

Our findings have implications for the wider adoption of work from home (WFH) arrangements. Hybrid approaches, combining home and work-based employment are preferred and could alleviate the negative health impacts associated with WFH. Addressing inequalities across the workforce to ensure that everyone can participate in this shift is also key.
Keywords: employment, work from home, remote working, mental well-being, health behaviors, inequalities, COVID-19
Objective
The aim of the study is to provide insights into the working Welsh adult population’s perceptions of the health impacts of working from home (WFH), their ability to WFH, and their WFH preferences.
Methods
Data were collected from 615 working adults in Wales between November 2020 and January 2021 in a household survey.
Results
More than 45% of those able to WFH reported worsened mental well-being and loneliness. Working from home worsened the diets, physical activity, smoking, and alcohol use of those in poorer health. Approximately 50% were able to WFH, although individuals living in more deprived areas, in atypical employment or with precarious income, were less able to WFH. Nearly 60% wanted to WFH to some capacity.
Conclusions
The new way of working introduces new challenges to preserving workforce mental well-being, regulating health behaviors, and tackling inequalities. Hybrid models and targeted health support could make WFH healthier and more equitable.
Learning Objectives
After participating in this activity, the learner will be better able to:
Identify advantages and disadvantages of working from home across this article’s surveyed populations.
Explain additional considerations for flexible working arrangements of the future.
Outline the advantage of hybrid models and targeted home health support as part of the work from option
Strict home working requirements have been implemented by numerous administrations globally as a key strategy to slow the spread of coronavirus (SARS-CoV-2).1–3 This has led to one of the most striking societal transformations of the COVID-19 pandemic. Home working, historically, the privilege of a small minority of workers,4 is now the new norm for many.5 Estimations from early on in the pandemic suggested that approximately 50% of Europeans worked from home to some extent as a result of the pandemic, compared with only 12% before its onset.6 The COVID-19 pandemic serves as an unplanned experiment at mass scale7—studying this transition into home working and people’s preferences for the future is vital.
Home working can offer benefits for individuals, employers, and society. For example, working from home offers greater flexibility. Having the option to work from home could make work and its associated health benefits more accessible for subgroups that need greater flexibility, for example, those with care responsibilities or those dealing with health conditions, which may make accessing work more challenging.8–11 In turn, improving the accessibility of work protects against unemployment and its negative health impacts.12 Home working may also improve work-life balance and the productivity of work, while also offering protection from exposure to communicable diseases.5,13 On a societal level, home working may provide an attractive opportunity to contribute to protecting the climate through reducing carbon emissions generated by the commute.14–16
However, the pandemic has also shed light on some of the potential negative outcomes of a more permanent adoption of work from home policies. The burden on mental health has been well documented throughout the COVID-19 pandemic. Working from home can be isolating, negatively impacting mental well-being and levels of physical activity, and holding the potential to detrimentally impact physical health for those with inadequate resources to ensure a safe working environment at home, for example, ergonomic equipment.13
Despite these potential disadvantages, there is both population- and policy-level evidence to suggest that the transition to home working has been welcomed. Of those within the UK population who have worked from home during the pandemic, 88.2% wish to continue to some degree, with 47.3% wishing to work from home either often or all the time.5 Several governments have announced their support for adopting work from home policies more permanently. For example, in 2020, the German labor minister stated their intention to publish a draft law establishing the legal right to work from home.17 In the same year, the Welsh Government demonstrated a desire to preserve the increased prevalence of remote working spurred by the pandemic, aiming to have 30% of Welsh workers working from or near home.18,19 This target aligns with estimates for global workforce remote working levels after the pandemic20 and would result in Wales mirroring a handful of European Union countries’ prepandemic levels of remote working—a surplus of 30% of those in work teleworked at least sometimes in Sweden, Luxembourg, Finland, and the Netherlands before the COVID-19 pandemic in 2019.21
While home working has increased, the availability of roles for which remote working is possible is largely dependent on the economic makeup of individual countries and the distribution of roles across sectors. Resultantly, some individuals are well positioned to benefit from a transition into home working, while others may be left disadvantaged. Higher-paid roles are more likely to allow for home working, while workers within certain sectors are less likely to be offered the opportunity to work remotely, for example, those working within hospitality or retail.21 The COVID-19 pandemic has also highlighted how work from home may be less accessible for key workers,13 those in precarious or low paid work,22,23 and the digitally excluded.24,25 Between 2018 and 2019, 11% of Welsh adults could be categorized as digitally excluded, with those within households in the most deprived areas being less likely to have access to the Internet than those in the least deprived areas (83% compared with 92%26). A transition into home working has potential to both ameliorate and exacerbate inequalities for certain population groups, which could in turn impact their health.
In conclusion, with work from home practices likely here to stay, exploring the perceived health impacts of home working and the extent to which the ability to work from home is equitable across population subgroups could generate valuable insights to inform its future rollout. Combining these insights with further evidence on people’s preferences for future home working could contribute in ensuring that any policy-level changes that promote the continuation of home working protect against causing damage to health or widening inequalities and cater to the preferences of the workforce.
In this article, we use Welsh data to assess:
How does working from home impact the self-reported health of the workforce and different population subgroups within it?
How does the ability to work from home differ across population subgroups?
How do preferences for time spent working from home in future compare across population subgroups?
METHODS
Study Design
This study uses data from the final wave of a 2-wave nationally representative longitudinal household survey undertaken across Wales. The Public Health Wales COVID-19, Employment and Health in Wales study was carried out between May 2020 and January 2021 to explore the impact of the novel coronavirus (COVID-19) outbreak on the employment, health, and well-being of the Welsh population. The Health Research Authority gave ethical approval for the study (IRAS: 282223). The survey was presented to respondents as an exploration of how their employment, and health and well-being compared before and during the pandemic. Questions relating to working from home were only asked in the final wave of the study—this article makes use of this cross-sectional data.
Study Population and Recruitment
All working age adults (between 18 and 64 years) resident in Wales, in current employment as of February 2020, were eligible, with those who were in full-time education or unemployed being excluded. Full details of the initial recruitment and sampling strategy for the longitudinal survey are discussed elsewhere.27 A push-to-web approach was used (with telephone and paper surveys offered to those without access). Respondents gave informed consent to participate at all stages of the study, being informed that their participation was voluntary and that their responses would be confidential.
Those consenting to follow up after the first wave (1084 of the 1382 in the initial survey sample) provided responses for the final wave between November 2020 and January 2021. If a valid email address was provided (n = 925), individuals were emailed an invitation to take part, with two further email reminders to encourage participation. If a valid email address was not provided (n = 159), individuals were sent a postal invitation and one reminder invitation. In total, 626 individuals completed the follow-up online questionnaire (58% of those who gave consent for follow-up). Nine responses were excluded as identification codes were inputted incorrectly, leaving a sample of 615 (98.2% of final wave responses).
Questionnaire Measures
Participants were asked whether it was possible for them to work from home in their main job (“able”/“unable”/“not sure”). Those stating that they were able to work from home were asked how working from home had affected 7 aspects of their health and well-being (“feelings of loneliness,” “mental well-being,” “smoking,” “eating well,” “drinking alcohol,” “exercise,” “work-life balance”), with a response of “better,” “no change,” and “worse,” with the comparator assumed to be employment and health before the pandemic.
All respondents, regardless of whether they were currently able to work from home, were asked to report their preferences for time spent working from home in the future (“all working days home working,” “half or more,” “less than half,” “no home working,” “not sure”), with the question making reference to the population-level increase in the prevalence of home working as a result of the pandemic. For further details on the questionnaire measures used, see Supplemental Digital Content 1, http://links.lww.com/JOM/B112.
To explore how the previously mentioned differed across population subgroups, measurements from questions relating to socioeconomic status, health, and employment/income were also taken. Explanatory variables included age group, sex, deprivation quintile (assigned using the Welsh Index of Multiple Deprivation28 and residential postcode data), individual self-reported general health and presence of limiting preexisting conditions (using validated questions from the National Survey for Wales29), and mental well-being (using the short version of the Warwick Edinburgh Mental Well-being Scale30 and using 1 standard deviation below the mean as our cutoff score for low mental well-being). Explanatory variables relating to employment and income were also included—these were employment contract type (permanent, fixed term, atypical, self-employed/freelance), furlough status, wage precariousness (see Supplemental Digital Content 1, http://links.lww.com/JOM/B112, for computation across 3 variables) based on the Employment Precariousness Scale,31 and job skill level (calculated using the Standard Occupational Classification for the United Kingdom32).
Statistical Approach
To account for differences in the representativeness of the respondents to the Welsh population, proportions and bivariate analyses were weighted against Welsh population estimates in 2018 for ages 18 to 64, for the same 5 age groups, sex, and Welsh Index of Multiple Deprivation quintiles.33 Sample characteristics, both crude and weighted to the Welsh population estimates, are presented (see Supplemental Digital Content 2, http://links.lww.com/JOM/B113).
χ2 and Fisher exact tests were used to explore associations across socioeconomic groups, employment and income, and health status. Multivariate binary and multinomial logistic regressions (adjusting for socioeconomic factors, employment and income, and self-reported health) were used to identify independent predictors of the health impacts of working from home, the ability to work from home, and preferences for future home working. Statistical analysis was undertaken in IBM SPSS Statistics (Version 24, Armonk, NY: IBM Corp) and RStudio (Version 1.4.1103, PBC, Boston, MA).
RESULTS
Sample Characteristics
Crude proportions demonstrated that respondents predominantly identified as women (63.7%) and that those aged between 40 and 59 years were overrepresented within the sample (40–49, 24.6%; 50–59, 32.7%). There was representation across all other working ages. These proportions were weighted against the Welsh population for sex, age, and Welsh Index of Multiple Deprivation in our bivariate analyses. Sample characteristics, crude, and weighted to the Welsh population are provided (see Supplemental Digital Content 2, http://links.lww.com/JOM/B113).
Research Question 1: How Does Working From Home Impact the Self-reported Health of the Workforce and Different Population Subgroups Within It?
Respondents who could work from home (n = 299) were asked to self-report how working from home had affected their health and well-being, noting whether feelings of loneliness, mental well-being, smoking, diet, exercise, alcohol consumption, and work-life balance were left unchanged, improved, or worsened, compared with life prepandemic (Fig. 1).
FIGURE 1.
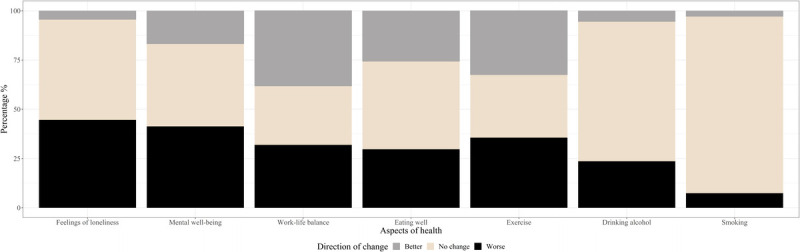
Percentage reporting improvements, no change or deteriorations in various aspects of their health and well-being as a result of home working. Weighted to 2018 Welsh population estimates for 18–64 year olds.
As shown in Figure 1, respondents who could work from home were more likely to report that it worsened their feelings of loneliness and mental well-being than to say it improved it, with more than 45% indicating deteriorations for both aspects of health and well-being (and only 2.5% and 16.9%, respectively, reporting improvements). The same pattern was seen for alcohol consumption, with 25.7% reporting deterioration, and only 5.7% reporting an improvement, and, to a lesser extent, smoking (with 2.5% reporting an improvement and 6% reporting deterioration). However, these patterns did differ across population subgroups (see Supplemental Digital Content 3, http://links.lww.com/JOM/B114, which show the proportion of individuals within each subgroup reporting each health outcome, and independent predictors of health outcomes as determined within multivariate logistic regression models).
Socioeconomic Factors and Living Arrangements
Respondents younger than 50 years were more likely to report a worsening in feelings of loneliness and their mental well-being as a result of working from home. When controlling for all other factors, it was found that those in their 30s were more than 3 times more likely than those in their 40s to report a worsening in their feelings of loneliness as a result of home working (adjusted odds ratio (aOR) = 3.32 [95% confidence interval (CI) = 1.24–8.88]). Those in their 50s were significantly less likely to report deteriorations in their mental well-being than those in their 40s (aOR = 0.30 [95% CI = 0.11–0.82]), again corroborating the idea that younger individuals were more likely to see the negative impacts of home working on their mental well-being.
Younger respondents were also more likely than older respondents to report that their diet worsened as a result of home working, with those in their 30s being nearly 5 times more likely to report deteriorations in their diet than those in their 40s (aOR = 4.65 [95% CI = 1.44–14.44]). Similarly, when controlling for all other factors, individuals in their 30s were 6 times more likely than those in their 40s to report that working from home had a detrimental impact on their levels of physical activity (aOR = 6.10 [95% CI = 1.76–21.15]).
Employment and Income
Those in fixed term employment were less likely than those in permanent employment to report a deterioration in their sense of loneliness (aOR = 0.10 [95% CI = 0.02–0.61]).
Health Status
The multivariate model indicated that those in poorer health were more than 7 times more likely to report a deterioration in their diet (aOR = 7.24 [95% CI = 2.33–22.49]), over 5 times more likely to report a deterioration in their levels of physical activity (aOR = 5.26 [95% CI = 1.72–16.12]), nearly 8 times more likely to report deteriorations in their smoking habits (aOR = 7.94 [95% CI = 1.03–61.43]), and nearly 3 times more likely to report a worsening of levels of alcohol consumption (aOR = 2.73 [95% CI = 1.05–7.10]) when compared with their healthier counterparts.
Individuals with low mental well-being who worked from home were significantly more likely to report a deterioration in their sense of loneliness than their counterparts with average mental well-being (aOR = 18.98 [95% CI = 3.53–102.07]), with 74.2% of those with low mental well-being reporting becoming lonelier, and only 45.4% of their healthier counterparts reporting the same. Those with low well-being were also more than 4 times more likely to say that their well-being deteriorated as a result of working from home (aOR = 4.44 [95% CI = 1.25–15.79]).
A significantly greater proportion of individuals with limiting preexisting health conditions reported that working from home worsened their mental well-being (61.4% compared with 41.7%, P = 0.02) and work-life balance (53.5% compared with 31.3%, P = 0.01), compared with those without such conditions. However, these effects were not mirrored in the model when controlling for other factors. The model did however indicate that individuals with limiting preexisting conditions were significantly less likely to report a worsening in their smoking habits, compared with their counterparts without such conditions (aOR = 0.08 [95% CI = 0.01–0.90]).
Research Question 2. How Does the Ability to Work From Home Differ Across Population Subgroups?
Respondents who were unsure of whether they were able to work from home were excluded from the analysis, leaving a total of 577 respondents. Of these individuals, 47.7% reported that it was possible for them to work from home in their main job. The ability to work from home differed by socioeconomic factors, employment and income, and health (see Supplemental Digital Content 4, http://links.lww.com/JOM/B115, for associations and full model outputs).
Socioeconomic Factors and Living Arrangements
When controlling for all other factors within the model, women were nearly twice as likely as men (aOR = 1.85 [95% CI = 1.11–3.08]) to report being able to work from home. In addition, associations indicated that a smaller proportion of those living in the most deprived areas (P < 0.0001), those living alone (P = 0.01), and those without children in their households (P = 0.003) were able to work from home (see Supplemental Digital Content 4, http://links.lww.com/JOM/B115).
Employment and Income
Those in atypical employment were less likely to be able to work from home than those in permanent employment (aOR = 0.11 [95% CI = 0.01–0.88])—only 15% could do so, compared with 49.4% of those in permanent employment. Those with high wage precarity were also less likely to be able to work from home than their counterparts with low wage precarity (aOR = 0.29 [95% CI = 0.15–0.55])—only 23.8% were able to work from home, compared with 56% for those with low wage precarity.
Health Status
A lower proportion of individuals who reported having lower mental well-being were able to work from home when compared with their healthier counterparts (32.6% compared with 50.3%, P = 0.002), with the same pattern holding true for those with limiting preexisting conditions (40% compared with 50.8%, P = 0.04). However, these effects were not reflected in the model when controlling for all other factors.
Research Question 3: How Do the Preferences for Time Spent Working From Home in Future Compare across Population Subgroups?
Nearly 60% of the sample wanted to spend at least some of their working week working from home (59.1%); however, only 13.3% wished to work from home all the time. A quarter of respondents indicated a desire to spend more than half their working week (but not the whole week) working from home in the future (25.1%), while 20.7% wished to spend less than half (but some of) the week working from home. A similar proportion indicated their desire to avoid working from home entirely (17.1%). There was also a degree of uncertainty, with over a fifth not sure of their preferences for future home working (23.8%). These proportions differed across the socioeconomic, employment and income, and health factors of interest (see Supplemental Digital Content 5, http://links.lww.com/JOM/B116, which show associations and multivariate multinomial regression model outputs).
Socioeconomic Factors and Living Arrangements
Women were nearly 3 times more likely than men to want to work from home all the time instead of half the time (aOR = 2.63 [95% CI = 1.06–6.50]). In contrast, those in their 30s were less likely to report wanting to work from home all the time than those in their 40s (aOR = 0.29 [95% CI = 0.09–0.96]), and individuals who lived alone were more than 2 times more likely to not want to work from home at all (aOR = 2.40 [95% CI = 1.05–5.50]).
A significant association was found between deprivation level and ability to work from home (P < 0.001), with a greater proportion of individuals living in the most deprived areas reporting that they wanted to avoid working from home entirely, and a lower proportion saying that they wanted to spent at least half the working week home working. A significantly lower proportion of those who lived alone wanted to work from home full-time (only 5% compared with 15.6% for those living with others), while a larger proportion of them wanted to work full-time from an office or base—27.7% compared with 13.8% (P < 0.0001). In addition, a greater proportion of those with children in their households wanted to spend all week, or at least half the week working from home, while a lower proportion wanted to spend less than half the week home working, or working from an office or base full-time (P = 0.01).
Employment and Income
The self-employed/freelancers were nearly 7 times more likely than those in permanent employment to want to work from home all the time instead of half the time or more (aOR = 6.98 [95% CI = 1.98–24.59]). More than half of those in atypical employment were not sure of their preferences, and this group was the least likely to report a preference for full-time home working.
Over a third of those furloughed were unsure of their preferences for future home working (38.8%), with these individuals being 3 times more likely to say that they were uncertain of their preferences for future home working than their counterparts who had not been furloughed (aOR = 3.09 [95% CI = 1.40–6.82]).
Likewise, a third of those with high wage precarity were not sure of their preferences for time spent working from home in future (33.6%), being more than 4 times more likely to state they were uncertain of their preference than those with low wage precarity (aOR = 4.32 [95% CI = 1.69–11.05]).
DISCUSSION
First and foremost, our findings offer new insights into the potential health impacts of working from home, highlighting major concerns for protecting the mental well-being and loneliness of home workers and population subgroups that may be particularly vulnerable to these negative health impacts. Second, we demonstrated that while approximately half the sample were able to work from home (47.7%), the potentiality to work from home was not evenly distributed across population subgroups, with some at a greater risk of being left behind in any wider rollout of work from home policies.
Despite these health concerns and inequities in potentiality to work from home, there is an appetite for working from home in the future in Wales, with approximately 60% showing a preference for working from home to some capacity. These findings align with previous work with an UK-wide sample, indicating that nearly 90% of those who worked from home during the pandemic wished to continue doing so to some extent, with nearly half wishing to work from home either often or all the time.5 Within our sample, over a third wished to continue to work from home either full-time or for half the working week or more.
The insights produced in this study, therefore, suggest that for many in Wales, working from home is a viable and preferable option. While, on one hand, these findings could be seen to forecast that efforts to achieve a wider adoption of home working in future are set to be well received by the workforce, they also highlight some key areas for implementing protective action. We discuss 3 key implications for the development of policy promoting and supporting home working, specifically around supporting the potential health impacts of working from home, addressing potential inequalities in home working, and flexing working arrangements and workplaces.
Identifying and Supporting the Health Impacts of Home Working
A key concern for the wider adoption of home working is its health impacts. Although home working can offer multiple benefits, including protecting health through limiting exposure to communicable diseases,5,8–13 working from home can present its own health challenges. Of those who could work from home, more than 45% reported that their mental well-being and their sense of loneliness deteriorated as a result of home working. These findings align with those of the Understanding Society COVID-19 Study, which showed that those who worked from home full-time during the United Kingdom’s first national lockdown reported significant deteriorations in their well-being, including their enjoyment of normal activities, experiences of strain, their ability to concentrate, and experiencing unhappiness/depression.5
Of note, the Understanding Society COVID-19 Study showed that those who worked from home part-time had significantly better outcomes and that those home working full-time became less severely affected by June 2020 (compared with April and May). The authors suggested that these effects became less apparent over time as individuals either became accustomed to home working or were able to return to work if it had severely affected their mental well-being. With our Welsh data gathered between November 2020 and January 2021, it would seem that the detrimental impacts of home working could have persisted later into the year, with this perhaps indicating a combined effect of home working, the winter months and government restrictions.
With the same Understanding Society COVID-19 Study showing that those who adopted a hybrid home working model were less affected,5 pursuing the Welsh public’s preference for a hybrid model (with 45.8% of our sample wanting a hybrid approach) could contribute in protecting against the negative impacts on well-being that full-time home working might produce. Caution must be taken to avoid the negative health outcomes that our sample reported experiencing, particularly for their mental well-being.
Our findings also suggest that younger individuals (younger than 50 years) and those with low mental well-being are more likely to report experiencing these detriments to their mental well-being and sense of loneliness when working from home. Processes that allow for regular review of full-time home workers’ health may prove beneficial in boosting the effectiveness of the adoption of home working on a longer term basis, as would providing targeted support for groups that are more likely to report feelings of isolation or see their mental well-being deteriorate (eg, peer support groups, access to work networks, advice and guidance).
Alcohol consumption and smoking habits were also more likely to worsen than improve for those working from home. Similar patterns have been found by others for both alcohol consumption (eg, 30% of a 2777 self-selected UK sample reported drinking more frequently during lockdown34; harmful alcohol use increased for those WFH under lockdown in the United States between April and September 202035) and smoking (eg, 28% of an US sample of 291 tobacco users reported increasing their cigarette use during the pandemic, reporting increased time at home as one of their reasons36). A possible explanation is that the increased freedoms and privacy that home working can offer opens the door for engaging in behaviors that would otherwise be reserved for outside of working hours or working environments.35 While hybrid approaches would reduce these impacts, employees may require additional support in maintaining workplace standards within the home environment. Home worker health reviews could signpost to resources for support in curbing unhealthy habits.
Home working seemed to detrimentally impact many subgroups’ diets and levels of physical activity—a pattern already highlighted as a risk of home working in previous work.37 In our sample, those in their 30s and those with poorer general health were more likely to report these effects. Our findings highlight an important issue, with the data indicating that home working introduced additional health challenges to those with poorer general and mental health. Individuals with poorer general health were 7 times more likely to report a worsened diet as a result of home working, over 5 times more likely to report a deterioration in their levels of physical activity, and reported a worsening in their engagement in health-harming behaviors (alcohol consumption and smoking). In addition to being more likely to experience deteriorations in their sense of loneliness and their mental well-being, individuals with low mental well-being also saw their diets suffer. The disruptive shift to home working may have interrupted many individuals’ preexisting habits and routines. While other research has suggested that the negative impacts of home working on diet and physical activity may subside as individuals get accustomed to these work-related changes,38 efforts should be made to support individuals in establishing healthier habits while working from home, particularly those individuals that may be balancing efforts to maintain such habits while attending to their other health needs. The disproportionate self-reported negative health impacts of home working on those with poorer health are of particular concern when considering the fact that working from home is associated with increased sickness presenteeism,39,40 which holds the potential to worsen existing health problems further still.
Addressing Inequalities in Home Working
The second concern for the wider adoption of home working is the fact that the ability to work from home is not evenly distributed across society. Within the context of the COVID-19 pandemic, the inaccessibility of home working translates to increased exposure to the virus if remaining in-work, or financial insecurity if the work cannot continue, for example, being placed on furlough or becoming unemployed.13,27,41 Our findings corroborate those of others, showing that those living in the most deprived areas (who are also most likely to be digitally excluded26), those in atypical employment, and those with high wage precarity are less likely to be able to work from home.22,23 Although not significant when controlling for other factors in the model, significant associations within this sample showed that those with low mental well-being or limiting preexisting conditions were also less likely to be able to work from home. For the latter in particular, provisions that can be put in place at the workplace to support employee needs may not be as easily adopted in the home, with research suggesting that equipment used during home working is less ergonomically suitable, with this affecting work performance for individuals with disabilities.42,43 Wage precarity and atypical working arrangements are associated with increased risks of experiencing ill-health and financial insecurity,44 and individuals with poorer health or limiting conditions are already at a disadvantage in obtaining and retaining work because of the challenges that their symptoms and their treatment needs present.41,45–52
Taken together, a more permanent transition toward home working may cause further insecurity and exclusions for subgroups that are experiencing greater financial insecurity and ill-health, who are at present less able to participate in this change. Supporting individuals with specific work-related needs to address them within the home working environment might help. Further drives to promote working from home that do not account for discrepancies in the accessibility of home working may widen existing inequalities. In the context of COVID-19 or another pandemic response, widening the accessibility of home working for these highlighted groups where possible could help protect their health. Where roles cannot be performed at home (eg, key workers, retail), the increased risk of infection that these subgroups face as a result of their inability to work from home should also be considered when designing support packages at a population level.
Flexing Working Arrangements and Workplaces
For the last of the 3 themes covered in this research, our findings highlight how a wider adoption of home working should account for how different subgroups have different preferences for the time they spend working from home. Doing so may contribute in reducing the negative health impacts and inequalities discussed previously.
While efforts should be made to increase the accessibility of home working for men, who were significantly less likely to be able to work from home than women, women were significantly more likely to want to work from home throughout the working week. The flexibility that home working can offer is well suited for a population group that are more likely to carry the burden of caring responsibilities. In contrast, those who lived in the most deprived areas and those who lived alone were more likely to show a preference for avoiding home working entirely, while those in their 30s were less likely to want to work from home full-time. For the latter two, working from a base (at least occasionally) would presumably allow for greater opportunities for socialization. Research has suggested that those living alone are more likely to experience mental illness.53 Furthermore, work-related situational constraints that affect the extent to which individuals spend time within physical proximity to colleagues, or the frequency of their interactions, can affect employees’ sense of isolation.54
Looking to the future, embedding these preferences into practice where appropriate could help alleviate some of the negative health impacts of working from home reported by our sample. With home working associated with increased loneliness and detriments to well-being, initiatives that promote further remote or home working could protect against isolation through adopting hybrid approaches, supporting individuals in accessing remote working hubs or through ensuring that employers provide home workers with support in maintaining social contact when they work from home. As discussed, younger individuals and those with low mental well-being were more likely to report deteriorations in their mental well-being and their sense of loneliness as a result of home working. These groups in particular might benefit from having the option to work in an office/base, in a remote working hub, or with a hybrid model combining working on and off site.
Strengths and Limitations
Only those who indicated that they were able to work from home were asked to report how it impacted their health. However, the former question did not allow for distinguishing whether people acted upon this potentiality and did indeed work from home. Despite government guidelines at the time strongly encouraging those able to work from home to do so,55 being able to quantitatively measure the extent to which people worked from home during this period would allow for exploring the associations between home working and health in greater detail. Nevertheless, the key strength of our research is that it can offer novel insights into the expected health impacts of working from home. These expectations are vital considerations when considering the viability of work from home policies and the workforce’s acceptance of such measures and can shape future work that explores whether these expectations do in fact represent causal links.
We assumed that the context given within the wider survey would have asserted that the comparator was prepandemic work and health for all responses, and the results were treated as such. That being said, we acknowledge that there may have been some variability in the ways in which questions using comparative phrasing such as “better,” “no change,” and “worse” were interpreted by different respondents. Interpretation may have differed dependent on whether individuals had worked from home (and to what extent) before the pandemic (2 factors that were not captured within the survey). In a related point about the survey design more widely, questions on working from home were only asked at one time point, meaning that an opportunity to explore the causal relationships between home working and health was missed. These are important caveats to consider when reflecting on the contribution of this work.
The fact that these were self-reported measures, taken during the COVID-19 pandemic, is also a point warranting discussion. For many in our sample, their experiences of home working came as a direct consequence of the pandemic, which in itself contributed to feelings of isolation, presented increased burdens on mental well-being, and impacted people’s engagement in many health-related behaviors. Home working coupled with these may have produced the effects seen here. While this could signify that our findings are best applied in informing future pandemic responses, they do pinpoint population subgroups that might be less able to participate in a transition toward home working and shed light on its potential health impacts. These insights can contribute to ensuring that future policies and practice that promote working from home (be that for future pandemic responses or as part of efforts to tackle climate change) adopt preventative measures, which contribute in protecting against the potential for experiencing increased isolation, declines in mental well-being, increases in health-harming behaviors and decreased engagement in healthy behaviors. Generating knowledge that allows for identifying those who are at risk of the negative health impacts of home working can help inform the development of targeted support for these subgroups going forward.
CONCLUSIONS
While home working has the potential to offer multiple benefits, many have seen it deteriorate their mental well-being and sense of loneliness, with this being particularly true for younger individuals and those with low mental well-being. Less healthy consumption behaviors and more sedentary lifestyles were also thought to arise because of home working within younger groups and those in poorer health.
Individuals with high wage precarity, those on atypical contracts, and those living in the most deprived areas were less likely to be able to work from home. Despite nearly 50% of our sample being able to work from home, the insights gathered in this study suggest that the potentiality to work from home is not equally distributed within Wales, with those facing greatest insecurity being more likely to lose out.
With working from home likely to be adopted as a common practice beyond the COVID-19 pandemic, there is potential for these inequities and adverse health impacts to present a unique public health challenge. The push for a more permanent transition to working from home should account for the current inequities in the potentiality of working from home and offer solutions that protect against the potential detriments to health as highlighted in this work. Supporting the adoption of more hybrid approaches is set to be well received, and some subgroups could benefit from receiving addition social and health support as they spend more time working from home. Supporting individuals as they adapt to this new way of working will help ensure that the benefits of home working can be enjoyed equally, without sacrificing the workforce’s health.
Supplementary Material
Footnotes
Funding sources: This study is supported by the National Centre for Population Health and Wellbeing Research, funded by Health and Care Research Wales.
Griffiths, Gray, Kyle, Song, and Davies have no relationships/conditions/circumstances that present potential conflict of interest.
The JOEM editorial board and planners have no financial interest related to this research.
Ethical approval: The Health Research Authority Research Ethics Committee gave ethical approval for this study (IRAS: 282223).
Supplemental digital contents are available for this article. Direct URL citation appears in the printed text and is provided in the HTML and PDF versions of this article on the journal’s Web site (www.joem.org).
Contributor Information
Benjamin J. Gray, Email: benjamin.gray@wales.nhs.uk.
Richard G. Kyle, Email: R.Kyle@exeter.ac.uk.
Jiao Song, Email: Jiao.Song@wales.nhs.uk.
Alisha R. Davies, Email: Alisha.Davies@wales.nhs.uk.
REFERENCES
- 1.Rubin O, Nikolaeva A, Nello-Deakin S, te Brömmelstroet M. What can we learn from the COVID-19 pandemic about how people experience working from home and commuting? Centre for Urban Studies, University of Amsterdam. May. 2020;6. Available at: https://urbanstudies.uva.nl/content/blog-series/covid-19-pandemic-working-from-home-and-commuting.html?cb. Accessed December 16, 2021. [Google Scholar]
- 2.Arshed N, Meo MS, Farooq F. Empirical assessment of government policies and flattening of the COVID19 curve. J Public Aff. 2020;20:e2333. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Miles D, Stedman M, Heald AH. “Stay at home, protect the National Health Service, save lives”: a cost benefit analysis of the lockdown in the United Kingdom. Int J Clin Pract. 2021;75:e13674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Felstead A, Jewson N, Phizacklea A, Walters S. The option to work at home: another privilege for the favoured few? New Technol Work Employ. 2002;17:204–223. [Google Scholar]
- 5.Felstead A, Reuschke D. Homeworking in the UK: before and during the 2020 lockdown. WISERD. 2020. Available at: https://wiserd.ac.uk/publications/homeworking-uk-and-during-2020-lockdown. Accessed November 11, 2021.
- 6.Eurofound . Living, working and COVID-19. Publications Office of the European Union. 2020. Available at: https://op.europa.eu/en/publication-detail/-/publication/3803fd7a-141b-11eb-b57e-01aa75ed71a1/language-en. Accessed December 12, 2021.
- 7.Kramer A, Kramer KZ. The potential impact of the COVID-19 pandemic on occupational status, work from home, and occupational mobility. J Vocat Behav. 2020;119:103442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Holland P, Collins AM. “Whenever I can I push myself to go to work”: a qualitative study of experiences of sickness presenteeism among workers with rheumatoid arthritis. Disabil Rehabil. 2018;40:404–13. [DOI] [PubMed] [Google Scholar]
- 9.UK Government . Government response: health is everyone’s business. UK Government. 2021. Available at: https://www.gov.uk/government/consultations/health-is-everyones-business-proposals-to-reduce-ill-health-related-job-loss/outcome/government-response-health-is-everyones-business. Accessed October 14, 2021.
- 10.Waddell G, Burton AK. Is Work Good for Your Health and Well-Being?. London: TSO; 2006. [Google Scholar]
- 11.Beatty JE, Joffe R. An overlooked dimension of diversity: the career effects of chronic illness. Organ Dyn. 2006;35:182–95. [Google Scholar]
- 12.van Aerden K, Gadeyne S, Vanroelen C. Is any job better than no job at all? Studying the relations between employment types, unemployment and subjective health in Belgium. Arch Belg. 2017;75:55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dyakova M Couzens L Allen J, et al. Placing health equity at the heart of the COVID-19 sustainable response and recovery: building prosperous lives for all in Wales. Public Health Wales. 2021. Available at: https://phw.nhs.wales/news/placing-health-equity-at-the-heart-of-coronavirus-recovery-for-building-a-sustainable-future-for-wales/. Accessed October 12, 2021.
- 14.Hook A, Court V, Sovacool BK, Sorrell S. A systematic review of the energy and climate impacts of teleworking. Environ Res Lett. 2020;15:093003. [Google Scholar]
- 15.Beno M. Face-to-display working: decarbonisation potential of not commuting to work before COVID-19 and during and after lockdowns. AJIS. 2021;10:17–24. doi: 10.36941/AJIS-2021-0060. [DOI] [Google Scholar]
- 16.Bachelet M, Kalkuhl M, Koch N. What if working From home will stick? Distributional and climate impacts for Germany. SSRN. 2021. [Google Scholar]
- 17.Elliott D. Germany drafting law to give people the legal right to work from home. World Economic Forum. 2020. Available at: https://www.weforum.org/agenda/2020/10/germany-is-set-to-make-home-working-a-legal-right/. Accessed December 2, 2021.
- 18.Welsh Government . Embedding remote working. Welsh Government. 2020. Available at: https://gov.wales/written-statement-embedding-remote-working. Accessed October 14, 2021.
- 19.Welsh Government . Aim for 30% of the Welsh workforce to work remotely. Welsh Government. 2020. Available at: https://gov.wales/aim-30-welsh-workforce-work-remotely#:~:text=Aim%20for%2030%25%20of%20the%20Welsh%20workforce%20to,home%2C%20including%20after%20the%20threat%20of%20Covid-19%20lessens. Accessed November 11, 2021.
- 20.Global Workplace Analytics . Work-at-home after COVID-19—our forecast. Global Workplace Analytics. 2021. Available at: https://globalworkplaceanalytics.com/work-at-home-after-covid-19-our-forecast. Accessed December 2, 2021.
- 21.European Commission Joint Research Centre . Telework in the EU before and after the COVID-19: where we were, where we head to. European Commission. 2020. Available at: https://ec.europa.eu/jrc/sites/default/files/jrc120945_policy_brief_-_covid_and_telework_final.pdf. Accessed December 2, 2021.
- 22.Williams SN, Armitage CJ, Tampe T, Dienes K. Public perceptions and experiences of social distancing and social isolation during the COVID-19 pandemic: a UK-based focus group study. BMJ Open. 2020;10:e039334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Dingel JI, Neiman B. How many jobs can be done at home? J Public Econ. 2020;189:104235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bhandari V. Improving internet connectivity during COVID-19. SSRN. 2020. [Google Scholar]
- 25.Yates S. COVID-19 and digital exclusion: insights and implications for the Liverpool City Region. Heseltine Institute for Public Policy, Practice and Place. 2020. Available at: https://livrepository.liverpool.ac.uk/3110809/1/Heseltine%20Institute%20Policy%20Briefing%20031.pdf. Accessed December 16, 2021.
- 26.Welsh Government . National Survey for Wales, 2018-2019 Internet use and digital skills. Welsh Government. 2019. Available at: https://gov.wales/sites/default/files/statistics-and-research/2019-09/internet-use-and-digital-skills-national-survey-wales-april-2018-march-2019-207.pdf. Accessed November 11, 2021.
- 27.Gray BJ, Kyle RG, Song J, Davies AR. Characteristics of those most vulnerable to employment changes during the COVID-19 pandemic: a nationally representative cross-sectional study in Wales. J Epidemiol Community Health. 2022;76:8–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Welsh Government . Welsh index of multiple deprivation. Welsh Government. 2021. Available: https://gov.wales/welsh-index-multiple-deprivation. Accessed October 13, 2021.
- 29.Welsh Government . National Survey for Wales. Welsh Government. 2021. Available at: https://gov.wales/national-survey-wales. Accessed October 13, 2021.
- 30.Stewart-Brown S Platt S Tennant A, et al. The Warwick-Edinburgh Mental Well-Being Scale (WEMWBS): a valid and reliable tool for measuring mental well-being in diverse populations and projects. J Epidemiol Community Health. 2011;65:A1–A40. [Google Scholar]
- 31.Vives A, González F, Moncada S, Llorens C, Benach J. Measuring precarious employment in times of crisis: the revised Employment Precariousness Scale (EPRES) in Spain. Gac Sanit. 2015;29:379–82. [DOI] [PubMed] [Google Scholar]
- 32.Office for National Statistics . Standard Occupational Classification—SOC 2020. Office for National Statistics. 2020. Available at: https://www.ons.gov.uk/methodology/classificationsandstandards/standardoccupationalclassificationsoc/soc2020. Accessed December 12, 2021.
- 33.Office for National Statistics . Population estimates. Office for National Statistics. 2022. Available at: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationestimates. Accessed February 24, 2022.
- 34.Oldham M, Garnett C, Brown J, Kale D, Shahab L, Herbec A. Characterising the patterns of and factors associated with increased alcohol consumption since COVID-19 in a UK sample. Drug Alcohol Rev. 2021;40:890–899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Killgore WDS, Cloonan SA, Taylor EC, Lucas DA, Dailey NS. Alcohol dependence during COVID-19 lockdowns. Psychiatry Res. 2021;296:113676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Yingst JM, Krebs NM, Bordner CR, Hobkirk AL, Allen SI, Foulds J. Tobacco use changes and perceived health risks among current tobacco users during the COVID-19 pandemic. Int J Environ Res Public Health. 2021;18:1795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Bevan S, Mason B, Bajorek Z. Homeworker Wellbeing Survey. Institute for Employment Studies, UK. 2020. Available at: https://www.employment-studies.co.uk/sites/default/files/resources/summarypdfs/IES%20Homeworker%20Wellbeing%20Survey%20-%20Interim%20Findings.pdf. Accessed November 11, 2021.
- 38.Rogers AM, Lauren BN, Baidal JAW, Ozanne EM, Hur C. Persistent effects of the COVID-19 pandemic on diet, exercise, risk for food insecurity, and quality of life: a longitudinal study among U.S. adults. Appetite. 2021;167:105639. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Karanikas N, Cauchi JP. Literature review on parameters related to work-from-home (WFH) arrangements. Queensland University of Technology. 2020. Available at: https://eprints.qut.edu.au/205308/. Accessed December 17, 2021.
- 40.Steidelmüller C, Meyer SC, Muller G. Home-based telework and presenteeism across Europe. J Occup Environ Med. 2020;62:998–1005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Brannigan C Galvin R Walsh ME, et al. Barriers and facilitators associated with return to work after stroke: a qualitative meta-synthesis. Disabil Rehabil. 2017;39:211–22. [DOI] [PubMed] [Google Scholar]
- 42.Guler MA, Guler K, Guneser Gulec M, Ozdoglar E. Working from home during a pandemic: investigation of the impact of COVID-19 on employee health and productivity. J Occup Environ Med. 2021;63:731–41. [DOI] [PubMed] [Google Scholar]
- 43.Ralph P Baltes S Adisaputri G, et al. Pandemic programming: how COVID-19 affects software developers and how their organizations can help. Empir Softw Eng. 2020;25:4927–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Benach J, Vives A, Amable M, Vanroelen C, Tarafa G, Muntaner C. Precarious employment: understanding an emerging social determinant of health. Annu Rev Public Health. 2014;35:229–53. [DOI] [PubMed] [Google Scholar]
- 45.Khan F, Ng L, Turner-Stokes L. Effectiveness of vocational rehabilitation intervention on the return to work and employment of persons with multiple sclerosis. Cochrane Database Syst Rev. 2009;2009:CD007256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mack H, Paylor I. Employment experiences of those living with and being treated for hepatitis C: seeking reasonable adjustments and the role of disability legislation. Soc Policy Soc. 2016;15:555–70. [Google Scholar]
- 47.van Egmond MP, Duijts SFA, Scholten APJ, van der Beek AJ, Anema JR. Offering a tailored return to work program to cancer survivors with job loss: a process evaluation. BMC Public Health. 2016;16:940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Nexo MA, Cleal B, Hagelund L, Willaing I, Olesen K. Willingness to pay for flexible working conditions of people with type 2 diabetes: discrete choice experiments. BMC Public Health. 2017;17:938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Booth S, Price E, Walker E. Fluctuation, invisibility, fatigue - the barriers to maintaining employment with systemic lupus erythematosus: results of an online survey. Lupus. 2018;27:2284–91. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Hanson H Hart RI Thompson B, et al. Experiences of employment among young people with juvenile idiopathic arthritis: a qualitative study. Disabil Rehabil. 2018;40:1921–8. [DOI] [PubMed] [Google Scholar]
- 51.Paltrinieri S Fugazzaro S Bertozzi L, et al. Return to work in European cancer survivors: a systematic review. Support Care Cancer. 2018;26:2983–94. [DOI] [PubMed] [Google Scholar]
- 52.Murray PD, Brodermann MH, Gralla J, Wiseman AC. Academic achievement and employment in young adults with end-stage kidney disease. J Ren Care. 2019;45:29–40. [DOI] [PubMed] [Google Scholar]
- 53.McManus S, Bebbington P, Jenkins R, Brugha T. Mental health and wellbeing in England: Adult Psychiatric Morbidity Survey [NHS Digital]. 2014. Available at: https://files.digital.nhs.uk/pdf/q/3/mental_health_and_wellbeing_in_england_full_report.pdf. Accessed December 16, 2021.
- 54.Perlman D, Peplau LA. Toward a social psychology of loneliness. In: Duck S, Gilmour R, eds. Personal Relationships in Disorder. London, United Kingdom: Academic Press; 1981:31–56. [Google Scholar]
- 55.Senedd Research . Coronavirus timeline: Welsh and UK government’s response. Welsh Parliament. 2021. Available at: https://research.senedd.wales/research-articles/coronavirus-timeline-welsh-and-uk-governments-response/. Accessed March 10 2022.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.