recorded data at 1000 Hz and had a 16 g recording threshold. The MIG recorded linear acceleration and angular velocity at 1000 and 8000 Hz, respectively, and had a 10 g recording threshold.
Geometric Head Kinematic Transformation
SIM-G data were uploaded to the cloud and processed by proprietary manufacturer software, which transformed linear acceleration data from the device location to the centre of gravity of the head using:
| (Equation 1) |
where aCG is linear acceleration of the centre of gravity of the head, aS is linear acceleration of the sensor, ω is angular velocity recorded by the sensor, ώ is angular acceleration recorded by the sensor and r is the distance between the sensor and the centre of gravity of the head for the 50th percentile male. Resultant linear acceleration and angular velocity were calculated from axis-specific data. Angular acceleration was calculated; however, given the errors associated with numerical differentiation of gyroscopic impact data [5], only angular velocity was analysed in the current study.
For the MIG transformation, raw linear acceleration and angular velocity data were filtered at 160 Hz using a 4th order low-pass Butterworth filter as per SAE J211 [6]. Angular acceleration was derived from angular velocity using the five-point stencil method. Transformations were performed using Equation 1 for all data points. The result was again passed through the same Butterworth filter. The MIG sensor is located at the front centre of the mouthguard. The position vector (−78, 0, 72 mm) to the 50th percentile male and head circumference measurements were used to scale the position vector for subject-specific transformations.
Data Analysis
Paired Student’s t-tests were used to compare head impact sensor kinematics from subject-specific and 50th percentile male transformation functions. Similarly, head impact sensor kinematics were compared for the same trials between sensors using a paired Student’s t-test.
III. INITIAL FINDINGS
A total of 15 soccer headers, completed by three female athletes, were studied. The MIG mouthguard and headband-mounted SIM-G recorded 10 and 12 headers, respectively. There were nine headers with data from both devices. Some headers may not have been recorded because the sensor linear acceleration threshold (MIG, 10 g, SIM-G, 16 g) to trigger a recording was not reached.
For mean peak linear acceleration recorded by the MIG, no significant difference was found between the transformation using anthropometrics from the 50th percentile male (20.2 ± 4.5 g) and individualised athlete anthropometrics (19.9 ± 4.1 g, p=0.21). Head circumference was measured as 5–10% less than the 50th percentile male, which resulted in a mean difference of 2% peak linear acceleration.
The SIM-G recorded significantly higher peak linear accelerations (29.7 ± 6.6 g) than the MIG (20.2 ± 4.8 g, p=0.008), but angular velocity measurements did not differ (SIM-G: 10.8 ± 4.0 rad/s, MIG: 10.5 ± 3.2 rad/s, p=0.85). The SIM-G and MIG devices did not correlate for peak linear accelerations (p=0.99, Fig. 1, left) or peak angular velocities (p=0.75, Fig. 1, right).
Fig. 1.
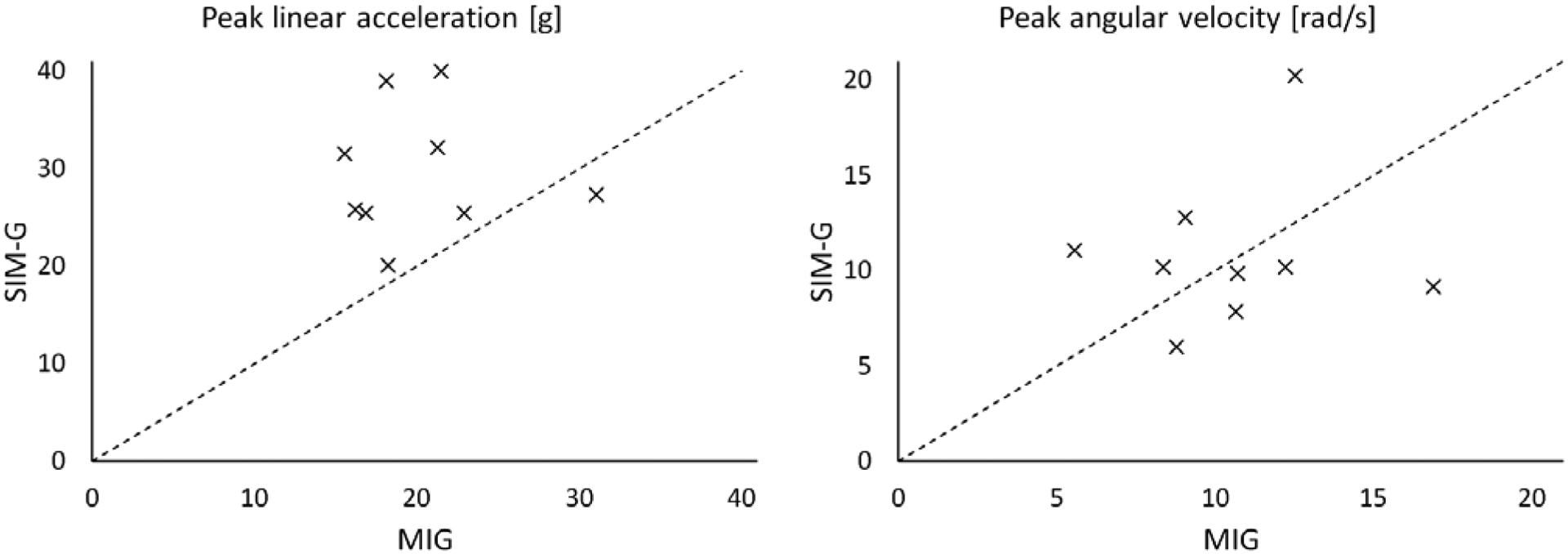
Peak linear accelerations (left) and peak angular velocities (right) from SIM-G and MIG devices. Dashed line represents equivalence.
IV. DISCUSSION
Linear acceleration transformations only differed by 2% for youth female athletes compared to the 50th percentile adult male. However, sample size was a limitation in the current study. Larger studies will be needed to confirm results in a larger sample size and to investigate the error in younger athletes.
The headband-mounted SIM-G device recorded significantly higher peak linear accelerations compared to the MIG instrumented mouthguard, which supported a laboratory study of the SIM-G using an ATD headform that reported overestimations of peak linear acceleration. Such findings were attributed to the poor sensor-skull coupling of the headband [3]. Peak angular velocities did not differ significantly between the SIM-G and MIG, however there was poor correlation between the sensors.
Acknowledgements:
The current study was funded by the Pennsylvania Department of Health and the National Institute of Neurologic Disorders and Stroke of the National Institutes of Health (R01NS097549). The content of this systematic review is solely the responsibility of the authors and does not necessarily represent the official views of the Pennsylvania Department of Health and/or the National Institutes of Health.
Contributor Information
Declan A. Patton, Center for Injury Research and Prevention, Children’s Hospital of Philadelphia in Philadelphia, PA.
Colin M. Huber, University of Pennsylvania in Philadelphia, PA.
Kristy B. Arbogast, Co-Scientific Director of the Center for Injury Research and Prevention, Children’s Hospital of Philadelphia and a Professor at the University of Pennsylvania in Philadelphia, PA.
V. REFERENCES
- [1].Cummiskey, et al. , J Sports Eng Tech, 2017. [Google Scholar]
- [2].Tyson, et al. , J Appl Biomech, 2018. [DOI] [PubMed] [Google Scholar]
- [3].Wu, et al. , Ann Biomed Eng, 2016. [Google Scholar]
- [4].Shah, et al. , IRCOBI, 2019. [Google Scholar]
- [5].Bussone WR, et al. , SAE Int J Trans Safety, 2017. [Google Scholar]
- [6].SAE International, J211–1, 2014. [Google Scholar]