

Abstract
The present study used a minority stress theory framework to investigate the direct and indirect relations of minority stressors (transgender discrimination experiences, internalized transphobia, identity nondisclosure), sense of belonging, and hopelessness with depression and anxiety symptoms in a sample of 301 trans and gender-diverse adults living in the United States. This study also explored the moderating effect of having knowledge of antitrans legislative efforts in one’s state of residence on the overall pattern of results through a nested model comparison of the hypothesized path analysis. Participants were recruited using Internet-based forums, listservs, and social media, and survey data were collected online. Significant moderation effects were found, such that for those who reported having knowledge of antitrans legislative efforts in their state of residence reported a stronger association of external stressors (discrimination) than internal stressors (internalized transphobia, identity nondisclosure) on sense of belonging and hopelessness than their peers who did not have any knowledge of such legislative efforts. Furthermore, hopelessness emerged as a stronger predictor for those who were aware of antitrans legislative efforts. Implications of study findings for counseling, advocacy, and future research are discussed.
Keywords: minority stress, social belongingness, hopelessness, trans policy
In 2014, trans actress, documentary film producer, and equal rights advocate Laverne Cox was featured on the cover page of TIME magazine (Steinmetz, 2014). She stood elegantly and proudly, the words “The transgender tipping point: America’s next civil rights frontier” blazoned next to her against a blank backdrop that seemed to capture the optimism for a better future, one of infinite possibilities for transgender and gender-diverse (TGD) people in the United States. However, only 2 years later, the Human Rights Campaign released a report (Ennis, 2016), calling 2016 “the most dangerous year” as a wave of antitransgender legislation was introduced in state legislative bodies around the country. Melissa Gira Grant succinctly noted in her 2016 essay, “the flip side of visibility … is vulnerability” (Grant, 2017).
Theoretical Frameworks
Research has shown that TGD people are at greater risk than many of their cisgender peers for higher rates of mental and physical health concerns, with such concerns robustly linked in the literature to antitrans stigma, prejudice, and discrimination (Bockting et al., 2013; Budge et al., 2013; Tebbe & Moradi, 2016; Testa et al., 2017). Minority stress theory is a helpful framework for explaining the higher rates of mental health concerns for TGD populations (Brooks, 1981; Meyer, 2003). Minority stress theory holds that members of stigmatized populations experience stress above and beyond that of general, daily stress. Minority stress occurs proximally, or internal to the self, and distally, or external to the self, and can lead to adverse mental and physical health over time. Examples of proximal stress include internalized negative attitudes about one’s personal identity; fear or expectation of experiencing identity-based stigma, prejudice, and discrimination; and concealing or not disclosing one’s stigmatized identity when it is invisible to others. Examples of distal stress include experiencing prejudice, discrimination, violence, harassment, and social rejection in response to one’s identity.
Although initially developed to explain health disparities among lesbian, gay, bisexual, and other sexual minority populations (e.g., Brooks, 1981; Meyer, 2003), key tenets of minority stress have since been applied to TGD populations, with research finding robust and direct links of proximal and distal stressors with adverse mental health. For example, numerous studies have demonstrated that experiences of trans-related prejudice, discrimination, harassment, and physical and sexual violence are associated with depression and suicide risk (e.g., Bockting et al., 2013; Clements-Nolle et al., 2006; Tebbe & Moradi, 2016; Testa et al., 2015). Additionally, proximal stressors are uniquely associated with psychological distress across community samples of TGD adults, even in models that included distal forms of minority stress (Bockting et al., 2013; Tebbe & Moradi, 2016).
Although much of the research to date has focused on the forms of minority stress that occur in interpersonal interactions and through internalized psychosocial processes, a growing body of literature suggests that structural stigma, or stigma that manifests within systems and institutions in the form of societal-level conditions, norms, and institutional policies, also acts to constrain the opportunities, resources, and well-being of individuals with stigmatized identities (Hatzenbuehler & Link, 2014). Indeed, some recent research has found that antitrans stigma that manifests within systems and institutions contributes to minority stress for many TGD individuals, with adverse impacts on psychological well-being (e.g., Davis & Wertz, 2009; Shumer et al., 2016; Tebbe et al., 2018). Measuring structural antitrans stigma is necessarily conceptually and methodologically complex, but one particular form that can more readily be captured is the codification of antitrans sentiment and discrimination through the introduction of antitrans legislation.
In 2016, it was estimated that approximately 300,000 trans youth and adults in the United States were affected by state legislation that was introduced to limit access to public accommodations, reduce protections, and permit discrimination (Herman et al., 2016). Although many of those bills have since failed to be signed into law, new legislation has been introduced each year targeting TGD people. For example, in early 2020, bills were introduced in states around the country criminalizing the provision of hormones, puberty blockers, or any other medical transition support to those under 18; prohibiting transgender youth from participating in sports; and making it impossible to change legal gender on some identity documents. Many of these bills have similarly failed (Freedom for All Americans, n.d.). However, in the process of being filed or introduced, these bills have often generated very intense public discussion and debate, with TGD advocates high-lighting the potential harm such legislation may have on TGD people and proponents of the legislation arguing they are necessary to protect vulnerable persons, most often cisgender women and girls. As a result, even when bills are not signed into law, the exposure to the discourse surrounding their introduction to state legislative agendas has the potential to be damaging. For example, when LGB individuals were asked to describe their reactions to marriage amendment efforts that were on the ballot in nine states in the 2006 midterm elections. Qualitative themes that emerged included indignation about discrimination, distress resulting from the negative rhetoric surrounding the campaigns, and fear and anxiety related to future family life and structures (Rostosky et al., 2010). Notably, the same themes emerged for participants who lived in states where the marriage amendment passed as they did for participants where the marriage amendment failed.
As a result, an underexplored but particularly timely form of antitrans stigma that increases stress for many TGD people is the wave of antitrans legislative efforts sweeping across the nation. Some preliminary evidence suggests that awareness of legislation that has been introduced (whether it passed or not) in one’s state of residence may act to shape or moderate the effects of inter- and intrapersonal forms of minority stress on adverse health. For example, in a recent study that investigated the impact of legal protections from employment discrimination in a sample of TGD working adults, researchers found that knowledge of legal protections buffered the deleterious impact of antitrans interpersonal experiences on internal vocational processes (Tebbe et al., 2018). However, more research is needed to determine if legislation aimed at curbing, rather than protecting, the rights of TGD people has a similar albeit inverse moderating effect on mental health among TGD community members. With lawmakers across the country targeting TGD individuals’ access to identity-affirming documents, spaces, and services, legislative efforts may contribute to increased stress associated with disclosing one’s identity to others, internalizing antitrans attitudes, and experiences of prejudice and discrimination.
Sense of Belonging and Hopelessness as Explanatory Links
Although research has generally supported the empirical links of minority stress with adverse health outcomes in sexual and gender minority populations, Hatzenbuehler (2009) notes the critical importance of also identifying the psychological mechanisms by which stigma-related stress may be linked to adverse health. In his psychological mediation framework, developed with and for sexual minority populations, Hatzenbuehler proposes that stigma-related stress leads to elevated problems with emotion dysregulation, social/interpersonal problems (e.g., social isolation), and cognitive processes (e.g., hopelessness, low self-esteem). In turn, it is these psychological mechanisms and processes that lead to psychopathology.
Two particular psychological processes by which minority stress may be linked with adverse mental health in TGD populations are sense of belonging and hopelessness, spanning the domains of social/interpersonal problems and cognitive processes delineated by Hatzenbuehler (2009). Sense of belonging is a vital component of mental health (Hagerty et al., 1992), and its absence has been associated with loneliness, hopelessness, depression, and psychological distress (Fisher et al., 2015; Hagerty & Patusky, 1995). Although individuals may affiliate with more than one group or community, some evidence suggests that sense of belonging—or, more specifically, its absence—to the larger collective may predict adverse mental health more than sense of belonging to one’s specific communities. For example, in a sample of Australian gay men, sense of belonging to gay friends and to the general (largely heterosexual) population was a stronger mediator of the links of internalized heterosexism with depressive symptoms than was participants’ sense of belonging to gay groups or gay community (Davidson et al., 2017). Moreover, sense of belonging to the general community had a greater direct effect with depressive symptoms than sense of belonging to gay friends, groups, or community. In research with trans youth, school belonging, or the sense of belonging one has to their larger school community, mediated the associations of distal minority stress with mental health and substance use (Hatchel et al., 2019; Hatchel & Marx, 2018). Thus, alongside concurrent efforts in legislatures across the country to limit trans individuals’ access to various institutional resources and structures and the negative discourse accompanying such efforts, sense of belonging may be a particularly timely and critical psychological mechanism to investigate in helping to understand how antitrans stigma may relate to adverse mental health.
With numerous barriers to economic stability, educational opportunity, career and employment advancement, and trans-competent and affirming health resources for many TGD persons in the United States today (James et al., 2016), hopelessness is a particularly critical response to consider in understanding the links of minority stress with adverse mental health in TGD populations. In a recent qualitative study with transgender adults, participants described feelings of hopelessness as a response to the daily lived experience of antitrans stigma (Nadal et al., 2014). The consequences of hopelessness in mental health can be severe; empirically, hopelessness has been found to be one of the strongest predictors of suicide risk across populations, including in LGBT populations (Beck et al., 1993; Mustanski & Liu, 2013). Theoretically, Hatzenbuehler (2009) proposes hopelessness as one cognitive process by which antitrans stigma may be linked to adverse mental health. As a result, investigating hopelessness as a possible mediator in the links between minority stress and adverse mental health may generate critical knowledge regarding the identification of mechanisms to target in the development of prevention strategies aimed at reducing mental health disparities within TGD communities.
Present Study
In the present study, we draw from minority stress theory (Meyer, 1995, 2003) and Hatzenbuehler’s psychological mediation and structural stigma frameworks (Hatzenbuehler, 2009, 2016) to test the moderating effect of one form of structural stigma (state antitrans legislative efforts) on the association of minority stressors (internalized transphobia, identity nondisclosure, discrimination experiences) with depressive and anxiety symptoms through the mediating role of sense of belonging and hopelessness. We hypothesize the following direct effects: internalized transphobia, identity nondisclosure, and discrimination experiences will be negatively associated with sense of belonging (H1–H1c) and positively associated with hopelessness (H2a–H2c); hopelessness will be positively associated with depressive symptoms (H3) and anxiety symptoms (H4); social belonging will be negatively associated with depressive symptoms (H5) and anxiety symptoms (H6). We also hypothesize the following indirect effects: internalized transphobia (H7a–H7d), identity nondisclosure (H8a–H8d), and discrimination experiences (H9a–H9d) will be indirectly associated with depressive and anxiety symptoms through sense of belonging and hopelessness. On the overall pattern of hypothesized relations among study variables, we will also explore the moderating effect of antitrans legislative efforts. We hypothesize that knowledge of antitrans legislative efforts in one’s state of residence will change the pattern of relations among study variables. At this time, however, our ability to specify the direction of such changes when all variables are considered together is limited by the dearth of existing research to date. As a result, this hypothesized moderation represents an exploratory aim of the present study.
Method
Participants
The sample consisted of 301 adults who self-identified as transgender and/or gender diverse. Participants ranged in age from 18 to 68 (M = 27.2, SD = 9.2, Mdn = 24). Participants completed a demographics questionnaire where they were able to select more than one response to each category; thus, total percentages may exceed 100%. Regarding gender identity, 27 gender identity options were provided (e.g., “male and/or man,” “female and/or woman,” “trans man [FTM, female-to-male],” “genderqueer,” “agender”). Over half of participants identified with a binary gender identity of “female and/or woman” (46.2%) or “male and/or man” (16.3%). In the total sample, participants also identified as genderqueer (4.3%), gender nonconforming (6.3%), transgender (13.0%), androgynous (3.3%), agender (3.0%), gender fluid (2.3%), third gender (.3%) and two-spirit (.3%), and with other categories, such as stud, part-time, butch, and gender variant, and a notable number wrote in their identity as “nonbinary” (6.5%).
Regarding race and ethnicity, participants identified as American Indian (1.3%), Asian or Asian American (4.7%), Black or African American (2.3%), Latinx (6.6%), Native Hawaiian (1.0%), White (81.1%), and with a different race (5.0%; e.g., “Mixed race,” “Mediterranean”). Participants also identified their sexual orientation identities as asexual (13.0%), bisexual (27.9%), gay (9.0%), straight or heterosexual (7.0%), lesbian (19.9%), pansexual (24.3%), queer (23.6%), and/or with another sexual orientation identity (6.0%; e.g., “gynosexual,” “transbian,” “demisexual,” “anything-but-cis-dudes”). The majority of participants reported having attended some college (40.9%) or having earned a college degree (24.6%), while a smaller proportion reported holding a trade or vocational degree (.7%) or a professional degree (8.0%). The remaining participants reported completing some or all of high school (16.6%) or never entering high school (2.0%). Regarding employment, participants worked full-time (7.6%) or part-time (9.6%), were self-employed (4.7%), were on disability (4.0%), were students (22.3%), were retired (1.3%), were unemployed (11.2%), or indicated a different employment status (6.0%).
Measures
Experiences of Discrimination
The 21-item Trans Discrimination Scale (TDS-21; Watson et al., 2019) measures transgender individuals’ experiences of discrimination and prejudice over the course of their lifetime. For the purposes of the present study, we adapted instructions to ask participants to indicate whether they had experienced specific discrimination and prejudice events in the past 2 years. Each item contains the following stem, “Because of others’ transgender prejudice, how often have you. …” An example item on the TDS-21 is “experienced harassment (e.g., slurs, physical harm, prolonged ‘pat downs’) from law enforcement?” Participants were asked to rate items on a scale from 1 (the event has not happened to you in the past 2 years) to 5 (the event happened almost all of the time; more than 70% of the time). Item ratings are averaged to produce total scale scores, with higher scores indicating a greater frequency of discrimination events. Regarding validity, the TDS-21 has been positively associated with measures of heterosexist harassment and discrimination in a community sample of trans adults (Watson et al., 2019). Regarding reliability, in the same sample, Cronbach’s alpha was .90 (Watson et al., 2019). In the present study, Cronbach’s alpha was .92.
Internalized Transphobia
The Internalized Transphobia Subscale of the Gender Minority Stress and Resilience Measure (GMSR; Testa et al., 2015) is composed of eight items measuring the internalization of transphobic attitudes. An example item of the Internalized Transphobia Subscale is, “I resent my gender identity or expression.” Items are rated from 1 (strongly disagree) to 5 (strongly agree). Overall scores are computed by averaging item scores, with higher scores indicate greater levels of internalized transphobia. Regarding validity, the GMSR has been positively associated with adverse mental health anxiety, depression, and stress (Testa et al., 2015), while its reliability in the same sample of trans adults was also good, with a Cronbach’s alpha of .91 (Testa et al., 2017). In the present study, Cronbach’s alpha was .90.
Identity Nondisclosure
The Identity Nondisclosure subscale of the GMSR is composed of five items measuring nondisclosure strategies trans individuals might use in response to privacy and/or safety concerns (Testa et al., 2015). A sample item is “Because I do not want others to know my gender identity/history, I pay special attention to the way I dress or groom myself.” Items are rated from 1 (strongly disagree) to 5 (strongly agree). Overall scores were computed by averaging item scores, and higher scores indicate greater levels of nondisclosure. Regarding validity, in a sample of trans adults, the Nondisclosure subscale has been positively correlated with adverse mental health, such as depression, anxiety, and stress (Testa et al., 2015), and demonstrated discriminant validity with statistical independence from thwarted belongingness and perceived burdensomeness (Testa et al., 2017). Regarding reliability, the Nondisclosure subscale demonstrated adequate internal consistency with a Cronbach’s alpha of .79 in the same sample (Testa et al., 2017). Cronbach’s alpha in the present study was .85.
Sense of Belonging
The Sense of Belonging Instrument–Psychological subscale (SBI; Hagerty & Patusky, 1995) is composed of 18 items measuring two core aspects of sense of belonging: involvement (“I could disappear for days and it wouldn’t matter to my family”) and fit (“I often wonder if there is any place on earth where I really fit in”). Items are rated from 1 (strongly disagree) to 4 (strongly agree). Overall scores were computed by averaging item scores, with higher scores indicating greater sense of belonging. Regarding validity, the SBI was associated with loneliness, reciprocity, and social support in samples of community college students, adults in treatment for depression, and Roman Catholic nuns (Hagerty & Patusky, 1995). Regarding reliability, the SBI has demonstrated good internal consistency, with Cronbach’s alphas ranging from .91 to .93 across the same three samples (Hagerty & Patusky, 1995). In the present study, Cronbach’s alpha was .93.
Hopelessness
The degree to which participants experienced hopelessness was measured using the 10 items from the Hopelessness subscale of the Hopelessness, Helplessness, and Haplessness Scale (Lester, 2001). An example item is, “It is very unlikely I will get any real satisfaction in the future.” Items are rated from 1 (strongly agree) to 6 (strongly disagree). Overall scores are averaged, with higher scores indicating greater hopelessness. Regarding validity, Lester and Walker (2007) found that scale scores were positively associated with suicidality and another measure of hopelessness in a nonclinical sample of adults. Regarding reliability, in a sample of undergraduate students, Cronbach’s alpha was .80 (Lester, 2001). In the present study, Cronbach’s alpha was .91.
Depressive Symptoms
Depressive symptoms were measured using the Center for Epidemiological Studies Depression Scale–Revised (Eaton et al., 2004). The CESD-R comprises 20 items reflecting nine symptomatic criteria of depression: dysphoria, anhedonia, appetite, sleep, thinking/concentration, worthlessness, tired/fatigue, agitation/retardation, and suicidal ideation. An example item is, “Nothing made me happy.” Participants are instructed to indicate how often they have felt each symptom in the past 2 weeks on a 5-point scale ranging from 0 (not at all) to 4 (nearly every day for 2 weeks). Item ratings are averaged to produce total scores, with higher scores reflecting greater levels of depressive symptoms. The CESD-R is used primarily with general, outpatient populations, where a total score of 17 or more indicates levels of depressive symptoms that would be associated with a clinical diagnosis of depression (Eaton et al., 2004). Regarding validity, the CESD-R has been associated with anxiety, positive and negative affect, and suicidality in diverse community samples (Eaton et al., 2004). Regarding reliability, Cronbach’s alpha has ranged from .90 or higher across diverse community samples (Eaton et al., 2004). In the present study, Cronbach’s alpha was .94.
Anxiety Symptoms
Anxiety symptoms were measured using the Burns Anxiety Inventory (BAI; Burns, 1998). The BAI is a 33-item self-report measure of the degree to which participants were bothered by three domains of anxiety symptoms over the past week: anxious thoughts, anxious feelings, and physical sensations. Response options range from 0 (not at all) to 3 (a lot). Sample items include “difficulty concentrating” and “pain, pressure, or tightness in the chest.” Overall scores are averaged, with higher scores indicating greater anxiety. Regarding validity, the BAI was positively correlated with depression and avoidant coping in the same sample (Budge et al., 2013). Regarding reliability, in a sample of transgender individuals, the BAI demonstrated good internal consistency, with a Cronbach’s alpha of .95 (Budge et al., 2013). Cronbach’s alpha in the present study was .95.
Knowledge of Antitrans Legislation
Participants’ knowledge of antitrans legislative efforts in their state of residence was assessed using two items that were created for the purposes of this study. “To your knowledge, has the city, county, or state in which you currently live introduced or passed legislation” and assessed for “restricting trans individuals’ right to use gender-appropriate bathroom or locker room” and “requiring proof of gender confirmation surgery for someone to change the gender marker on an identity document?” Response options were “yes,” “no,” and “do not know.” To assess knowledge of antitrans legislative efforts, responses were dichotomized such that participants who responded “yes” were considered to have knowledge of antitrans legislative efforts in their state, while a “no” or “do not know” indicated that participants were not aware of such efforts in their state.
Procedure
This study was approved by the institutional review board at a large university in the midwestern United States. Participants were recruited nationally through variety of online forums, including Reddit threads and Facebook groups for transgender individuals and email listservs through university LGBTQ centers. All recruitment posts were approved by moderators of the individual group and/or site in order to respect these community spaces, and the researcher leading recruitment responded to prospective participants’ questions or comments on a regular basis (see Tebbe & Budge, 2016). This study was advertised as an exploration of transgender individuals’ experiences of recent U.S. legislation and policy efforts related to access to bathrooms and locker rooms, health care access, and identity documents.
In order to participate in the study, respondents had to affirm that they were (a) at least the age of majority in the state where they reside (19+ in Nebraska and Alabama; 18 years or older in other states), (b) reside in the United States, and (c) identify as trans, gender nonconforming, or gender diverse. All study measures were administered online using Qualtrics. Participants had the choice to enter their email into a separate confidential Qualtrics survey in order to enter a lottery for one of twenty $25 e-gift cards. After completing the survey, participants received contact information about local and national mental health support and community resources.
Statistical Analysis
All model assumptions and sample descriptive statistics were tested with IBM SPSS 25 computer software. All path analyses were tested using Mplus 7 (Muthén & Muthén, 2011). A series of one-way analysis of variance (ANOVA) tests were run to identify mean differences on study variables between those who knew about antitrans legislative efforts in their states of residence and those who did not. Path analyses were conducted to investigate the direct and indirect effects of the relations of transgender discrimination (X1), identity nondisclosure (X2), and internalized transphobia (X3) with depressive (Y1) and anxiety (Y2) symptoms, through the roles of hopelessness (M1) and sense of belonging (M2). Per scholarly recommendations, mediation effects were estimated using bias-corrected bootstrap resampling (MacKinnon et al., 2004). Mediation effects are deemed significant if their 95% confidence intervals do not contain 0 (Mallinckrodt et al., 2006). We used the following scholarly recommendations for assessing model fit: chi-square statistic where p ≤.05, comparative fit index (CFI) ≥.95, root mean square error of approximation (RMSEA) ≤.08, standardized mean square residual (SRMR) ≤.06, and Tucker–Lewis Index (TLI) ≥.95 (Hu & Bentler, 1998, 1999).
For our exploratory aim of determining whether knowledge of antitrans legislation in one’s state of residence acted to moderate the overall pattern of relations of minority stressors with sense of belonging, hopelessness, and depressive and anxiety symptomatology, nested model comparisons were conducted, where the pattern of the strength of associations among study variables was compared between individuals who had knowledge that antitrans legislation had been introduced in their state and those who did not. Thus, first a nested path analysis was fit where the effects were allowed to vary across the two groups. In a second step, the paths were constrained to be equal across both groups, and a chi-square difference test was examined to determine whether the model with equal or constrained estimates fit the data better.
Results
Preliminary analyses were conducted to assess missing data, obtain descriptive and bivariate correlational statistics among study variables (see Table 1), and assess any within-sample variation in study predictors and outcomes. The level of missingness in the study data at the item level was deemed acceptable (e.g., < 10%; Bennett, 2001). Specifically, missing data ranged from 4.9% to 7.1% for study predictors, 6.8% to 7.1% for mediators, and 5.5% to 5.8% for study outcomes. As such, all available data for each participant were included in the model. In the total sample, applying the Van Dam and Earleywine (2011) classification algorithm for CESD-R scores that aligns with modern diagnostic criteria for major depressive disorder (MDD; American Psychiatric Association, 2013), 32.2% of participants reported levels of depressive symptoms to be classified as probable for an MDD diagnosis. Regarding anxiety, 71.4% reported moderate or higher levels of anxiety. The majority of the sample reported living in a state that had not introduced or did not know if any antitrans legislation had been introduced (71.4%; Group 1), while the remainder reported that they lived in a state where antitrans legislation had been introduced (28.6%; Group 2). Preliminary ANOVA tests revealed that participants who were aware of legislation efforts in their state reported higher frequency of discrimination and greater depressive symptoms, as well as decreased sense of belonging compared to those who did not have such knowledge (see Table 2).
Table 1.
Sample Descriptive Statistics by Group
| Variable | Group 1 | Group 2 | Group comparisonsa | |||
|---|---|---|---|---|---|---|
| M | SD | M | SD | F | p value | |
| Minority stress predictors | ||||||
| Transgender discrimination | 2.22 | 0.89 | 2.55 | 0.92 | 8.09 | <.01 |
| Identity nondisclosure | 3.75 | 1.02 | 3.77 | 1.00 | 0.03 | .85 |
| Internalized transphobia | 2.95 | 1.11 | 3.03 | 0.99 | 0.31 | .58 |
| Mediating processes | ||||||
| Hopelessness | 3.32 | 1.03 | 3.55 | 0.87 | 3.32 | .07 |
| Sense of belonging | 2.69 | 0.66 | 2.90 | 0.60 | 6.51 | .01 |
| Psychological health outcomes | ||||||
| Depressive symptoms | 1.51 | 0.99 | 1.79 | 0.97 | 5.13 | .02 |
| Anxiety symptoms | 1.05 | 0.63 | 1.19 | 0.61 | 3.30 | .07 |
Note. Group 1 = individuals who do not have knowledge of antitrans legislation introduced in their state of residence. Group 2 = individuals who have knowledge of antitrans legislation introduced in their state of residence.
Values derived from a series of one-way analyses of variance. Bold font indicates significant differences at p < .05.
Table 2.
Bivariate Correlations Among Study Variables for Overall Sample
| Variable | TDS | IT | ND | SBI | HOPE | CESD-R | BAI |
|---|---|---|---|---|---|---|---|
| TDS | — | ||||||
| IT | .27 | — | |||||
| ND | .27 | .45 | — | ||||
| SBI | .45 | .57 | .40 | — | |||
| HOPE | .36 | .44 | .22 | .71 | — | ||
| CESD-R | .42 | .42 | .29 | .65 | .65 | — | |
| BAI | .45 | .41 | .26 | .61 | .56 | .78 | — |
| M | 2.31 | 2.98 | 3.76 | 2.75 | 3.21 | 31.75 | 35.93 |
| SD | .91 | 1.08 | 1.01 | .65 | 1.10 | 19.80 | 20.74 |
| α | .92 | .90 | .85 | .93 | .91 | .94 | .95 |
Note. All bivariate correlations were significant at p < .001. TDS = Transgender Discrimination Scale; IT = Internalized Transphobia subscale of the Gender Minority Stress and Resilience Measure (GMSR); ND = Identity Nondisclosure subscale of the GMSR; SBI = Sense of Belonging Instrument–Psychological subscale; CESD-R = Center for Epidemiological Studies Depression–Revised; BAI = Burns Anxiety Inventory.
For study analyses, because all possible direct and indirect relations among study variables were included in the hypothesized path analysis, the first study model tested was saturated (i.e., there were insufficient degrees of freedom to achieve model fit indices). Therefore, nonsignificant paths were removed to increase model parsimony, which also allowed for model fit indices to be estimated. Only identity nondisclosure with hopelessness was non-significant, and this path was thus dropped from the model. Modification indices also indicated a better fit of the data to the model with the addition of a covariance path between sense of belonging and hopelessness. After these modifications, data fit this model well: χ2(1) = .08, p = .77, CFI = 1.00, TLI = 1.00, RMSEA < .001 (90% CI [.00, .10]), SRMR = .003.
Moderation Analysis
Knowledge of antitrans legislation introduced in one’s state of residence was used as a grouping variable to conduct the nested model comparisons of the path analysis. In the first step where the paths were constrained to be equal, model fit indices were as follows: χ2(17) = 26.45, p = .07, CFI = .99, TLI = .98, RMSEA = .06 (90% CI [.00, .10]), SRMR = .05. These model fit indices were compared to those where the paths were allowed to vary freely between results, which yielded the following fit statistics χ2(2) = .87, p = .65, CFI = 1.00, TLI = 1.00, RMSEA < .001 (90% CI [.00, .13]), SRMR = .01. The chi-square difference between the two models was significant, Δχ2(15) = 25.59, p = .04. This suggests that a significant moderation of the overall pattern occurred based on knowledge of antitrans legislation efforts in one’s state of residence. As a result, we present findings from the two group models separately below.
Path Analysis Results for Individuals Who Do Not Have Knowledge of Antitrans Legislation Introduced in One’s State of Residence (Group 1)
The results from the path analysis supported the remaining study hypotheses (see Figure 1). Specifically, the direct effects of transgender discrimination, identity nondisclosure, and internalized transphobia were negatively associated with sense of belonging (a11, a12, a13). Transgender discrimination and internalized transphobia were positively associated with hopelessness (a21, a22). Also as hypothesized\hbox{,} sense of belonging was negatively associated with depressive and anxiety scores (b11\hbox{,} b12) and hopelessness was positively associated with depressive and anxiety scores (b21\hbox{,} b22).
Figure 1.
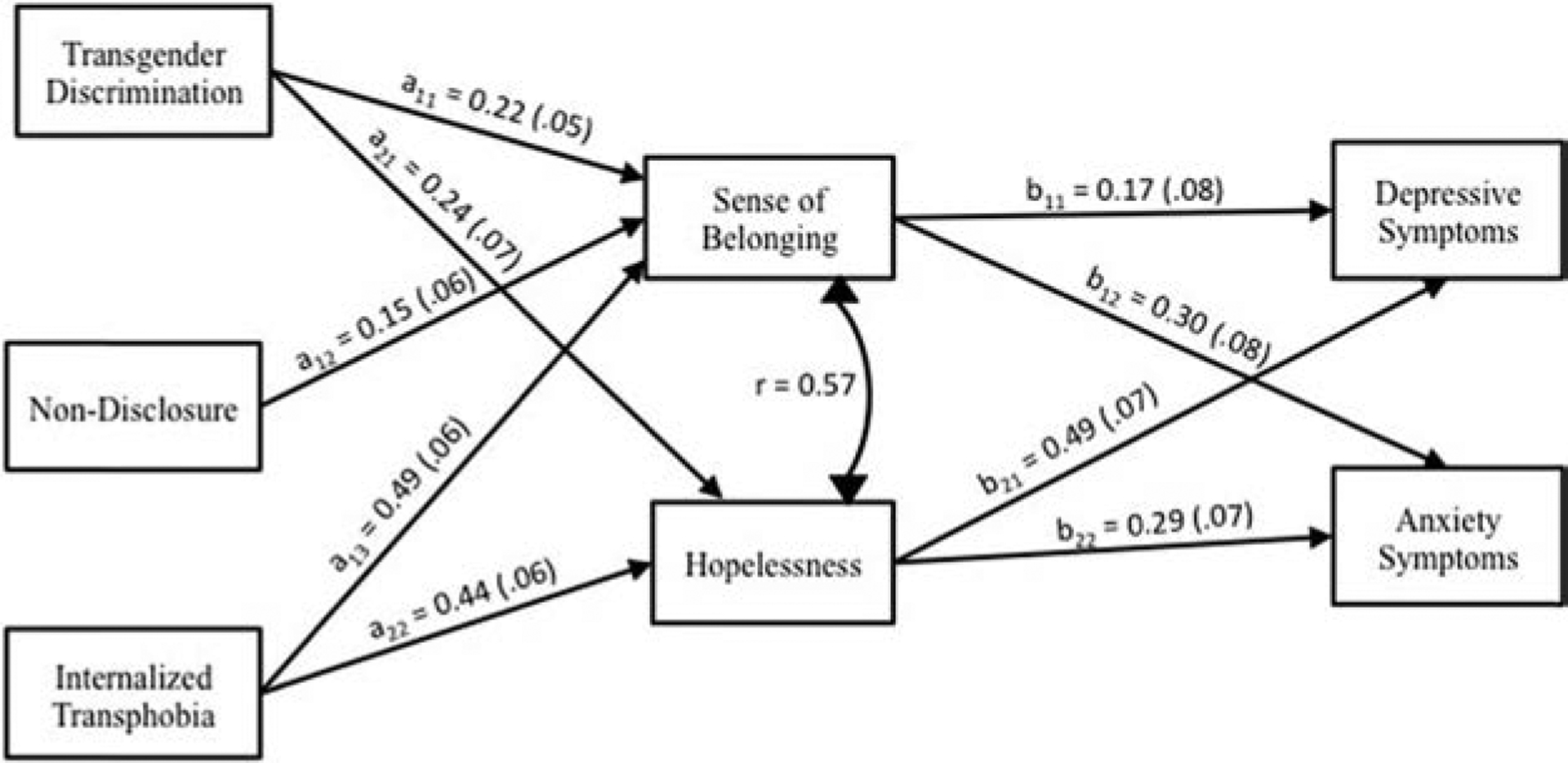
Path Analysis Results for Transgender and Gender-Diverse Adults Who Are Not Aware of Antitrans Legislation Introduced in Their State of Residence (Group 1)
Depressive Symptoms.
Atemporal mediation analysis revealed that the relation of transgender discrimination with depressive symptoms was mediated by hopelessness in the hypothesized direction (see Figure 1) but not by sense of belonging. The atemporal mediating pathway of hopelessness explained 39% of the total effect of transgender discrimination on depressive symptoms. Similarly, internalized transphobia was indirectly associated with depressive symptoms through hopelessness but not sense of belonging. The atemporal mediating role of hopelessness explained 65% of the total effect of internalized transphobia on depressive symptoms. Finally, the relationship between identity nondisclosure and depressive symptoms was not mediated by sense of belonging.
Anxiety Symptoms.
Atemporal mediation analysis revealed that the relation of transgender discrimination with anxiety symptoms was mediated by both hopelessness and social belongingness in the hypothesized direction (see Figure 1). The mediating pathway of hopelessness and sense of belonging each explained 18% of the total effect of transgender discrimination on anxiety symptoms. Similar findings were also found regarding the indirect links of internalized transphobia with anxiety symptoms through both hopelessness and sense of belonging; atemporal mediated pathways involving hopelessness explained 43% of the total effect, and sense of belonging explained 50% of the total effect on anxiety symptoms. Finally, identity nondisclosure was indirectly related to anxiety symptoms through sense of belonging, with the mediating pathway explaining 50% of the total effect on anxiety symptoms (see Table 3 for all direct and indirect effects for Group 1).
Table 3.
Nested Mediated Path Analysis for Group 1: Individuals Who Do Not Have Knowledge of Antitrans Legislation Introduced in Their State of Residence
| Mediated Path Estimates | Proportion mediateda | β | SE | p value | Adjusted 95% CIs |
|---|---|---|---|---|---|
| Outcome: Depressive symptoms | |||||
| M1: Discrimination → Hopelessness → Depression | |||||
| Indirect effect | 0.39 | 0.12 | 0.04 | .001 | [0.05, 0.19] |
| M2: Discrimination → Belongingness → Depression | |||||
| Indirect effect | 0.04 | 0.02 | .05 | [0.00, 0.08] | |
| Direct effect | 0.15 | 0.06 | .01 | [0.03, 0.27] | |
| Total effect | 0.31 | 0.07 | <.001 | [0.18, 0.50] | |
| Nondisclosure → Belongingness → Depression | |||||
| Indirect effect | 0.02 | 0.02 | .15 | [0.00, 0.07] | |
| Direct effect | 0.01 | 0.06 | .90 | [−0.11, 0.12] | |
| Total effect | 0.03 | 0.06 | .60 | [−0.08, 0.14] | |
| M1: Internalization → Hopelessness → Depression | |||||
| Indirect effect | 0.65 | 0.22 | 0.05 | .007 | [0.13, 0.31] |
| M2: Internalization → Belongingness → Depression | |||||
| Indirect effect | 0.08 | 0.04 | .05 | [0.00, 0.17] | |
| Direct effect | 0.04 | 0.07 | .55 | [−0.09, 0.18] | |
| Total effect | 0.34 | 0.07 | <.001 | [0.19, 0.41] | |
| Outcome: Anxiety symptoms | |||||
| M1: Discrimination → Hopelessness → Anxiety | |||||
| Indirect effect | 0.18 | 0.07 | 0.03 | .007 | [0.03, 0.13] |
| M2: Discrimination → Belongingness → Anxiety | |||||
| Indirect effect | 0.18 | 0.07 | 0.02 | .007 | [0.03, 0.13] |
| Direct effect | 0.27 | 0.07 | <.001 | [0.09, 0.39] | |
| Total effect | 0.40 | 0.07 | <.001 | [0.19, 0.37] | |
| Nondisclosure → Belongingness → Anxiety | |||||
| Indirect effect | 0.50 | 0.04 | 0.02 | .02 | [0.01, 0.09] |
| Direct effect | −0.08 | 0.07 | .25 | [−0.22, 0.05] | |
| Total effect | −0.04 | 0.07 | .61 | [−0.11, 0.06] | |
| M1: Internalization → Hopelessness → Anxiety | |||||
| Indirect effect | 0.43 | 0.13 | 0.04 | .001 | [0.06, 0.21] |
| M2: Internalization → Belongingness → Anxiety | |||||
| Indirect effect | 0.50 | 0.15 | 0.04 | .001 | [0.08, 0.25] |
| Direct effect | 0.02 | 0.07 | .72 | [−0.11, 0.15] | |
| Total effect | 0.30 | 0.06 | <.001 | [0.10, 0.24] | |
Note. Proportion mediated is only presented for significant indirect effects.
Path Analysis Results for Individuals Who Have Knowledge of Antitrans Legislation Introduced in One’s State of Residence (Group 2)
Regarding direct effects, many but not all hypotheses were supported for individuals who were aware that antitrans legislation had been introduced in their state of residence (see Figure 2). More specifically, transgender discrimination and internalized transphobia were negatively associated with sense of belonging (a11, a13) and positively associated with hopelessness (a21, a22). Hopelessness was in turn positively associated with both depressive and anxiety symptoms (b21, b22). Contrary to hypotheses, however, identity nondisclosure was not associated with sense of belonging. In turn, sense of belonging was not associated with depressive or anxiety symptoms. Notably, beyond differences in the statistical significance of relations among study variables, the size of some atemporal effects differed for individuals in Group 2 compared to those in Group 1 as well. Among predictors, the strength of the atemporal association of transgender discrimination with sense of belonging and hopelessness increased, while the strength of the association of internalized transphobia with sense of belonging decreased. Further, the strength of the atemporal association of hopelessness with anxiety also increased.
Figure 2.

Path Analysis Results for Transgender and Gender-Diverse Adults Who Are Aware of Antitrans Legislation Introduced in Their State of Residence (Group 2)
Depressive Symptoms.
Atemporal mediation analysis revealed that transgender discrimination was indirectly associated with depressive symptoms through sense of belonging and hopelessness, with hopelessness explaining 47% and sense of belonging 32% of the total atemporal effect of transgender discrimination on depressive symptoms. Internalized transphobia was also indirectly associated with depressive symptoms, but only through hopelessness and not sense of belonging, with hopelessness explaining 62% of the total atemporal effect of internalized transphobia with depressive symptoms. Finally, identity nondisclosure was not indirectly related to depressive symptoms.
Anxiety Symptoms.
Regarding atemporal indirect effects of study predictors with anxiety symptoms, transgender discrimination and internalized transphobia were also indirectly associated with anxiety symptoms through the mediating role of hopelessness, explaining 62% of the total effect of discrimination with anxiety symptoms and 58% of the total effect of internalized transphobia with anxiety symptoms. Transgender discrimination, identity nondisclosure, and internalized transphobia were not indirectly linked with anxiety symptoms through sense of belonging (see Table 4 for all direct and indirect effects for Group 2).
Table 4.
Nested Mediated Path Analysis for Group 2: Individuals Who Have Knowledge of Antitrans Legislation Introduced in Their State of Residence
| Mediated Path Estimates | Proportion mediateda | β | SE | p value | Adjusted 95% CIs |
|---|---|---|---|---|---|
| Outcome: Depressive symptoms | |||||
| M1: Discrimination → Hopelessness → Depression | |||||
| Indirect effect | 0.47 | 0.16 | 0.05 | .002 | [0.09, 0.31] |
| M2: Discrimination → Belongingness → Depression | |||||
| Indirect effect | 0.32 | 0.11 | 0.06 | .06 | [0.02, 0.25] |
| Direct effect | 0.07 | 0.09 | .44 | [−0.10, 0.26] | |
| Total effect | 0.34 | 0.08 | <.001 | [0.17, 0.52] | |
| Nondisclosure → Belongingness → Depression | |||||
| Indirect effect | 0.03 | 0.03 | .39 | [−0.01, 0.13] | |
| Direct effect | 0.11 | 0.09 | .21 | [−0.07, 0.27] | |
| Total effect | 0.14 | 0.09 | .10 | [−0.04, 0.28] | |
| M1: Internalization → Hopelessness → Depression | |||||
| Indirect effect | 0.62 | 0.13 | 0.06 | .03 | [0.03, 0.26] |
| M2: Internalization → Belongingness → Depression | |||||
| Indirect effect | 0.08 | 0.05 | .12 | [0.00, 0.20] | |
| Direct effect | −0.01 | 0.10 | .97 | [−0.21, 0.18] | |
| Total effect | 0.21 | 0.12 | .07 | [−0.02, 0.40] | |
| Outcome: Anxiety symptoms | |||||
| M1: Discrimination → Hopelessness → Anxiety | |||||
| Indirect effect | 0.62 | 0.18 | 0.06 | .002 | [0.10, 0.36] |
| M2: Discrimination → Belongingness → Anxiety | |||||
| Indirect effect | 0.03 | 0.06 | .62 | [−0.08, 0.16] | |
| Direct effect | 0.08 | 0.09 | .39 | [−0.10, 0.26] | |
| Total effect | 0.29 | 0.08 | .001 | [0.07, 0.31] | |
| Nondisclosure → Belongingness → Anxiety | |||||
| Indirect effect | 0.01 | 0.03 | .75 | [−0.02, 0.08] | |
| Direct effect | 0.13 | 0.13 | .29 | [−0.11, 0.37] | |
| Total effect | 0.14 | 0.12 | .24 | [−0.06, 0.22] | |
| M1: Internalization → Hopelessness → Anxiety | |||||
| Indirect effect | 0.58 | 0.15 | 0.07 | .04 | [0.03, 0.30] |
| M2: Internalization → Belongingness → Anxiety | |||||
| Indirect effect | 0.02 | 0.05 | .68 | [−0.07, 0.13] | |
| Direct effect | 0.09 | 0.11 | .44 | [−0.14, 0.30] | |
| Total effect | 0.26 | 0.13 | .04 | [0.01, 0.29] | |
Note. Proportion mediated is only presented for significant indirect effects
Discussion
The present study investigated the role of sense of belonging and hopelessness as two psychological mechanisms by which minority stress may be linked to depressive and anxiety symptoms among TGD adults. An additional aim of this study was to explore the degree to which knowledge regarding a critically time-relevant form of antitrans structural stigma (antitrans legislative efforts in one’s state of residence) moderated the pattern of relations among study variables. Because results suggested that antitrans legislation did have a moderating impact on the overall pattern of results, we conducted a nested model path analysis in order to identify the differences that emerged between the two groups (those who had knowledge of antitrans legislation in their state of residence and those who did not). First, regarding the direct relations of minority stressors (transgender discrimination, internalized transphobia, and identity nondisclosure) with sense of belonging and hopelessness, knowledge of antitrans legislative efforts in one’s state of residence exacerbated the deleterious links of transgender discrimination with both sense of belonging and hopelessness. Inversely, the strength of the links of internalized transphobia with sense of belonging and hopelessness decreased. This pattern suggests that for those who resided in a state where antitrans legislation has been introduced or passed and were aware of such legislative efforts, discrimination events may have a more negative impact on hopelessness and one’s sense of belonging in society compared to internalized processes. Moreover, for these individuals, hopelessness increased, which in turn strengthened its association with adverse mental health. As a result, hopelessness may reflect an affective and cognitive response to powerlessness and disempowerment at the hands of individuals in direct positions of power (e.g., police officers, supervisors), as well as by the state.
Although powerlessness is often described in the literature as synonymous with helplessness, they are conceptually distinct phenomena (Drew, 1990). Helplessness, or the inability to help oneself (Clements & Cummings, 1991), is a phenomenon often discussed as a key component of “learned helplessness” (Seligman, 1972). With learned helplessness, an individual’s perceived inability to affect an outcome results in failing to initiate effective interventions, which leads to further perceived helplessness. In contrast, powerlessness, although also marked by a perceived inability to affect an outcome, is defined as the inability to defend oneself against existential and other forms of threat (Clements & Cummings, 1991). As a result, for TGD individuals who face threats to their well-being and to some basic civil rights, the pattern of results in the present study suggests that powerlessness may be a mechanism by which hopelessness and subsequent depression and anxiety may relate. Future research could therefore investigate the relations of hopelessness and powerlessness with psychological distress using longitudinal methods that also more clearly delineate temporal and causal effects among variables of interest.
Another key finding that emerged was that for those who had knowledge of antitrans legislation in their state, sense of belonging was not associated with depressive and anxiety symptoms directly, nor did it explain the links of minority stressors with depressive and anxiety symptoms indirectly. This finding was inconsistent with study hypotheses where we expected that antitrans sentiment, as expressed not only through interpersonal discriminatory experiences but also through systemic efforts to curb trans rights, would detract from one’s sense of belonging in society and act to exacerbate its impact on mental health. Instead, the percentage of variance explained in depressive and anxiety symptoms increased dramatically in the links of minority stress with mental health outcomes through hopelessness for those who had knowledge of antitrans legislative efforts in their state of residence. This specific finding suggests that sense of belonging may be less salient for those facing greater systemic barriers than hopelessness. This finding also raises questions regarding how belongingness was operationalized in this study. In the present study, we investigated TGD individuals’ general sense of belonging in society, which fit with our study aims of exploring the degree to which systemic efforts to restrict trans rights might impact mental health. However, past research suggests that TGD community engagement and connectedness as a strategy for coping with oppression and marginalization are critical for many TGD people’s mental health and well-being (e.g., Barr et al., 2016). As a result, facing the threat or actual enactment of legislation restricting trans rights may lead TGD people to seek out connection with other TGD individuals and communities to bolster external resources and sense of safety. Future research could explore this by including measures of general societal belongingness as well as TGD community connectedness. A longitudinal design, for example, could assess the temporal mediating effects of general belongingness in predicting psychological distress, while investigating the potential moderating role of TGD community connection and other variables (e.g., TGD identity strength) as resistance strategies and resilience factors to buffering the harmful impacts of antitrans stigma. Such a design could add rich nuance to our understanding of how, when, and why antitrans stigma may lead to adverse health outcomes within TGD populations.
Limitations and Future Directions
This study has a number of limitations. First, its cross-sectional design precludes our ability to determine temporal and causal effects in our model testing. Instead, data were collected at a single time point over a period of 3–4 months; this allowed us to gather timely and relevant data related to participants’ knowledge and awareness of any antitrans legislative efforts under way in their state of residence but did not allow us to determine changes that might have occurred over time. A fruitful approach for determining more directly how such legislative efforts impact TGD individuals may be to design and conduct a longitudinal study where data can be collected prior and then in response to critical events, for example, conducting a data collection wave shortly after legislation is first introduced in a state and measuring the rate of change in study variables in subsequent waves.
Another limitation of this study is its overrepresentation of White study participants. Although this study’s demographic composition is similar to published research employing similar online participant recruitment methods (e.g., Bockting et al., 2013; Budge et al., 2013; Kuper et al., 2012; Tebbe & Moradi, 2016), research with TGD populations must shift in its recruitment methods to increase racial and ethnic diversity in sampling. Furthermore, because of this study’s design, participants were recruited through online forums, which necessarily limited participation in this study to those who have access to the Internet and a device on which to complete the survey (e.g., a computer or smartphone). With research documenting far greater rates of poverty, housing insecurity and instability, and discrimination, harassment, and violence for TGD Black, Indigenous, and people of color (BIPOC) compared to White TGD persons (James et al., 2016), issues of equity in access to the resources that were necessary for completing this study likely contributed to the disproportionate overrepresentation of White TGD individuals and underrepresentation of TGD BIPOC individuals. As a result, future research in this area needs to critically consider issues of equity regarding study access and participation, as well as relevance of study aims.
Finally, it should be noted that levels of depression and anxiety symptoms among participants in this study were high, with 71.4% reporting moderate or higher levels of anxiety and 32.2% of participants being classified as probable for an MDD diagnosis using the Van Dam and Earleywine (2011) classification algorithm of CESD-R scores. At this time, true prevalence rates of mental health concerns among TGD populations are unknown in the absence of large-scale epidemiological studies employing probabilistic sampling methods. However, it should not be assumed that this sample is representative of the larger TGD adult population in the United States, likely overrepresenting individuals with significant anxiety and depression symptoms. Thus, a separate but related avenue for future research should attend to obtaining better estimates of the scope of mental health concerns across TGD populations on the whole and within specific TGD communities.
Clinical and Advocacy Implications
Findings from the present study point to a number of important clinical and advocacy considerations for mental health providers working with TGD individuals and communities. First, we join other scholars’ calls for psychologists and other mental health providers to consider the social, legal, political, and cultural context in which TGD individuals’ psychological distress is embedded (e.g., American Psychological Association, 2015; Hendricks & Testa, 2012; Singh, 2016). Results from this study underscore the critical need for mental health providers to be attentive to the rapidly shifting landscape of legislation and policy affecting TGD persons in their local and state community, as well as to integrate this awareness into case conceptualization and treatment planning with TGD clients. Recently, Coyne et al. (2020) recommended that case conceptualizations of transgender youth clients focus on (a) normalizing the adverse impact of minority stress, (b) facilitating emotional awareness and regulation, (c) restructuring minority stress cognitions, (d) empowering assertive communication, (e) reducing maladaptive avoidance, (f) validating strengths, and (g) building supportive relationships.
In particular, because hopelessness explained far more variance in the relations of minority stress and depressive and anxiety symptoms for individuals who have knowledge of antitrans legislation, hopelessness is an especially important consideration for conceptualization, treatment planning, and intervention. Therapeutic strategies for addressing hopelessness in the face of such widespread marginalization could include helping clients connect to others who have faced similar experiences and barriers, identify personal strengths and resources, and explore possibilities for the future. There is now a substantial body of literature focused on the strengths and resilience of transgender individuals. A synthesis of this literature, the Transgender Resilience Intervention model (Matsuno & Israel, 2018), seeks to guide the development of interventions to increase the resilience of TGD people by categorizing group and individual resilience factors and examining their potential for buffering, preventing, and ameliorating the effects of proximal and distal stressors on mental health. Strength-based interventions focused on fostering resilience are a promising avenue for partnering with TGD clients and communities to address hopelessness and other discrimination-related adverse mental health outcomes. Furthermore, treatment models that offer TGD clients greater autonomy and empowerment when navigating interactions with medical gender-affirmation treatment (e.g., informed consent model of care; Schulz, 2018) should be prioritized over practitioner-gatekeeper models of care.
Second, the findings of this study emphasize the relevance of structural competency as a framework for training and professional development in counseling psychology (Ali & Sichel, 2014). Structural competency refers to a health care provider’s trained ability to discern how clients’ presenting problems reflect down-stream implications of structural factors like health care, policy, institutional practices, and access to food, education, decent work, and housing (Metzl & Hansen, 2014). Structural competency involves recognizing the structures that shape clinical interactions, developing extraclinical language, developing structural interventions, and developing structural humility (Metzl & Hansen, 2014). This requires an explicit focus, in education, training, research, and practice, on the structural processes by which individuals are marginalized and their health affected. Such knowledge over time can create opportunities to move beyond addressing specific instances of distress to prevention and emancipation (Ali & Sichel, 2014). Thus, ways forward for improving mental health care for TGD clients should involve developing research-based, advocacy-oriented programs that train practitioners to think about how social, cultural, and material structures affect the well-being of transgender clients.
Beyond the direct services mental health providers can provide when face-to-face with clients, mental health providers are also well suited to be advocates within the systems they work (Myers et al., 2002). Providers receive extensive training in how to listen, how to hold difficult conversations, and how to communicate effectively even when closely held values do not align—all skills essential to advocacy within larger systems. Mental health providers can also serve as bridges to connect community members with organizations to build and support community coalitions that can carry advocacy efforts forward with pooled resources and supports. Indeed, any advocacy efforts toward ending marginalization and oppression of trans people and communities should align with existing movements, such as Black Lives Matter and #MeToo, as racism and sexism intersect with transphobia to reinforce and maintain oppression across marginalized groups (e.g., Files-Thompson & McConatha, 2019).
Finally, we contend that continuing to conduct, publish, and disseminate health research aiming to identify structural and other contextual factors underlying TGD health concerns is a critical form of advocacy in which psychologists and other health researchers can engage. Health research knowledge has the potential to shape policy and legislation in a way that we believe complements the direction action advocacy efforts of community organizers and others. Indeed, leading public health organizations (e.g., World Health Organization) have called for more effective utilization of health research into policy implementation and practice (Hanney et al., 2003; Hanney & González-Block, 2017; Pang et al., 2003), and evidence suggests that scientific research is frequently drawn upon in the policy development process (Clancy et al., 2012; Tabak et al., 2015). For example, a recent study investigated the sources of information that health advocates looked for and relied upon in their efforts to influence health policy and legislation, finding that advocates frequently searched for scientific sources (e.g., published studies, reports) and rated information and research originating from universities as more reliable and believable than any other source after the advocate’s own organization (Tabak et al., 2015). Despite these findings, however, there remains a gap in health research knowledge and application to practice settings and policy development, which scholars argue is due in part to ineffective dissemination (Brownson et al., 2018). Drawing across disciplines, Brownson and colleagues set forward recommendations for how researchers can expand current dissemination practices to reach key audiences more effectively and measure their impact. Although a lengthier discussion of these practices is beyond the scope of this present study, we encourage researchers in this area to review Brownson and colleagues’ recommendations and to turn to the growing literature on health research and policy to expand the reach of published research. We believe that continued efforts to document the harmful health impacts of antitrans stigma, paired with effective and wider-reaching dissemination strategies, are critical apparatuses in health advocacy work.
In conclusion, this study investigated sense of belonging and hopelessness as two mechanisms by which TGD minority stressors related to depressive and anxiety symptoms. With the recent rise of antitrans legislation introduced in states around the nation, we also explored the degree to which knowledge of such legislative efforts moderated the pattern of relations among study variables. Findings suggest that these legislative efforts do have a significant impact on how minority stress relates to depressive and anxiety symptoms, providing some important considerations for intervention strategies aimed at addressing TGD mental health.
Public Significance Statement.
Antitrans legislative efforts significantly shape the effects of antitrans stigma and marginalization on mental health for trans and gender-diverse (TGD) individuals, exacerbating the relative importance of hopelessness over sense of belonging, as well as external events versus internalized processes in predicting depression and anxiety. Findings point to the need for continued advocacy for trans-affirmative policy and protections to address known TGD mental health disparities.
Acknowledgments
This study is supported by the National Institute of Mental Health (T32MH082761). The content of the manuscript is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute of Mental Health or the National Institutes of Health. To the best of our knowledge, no conflict of interest, financial or other, exists.
References
- Ali A, & Sichel CE (2014). Structural competency as a framework for training in counseling psychology. The Counseling Psychologist, 42 (7), 901–918. 10.1177/0011000014550320 [DOI] [Google Scholar]
- American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). [Google Scholar]
- American Psychological Association. (2015). Guidelines for psychological practice with transgender and gender nonconforming people. American Psychologist, 70(9), 832–864. 10.1037/a0039906 [DOI] [PubMed] [Google Scholar]
- Barr SM, Budge SL, & Adelson JL (2016). Transgender community belongingness as a mediator between strength of transgender identity and well-being. Journal of Counseling Psychology, 63(1), 87–97. 10.1037/cou0000127 [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA, Beck JS, & Newman CF (1993). Hopelessness, depression, suicidal ideation, and clinical diagnosis of depression. Suicide &Life-Threatening Behavior, 23(2), 139–145. 10.1111/j.1943-278X.1993.tb00378.x [DOI] [PubMed] [Google Scholar]
- Bennett DA (2001). How can I deal with missing data in my study? Australian and New Zealand Journal of Public Health, 25(5), 464–469. 10.1111/j.1467-842X.2001.tb00294.x [DOI] [PubMed] [Google Scholar]
- Bockting WO, Miner MH, Swinburne Romine RE, Hamilton A, & Coleman E (2013). Stigma, mental health, and resilience in an online sample of the U.S. transgender population. American Journal of Public Health, 103(5), 943–951. 10.2105/AJPH.2013.301241 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brooks V (1981). Minority stress and lesbian women. Free Press. [Google Scholar]
- Brownson RC, Eyler AA, Harris JK, Moore JB, & Tabak RG (2018). Getting the word out: New approaches for disseminating public health science. Journal of Public Health Management and Practice, 24(2), 102–111. 10.1097/PHH.0000000000000673 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Budge SL, Adelson JL, & Howard KAS (2013). Anxiety and depression in transgender individuals: The roles of transition status, loss, social support, and coping. Journal of Consulting and Clinical Psychology, 81(3), 545–557. 10.1037/a0031774 [DOI] [PubMed] [Google Scholar]
- Burns DD (1998). Therapist’s toolkit. Unpublished manuscript.
- Clancy CM, Glied SA, & Lurie N (2012). From research to health policy impact. Health Services Research, 47(1, Part 2), 337–343. 10.1111/j.1475-6773.2011.01374.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clements S, & Cummings S (1991). Helplessness and powerlessness: Caring for clients in pain. Holistic Nursing Practice, 6(1), 76–85. 10.1097/00004650-199110000-00013 [DOI] [PubMed] [Google Scholar]
- Clements-Nolle K, Marx R, & Katz M (2006). Attempted suicide among transgender persons. Journal of Homosexuality, 51(3), 53–69. 10.1300/J082v51n03_04 [DOI] [PubMed] [Google Scholar]
- Coyne CA, Poquiz JL, Janssen A, & Chen D (2020). Evidence-based psychological practice for transgender and non-binary youth: Defining the need, framework for treatment adaptation, and future directions. Evidence-Based Practice in Child and Adolescent Mental Health, 5(3), 340–353. 10.1080/23794925.2020.1765433 [DOI] [Google Scholar]
- Davidson K, McLaren S, Jenkins M, Corboy D, Gibbs PM, & Molloy M (2017). Internalized homonegativity, sense of belonging, and depressive symptoms among Australian gay men. Journal of Homosexuality, 64(4), 450–465. 10.1080/00918369.2016.1190215 [DOI] [PubMed] [Google Scholar]
- Davis M, & Wertz K (2009). When laws are not enough: A study of the economy health of transgender people and the need for a multidisciplinary approach to economic justice transgender issues and the law. Seattle Journal for Social Justice, 8(2), 467–496. [Google Scholar]
- Drew BL (1990). Differentiation of hopelessness, helplessness, and powerlessness using Erik Erikson’s “Roots of virtue.” Archives of Psychiatric Nursing, 4(5), 332–337. 10.1016/0883-9417(90)90053-N [DOI] [PubMed] [Google Scholar]
- Eaton WW, Smith C, Ybarra M, Muntaner C, & Tien A (2004). Center for Epidemiologic Studies Depression Scale: Review and revision (CESD and CESD-R). In Maruish ME & Maruish ME (Eds.), The use of psychological testing for treatment planning and outcomes assessment: Instruments for adults (Vol. 3, 3rd ed., pp. 363–377). Erlbaum. [Google Scholar]
- Ennis D (2016, February 22). Report: 2016 is the most dangerous year for transgender Americans. Advocate. https://www.advocate.com/transgender/2016/2/22/report-2016-most-dangerous-year-transgender-americans [Google Scholar]
- Files-Thompson N, & McConatha M (2019). Mobilizing allies for Black transgender women: Digital stories, intersectionality, and #sayhername. In Eguchi S & Calafell B (Eds.), Queer intercultural communication: The intersectional politics of belonging in and across differences (pp. 239–257). Rowman & Littlefield. [Google Scholar]
- Fisher LB, Overholser JC, Ridley J, Braden A, & Rosoff C (2015). From the outside looking in: Sense of belonging, depression, and suicide risk. Psychiatry, 78(1), 29–41. 10.1080/00332747.2015.1015867 [DOI] [PubMed] [Google Scholar]
- Freedom for All Americans. (n.d.). 2020. Legislative tracker: Anti-transgender legislation. https://www.freedomforallamericans.org/2020-legislative-tracker/2020-anti-transgender-legislation [Google Scholar]
- Grant MG (2017, May 3). After the transgender tipping point. Pacific Standard Magazine. https://psmag.com/news/after-the-transgender-tipping-point#.tlm6cfos4 [Google Scholar]
- Hagerty BM, Lynch-Sauer J, Patusky KL, Bouwsema M, & Collier P (1992). Sense of belonging: A vital mental health concept. Archives of Psychiatric Nursing, 6(3), 172–177. 10.1016/0883-9417(92)90028-H [DOI] [PubMed] [Google Scholar]
- Hagerty BM, & Patusky K (1995). Developing a measure of sense of belonging. Nursing Research, 44(1), 9–13. 10.1097/00006199-199501000-00003 [DOI] [PubMed] [Google Scholar]
- Hanney SR, & González-Block MA (2017). ‘Knowledge for better health’ revisited—the increasing significance of health research systems: A review by departing editors-in-chief. Health Research Policy and Systems, 15(1), 81. 10.1186/s12961-017-0248-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hanney SR, Gonzalez-Block MA, Buxton MJ, & Kogan M (2003). The utilisation of health research in policy-making: Concepts, examples and methods of assessment. Health Research Policy and Systems, 1(1), 2. 10.1186/1478-4505-1-2 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML (2009). How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychological Bulletin, 135(5), 707–730. 10.1037/a0016441 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML (2016). Structural stigma and health inequalities: Research evidence and implications for psychological science. The American Psychologist, 71(8), 742–751. 10.1037/amp0000068 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatzenbuehler ML, & Link BG (2014). Introduction to the special issue on structural stigma and health. Social Science & Medicine, 103, 1–6. 10.1016/j.socscimed.2013.12.017 [DOI] [PubMed] [Google Scholar]
- Hatchel T, & Marx R (2018). Understanding intersectionality and resiliency among transgender adolescents: Exploring pathways among peer victimization, school belonging, and drug use. International Journal of Environmental Research and Public Health, 15(6), Article 1289. 10.3390/ijerph15061289 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hatchel T, Valido A, De Pedro KT, Huang Y, & Espelage DL (2019). Minority stress among transgender adolescents: The role of peer victimization, school belonging, and ethnicity. Journal of Child and Family Studies, 28(9), 2467–2476. 10.1007/s10826-018-1168-3 [DOI] [Google Scholar]
- Hendricks ML, & Testa RJ (2012). A conceptual framework for clinical work with transgender and gender clients: An adaptation of the minority stress model. Professional Psychology: Research and Practice, 43(5), 460–467. 10.1037/a0029597 [DOI] [Google Scholar]
- Herman JL, Mallory C, & Wilson BD (2016). Estimates of transgender populations in states with legislation impacting transgender people. https://escholarship.org/uc/item/7f78c7xq
- Hu L, & Bentler PM (1998). Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychological Methods, 3(4), 424–453. 10.1037/1082-989X.3.4.424 [DOI] [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. 10.1080/10705519909540118 [DOI] [Google Scholar]
- James SE, Herman JL, Rankin S, Keisling M, Mottet L, & Anafi M (2016). The report of the 2015 U.S. Trans Survey. National Center for Transgender Equality; http://www.ustranssurvey.org/report/ [Google Scholar]
- Kuper LE, Nussbaum R, & Mustanski B (2012). Exploring the diversity of gender and sexual orientation identities in an online sample of transgender individuals. Journal of Sex Research, 49(2–3), 244–254. 10.1080/00224499.2011.596954 [DOI] [PubMed] [Google Scholar]
- Lester D (2001). An inventory to measure helplessness, hopelessness, and haplessness. Psychological Reports, 89(3), 495–498. 10.2466/pr0.2001.89.3.495 [DOI] [PubMed] [Google Scholar]
- Lester D, & Walker RL (2007). Hopelessness, helplessness, and haplessness as predictors of suicidal ideation. Omega: Journal of Death and Dying, 55(4), 321–324. 10.2190/OM.55.4.f [DOI] [PubMed] [Google Scholar]
- MacKinnon DP, Lockwood CM, & Williams J (2004). Confidence limits for the indirect effect: Distribution of the product and resampling methods. Multivariate Behavioral Research, 39(1), 99–128. 10.1207/s15327906mbr3901_4 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mallinckrodt B, Abraham WT, Wei M, & Russell DW (2006). Advances in testing the statistical significance of mediation effects. Journal of Counseling Psychology, 53(3), 372–378. 10.1037/0022-0167.53.3.372 [DOI] [Google Scholar]
- Matsuno E, & Israel T (2018). Psychological interventions promoting resilience among transgender individuals: Transgender Resilience Intervention Model (TRIM). The Counseling Psychologist, 46(5), 632–655. 10.1177/0011000018787261 [DOI] [Google Scholar]
- Metzl JM, & Hansen H (2014). Structural competency: Theorizing a new medical engagement with stigma and inequality. Social Science & Medicine, 103, 126–133. 10.1016/j.socscimed.2013.06.032 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer IH (1995). Minority stress and mental health in gay men. Journal of Health and Social Behavior, 36(1), 38–56. 10.2307/2137286 [DOI] [PubMed] [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129(5), 674–697. 10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mustanski B, & Liu RT (2013). A longitudinal study of predictors of suicide attempts among lesbian, gay, bisexual, and transgender youth. Archives of Sexual Behavior, 42(3), 437–448. 10.1007/s10508-012-0013-9 [DOI] [PubMed] [Google Scholar]
- Muthén LK, & Muthén BO (2011). Mplus user’s guide.
- Myers JE, Sweeney TJ, & White VE (2002). Advocacy for counseling and counselors: A professional imperative. Journal of Counseling and Development, 80(4), 394–402. 10.1002/j.1556-6678.2002.tb00205.x [DOI] [Google Scholar]
- Nadal KL, Davidoff KC, Davis LS, & Wong Y (2014). Emotional, behavioral, and cognitive reactions to microaggressions: Transgender perspectives. Psychology of Sexual Orientation and Gender Diversity, 1(1), 72–81. 10.1037/sgd0000011 [DOI] [Google Scholar]
- Pang T, Sadana R, Hanney S, Bhutta ZA, Hyder AA, & Simon J (2003). Knowledge for better health: A conceptual framework and foundation for health research systems. Bulletin of the World Health Organization, 81(11), 815–820. 10.1590/S0042-96862003001100008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rostosky SS, Riggle EDB, Horne SG, Denton FN, & Huellemeier JD (2010). Lesbian, gay, and bisexual individuals’ psychological reactions to amendments denying access to civil marriage. American Journal of Orthopsychiatry, 80(3), 302–310. 10.1111/j.1939-0025.2010.01033.x [DOI] [PubMed] [Google Scholar]
- Schulz SL (2018). The informed consent model of transgender care: An alternative to the diagnosis of gender dysphoria. Journal of Humanistic Psychology, 58(1), 72–92. 10.1177/0022167817745217 [DOI] [Google Scholar]
- Seligman MEP (1972). Learned helplessness. Annual Review of Medicine, 23(1), 407–412. 10.1146/annurev.me.23.020172.002203 [DOI] [PubMed] [Google Scholar]
- Shumer DE, Harris LH, & Opipari VP (2016). The effect of lesbian, gay, bisexual, and transgender-related legislation on children. Journal of Pediatrics, 178, 5–6.e1. 10.1016/j.jpeds.2016.08.028 [DOI] [PubMed] [Google Scholar]
- Singh AA (2016). Moving from affirmation to liberation in psychological practice with transgender and gender nonconforming clients. American Psychologist, 71(8), 755–762. 10.1037/amp0000106 [DOI] [PubMed] [Google Scholar]
- Steinmetz K (2014, May 29). The transgender tipping point. TIME. https://time.com/magazine/us/135460/june-9th-2014-Vol.-183-no-22-u-s/ [Google Scholar]
- Tabak RG, Eyler AA, Dodson EA, & Brownson RC (2015). Accessing evidence to inform public health policy: A study to enhance advocacy. Public Health, 129(6), 698–704. 10.1016/j.puhe.2015.02.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tebbe EA, Allan BA, & Bell HL (2018). Work and well-being in TGNC adults: The moderating effect of workplace protections. Journal of Counseling Psychology, 66(1), 1–13. 10.1037/cou0000308 [DOI] [PubMed] [Google Scholar]
- Tebbe EA, & Budge SL (2016). Research with trans communities: Applying a process-oriented approach to methodological considerations and research recommendations. The Counseling Psychologist, 44(7), 996–1024. 10.1177/0011000015609045 [DOI] [Google Scholar]
- Tebbe EA, & Moradi B (2016). Suicide risk in trans populations: An application of minority stress theory. Journal of Counseling Psychology, 63(5), 520–533. 10.1037/cou0000152 [DOI] [PubMed] [Google Scholar]
- Testa RJ, Habarth J, Peta J, Balsam K, & Bockting W (2015). Development of the gender minority stress and resilience measure. Psychology of Sexual Orientation and Gender Diversity, 2(1), 65–77. 10.1037/sgd0000081 [DOI] [Google Scholar]
- Testa RJ, Michaels MS, Bliss W, Rogers ML, Balsam KF, & Joiner T (2017). Suicidal ideation in transgender people: Gender minority stress and interpersonal theory factors. Journal of Abnormal Psychology, 126(1), 125–136. 10.1037/abn0000234 [DOI] [PubMed] [Google Scholar]
- Van Dam NT, & Earleywine M (2011). Validation of the Center for Epidemiologic Studies Depression Scale–Revised (CESD-R): Pragmatic depression assessment in the general population. Psychiatry Research, 186(1), 128–132. 10.1016/j.psychres.2010.08.018 [DOI] [PubMed] [Google Scholar]
- Watson LB, Allen LR, Flores MJ, Serpe C, & Farrell M (2019). The development and psychometric evaluation of the Trans Discrimination Scale: TDS-21. Journal of Counseling Psychology, 66(1), 14–29. 10.1037/cou0000301 [DOI] [PubMed] [Google Scholar]