

Abstract
Axenfeld-Rieger syndrome (ARS) is a genetic disease affecting multiple organ systems. In the eye, it is associated with anterior segment dysgenesis with a high risk for glaucoma. Dental anomalies, cardiovascular malformations, hypospadias, and craniofacial abnormalities are other associated systemic conditions. Five years old monozygotic twin brothers with ARS were referred to Umraniye Training and Research Hospital, ophthalmology clinic for iris abnormalities. At presentation, pathognomonic components of ARS were found in both patients, including iris anomaly (corectopia, iris hypoplasia, and iris strands in Scwalbe’s ring), oligodontia, hypodontia, hypospadias, and periumbilical skin fold. Intraocular pressure was within normal ranges in both of the patients. Patients were followed up in the glaucoma unit.
Keywords: Axenfeld-Rieger syndrome, glaucoma, monozygotic, twins
Axenfeld-Rieger syndrome (ARS) is a genetic disease with prevalence of 1:200,000 [1]. Axenfeld reported a line in the posterior segment of the cornea as called “embryotoxon cornea posterius” in a patient in 1920 [2]. On the other hand, Rieger described two patients with similar phenotypes with increased iris stroma and congenital pupillary malformations. Rieger called this condition as “dysgenesis mesodermalis corneae et iridis” in 1934 [3]. Axenfeld anomaly (AA) was described as posterior embryotoxon and peripheral anterior adhesions, while axenfeld syndrome was associated with both AA and non-ocular defects. Rieger anomaly (RA) was the diagnosis for patient with ocular phenotypes including peripheral anterior adhesions, iris hypoplasia, polycoria, corectopia, and posterior embryotoxon, while Rieger syndrome includes both RA and systemic malformations. However, these four groups of disorders resulting from mutations of the same genes associated with deranged or arrested development of neural crest cells in the anterior chambers of the eyes, facial bones, teeth, periumbilical skin, and the cardiovascular system are now called ARS [4].
Herein, we present monozygotic twin brothers with ARS who were referred to our center from the local hospital for pupil abnormalities. As far as we know, this is the second report that has described monozygotic twins with ARS in the literature.
CASE REPORT
The monozygotic twin brothers were born in May 2010 after a full-term pregnancy. Both twin brothers received no ophthalmic attention until they were 5 years of age (October, 2015) when they were referred to a local hospital for routine ophthalmological examination. Bilateral pupil anomalies was diagnosed in the local hospital and they were referred to Umraniye Training and Research Hospital, ophthalmology clinic, glaucoma department. Diagnosis of ARS was made based on characteristic ocular and dental anomalies as shown in Table 1, (Fig. 1A, B; Fig. 2A, B). Periumblical skin fold and hypospadias are also present during presentation. Informed consent form has been signed by the parents for publication.
Table 1.
Main ocular features of twin brothers
| Elder brother | Elder brother | Younger brother | Younger brother | |
|---|---|---|---|---|
| (OD) | (OS) | (OD) | (OD) | |
| BCVA | 0.8 | 0.8 | 0.8 | 0.8 |
| IOP (mmHg) | 14 | 16 | 17 | 16 |
| Cup/disc ratio | 0.3 | 0.3 | 0.3 | 0.3 |
| Cornea diameter (mm) | 10 | 10 | 10.5 | 10.5 |
| Anterior chamber angle | Grade 3 | Grade 3 | Grade 3 | Grade 3 |
| Cornea endothelium count (cell/mm2) | 1870 | 1780 | 1900 | 1950 |
OD: Right eye; OS: Left eye; BCVA: Best corrected visual acuity; IOP: Intraocular pressure.
Figure 1.
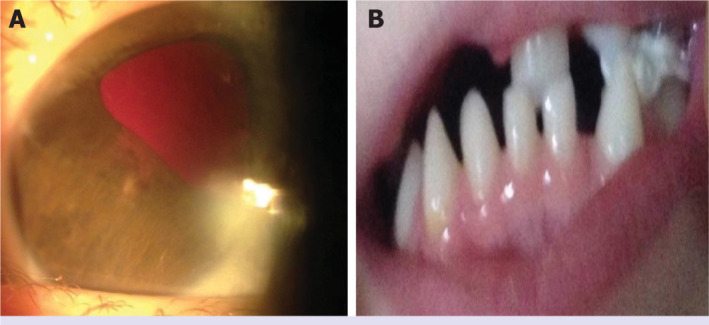
(A and B) Ocular and dental traits of the younger brother. Biomicroscopic photograph of the anterior segment of right eye showing irregular and corectopia pupil and iris abnormalities. The statement for “Figure 1” describes corectopia in two eyes, but shows corectopia in “Figure 1A” and dental anomaly in “Figure 1B”.
Figure 2.
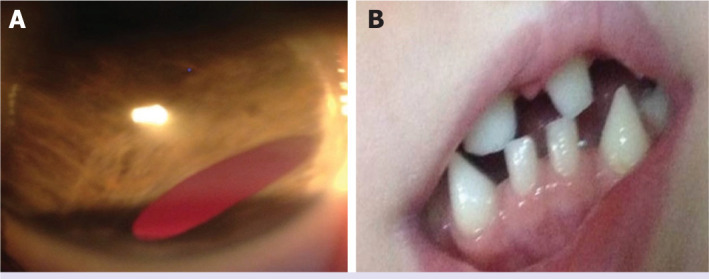
(A and B) Ocular and dental traits of the elder brother. Biomicroscopic photograph of the anterior segment of left eye showing irregular and corectopia pupil and iris abnormalities The statement for “Figure 1” describes corectopia in two eyes, but shows corectopia in “Figure 1A” and dental anomaly in “Figure 1B”.
DISCUSSION
ARS is an autosomal dominant disorder caused by abnormal migration of neural crest cells [5], which are involved in craniofacial, dental, and ocular development [6]. Two genes (PITX2 and FOXC1) are responsible for pathogenesis of Axenfeld-Rieger malformation. FOXC1 duplication is associated with the risk of glaucoma while PITX2 mutation is more likely to be associated with systemic findings [7]. Ocular involvement of ARS is usually bilateral and asymmetric. İris hypoplasia, corectopia, polycoria, posterior embryotoxon (anterior displacement of Schwalbe’s line), and glaucoma are major findings. Glaucoma is the most serious consequence of ARS and develops in approximately 50% of patients in childhood or early adulthood [8]. Posterior embryotoxon can be helpful in establishing a diagnosis of ARS but it does not necessarily make a diagnosis of ARS, as this finding occurs in 8–15% of the normal population [9]. The most significant findings in ARS are the iris abnormalities with a range of slight stromal atrophy to extremely minimal presence of iris tissue. Corectopia and pseudopolycoria are the most common anomalies [10]. Despite being striking, these abnormalities are not likely to be vision threatening. Extensions of the peripheral iris to Schwalbe’s line and trabecular meshwork and obscurance of the scleral spur [11] are common gonioscopic findings. Schlemm’s canal may be rudimentary or discontinuous in its development. Because of these changes in the trabecular meshwork and iris, individuals with ARS are at risk for developing glaucoma throughout the lifetime. Initial treatment of glaucoma involves topical medications; however, surgical interventions in the majority of cases are usually inevitable as disease progresses. Although goniotomy, trabeculectomy, and trabeculotomy were found to be effective trabeculectomy, antimetabolite treatment is usually preferred by most specialists [12].
ARS can also cause non-ocular systemic defects included dental anomalies, mild craniofacial dysmorphism, and redundant periumblical skin and abnormality of the cardiovascular outflow tract [8]. Craniofacial anomalies include hypertelorism, prominent forehead, telecanthus, maxillary hypoplasia, thin upper lip, flattened mid-face with a broad nasal bridge, and protruding lower lip [8, 13]. Dental anomalies included microdontia, hypodontia, oligodontia, anodontia, and cone-shaped teeth [13, 14]. Failure of involution in the periumbilical skin, umbilical or inguinal hernia, hypospadias, anal stenosis, or atresia is also abnormalities associated with ARS [10].
In this case report, we present monozygotic twin brothers with ARS. As far as, we know that this is the second case report in the literature concerning monozygotic twins with the ARS. In our case report, twin brothers presented with characteristic ocular anomalies of ARS including corectopia, iris hypoplasia, and iris strands in Scwalbe’s ring. Dental anomalies included microdontia, hypodontia, and oligodontia. Periumblical skin fold and hypospadias are also present during presentation. Ma et al. [15] presented two teenaged monozygotic twin sisters with ARS with typical components of ARS; iris anomaly, maxillary hypoplasia, hypodontia, and umbilical skin fold and both sisters received trabeculectomy in both the eyes. As glaucoma can be seen in 50% of ARS, routine follow-up in glaucoma department is crucial for this patients. Systematic surveillance of both ocular and extraocular abnormalities is also requisite for the correct diagnosis and treatment of ARS.
Footnotes
Cite this article as: Sezgin Akcay BI, Kardes E, Limon U. Axenfeld-Rieger syndrome in monozygotic twin brothers: Case report. North Clin Istanb 2022;9(4):411–413.
Informed Consent
Written informed consent was obtained from the patient for the publication of the case report and the accompanying images.
Conflict of Interest
No conflict of interest was declared by the authors.
Financial Disclosure
The authors declared that this study has received no financial support.
Authorship Contributions
Concept – BISA; Design – EK; Supervision – EK; Materials – UL; Data collection and/or processing – BISA; Analysis and/or interpretation – UL; Literature review – EK; Writing – BISA; Critical review – UL.
References
- 1.Meyer-Marcotty P, Weisschuh N, Dressler P, Hartmann J, Stellzig-Eisenhauer A. Morphology of the sella turcica in Axenfeld-Rieger syndrome with PITX2 mutation. J Oral Pathol Med. 2008;37:504–10. doi: 10.1111/j.1600-0714.2008.00650.x. [DOI] [PubMed] [Google Scholar]
- 2.Axenfeld T. Embryotoxon corneae posterious. Ber Deutsch Ophthalmol Ges. 1920;42:301–2. [Google Scholar]
- 3.Rieger H. Dysgenesis mesodermalis corneae et iridis. Z Augenheilkd. 1935;86:333. [Google Scholar]
- 4.Seifi M, Walter MA. Axenfeld-Rieger syndrome. Clin Genet. 2018;93:23–30. doi: 10.1111/cge.13148. [DOI] [PubMed] [Google Scholar]
- 5.Bahn CF, Falls HF, Varley GA, Meyer RF, Edelhauser HF, Bourne WM. Classification of corneal endothelial disorders based on neural crest origin. Ophthalmology. 1984;91:558–63. doi: 10.1016/s0161-6420(84)34249-x. [DOI] [PubMed] [Google Scholar]
- 6.Childers NK, Wright JT. Dental and craniofacial anomalies of Axenfeld-Rieger syndrome. J Oral Pathol. 1986;15:534–9. doi: 10.1111/j.1600-0714.1986.tb00572.x. [DOI] [PubMed] [Google Scholar]
- 7.Chang TC, Summers CG, Schimmenti LA, Grajewski AL. Axenfeld-Rieger syndrome: new perspectives. Br J Ophthalmol. 2012;96:318–22. doi: 10.1136/bjophthalmol-2011-300801. [DOI] [PubMed] [Google Scholar]
- 8.Tümer Z, Bach-Holm D. Axenfeld-Rieger syndrome and spectrum of PITX2 and FOXC1 mutations. Eur J Hum Genet. 2009;17:1527–39. doi: 10.1038/ejhg.2009.93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Waring GO, 3rd, Rodrigues MM, Laibson PR. Anterior chamber cleavage syndrome. A stepladder classification. Surv Ophthalmol. 1975;20:3–27. doi: 10.1016/0039-6257(75)90034-x. [DOI] [PubMed] [Google Scholar]
- 10.Mandal AK, Netland PA. The Pediatric Glaucomas. Elsevier. 2006. p. 41.
- 11.Idrees F, Vaideanu D, Fraser SG, Sowden JC, Khaw PT. A review of anterior segment dysgeneses. Surv Ophthalmol. 2006;51:213–31. doi: 10.1016/j.survophthal.2006.02.006. [DOI] [PubMed] [Google Scholar]
- 12.Shields MB, Buckley E, Klintworth GK, Thresher R. Axenfeld-Rieger syndrome. A spectrum of developmental disorders. Surv Ophthalmol. 1985;29:387–409. doi: 10.1016/0039-6257(85)90205-x. [DOI] [PubMed] [Google Scholar]
- 13.O’Dwyer EM, Jones DC. Dental anomalies in Axenfeld-Rieger syndrome. Int J Paediatr Dent. 2005;15:459–63. doi: 10.1111/j.1365-263X.2005.00639.x. [DOI] [PubMed] [Google Scholar]
- 14.Jena AK, Kharbanda OP. Axenfeld-Rieger syndrome: report on dental and craniofacial findings. J Clin Pediatr Dent. 2005;30:83–8. doi: 10.17796/jcpd.30.1.v1732398454r0244. [DOI] [PubMed] [Google Scholar]
- 15.Ma J, Zhong Y, Zhao C, Zhang X, Sui R, Chu P, et al. Axenfeld-Rieger syndrome in monozygotic twins. J Glaucoma. 2011;20:584–6. doi: 10.1097/IJG.0b013e3181f7b258. [DOI] [PubMed] [Google Scholar]