

Abstract
Background
We sought to clarify the impact of adolescent alcohol misuse on adult physical health and subjective well‐being. To do so, we investigated both the direct associations between adolescent alcohol misuse and early midlife physical health and life satisfaction and the indirect effects on these outcomes attributable to subsequent alcohol problems.
Method
The sample included 2733 twin pairs (32% monozygotic; 52% female) from the FinnTwin16 study. Adolescent alcohol misuse was a composite of frequency of drunkenness, frequency of alcohol use, and alcohol problems at ages 16, 17, and 18.5. The early midlife outcomes included somatic symptoms, self‐rated health, and life satisfaction at age 34. The mediators examined as part of the indirect effect analyses included alcohol problems from the Rutgers Alcohol Problem Index at ages 24 and 34. Serial mediation and co‐twin comparison models were applied and included covariates from adolescence and early midlife.
Results
There were weak direct associations between adolescent alcohol misuse and early midlife physical health and life satisfaction. However, there was stronger evidence for indirect effects, whereby young adult and early midlife alcohol problems serially mediated the relationship between adolescent alcohol misuse and early midlife somatic symptoms (β = 0.03, 95% CI [0.03, 0.04]), self‐rated health (β = −0.02, 95% CI [−0.03, −0.01]), and life satisfaction (β = −0.03, CI [−0.04, −0.02]). These serial mediation effects were robust in co‐twin comparison analyses.
Conclusions
These results provide evidence that alcohol problems are a primary driver linking adolescent alcohol misuse and poor health outcomes across the lifespan.
Keywords: adolescence, alcohol use, early midlife, life satisfaction, physical health
In a sample of 2,733 twin pairs from Finland, we found evidence that young adult and early midlife alcohol problems serially mediate the relationship between adolescent alcohol misuse and higher somatic symptoms, lower self‐rated health, and lower life satisfaction in early midlife. These effects were robust following rigorous control for potentially confounding genetic and environmental factors using a co‐twin comparison design. These findings indicate alcohol problems are a primary driver linking adolescent alcohol misuse and poor health outcomes across the lifespan.

INTRODUCTION
Adolescence is a critical time for the initiation and progression of alcohol use (Swendsen et al., 2012), and adolescent alcohol misuse is associated with an increased risk of developing long‐term substance use problems (Chen & Jacobson, 2012; Lee & Sher, 2018; Swendsen et al., 2012). Yet, the impact of adolescent alcohol misuse on indicators of adult physical health (e.g., somatic symptoms and subjective health) and subjective well‐being (e.g., life satisfaction) is less clear (Marshall, 2014; McCambridge et al., 2011; Viner & Taylor, 2007). Prior studies of the health consequences of adolescent alcohol use, which have typically terminated in young adulthood, indicate that adolescent alcohol misuse and problems are associated with poorer self‐rated health, more physical symptoms, lower life satisfaction (Rose et al., 2014), and poorer mental health and social functioning (Waldron et al., 2018). Clarifying the pathways through which adolescent alcohol use impacts physical health and subjective well‐being beyond young adulthood has potentially important implications for our understanding of the long reach of adolescent alcohol use and can be informative for appropriately timing interventions to mitigate the health consequences associated with early alcohol misuse.
Delineating the nature of associations between adolescent alcohol misuse and adult physical health and other indicators of well‐being raises two key questions. The first is whether the associations are direct (i.e., alcohol use during adolescence is associated with physical health and well‐being) or indirect and mediated through subsequent drinking behaviors. It is well established that adolescent alcohol misuse is strongly associated with alcohol‐related problems (e.g., alcohol consequences, alcohol misuse, alcohol dependence) in young adulthood and beyond (Boden et al., 2020; Newton‐Howes & Boden, 2016; Newton‐Howes et al., 2019). In turn, alcohol‐related problems in young adulthood are associated with a host of health consequences, including a greater number of physical health conditions (e.g., cardiovascular disease, headache, sleep problems) and poorer subjective and mental health (Patrick et al., 2020; Piano, 2017). This pattern of associations suggests early alcohol use promotes a cascade of alcohol‐related problems in young adulthood, and in turn later life negative physical health and well‐being outcomes.
However, the bulk of the extant literature on the longitudinal consequences of adolescent alcohol use has focused on psychiatric and substance use disorders and symptoms as outcomes. Given the evidence of direct associations between adolescent alcohol misuse and poor physical health and well‐being in young adulthood (Aarons et al., 1999; Oesterle et al., 2004; Rose et al., 2014; Waldron et al., 2017, 2018) as well as direct associations between adolescent alcohol misuse and other early midlife health outcomes (e.g., substance use disorder, depression, anxiety; Boden et al., 2020; Huurre et al., 2010), exploring long‐reaching consequences of adolescent alcohol use on physical health and well‐being remains a critical gap in the literature. Moreover, establishing that alcohol problems serially mediate the indirect effects of adolescent alcohol misuse on early midlife health outcomes would provide strong evidence that targeted interventions centered on the prevention of alcohol misuse in adolescence may mitigate physical health consequences later in life (McCambridge et al., 2011).
A second key question is whether the associations between adolescent alcohol misuse and adult physical health and subjective well‐being are robust to potentially confounding familial factors. These potentially confounding familial factors include shared genes (Edwards et al., 2017; Koopmans & Boomsma, 1996; Prescott & Kendler, 1999) and shared rearing environments ranging from urban/rural residency and the neighborhood schools one attends, to adversities such as the experience of parental divorce (Amato & Keith, 1991) or low socioeconomic status that could influence the propensity to use alcohol as well as the likelihood of poor health (Rose et al., 2014; Waldron et al., 2017, 2018). Co‐twin comparisons provide a useful inferential tool for this purpose. The logic of this type of analysis is to examine whether differences between twin siblings in a purported risk factor, such as adolescent alcohol misuse, map onto differences in their physical health and life satisfaction outcomes. The distinct inferential advantage of a co‐twin comparison design is that it permits examination of whether predictors are robust after controlling for the genetic and shared environmental factors that twin siblings share, enabling stronger inferences not possible in standard epidemiological designs of unrelated individuals (McGue et al., 2010; Rutter et al., 2001). The results from prior co‐twin comparison studies of the associations between adolescent alcohol misuse and health outcomes in young adulthood (e.g., physical symptoms, life satisfaction, subjective health, mental health, social functioning) suggest some degree of genetic confounding, meaning shared genetic factors contribute to both (Irons et al., 2015; Rose et al., 2014; Waldron et al., 2017, 2018). This underscores the utility of genetically informative designs for strengthening inferences about the impact of adolescent alcohol misuse. Such knowledge is important for understanding whether preventive interventions for alcohol misuse in adolescence may mitigate long‐term health consequences with the ability to control for unmeasured confounders apart of the co‐twin comparisons design and thus allow for stronger inferences made about the nature of the associations between adolescent alcohol use and early midlife health outcomes (Jacob et al., 2021; Yap et al., 2011).
In a large population‐based sample of twins, we examined the nature of the associations between adolescent alcohol misuse and physical health and life satisfaction outcomes in early midlife (i.e., the mid‐30s). We had two aims:
To establish, in a population‐based sample, whether the associations between adolescent alcohol misuse and early midlife physical health and life satisfaction are direct, or whether they are indirect and mediated through adult alcohol problems.
To use a co‐twin comparison design to evaluate whether the associations between adolescent alcohol misuse and early midlife physical health and life satisfaction are robust to latent genetic and shared environmental confounders, as well as measured confounders (body mass index [BMI] and smoking).
MATERIALS AND METHODS
Sample
Participants were from FinnTwin16, a population‐based longitudinal study of Finnish twins born from 1975 to 1979 (Kaprio, 2013; Kaprio et al., 2002). Twins were identified from the Population Information System at the Digital and Population Data Services Agency, Finland. For the first round of data collection, 3215 twin pairs were contacted who resided in Finland at the time of baseline assessment at age 16 and lived with one or both parents (Kaidesoja et al., 2019). Baseline assessments at age 16 had a high participation rate of 88%, yielding a total of 2733 twin pairs for baseline data. The twins then completed the second and third‐wave questionnaires when they were 17 and 18.5 years old, respectively. The fourth wave questionnaire was completed when twins were young adults at a mean age of 24. Lastly, the fifth wave questionnaire was completed when twins were aged between 32 and 38, with a mean age of 34. Retention rates across the waves were the following: age 17 (97% retention), age 18.5 (97% retention), young adulthood (mean age 24, 88% retention), and early mid‐life (mean age 34, 79% retention). Zygosity was determined via two validated items in the baseline questionnaire sent to twins and their parents. Items included similarity of their appearance in childhood and confusion by strangers, classmates, and teachers. DNA was obtained to confirm zygosity in >750 same‐sex pairs who participated in laboratory protocols. The Indiana University IRB and Ethics Committee of the University of Helsinki or Hospital District of Central Finland approved study protocols.
Measures
An adolescent alcohol misuse index (AUI) was modeled after Vachon et al. (2017) and was based on three indicators: frequency of intoxication (1‐item: “how often do you get really drunk,” with a 4‐point ordinal response option, ranging from “once a week or more” to “never”), frequency of alcohol use (1‐ item: “how often do you drink alcohol at all,” with a 9‐point ordinal response option ranging from “daily” to “I don't drink at all”), and alcohol problems as measured with an abbreviated version of the Rutgers Alcohol Problem Index (RAPI; White & Labouvie, 1989). Frequency of alcohol use and intoxication was assessed at ages 16, 17, and 18.5. Adolescent alcohol problems were measured at age 17, with a total of five items, each with a yes/no response option. Sum scores were calculated and participants missing more than two items were coded as missing. To create the AUI, maximum values for frequency of intoxication and alcohol use were selected (separately for misuse and frequency) by selecting the highest value across the ages 16, 17, and 18.5 assessments. A factor score of adolescent frequency of intoxication, frequency of alcohol use, and alcohol problems was then calculated using the confirmatory factor analysis (CFA) approach. To do this, we used the “cfa” function in the R {lavaan} package, where we used maximum likelihood estimation, with a comparative fit index >0.90 and a standardized root mean squared residual <0.08 as criteria for an acceptable model fit (Hu & Bentler, 1999). Next, we used the “lavPredict” function in “lavaan” to derive factor scores for the full sample based on the three alcohol use indicators. Lastly, the “quantcut” function in {gtools}package was used to split the factor scores into quantiles (Warnes et al., 2015). The quantile variable was used for the primary analyses.
Young adult and early midlife alcohol problems were measured using the RAPI at ages 24 and 34 (White & Labouvie, 1989), which consists of 22 items assessing dependence, withdrawal, blackouts, neglect of responsibilities, inappropriate behaviors, and shame or embarrassment because of drinking. Participants reported their experience of each alcohol consequence on a 4‐point Likert‐type scale, ranging from “never” to “quite often.” Pro‐rated sums were calculated yielding total scores from 22 to 88 for ages 24 and 34, separately. Participants missing more than four items were coded as missing.
Early midlife physical health and life satisfaction were measured at age of 34. Physical health was assessed with two measures: somatic symptoms and self‐rated health. Somatic symptoms (e.g., stomachaches, tension or nervousness, low back pain) were measured with 6‐items using a 4‐point Likert‐type scale for each symptom, ranging from “seldom or never” to “nearly every day.” Pro‐rated sums were calculated yielding total scores from 6 to 24 (α = 0.71), with higher scores indicating higher somatic symptoms (Silventoinen et al., 2007). Participants missing more than two items were coded as missing. Self‐rated health was assessed using one item on a 5‐point Likert‐type scale, ranging “very poor” to from “very good,” with higher scores indicating good health (Silventoinen et al., 2007). Life satisfaction was measured using a 5‐item questionnaire with 7‐point Likert‐type scale response options ranging from “much less than usual” to “better than usual” (Diener et al., 1985). Sum scores were calculated yielding scores from 5 to 35 (α = 0.91), with higher scores indicating high life satisfaction. Participants missing more than two items were coded as missing.
Adolescent covariates included sex and adolescent BMI and cigarette use, measured using the maximum values across ages 16, 17, and 18.5. These covariates were selected in view of prior evidence that adolescents with higher cigarette use are at an increased risk for later alcohol misuse (Huurre et al., 2010; Merline et al., 2008), while higher BMI is related to fewer alcohol problems in adolescence and young adulthood (Duncan et al., 2009; Gearhardt et al., 2018). More broadly, high BMI and cigarette use are typically associated with poorer health and life satisfaction (Constance Wiener et al., 2016; Juon et al., 2002; Kleiner et al., 2004; Simmonds et al., 2015). Cigarette use at age 16 was assessed using 1‐item: “which of the following best describes your present smoking habits” with five response options ranging from “I have never smoked” to “I smoke once or more daily.” Due to sparseness, the “I have stopped smoking at the moment or have quit entirely” response option was combined with the “I have never smoked” option. Cigarette use measured at ages 17 and 18.5 also included the response option “I smoked at least 10 cigarettes a day,” which was combined with “I smoke every day, but no more than 9 cigarettes per day” to remain consistent with the age 16 survey. BMI at ages 16, 17, and 18.5 was assessed by dividing participants' self‐reported weight in kilograms by height in meters squared.
We also controlled for a series of early midlife covariates including relationship status, educational attainment, economic standing, employment, current cigarette use, and other drug use by age 34. Relationship status at age 34 was assessed using 1‐item: “for how long has your relationship with your current spouse lasted?,” with options of “I'm not going steady with somebody” or “I'm going steady or I'm married or living together with somebody.” Educational attainment at age 34 was assessed with four category options: (1) Primary education: elementary school and completed over a 9‐year period, (2) Secondary education: an additional 2 to 3 years of education, (3) Vocational School: a total of 13 to 16 years if total education, and (4) highest level of education, falling under masters of Doctoral level. For educational attainment, a dummy code variable was created with primary education selected as the reference group. Economic standing at age 34 was assessed using 1‐item: “at present what is your economic living like,” with five point‐Likert scale response option ranging from “very good” to “very poor.” Employment at age 34 was assessed using 1‐item: “are you currently” with response options of employed, stay‐at‐home mother/father, student, and unemployed/retired. For employment, a dummy code variable was created with employment selected as the reference group. Current cigarette use at age 34 was measured using 1‐item: “which of the following alternatives describes best your current use of cigarettes” with five response options ranging from “I have never smoked” to “I smoke once or more daily.” For analyses, the response options of “I have stopped or quit smoking” and “I have never smoked” were collapsed into one item to represent current nonsmoking. Lastly, other drug use by age 34 was assessed using 1‐item: “have you ever used hash, marijuana or other drugs or e.g., sniffed glue?,” with five response options ranging from “not once” to “20 times or more.”
Statistical analyses
The preregistered analytic plan and a summary of the rationale for subsequent modifications can be viewed through the Open Science Framework (doi: 10.17605/OSF.IO/T8WC9). Consistent with our study preregistration, we first examined the associations between adolescent alcohol misuse and early midlife health and life satisfaction outcomes with zero order‐correlations. Based on patterns of zero‐order correlations, we modified our preregistered analytic plan (which originally focused on decomposing the direct associations between adolescent alcohol use and early midlife health outcomes) to instead implement serial multiple mediational models (Figure 1) to examine young adult and early midlife alcohol problems as mediators of the association between adolescent alcohol misuse and early midlife outcomes using the “sem” function in the R lavaan package (Rosseel, 2012).
FIGURE 1.
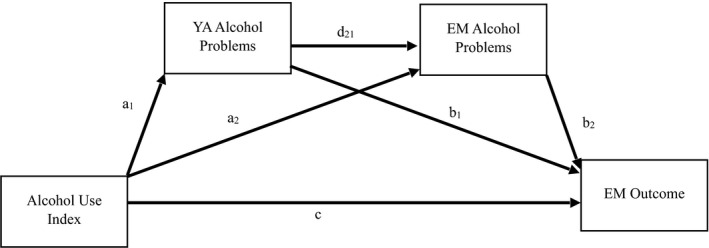
Conceptual diagram of serial multiple mediator model. YA, Young Adult; EM, Early Midlife. The serially mediated indirect effect of interest consists of the following pathways: adolescent alcohol misuse to young adult alcohol problems (a 1), young adult alcohol problems to early midlife alcohol problems (d 21), and early midlife alcohol problems to early midlife physical health and life satisfaction (b 2). The direct association between adolescent alcohol misuse and the early midlife physical health and life satisfaction outcomes is captured with path (c). Covariates included adolescent BMI, cigarette use, and sex as well as a series of early midlife covariates on the EM outcomes.
Serial mediation refers to multiple mediators in a hypothesized pathway of interest, where the focal predictor (i.e., adolescent alcohol misuse) affects the outcome through its effects on a mediator (i.e., young adult alcohol problems), which in turn affects another mediator (i.e., early midlife alcohol problems; Hayes, 2013). Thus, the serial indirect effect of interest consists of the multiple indirect effects (i.e., adolescent alcohol misuse to young adult alcohol problems (a 1), young adult alcohol problems to early midlife alcohol problems (d 21), and early midlife alcohol problems to early midlife physical health and life satisfaction (b 2)). Associations between adolescent alcohol misuse and early midlife alcohol problems (a 2) and young adult alcohol problems to early midlife outcomes (b 1) were included as well. The direct effect (c) reflects the association between adolescent alcohol misuse and the early midlife physical health and life satisfaction outcomes. Separate serial mediation models were tested for early midlife somatic symptoms, self‐rated health, and life satisfaction. Sex, adolescent cigarette use, and BMI as well as early midlife relationship status, educational attainment, economic standing, employment, current cigarette use, and other drug use by age 34 were included as covariates in the serial mediation models.
Finally, to examine whether serial mediation effects observed in the epidemiological sample remained statistically significant after controlling for genetic and shared environmental confounders, we re‐ran the serial mediation models in a co‐twin control comparison framework to examine whether differences in adolescent alcohol misuse within twin pairs predicted differences in early midlife physical health and life satisfaction. This was done by calculating twin difference scores for each measure in the serial mediation models using the R dplyr package (Wickham et al., 2021). The co‐twin comparison is captured by the twin difference score. Sex, adolescent cigarette use, BMI, and a series of early midlife covariates were included as covariates in serial mediation models. We ran the co‐twin comparison models in two stages. In the first stage, we included both monozygotic (MZ) and dizygotic (DZ) pairs. In the second stage, we restricted the co‐twin comparisons to MZ twins only. MZ twins share all of their genetic variation identical‐by‐descent; accordingly, co‐twin comparisons within this subsample provides the most stringent control of potential genetic confounds.
RESULTS
Descriptive statistics
Table 1 summarizes descriptive information about the key study measures. Approximately 52% of the participants were female and 32% were MZ twins. Zero order correlations among all study measures are shown in the Supporting Information (Table S1). Of interest, although adolescent alcohol misuse was associated at a statistically significant level with early midlife somatic symptoms (r = 0.07, 95% CI [0.04, 0.10]) and self‐rated health (r = −0.05, 95% CI [−0.08, −0.02]), the associations were of very modest effect. Adolescent alcohol misuse was not associated with early midlife life satisfaction at a statistically significant level (r = −0.01, 95% CI [−0.04, 0.02]). At the zero‐order level, a pattern emerged where higher adolescent alcohol misuse was associated with higher young adult alcohol problems (r = 0.39, 95% CI [0.36, 0.41]). In turn, young adult alcohol problems were associated with greater early midlife alcohol problems (r = 0.56, 95% CI [0.53, 0.58]). Early midlife alcohol problems were associated with more somatic symptoms (r = 0.18, 95% CI [0.15, 0.21]), lower self‐rated health (r = −0.18, 95% CI [−0.21, −0.14]), and lower life satisfaction (r = −0.28, 95% CI [−0.31, −0.25]). Lastly, twin sibling pair correlations are shown in Supporting Information (Table S2). In general, and as expected, MZ twin pairs more closely resembled each other across all the outcomes, compared to DZ twin pairs.
TABLE 1.
Descriptive statistics for study measures
| Measure | Full sample (mean/N) | Female (mean/N) | Male (mean/N) | Sex difference (t/χ2) |
|---|---|---|---|---|
| Alcohol measures | ||||
| Adolescent alcohol use index | 5.43 | 5.26 | 5.61 | t = −4.58 |
| Young adult alcohol problems | 27.78 | 26.46 | 29.36 | t = −13.75 |
| Early midlife alcohol problems | 25.53 | 24.39 | 26.99 | t = −12.72 |
| Early midlife outcomes | ||||
| Life satisfaction | 24.4 | 24.98 | 23.66 | t = 6.06 |
| Somatic symptoms | 10.8 | 11.37 | 10.07 | t = 12 |
| Self‐rated health | χ 2 = 2.54 | |||
| Very poor | 11 | 7 | 4 | |
| Fairly poor | 98 | 61 | 37 | |
| Moderate | 617 | 339 | 278 | |
| Fairly good | 2296 | 1278 | 1018 | |
| Very good | 849 | 484 | 365 | |
| Adolescent covariates | ||||
| BMI | 21.62 | 21.24 | 22.01 | t = −10.60 |
| Cigarette use | χ 2 = 44.05 | |||
| I have never smoked, or I have smoking at the moment | 2882 | 1486 | 1396 | |
| I smoke less often than once a week | 658 | 401 | 257 | |
| I smoke once or more a week, but not every day | 400 | 235 | 165 | |
| I smoke once or more daily | 1682 | 794 | 888 | |
| Early midlife covariates | ||||
| Yes partnership | 3131 | 1796 | 1335 | χ 2 = 8.99 |
| No partnership | 716 | 366 | 350 | |
| Economic standing | 4.97 | 2.58 | 2.39 | t = 6.46 |
| Educational attainment | ||||
| Primary education | 965 | 443 | 522 | |
| Secondary education | 709 | 366 | 343 | |
| Vocational education | 1134 | 702 | 432 | |
| Masers or Doctorate | 1076 | 663 | 413 | |
| Employment | ||||
| Employed | 2973 | 1519 | 1454 | |
| Stay at home | 333 | 325 | 8 | |
| Student | 163 | 104 | 59 | |
| Unemployed | 408 | 223 | 185 | |
| Cigarette use | χ 2 = 50.12 | |||
| I have never smoked or have stopped | 2773 | 1651 | 1122 | |
| I smoke less frequent than once a week | 204 | 87 | 117 | |
| I smoke once a week or more often, though not daily | 178 | 89 | 89 | |
| I smoke daily | 686 | 328 | 358 | |
| Other drug use | χ 2 = 78.62 | |||
| No | 2872 | 1713 | 1159 | |
| 1 to 3 times | 588 | 286 | 302 | |
| 4 to 9 times | 158 | 80 | 78 | |
| 10 to 19 times | 73 | 33 | 40 | |
| More than 20 times | 147 | 42 | 105 | |
Note: Bolded values indicate significant sex difference, p < 0.001.
Serial mediation results
The pattern of associations observed in simple correlations suggested a potential indirect effect of adolescent alcohol misuse on early midlife physical health and life satisfaction that is transmitted via young adult and early midlife alcohol problems. This was further explored in serial mediation analyses. As summarized in Table 2 and illustrated in Supporting Information (Figure S1), young adult and early midlife alcohol problems fully serially mediated the effect of adolescent alcohol misuse on early midlife somatic symptoms (β = 0.03, 95% CI [0.03, 0.04]) and self‐rated health (β = −0.02, 95% CI [−0.03, −0.01]), and partially serially mediated the effect of adolescent alcohol misuse on early midlife life satisfaction (β = −0.03, 95% CI [−0.04, −0.02]). Mirroring the effects observed in the zero‐order correlations, the direct associations between adolescent alcohol misuse and somatic symptoms (β = −0.01, 95% CI [−0.05, 0.04]) and self‐rated health (β = 0.01, 95% CI [−0.03, 0.06]) were not statistically significant. In contrast to the zero‐order correlations, the association between adolescent alcohol misuse and early midlife life satisfaction was significant and positive in the serial mediation model (β = 0.08, 95% CI [0.04, 0.11]).
TABLE 2.
Estimates for serial mediation model in epidemiological sample
| Somatic symptoms (N = 3437) | Self‐rated health (N = 3455) | Life satisfaction (N = 3459) | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | β | 95% CI | β | 95% CI | |
| Direct effects | ||||||
| AUI to YA Alc Prob(a 1) | 0.38 | [0.35, 0.40] | 0.38 | [0.36, 0.40] | 0.38 | [0.35, 0.40] |
| AUI to EM Alc Prob(a 2) | 0.06 | [0.03, 0.09] | 0.06 | [0.03, 0.09] | 0.06 | [0.03, 0.09] |
| YA Alc Prob to EM Alc Prob(d 21) | 0.53 | [0.51, 0.56] | 0.53 | [0.51, 0.56] | 0.53 | [0.51, 0.56] |
| YA Alc Prob to EM outcome (b 1) | 0.05 | [0.01, 0.10] | −0.01 | [−0.05, 0.03] | −0.05 | [−0.09, −0.02] |
| EM Alc Prob to EM outcome (b 2) | 0.17 | [0.13, 0.20] | −0.11 | [−0.15, −0.07] | −0.15 | [−0.18, −0.11] |
| AUI to EM outcome | −0.01 | [−0.05, 0.04] | 0.01 | [−0.03, 0.06] | 0.08 | [0.04, 0.11] |
| Indirect effect | ||||||
| AUI via YA and EM alcohol Prob (a 1 * d 21 * b 2) | 0.03 | [0.03, 0.04] | −0.02 | [−0.03, −0.01] | −0.03 | [−0.04, −0.02] |
| Adolescent covariates | ||||||
| BMI to EM outcome | 0.04 | [0.00, 0.07] | −0.12 | [−0.15, −0.09] | −0.03 | [−0.06, 0.00] |
| Cigarette use to EM outcome | 0.03 | [−0.01, 0.07] | 0.01 | [−0.04, 0.06] | 0.00 | [−0.04, 0.04] |
| Sex to EM outcome | −0.22 | [−0.25, −0.19] | 0.03 | [−0.01, 0.06] | −0.05 | [−0.08, −0.02] |
| Early midlife covariates | ||||||
| EM rel status to EM outcome | 0.02 | [−0.01, 0.05] | 0.01 | [−0.02, 0.05] | 0.31 | [0.28, 0.34] |
| EM econ standing to EM outcome | 0.16 | [0.12, 0.19] | −0.21 | [−0.24, −0.17] | −0.29 | [−0.33, −0.26] |
| Educational attainment | ||||||
| Secondary education | 0.02 | [−0.02, 0.06] | 0.00 | [−0.04, 0.04] | −0.01 | [−0.04, 0.03] |
| Vocational education | 0.02 | [−0.02, 0.06] | 0.03 | [−0.01, 0.08] | 0.02 | [−0.02, 0.06] |
| Masers or Doctorate | 0.02 | [−0.03, 0.06] | 0.06 | [0.01, 0.10] | 0.02 | [−0.02, 0.06] |
| Employment | ||||||
| Stay at home | 0.01 | [−0.03, 0.04] | 0.00 | [−0.04, 0.03] | 0.09 | [0.06, 0.12] |
| Student | 0.02 | [−0.01, 0.05] | −0.01 | [−0.05, 0.02] | −0.01 | [−0.04, 0.03] |
| Unemployed | 0.02 | [−0.02, 0.05] | −0.06 | [−0.09, −0.03] | 0.00 | [−0.03, 0.03] |
| EM cigarette use | 0.00 | [−0.04, 0.04] | −0.07 | [−0.10, −0.03] | −0.00 | [−0.03, 0.04] |
| EM other drug use | 0.02 | [−0.02, 0.05] | 0.01 | [−0.02, 0.05] | −0.06 | [−0.09, −0.03] |
Note: AUI, Alcohol Use Index; YA, Young Adult; EM, Early Midlife; Alc Prob, Alcohol Problems; Rel, Relationship; Econ, Economic. Bolded values indicate p < 0.05.
With respect to effect sizes (r‐squared), in the somatic symptoms model, adolescent alcohol misuse accounted for 0.5% of the variance, the covariates accounted for an additional 8.7% of the variance, and the mediators accounted for an additional 3.6% of the variance. In the self‐rated health model, adolescent alcohol misuse accounted for 0.3% of the variance and the covariates accounted for an additional 10.6% of the variance; however, the addition of the mediators did not appreciably increase the variance accounted for. In the life satisfaction model, adolescent alcohol use accounted for 0% of the variance, the covariates accounted for 26.3% of the variance, and the mediators accounted for an additional 0.7% of the variance.
With respect to covariates, higher adolescent BMI was associated with greater early midlife somatic symptoms, lower early midlife self‐rated health, and lower early midlife life satisfaction. Adolescent cigarette use was not associated to early midlife outcomes. For significant sex effects, males had fewer somatic symptoms, and lower life satisfaction compared to females. Of the early midlife covariates, relationship status was significantly associated with life satisfaction, where individuals in a relationship reported higher life satisfaction relative to those not in a relationship but was not associated with somatic symptoms or self‐rated health. For educational attainment, individuals who had a Masters or Doctorate had higher self‐rated health compared to those who completed primary education. Poorer economic standing was significantly associated with higher somatic symptoms, lower self‐rated health, and lower life satisfaction. For employment, being a stay‐at‐home mother/father was significantly associated with higher life satisfaction relative to being employed. In addition, being unemployed was significantly associated with poorer self‐rated health compared to being employed. Current cigarette use at age 34 was significantly associated with poorer self‐rated health, but not with somatic symptoms or life satisfaction. Other drug use by age 34 was significantly associated with lower life satisfaction, but not with somatic symptoms or self‐rated health. 1
Co‐Twin comparison serial mediation models
Following the serial mediation models in the epidemiological sample, we conducted a series of co‐twin comparison serial mediation models to assess whether the indirect effects of adolescent alcohol misuse on early midlife physical health and life satisfaction remained statistically significant when controlling for the genetic and environmental factors that twin siblings share. In total, there were 449 MZ and 778 DZ twin pairs for the somatic symptoms co‐twin comparison serial mediation model with complete data, 450 MZ and 785 DZ twin pairs for the self‐rated health co‐twin comparison serial mediation model with complete data, and 444 MZ and 788 DZ twin pairs for life satisfaction co‐twin comparison serial mediation model with complete data. As summarized in Table 3, the effects observed in the epidemiological sample remained significant in the co‐twin comparison models. Within families, adolescent alcohol misuse was serially mediated by young adult and early midlife alcohol problems to predict early midlife somatic symptoms (β = 0.02, 95% CI [0.01, 0.02]), self‐rated health (β = −0.01, 95% CI [−0.014, −0.006]), and life satisfaction (β = −0.02, 95% CI [−0.02, −0.01]). In the co‐twin comparison models, adolescent alcohol misuse was not directly positively associated at a statistically significant level with somatic symptoms (β = −0.03, 95% CI [−0.06, 0.01]), self‐rated‐health (β = 0.01, 95% CI [−0.03, 0.05]), nor life satisfaction (β = 0.01, 95% CI [−0.02, 0.05]).
TABLE 3.
Estimates for co‐twin serial mediation models
| Somatic symptoms (N = 3079) | Self‐rated health (N = 3079) | Life satisfaction (N = 3079) | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | β | 95% CI | β | 95% CI | |
| Direct effects | ||||||
| AUI to YA Alc Prob (a 1) | 0.27 | [0.24, 0.30] | 0.27 | [0.24, 0.30] | 0.27 | [0.24, 0.30] |
| AUI to EM Alc Prob(a 2) | 0.06 | [0.03, 0.10] | 0.06 | [0.03, 0.10] | 0.06 | [0.03, 0.10] |
| YA Alc Prob to EM Alc Prob(d 21) | 0.36 | [0.32, 0.39] | 0.36 | [0.32, 0.39] | 0.36 | [0.32, 0.39] |
| YA Alc Prob to EM outcome (b 1) | 0.03 | [0.00, 0.07] | 0.00 | [−0.04, 0.04] | −0.02 | [−0.06, 0.01] |
| EM Alc Prob to EM outcome (b 2) | 0.16 | [0.12, 0.20] | −0.10 | [−0.14, −0.06] | −0.19 | [−0.22, –0.15] |
| AUI to EM outcome | −0.03 | [−0.06, 0.01] | 0.01 | [−0.03, 0.05] | 0.01 | [−0.02, 0.05] |
| Indirect effect | ||||||
| AUI via YA and EM alcohol Prob (a 1 * d 21 * b 2) | 0.02 | [0.01, 0.02] | −0.01 | [−0.014, −0.006] | −0.02 | [−0.02, −0.01] |
| Adolescent covariates | ||||||
| BMI to EM outcome | −0.03 | [−0.07, 0.00] | −0.05 | [−0.09, −0.02] | −0.01 | [−0.04, 0.03] |
| Cigarette use to EM outcome | 0.06 | [0.02, 0.09] | 0.00 | [−0.04, 0.04] | 0.02 | [−0.02, 0.05] |
| Sex to EM outcome | −0.10 | [−0.14, −0.07] | 0.02 | [−0.02, 0.06] | −0.00 | [−0.04, 0.03] |
| Early midlife covariates | ||||||
| EM Rel status to EM Outcome | 0.01 | [−0.03, 0.04] | 0.02 | [−0.01, 0.06] | 0.18 | [0.15, 0.21] |
| EM Econ Standing to EM Outcome | 0.15 | [0.12, 0.19] | −0.16 | [−0.19, −0.12] | −0.27 | [−0.31, −0.24] |
| Educational attainment | ||||||
| Secondary education | −0.01 | [−0.05, 0.03] | −0.01 | [−0.05, 0.03] | 0.02 | [−0.02, 0.06] |
| Vocational education | −0.01 | [−0.05, 0.03] | 0.01 | [−0.04, 0.06] | 0.01 | [−0.03, 0.06] |
| Masters or Doctorate | −0.02 | [−0.06, 0.02] | 0.02 | [−0.02, 0.07] | 0.02 | [−0.02, 0.07] |
| Employment | ||||||
| Stay at home | −0.01 | [−0.05, 0.02] | 0.01 | [−0.03, 0.05] | 0.04 | [0.01, 0.08] |
| Student | 0.03 | [−0.01, 0.06] | 0.00 | [−0.03, 0.04] | 0.02 | [−0.02, 0.05] |
| Unemployed | 0.04 | [0.00, 0.07] | −0.02 | [−0.06, 0.01] | 0.02 | [−0.02, 0.05] |
| EM cigarette use | −0.03 | [−0.07, 0.02] | −0.04 | [−0.08, 0.00] | −0.06 | [−0.10, −0.03] |
| EM other drug use | −0.05 | [−0.09, −0.02] | 0.01 | [−0.03, 0.05] | −0.06 | [−0.09, −0.03] |
Note: AUI, Alcohol Use Index; YA, Young Adult; EM, Early Midlife; Alc Prob, Alcohol Problems; Rel, Relationship; Econ, Economic. Bolded values indicate p < 0.05.
Higher adolescent BMI was associated with lower self‐rated health but was not associated with somatic symptoms or life satisfaction. Adolescent cigarette use was associated with higher early midlife somatic symptoms, but was not associated with self‐rated health or life satisfaction. Males had fewer somatic symptoms compared to females, but there were no statistically significant sex differences for self‐rated health or life satisfaction. Of the early midlife covariates, relationship status was significantly associated with life satisfaction, where individuals in a relationship reported higher life satisfaction relative to those not in a relationship. Educational attainment was not significantly associated with early midlife outcomes. Poorer economic standing was significantly associated with higher somatic symptoms, and lower self‐rated health and life satisfaction. For employment, being a stay‐at‐home mother/father was significantly associated with higher life satisfaction relative to being employed. Current cigarette use at age 34 was significantly associated with lower self‐rated health and lower life satisfaction, but not with somatic symptoms. Other drug use by age 34 was significantly associated with lower somatic symptoms and lower life satisfaction, but not with self‐rated health.
As summarized in Table 4, the serially mediated indirect effects of adolescent alcohol misuse on early midlife somatic symptoms (β = 0.006, 95% CI [0.002, 0.009]), self‐rated health (β = −0.002, 95% CI [−0.005, 0.000]) and life satisfaction (β = −0.006, 95% CI [−0.010, −0.003]) remained significant in the MZ‐only co‐twin comparison models. In these models, adolescent alcohol misuse was not directly associated at a statistically significant level with somatic symptoms (β = −0.01, 95% CI [−0.07, 0.05]) or self‐rated health (β = 0.05, 95% CI [−0.02, 0.11]). There was, however, an association between adolescent alcohol misuse and life satisfaction (β = 0.10, 95% CI [0.04, 0.16]).
TABLE 4.
Estimates for co‐twin serial mediation models in monozygotic twins only
| Somatic symptoms (N = 1027) | Self‐rated health (N = 1027) | Life satisfaction (N = 1027) | ||||
|---|---|---|---|---|---|---|
| β | 95% CI | β | 95% CI | β | 95% CI | |
| Direct effects | ||||||
| AUI to YA Alc Prob(a 1) | 0.22 | [0.16, 0.28] | 0.22 | [0.16, 0.28] | 0.22 | [0.16, 0.28] |
| AUI to EM Alc Prob(a 2) | 0.01 | [−0.06, 0.07] | 0.01 | [−0.06, 0.07] | 0.01 | [−0.05, 0.07] |
| YA Alc Prob to EM Alc Prob(d 21) | 0.16 | [0.10, 0.22] | 0.16 | [0.10, 0.22] | 0.16 | [0.11, 0.22] |
| YA Alc Prob to EM outcome (b 1) | 0.01 | [−0.05, 0.07] | −0.04 | [−0.11, 0.02] | −0.06 | [−0.12, 0.00] |
| EM Alc Prob to EM outcome (b 2) | 0.16 | [0.10, 0.22] | −0.07 | [−0.13, −0.01] | −0.17 | [−0.23, −0.12] |
| AUI to EM outcome | −0.01 | [−0.07, 0.05] | 0.05 | [−0.02, 0.11] | 0.10 | [0.04, 0.16] |
| Indirect effect | ||||||
| AUI via YA and EM alcohol Prob (a 1 * d 21 * b 2) | 0.006 | [0.002, 0.009] | −0.002 | [−0.005, 0.000] | −0.006 | [−0.010, −0.003] |
| Adolescent covariates | ||||||
| Adol BMI to EM outcome | 0.04 | [−0.02, 0.10] | −0.06 | [−0.12, 0.01] | 0.00 | [−0.06, 0.06] |
| Adol cigarette to EM outcome | 0.04 | [−0.02, 0.11] | 0.03 | [−0.04, 0.09] | 0.05 | [−0.01, 0.11] |
| Sex | −0.02 | [−0.08, 0.05] | 0.01 | [−0.05, 0.07] | 0.02 | [−0.03, 0.08] |
| Early midlife covariates | ||||||
| EM Rel status to EM outcome | −0.05 | [−0.11, 0.01] | 0.05 | [−0.02, 0.11] | 0.16 | [0.10, 0.21] |
| EM Econ standing to EM outcome | 0.09 | [0.03, 0.15] | −0.09 | [−0.15, −0.02] | −0.23 | [−0.29, −0.17] |
| Educational attainment | ||||||
| Secondary education | −0.07 | [−0.14, 0.01] | 0.03 | [−0.04, 0.11] | 0.05 | [−0.02, 0.12] |
| Vocational education | −0.04 | [−0.12, 0.04] | 0.01 | [−0.08, 0.09] | 0.02 | [−0.05, 0.10] |
| Masers or doctorate | −0.03 | [−0.11, 0.05] | 0.02 | [−0.06, 0.10] | 0.03 | [−0.05, 0.11] |
| Employment | ||||||
| Stay at home | −0.02 | [−0.08, 0.05] | −0.00 | [−0.06, 0.07] | 0.02 | [−0.04, 0.08] |
| Student | 0.04 | [−0.02, 0.11] | 0.00 | [−0.07, 0.06] | 0.00 | [−0.06, 0.06] |
| Unemployed | −0.01 | [−0.07, 0.05] | 0.02 | [−0.04, 0.09] | 0.03 | [−0.03, 0.08] |
| EM cigarette use | −0.07 | [−0.13, −0.01] | 0.00 | [−0.06, 0.06] | −0.08 | [−0.14, −0.02] |
| EM other drug use | −0.11 | [−0.17, −0.05] | 0.04 | [−0.02, 0.10] | −0.07 | [−0.13, −0.01] |
Note: AUI, Alcohol Use Index; YA, Young Adult; EM, Early Midlife; Alc Prob, Alcohol Problems; Econ, Economic. Bolded values indicate p < 0.05.
Neither the adolescent BMI, cigarette use, nor sex were associated with early midlife outcomes. Of the early midlife covariates, relationship status was significantly associated with life satisfaction, where individuals in a relationship reported higher life satisfaction relative to those not in a relationship. Educational attainment was not significantly associated with early midlife outcomes. Poor economic standing was significantly associated with higher somatic symptoms, lower self‐rated health, and lower life satisfaction. There were no significant effects of employment on early midlife outcomes. Current cigarette use at age 34 was significantly associated with lower somatic symptoms and lower life satisfaction, but not with self‐rated health. Other drug use by age 34 was associated with lower somatic symptoms and lower life satisfaction, but not with self‐rated health.
DISCUSSION
In a population‐based sample of twins, we aimed to delineate the associations between adolescent alcohol misuse and early midlife health outcomes and life satisfaction. In addition, we aimed to evaluate whether these associations were robust to potential genetic and shared environmental familial confounders.
Our first goal was to characterize the associations among adolescent alcohol misuse and early midlife physical health and life satisfaction. In zero‐order correlations, there were weak associations between adolescent alcohol misuse and early midlife physical health (i.e., somatic symptoms, self‐rated health) and life satisfaction. Given robust evidence in prior literature finding longitudinal consequences and direct effects of adolescent alcohol use on later life substance use and mental health‐related outcomes, our findings suggest adolescent alcohol use may influence long‐term physical health outcomes and life satisfaction in an indirect pathway rather than directly. This was supported by patterns identified in zero‐order correlations which indicated a potentially indirect pathway from adolescent alcohol misuse to early midlife physical health and life satisfaction. Consistent with prior evidence linking adolescent alcohol misuse and adult alcohol problems (Boden et al., 2020; Duncan et al., 1997; Irons et al., 2015), we found that adolescent alcohol misuse was associated with higher alcohol problems in young adulthood. In turn, young adulthood problems were associated with higher early midlife alcohol problems, which were associated with poorer early midlife physical health and life satisfaction. These latter effects are consistent with prior evidence that alcohol‐related problems in young adulthood are associated with poor physical and mental health and lower life satisfaction in early midlife (Fergusson et al., 2015; Koivumaa‐Honkanen et al., 2012; Patrick et al., 2020; Swain et al., 2012).
The pattern of associations observed in the zero‐order correlations indicated that the impact of adolescent alcohol misuse on later life health may be transmitted via alcohol problems in young adulthood and early midlife. In formal tests of this using serial mediation models, we found that alcohol problems in young adulthood and early midlife serially mediated the associations between adolescent alcohol misuse and early midlife physical health and life satisfaction. Notably, there was a direct effect between adolescent alcohol and early midlife life satisfaction, but not somatic symptoms or self‐rated health. This is consistent with a prior study that found a direct association between adolescent alcohol misuse and early midlife depression, anxiety, and poorer psychosocial outcomes (e.g., lower levels of educational attainment, increased risk of receiving welfare benefits; Boden et al., 2020), and suggests adolescent alcohol use may be a particularly salient influence on well‐being into later adulthood. Moreover, the magnitude of effects of the alcohol problem serial mediators in the epidemiological models was modest and negligible for life satisfaction and self‐rated health, and moderate for somatic symptoms. Taken together, our results suggest adolescent alcohol misuse sets the stage for later life alcohol problems, which in turn has negative consequences for early midlife physical health and life satisfaction. However, it should be noted that the magnitude of effects of the alcohol problem serial mediators in the epidemiological models were modest and negligible for life satisfaction and self‐rated health, and moderate for somatic symptoms.
Our second goal was to examine whether these associations remained statistically significant after controlling for factors that might confound the associations between adolescent alcohol misuse and poor health outcomes later in life. There is evidence that genetic factors and shared familial experiences (e.g., parental divorce, urban/rural residency, family socioeconomic status), might contribute to both adolescent alcohol use and poorer health in early midlife (Amato & Keith, 1991; Waldron et al., 2017). Thus, these potentially confounding familial factors underscore the need for a design that permits rigorous control of confounds to delineate if associations of adolescent alcohol misuse with poor later life outcomes are explained by familial background and shared genetic influences. To do this, we ran additional serial mediation models using a co‐twin comparisons framework. The effects observed in the epidemiological sample remained significant in co‐twin comparison models, including in analyses where the co‐twin comparisons were limited to monozygotic pairs, albeit of more modest magnitude. As noted by others, family‐based designs such as co‐twin comparisons (D'Onofrio et al., 2013; Lahey & D'Onofrio, 2010) can strengthen inferences regarding the nature of the associations in observational studies. As a set, our results suggest that the serially mediated associations between adolescent alcohol misuse and early midlife satisfaction are robust to strict controls for familial confounding.
Implications
The findings from this study highlight the significance of adolescent alcohol misuse for adult alcohol problems that in turn have negative impacts on indicators of health and well‐being later in life. The long reach of adolescent misuse, and in particular our findings that these effects were robust to confounding genetic and rearing environmental factors that twin siblings share, suggests that preventive interventions targeting adolescents with alcohol misuse may mitigate a host of health consequences across the lifespan. Despite these effects being statistically significant, we also recognize that the corresponding magnitude of the effects was small. A number of effective adolescent alcohol prevention programs exist (Chun & Linakis, 2012; Yap et al., 2011), such as one that pairs psychoeducation with exercises that help youth address unique personality risk factors (e.g., sensation seeking, anxiety sensitivity) and associated maladaptive coping strategies (Conrod et al., 2006). Additionally, family‐ and school‐based preventative interventions that encourage parental rule‐setting and educational lessons on youth alcohol and substance use can prevent heavy alcohol use in adolescence (Koning et al., 2009). In sum, the findings reveal that adolescent AUIs risk for poor physical health and well‐being two decades later, highlighting the salience of early preventive intervention efforts.
Limitations
Our results should be considered in the context of potential limitations. First, we note that the statistical package lavaan used for serial mediation (Rosseel, 2012) did not have the capability to control for the correlated observations (i.e., twins nested in pairs), which could have the consequence of artificially deflating the standard errors. To address this, we calculated additional mediation models that randomly selected one member of each twin pair. Findings, shown in Table S4, were consistent with mediation models using the overall epidemiological sample that included both twins from each pair. Second, we recognize that we focused on a small set of physical health and well‐being outcomes, and that alcohol misuse has other serious negative health consequences that we did not examine (as they were expected to be less common in this age group) such as acute myocardial infarction (Russell et al., 2019) and cardiometabolic risk (Fan et al., 2008). Third, although the co‐twin design permits control of genetic and environmental influences that twins share, the confounding effect of unmeasured individual characteristics are not accounted for. For example, if one co‐twin experienced a traumatic event, this differential exposure to trauma may confound the observed association of adolescent alcohol use on later life physical health and well‐being (Dixon et al., 2009; Keyes et al., 2013; Overstreet et al., 2017). Fourth, we recognize the early midlife outcome of self‐rated health was an ordinal measure fit in a linear regression model. However, prior evidence suggests that linear regression coefficients of binary and ordinal outcomes yield robust unbiased estimates and are interpretable in terms of probabilities (Gomila, 2021).
Fifth, we recognize that a twin sample may not generalize to the broader nontwin population. However, attenuating this concern is that the rates of alcohol use as reported by the FinnTwin16 participants in adolescence and early midlife are similar to rates reported in other Finnish population health studies. For example, 32% of individuals aged 15 to 19 in the general population consumed at least 60 or more grams of pure alcohol (i.e., five standard drinks) on at least one occasion in the past 30 days (WHO, 2016). This rate is consistent with the approximately 29% of FinnTwin16 participants who reported misusing alcohol one to two times a month at the adolescent assessments. Similarly, 28% of individuals aged 15 plus in the general population consumed at least consumed at least 60 or more grams of pure alcohol on at least one occasion in the past 30 days (WHO, 2016). This is again consistent to the approximately 22% of FinnTwin16 participants who reported misusing alcohol one to two times a month. Further, we only examined alcohol use as a pathway connecting adolescent alcohol misuse and early midlife outcomes. However, it is possible that there may be other pathways linking this association, such as other substance use. Thus, future research should examine alternate pathways outside the scope of alcohol use in this association. Lastly, we recognize the effects reported here were relatively modest. This suggests adolescent alcohol misuse is likely just one target to address as part of comprehensive preventive interventions to reduce later alcohol problems and, in turn, promote early midlife physical health and well‐being (Funder & Ozer, 2019).
CONCLUSIONS
In a population‐based sample of twins, we found support that adolescent alcohol misuse impacts early midlife physical health and life satisfaction indirectly through elevations in young adult and early midlife alcohol problems. The sequence of indirect effects linking adolescent alcohol misuse and poor health outcomes were robust in co‐twin comparison models as well. The convergent results across the serial mediation models suggest that alcohol problems are a primary driver linking adolescent alcohol misuse and poor health outcomes across multiple decades of the lifespan. Identifying factors that may alter the pathways between adolescent alcohol misuse and subsequent later life health and life satisfaction outcomes represents an important direction for future work.
CONFLICT OF INTEREST
None.
Supporting information
Appendix S1
ACKNOWLEDGMENTS
This work was supported by the National Institute on Alcohol Abuse and Alcoholism of the National Institutes of Health under award numbers R01 AA015416, R01 AA09203, K02 AA018755, and K01 AA024152; and the Academy of Finland (grants 100499, 205585, 118555, 141054, 265240, 263278, and 264146). JK and AL have been supported by the Academy of Finland (grants 265240, 263278, 308248, and 312073 to JK; grant 308698 to AL). The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Pascale, A. , Stephenson, M. , Barr, P. , Latvala, A. , Aaltonen, S. & Piirtola, M. et al. (2022) Exploring the relationships between adolescent alcohol misuse and later life health outcomes. Alcoholism: Clinical and Experimental Research, 46, 1753–1765. Available from: 10.1111/acer.14917
Endnote
A reviewer noted that including adolescent health covariates from age 16 would provide additional analytic rigor. We examined age 16 adolescent somatic symptoms and self‐rated health as covariates in the corresponding serial mediation models (life satisfaction was not measured at age 16 and thus this was only done for the somatic symptom and self‐rated health models). Results, summarized in Table S1, indicated that the serial mediation effects remained consistent even after statistically controlling for the adolescent health covariates.
Contributor Information
Angela Pascale, Email: pascaleac@vcu.edu.
Jessica E. Salvatore, Email: jessica.salvatore@rutgers.edu.
REFERENCES
- Aarons, G.A. , Brown, S.A. , Coe, M.T. , Myers, M.G. , Garland, A.F. , Ezzet‐Lofstram, R. et al. (1999) Adolescent alcohol and drug abuse and health. Journal of Adolescent Health, 24, 412–421. [DOI] [PubMed] [Google Scholar]
- Amato, P.R. & Keith, B. (1991) Parental divorce and adult well‐being: a meta‐analysis. Journal of Marriage and Family, 53, 43–58. [Google Scholar]
- Boden, J. , Blair, S. & Newton‐Howes, G. (2020) Alcohol use in adolescents and adult psychopathology and social outcomes: findings from a 35‐year cohort study. The Australian and New Zealand Journal of Psychiatry, 54, 909–918. [DOI] [PubMed] [Google Scholar]
- Chen, P.P.D. & Jacobson, K.C.P.D. (2012) Developmental trajectories of substance use from early adolescence to young adulthood: gender and racial/ethnic differences. The Journal of Adolescent Health, 50, 154–163. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chun, T.H. & Linakis, J.G. (2012) Interventions for adolescent alcohol use. Current Opinion in Pediatrics, 24, 238–242. [DOI] [PubMed] [Google Scholar]
- Conrod, P.J. , Stewart, S.H. , Comeau, N. & Maclean, A.M. (2006) Efficacy of cognitive–behavioral interventions targeting personality risk factors for youth alcohol misuse. Journal of Clinical Child and Adolescent Psychology, 35, 550–563. [DOI] [PubMed] [Google Scholar]
- Constance Wiener, R. , Trickett Shockey, A.K. & Morgan, S.K. (2016) Adolescent light cigarette smoking patterns and adult cigarette smoking. Advanced Epidemiology, 2016, 1–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- D'Onofrio, B.M. , Lahey, B.B. , Turkheimer, E. & Lichtenstein, P. (2013) Critical need for family‐based, quasi‐experimental designs in integrating genetic and social science research. American Journal of Public Health, 103, S46–S55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Diener, E. , Emmons, R.A. , Larsen, R.J. & Griffin, S. (1985) The satisfaction with life scale. Journal of Personality Assessment, 49, 71–75. [DOI] [PubMed] [Google Scholar]
- Dixon, L.J. , Leen‐Feldner, E.W. , Ham, L.S. , Feldner, M.T. & Lewis, S.F. (2009) Alcohol use motives among traumatic event‐exposed, treatment‐seeking adolescents: associations with posttraumatic stress. Addictive Behaviors, 34, 1065–1068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan, A.E. , Grant, J.D. , Keenan Bucholz, K. , Madden, P.A.F. & Heath, A.C. (2009) Relationship between body mass index, alcohol use, and alcohol misuse in a young adult female twin sample. Journal of Studies on Alcohol and Drugs, 70, 458–466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Duncan, S.C. , Alpert, A. , Duncan, T.E. & Hops, H. (1997) Adolescent alcohol use development and young adult outcomes. Drug and Alcohol Dependence, 49, 39–48. [DOI] [PubMed] [Google Scholar]
- Edwards, A.C. , Heron, J. , Vladimirov, V. , Wolen, A.R. , Adkins, D.E. , Aliev, F. et al. (2017) The rate of change in alcohol misuse across adolescence is heritable. Alcoholism, Clinical and Experimental Research, 41, 57–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fan, A.Z. , Russell, M. , Stranges, S. , Dorn, J. & Trevisan, M. (2008) Association of lifetime alcohol drinking trajectories with cardiometabolic risk. The Journal of Clinical Endocrinology and Metabolism, 93, 154–161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fergusson, D.M. , McLeod, G.F.H. , Horwood, L.J. , Swain, N.R. , Chapple, S. & Poulton, R. (2015) Life satisfaction and mental health problems (18 to 35 years). Psychological Medicine, 45, 2427–2436. [DOI] [PubMed] [Google Scholar]
- Funder, D.C. & Ozer, D.J. (2019) Evaluating effect size in psychological research: sense and nonsense. Advances in Methods and Practices in Psychological Science, 2, 156–168. [Google Scholar]
- Gearhardt, A.N. , Waller, R. , Jester, J.M. , Hyde, L.W. & Zucker, R.A. (2018) Body mass index across adolescence and substance use problems in early adulthood. Psychology of Addictive Behaviors, 32, 309–319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gomila, R. (2021) Logistic or linear? Estimating causal effects of experimental treatments on binary outcomes using regression analysis. Journal of Experimental Psychology, General, 150, 700–709. [DOI] [PubMed] [Google Scholar]
- Hayes, A.F. (2013) Introduction to mediation, moderation, and conditional process analysis: a regression‐based approach. Methodology in the social sciences. New York: The Guilford Press. [Google Scholar]
- Hu, L. & Bentler, P.M. (1999) Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55. [Google Scholar]
- Huurre, T. , Lintonen, T. , Kaprio, J. , Pelkonen, M. , Marttunen, M. & Aro, H. (2010) Adolescent risk factors for excessive alcohol use at age 32 years. A 16‐year prospective follow‐up study. Social Psychiatry and Psychiatric Epidemiology, 45, 125–134. [DOI] [PubMed] [Google Scholar]
- Irons, D.E. , Iacono, W.G. & McGue, M. (2015) Tests of the effects of adolescent early alcohol exposures on adult outcomes. Addiction, 110, 269–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jacob, L. , Smith, L. , Armstrong, N.C. , Yakkundi, A. , Barnett, Y. , Butler, L. et al. (2021) Alcohol use and mental health during covid‐19 lockdown: a cross‐sectional study in a sample of UKadults. Drug and Alcohol Dependence, 219, 108488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Juon, H.‐S. , Ensminger, M.E. & Sydnor, K.D. (2002) A longitudinal study of developmental trajectories to young adult cigarette smoking. Drug and Alcohol Dependence, 66, 303–314. [DOI] [PubMed] [Google Scholar]
- Kaidesoja, M. , Aaltonen, S. , Bogl, L.H. , Heikkilä, K. , Kaartinen, S. , Kujala, U.M. et al. (2019) Finntwin16: a longitudinal study from age 16 of a population‐based finnish twin cohort. Twin Research and Human Genetics, 22, 530–539. [DOI] [PubMed] [Google Scholar]
- Kaprio, J. (2013) The finnish twin cohort study: an update. Twin Research and Human Genetics, 16, 157–162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaprio, J. , Pulkkinen, L. & Rose, R.J. (2002) Genetic and environmental factors in health‐related behaviors: studies on finnish twins and twin families. Twin Research, 5, 366–371. [DOI] [PubMed] [Google Scholar]
- Keyes, K.M. , McLaughlin, K.A. , Demmer, R.T. , Cerdá, M. , Koenen, K.C. , Uddin, M. et al. (2013) Potentially traumatic events and the risk of six physical health conditions in a population‐based sample. Depression and Anxiety, 30, 451–460. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kleiner, K.D. , Gold, M.S. , Frostpineda, K. , Lenzbrunsman, B. , Perri, M.G. & Jacobs, W.S. (2004) Body mass index and alcohol use. Journal of Addictive Diseases, 23, 105–118. [DOI] [PubMed] [Google Scholar]
- Koivumaa‐Honkanen, H. , Kaprio, J. , Korhonen, T. , Honkanen, R.J. , Heikkilä, K. & Koskenvuo, M. (2012) Self‐reported life satisfaction and alcohol use: a 15‐year follow‐up of healthy adult twins. Alcohol and Alcoholism, 47, 160–168. [DOI] [PubMed] [Google Scholar]
- Koning, I.M. , Vollebergh, W.A.M. , Smit, F. , Verdurmen, J.E.E. , van den Eijnden, R.J.J.M. , ter Bogt, T.F.M. et al. (2009) Preventing heavy alcohol use in adolescents (pas): cluster randomized trial of a parent and student intervention offered separately and simultaneously. Addiction, 104, 1669–1678. [DOI] [PubMed] [Google Scholar]
- Koopmans, J.R. & Boomsma, D.I. (1996) Familial resemblances in alcohol use: genetic or cultural transmission? Journal of Studies on Alcohol, 57, 19–28. [DOI] [PubMed] [Google Scholar]
- Lahey, B.B. & D'Onofrio, B.M. (2010) All in the family: comparing siblings to test causal hypotheses regarding environmental influences on behavior. Current Directions in Psychological Science, 19, 319–323. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee, M.R. & Sher, K.J. (2018) "maturing out" of binge and problem drinking. Alcohol Research & Health, 39, 31. [PMC free article] [PubMed] [Google Scholar]
- Marshall, E.J. (2014) Adolescent alcohol use: risks and consequences. Alcohol and Alcoholism, 49, 160–164. [DOI] [PubMed] [Google Scholar]
- McCambridge, J. , McAlaney, J. & Rowe, R. (2011) Adult consequences of late adolescent alcohol consumption: a systematic review of cohort studies. PLoS Medicine, 8, e1000413. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McGue, M. , Osler, M. & Christensen, K. (2010) Causal inference and observational research: the utility of twins. Perspectives on Psychological Science, 5, 546–556. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Merline, A. , Jager, J. & Schulenberg, J.E. (2008) Adolescent risk factors for adult alcohol use and abuse: stability and change of predictive value across early and middle adulthood. Addiction, 103, 84–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newton‐Howes, G. & Boden, J.M. (2016) Relation between age of first drinking and mental health and alcohol and drug disorders in adulthood: evidence from a 35‐year cohort study. Addiction, 111, 637–644. [DOI] [PubMed] [Google Scholar]
- Newton‐Howes, G. , Cook, S. , Martin, G. , Foulds, J.A. & Boden, J.M. (2019) Comparison of age of first drink and age of first intoxication as predictors of substance use and mental health problems in adulthood. Drug and Alcohol Dependence, 194, 238–243. [DOI] [PubMed] [Google Scholar]
- Oesterle, S. , Hill, K.G. , Hawkins, J.D. , Guo, J. , Catalano, R.F. & Abbott, R.D. (2004) Adolescent heavy episodic drinking trajectories and health in young adulthood. Journal of Studies on Alcohol, 65, 204–212. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Overstreet, C. , Berenz, E.C. , Kendler, K.S. , Dick, D.M. & Amstadter, A.B. (2017) Predictors and mental health outcomes of potentially traumatic event exposure. Psychiatry Research, 247, 296–304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patrick, M.E. , Berglund, P.A. , Joshi, S. & Bray, B.C. (2020) A latent class analysis of heavy substance use in young adulthood and impacts on physical, cognitive, and mental health outcomes in middle age. Drug and Alcohol Dependence, 212, 108018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piano, M.R. (2017) Alcohol's effects on the cardiovascular system. Alcohol Research: Current Reviews, 38, 219–241. [PMC free article] [PubMed] [Google Scholar]
- Prescott, C.A. & Kendler, K.S. (1999) Age at first drink and risk for alcoholism: a noncausal association. Alcoholism, Clinical and Experimental Research, 23, 101–107. [PubMed] [Google Scholar]
- Rose, R.J. , Winter, T. , Viken, R.J. & Kaprio, J. (2014) Adolescent alcohol abuse and adverse adult outcomes: evaluating confounds with drinking‐discordant twins. Alcoholism, Clinical and Experimental Research, 38, 2314–2321. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rosseel, Y. (2012) Lavaan: An R package for structural equation modeling, Vol. 48. Journal of Statistical Software, p. 36. [Google Scholar]
- Russell, M. , Fan, A.Z. , Freudenheim, J.L. , Dorn, J. & Trevisan, M. (2019) Lifetime drinking trajectories and nonfatal acute myocardial infarction. Alcoholism, Clinical and Experimental Research, 43, 2384–2394. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rutter, M. , Pickles, A. , Murray, R. & Eaves, L. (2001) Testing hypotheses on specific environmental causal effects on behavior. Psychological Bulletin, 127, 291–324. [DOI] [PubMed] [Google Scholar]
- Silventoinen, K. , Posthuma, D. , Lahelma, E. , Rose, R.J. & Kaprio, J. (2007) Genetic and environmental factors affecting self‐rated health from age 16‐25: a longitudinal study of finnish twins. Behavior Genetics, 37, 326–333. [DOI] [PubMed] [Google Scholar]
- Simmonds, M. , Burch, J. , Llewellyn, A. , Griffiths, C. , Yang, H. , Owen, C. et al. (2015) The use of measures of obesity in childhood for predicting obesity and the development of obesity‐related diseases in adulthood: a systematic review and meta‐analysis. Health Technology Assessment, 19, 1–336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Swain, N.R. , Gibb, S.J. , Horwood, L.J. & Fergusson, D.M. (2012) Alcohol and cannabis abuse/dependence symptoms and life satisfaction in young adulthood: alcohol, cannabis and life satisfaction. Drug and Alcohol Review, 31, 327–333. [DOI] [PubMed] [Google Scholar]
- Swendsen, J. , Burstein, M. , Case, B. , Conway, K.P. , Dierker, L. , He, J. et al. (2012) Use and abuse of alcohol and illicit drugs in us adolescents: results of the national comorbidity survey‐adolescent supplement. Archives of General Psychiatry, 69, 390–398. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vachon, D.D. , Krueger, R.F. , Irons, D.E. , Iacono, W.G. & McGue, M. (2017) Are alcohol trajectories a useful way of identifying at‐risk youth? A multiwave longitudinal‐epidemiologic study. Journal of the American Academy of Child and Adolescent Psychiatry, 56, 498–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Viner, R.M. & Taylor, B. (2007) Adult outcomes of binge drinking in adolescence: findings from a UKnational birth cohort. Journal of Epidemiology and Community Health, 61, 902–907. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waldron, J.S. , Malone, S.M. , McGue, M. & Iacono, W.G. (2017) Genetic and environmental sources of covariation between early drinking and adult functioning. Psychology of Addictive Behaviors, 31, 589–600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Waldron, J.S. , Malone, S.M. , McGue, M. & Iacono, W.G. (2018) A co‐twin control study of the relationship between adolescent drinking and adult outcomes. Journal of Studies on Alcohol and Drugs, 79, 635–643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Warnes, GR , Bolker, B , Lumley, T , Warnes, MGR (2015) Package ‘gtools’, R Package version, 3.
- White, H.R. & Labouvie, E.W. (1989) Towards the assessment of adolescent problem drinking. Journal of Studies on Alcohol, 50, 30–37. [DOI] [PubMed] [Google Scholar]
- WHO . (2016) Finland ‐ WHO . Available at: https://www.who.int/substance_abuse/publications/en/finland.pdf [Accessed 04th January 2022].
- Wickham, H , Francois, R , Lionel, H , Muller, K (2021) dplyr: A Grammar of Data (Version 1.0.7). Available at: https://CRAN.R‐project.org/package=dplyr
- Yap, M. , Jorm, A. , Bazley, R. , Kelly, C. , Ryan, S. & Lubman, D. (2011) Web‐based parenting program to prevent adolescent alcohol misuse: rationale and development. Australasian Psychiatry, 19, 339–344. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1