

Abstract
We performed distal bypass and free flap transfer in a single-stage operation to repair an extensive soft tissue defect in an ischemic foot of an 84-year-old woman. The nutrient artery of the free flap was anastomosed to the bypass graft in an end-to-side manner. Subsequently, the bypass graft became occluded on several occasions. Although intravascular and surgical interventions were performed each time, the bypass graft eventually became completely occluded. However, despite late occlusion of the nutrient artery, the free flap has remained viable and the patient is ambulatory. The time required for a transplanted free flap to become completely viable without a nutrient artery is likely longer for an ischemic foot compared with a healthy foot. However, the exact period of time required is not known. A period of month was required in our patient. We report this case to help clarify the process by which a free flap becomes viable when applied to an ischemic foot.
Keywords: limb salvage, critical limb ischemia, revascularization
Introduction
Combined distal bypass surgery and free flap surgery can avoid the need for major amputation in patients with critical limb ischemia. 1 In 1989, Mimoun et al introduced the concept of the nutrient flap, which is intended primarily to increase perfusion of the ischemic lower extremity, with defect coverage as a secondary aim. 2 Since then, there have been several reports showing that a patent inflow artery is not essential for flap survival if blood flow to the lower extremity is increased by the nutrient flap. 2 3 4
Angiography is useful for anatomical and hemodynamic evaluation of the inflow artery before and after surgery but is highly invasive and not widely used for monitoring during postoperative follow-up. Therefore, the process of free flap survival is not fully understood. 5
In the present case, we performed a simultaneous distal bypass and free flap transfer operation to repair an extensive soft tissue defect in an ischemic foot. Despite the bypass graft becoming occluded on several occasions and the need for endovascular and surgical intervention to salvage the free flap, it has remained viable and the patient continues to be ambulatory. In this report, we discuss some newly recognized aspects of free flap survival highlighted by this case and review the relevant literature.
Case
An 84-year-old woman with a 20-year history of hypertension and dyslipidemia presented to our plastic surgery department with gangrene of the right foot. There was no diabetes or renal impairment.
At the first visit, there was necrosis on the dorsum and fourth toe of the right foot. Her skin perfusion pressure was 16 mm Hg on the dorsal surface and 28 mm Hg on the plantar surface ( Fig. 1 ). Angiography revealed triple-vessel disease below the knee, which was treated by endovascular therapy ( Fig. 2 ); thereafter, the respective skin perfusion pressure values increased to 44 and 65 mm Hg. The right foot was then amputated at the level of the metatarsal bone to limit the necrosis and spread of soft tissue infection. Healing of the surgical wound was delayed. Repeat endovascular therapy was attempted but failed. Distal bypass was performed using a non-reversed contralateral great saphenous vein graft and the defect was covered using a free latissimus dorsi flap. The graft was anastomosed to the popliteal artery in an end-to-side manner proximally and to the posterior tibial artery in an end-to-side manner distally. The thoracodorsal artery supplying the latissimus dorsi muscle and the bypass graft was anastomosed end-to-side and the accompanying vein and ipsilateral great saphenous vein were anastomosed end-to-side.
Fig. 1.

Initial status at initial presentation. Dry necrosis on the fourth toe indicates limb ischemia.
Fig. 2.
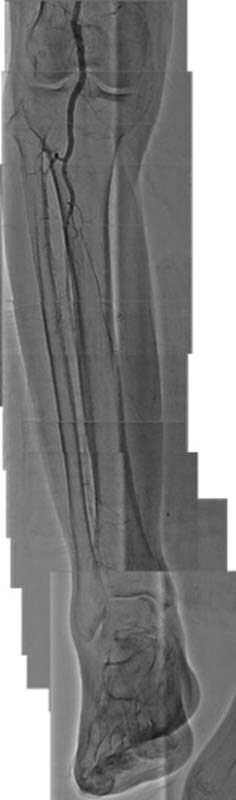
Recombined angiographic findings. Three vessels below the knee are occluded.
On postoperative day (POD) 16, angiography showed narrowing at the anastomosis site between the bypass graft and the thoracodorsal artery ( Fig. 3 ). On POD 22, surgical exploration of the narrowed site revealed a kinked artery. The kinking was released and a venous patch graft was used to cover the site. By POD 64, the patient could stand without assistance and was transferred to a rehabilitation facility.
Fig. 3.
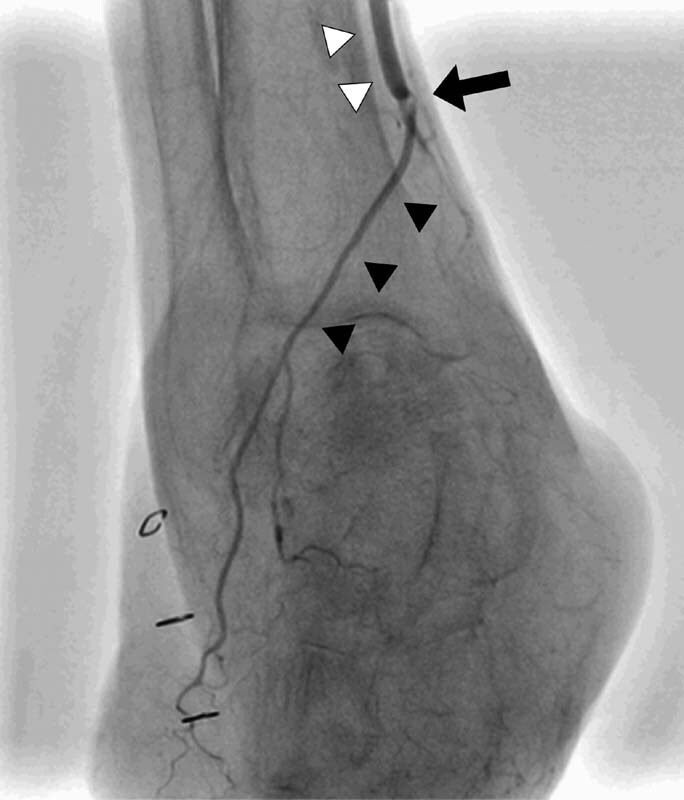
Angiographic finding on postoperative day (POD) 16. →, narrowed anastomotic site. ▲, thoracodorsal artery. △, bypass graft.
At an outpatient visit on POD 76, there was no pulse in the bypass graft ( Fig. 4 ). Endovascular therapy was performed and perfusion was recovered. Thereafter, occlusion was detected on three occasions, with repeat endovascular therapy performed on POD 96, 159, and 203 ( Fig. 5 ).
Fig. 4.

Angiographic finding on POD 76 →: occluded bypass graft.
Fig. 5.

(A) Angiographic findings on POD 96. (B) Angiographic findings on POD 159. (C) Angiographic findings on POD 203.
No pulse could be detected in the bypass graft on POD 212, so surgical exploration was performed on POD 213. Intraoperatively, the lumen at the site of anastomosis of the thoracodorsal artery was found to be occluded by a blood clot. Furthermore, the lumen at the site of anastomosis between the bypass graft and popliteal artery was hypertrophied and a remnant vein valve was observed. Despite valvectomy and thrombectomy, perfusion was not restored. Primary suturing of the vessels was performed. The latissimus dorsi flap remained viable and the patient was still ambulatory on POD 905 after the free flap transfer ( Fig. 6 ).
Fig. 6.
Clinical status in the third year after the last intervention. The patient was still ambulatory at the final follow-up.
Discussion
Combined surgical revascularization and free flap transfer is an effective surgical procedure that avoids the need for major amputation in patients with critical limb ischemia and a soft tissue defect. 1 The free flap in such cases serves as a nutrient flap, which nourishes the ischemic area, promotes angioneogenesis, and provides soft tissue coverage. 5
Free flaps often survive after occlusion of the pedicle, 6 possibly because of angioneogenesis or a vascular connection between the wound bed and the flap. 7 Yoon and Jones reported that approximately 12 days, or at least 6 days, is necessary for formation of a new vascular connection. 7 However, in an ischemic limb, this period may be as long as 3 weeks. 2 Mätzke et al reported a case in which a free flap survived after late occlusion of the inflow artery at 5 months after surgery. 3 In our case, there was no angiographic evidence of newly formed vessels on POD 16. However, on POD 76, angiography confirmed blood flow in the thoracodorsal artery within the muscle flap despite occlusion of the bypass graft ( Fig. 7 ). At that time, the muscle flap was partially cyanotic, so endovascular therapy was needed. We suspect that the repeated episodes of graft occlusion resulted from the poor run-off in the distal part of the foot. In this case, a period of approximately 7 months was needed to establish sufficient blood flow from surrounding tissue for survival of the muscle flap.
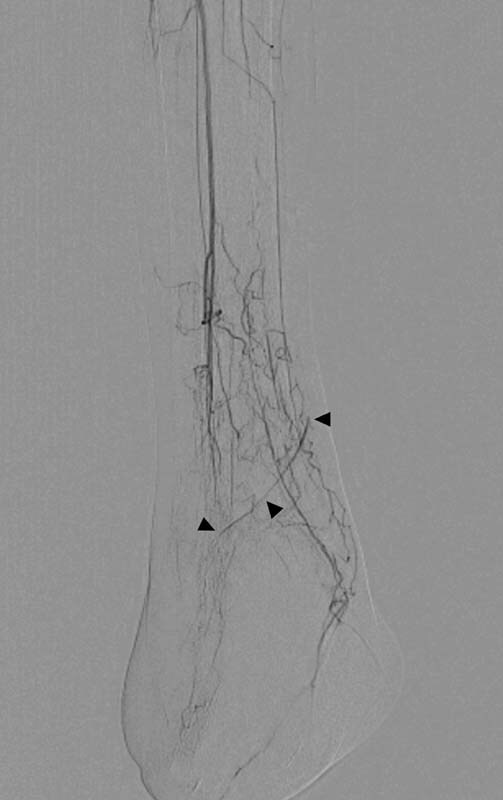
Fig. 7.

Digital subtraction angiography on POD 76. Numerous small vessels have appeared around the flap and the recipient bed. ▲, thoracodorsal artery.
When a free flap is used in an ischemic limb, a longer time is required to establish adequate blood flow than would be required in a healthy limb. This process includes at least 3 weeks while the flap is supplied by a nutrient artery. 2 Therefore, in patients with critical limb ischemia, the inflow segment needs to remain patent for longer than would normally be the case.
Conflict of Interest None declared.
Patient Consent
The patient provided written informed consent for the publication and the use of her images.
Authors' Contributions
Conceptualization: K.H. Data curation: Y.D. Writing - original draft: D.S. Writing - review & editing: D.S., Y.D., R.I., K.T., K.K., T.Y., K.H.
Ethical Approval
This is a case report and we have got approval for publication from our patient and submitted the form at the time of submission of this article.
References
- 1.Meyer A, Goller K, Horch R E. Results of combined vascular reconstruction and free flap transfer for limb salvage in patients with critical limb ischemia. J Vasc Surg. 2015;61(05):1239–1248. doi: 10.1016/j.jvs.2014.12.005. [DOI] [PubMed] [Google Scholar]
- 2.Mimoun M, Hilligot P, Baux S. The nutrient flap: a new concept of the role of the flap and application to the salvage of arteriosclerotic lower limbs. Plast Reconstr Surg. 1989;84(03):458–467. [PubMed] [Google Scholar]
- 3.Mätzke S, Tukiainen E J, Lepäntalo M J. Survival of a microvascular muscle flap despite the late occlusion of the inflow artery in a neuroischaemic diabetic foot. Scand J Plast Reconstr Surg Hand Surg. 1997;31(01):71–75. doi: 10.3109/02844319709010508. [DOI] [PubMed] [Google Scholar]
- 4.Igari K, Kudo T, Toyofuku T. Combined arterial reconstruction and free tissue transfer for patients with critical limb ischemia. Ann Vasc Dis. 2013;6(04):706–710. doi: 10.3400/avd.oa.13-00052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Tanaka K, Igari K, Kishino M. The possibility of free tissue transfer as a nutrient flap for critical ischemic foot: a case report. Microsurgery. 2017;37(06):694–698. doi: 10.1002/micr.30215. [DOI] [PubMed] [Google Scholar]
- 6.Rothaus K O, Acland R D. Free flap neo-vascularisation: case report. Br J Plast Surg. 1983;36(03):348–349. doi: 10.1016/s0007-1226(83)90059-0. [DOI] [PubMed] [Google Scholar]
- 7.Yoon A P, Jones N F. Critical time for neovascularization/angiogenesis to allow free flap survival after delayed postoperative anastomotic compromise without surgical intervention: a review of the literature. Microsurgery. 2016;36(07):604–612. doi: 10.1002/micr.30082. [DOI] [PubMed] [Google Scholar]